
Abstract
Background
Double origin of the posterior inferior cerebellar artery (DOPICA) has been rarely reported in the literature, with a reported incidence of 1.45%. In contrast, a high concurrence rate of DOPICA and vertebral artery dissecting aneurysm has been reported.
Clinical presentation
A 61-year old woman presented with vomiting and diplopia with preceding headache. Magnetic resonance imaging (MRI) showed fresh infarction of the left lateral medulla and a vertebral artery dissecting aneurysm of the left vertebral artery. The next day, she exhibited transient loss of consciousness and worsening of headache, and MRI depicted subarachnoid hemorrhage. Four-vessel digital subtraction angiography showed a posterior inferior cerebellar artery (PICA) arising both intracranially and extracranially from the left vertebral artery. Although the dissecting lesion involved the V3 and V4 portion, it did not involve an extracranially originating PICA. Internal trapping of the V3 and V4 portion was chosen as the extracranial channel was expected to supply the PICA territory. This procedure was safely performed.
Conclusion
Early endovascular intervention should be considered in the treatment of dissecting aneurysm of vertebral artery associated with DOPICA for patients with relatively long lesions even in unruptured cases.
Keywords
Introduction
Reports of developmental anomaly of double origin of the posterior inferior cerebellar artery (DOPICA) are rare, with an incidence of 1.45%.1–7 The significance of DOPICA remains unclear, although it is sometimes associated with intracranial aneurysms.2,3,6 In particular, a high rate of concurrence of DOPICA and vertebral artery dissecting aneurysm (VADA) or posterior inferior cerebellar artery (PICA) dissection has been reported.4,7 Intracranial vertebral artery dissections initially presenting without subarachnoid hemorrhage (SAH) usually have a benign nature, and the incidence of recurrent ischemic stroke is low.8–10 However, the optimal management has not been established, partly because of a possibility of subsequent SAH.
Case report
A 61-year-old woman had a preceding headache. The next day, she also had left neck pain and vomiting after a floating sensation. She presented to the emergency department of our hospital while she was almost fully conscious. She also claimed double vision when she looked straight ahead. Diffusion-weighted magnetic resonance imaging (MRI) of the head showed high signal intensity of the left lateral medulla (Figure 1(a)), and magnetic resonance angiography (MRA) showed poor visualization of the left vertebral artery (Figure 1(b)). A fresh infarction of the left medulla due to dissection of the left vertebral artery was suspected, and she was treated conservatively, not using antiplatelets or anticoagulants. However, on the morning following admission, she had transient loss of consciousness, while electrocardiogram showed running of premature ventricular contraction. Thereafter, she had worsening of headache, and subsequent stroke was suspected.
(a) Diffusion weighted image of magnetic resonance imaging (MRI) showed a slightly high signal intensity of left lateral medulla (white arrow). (b) Magnetic resonance angiography showed poor visualization of left vertebral artery, suggesting a dissecting aneurysm. (c) T2* of MRI on the next day showed low signal intensity of subarachnoid space and within ventricles.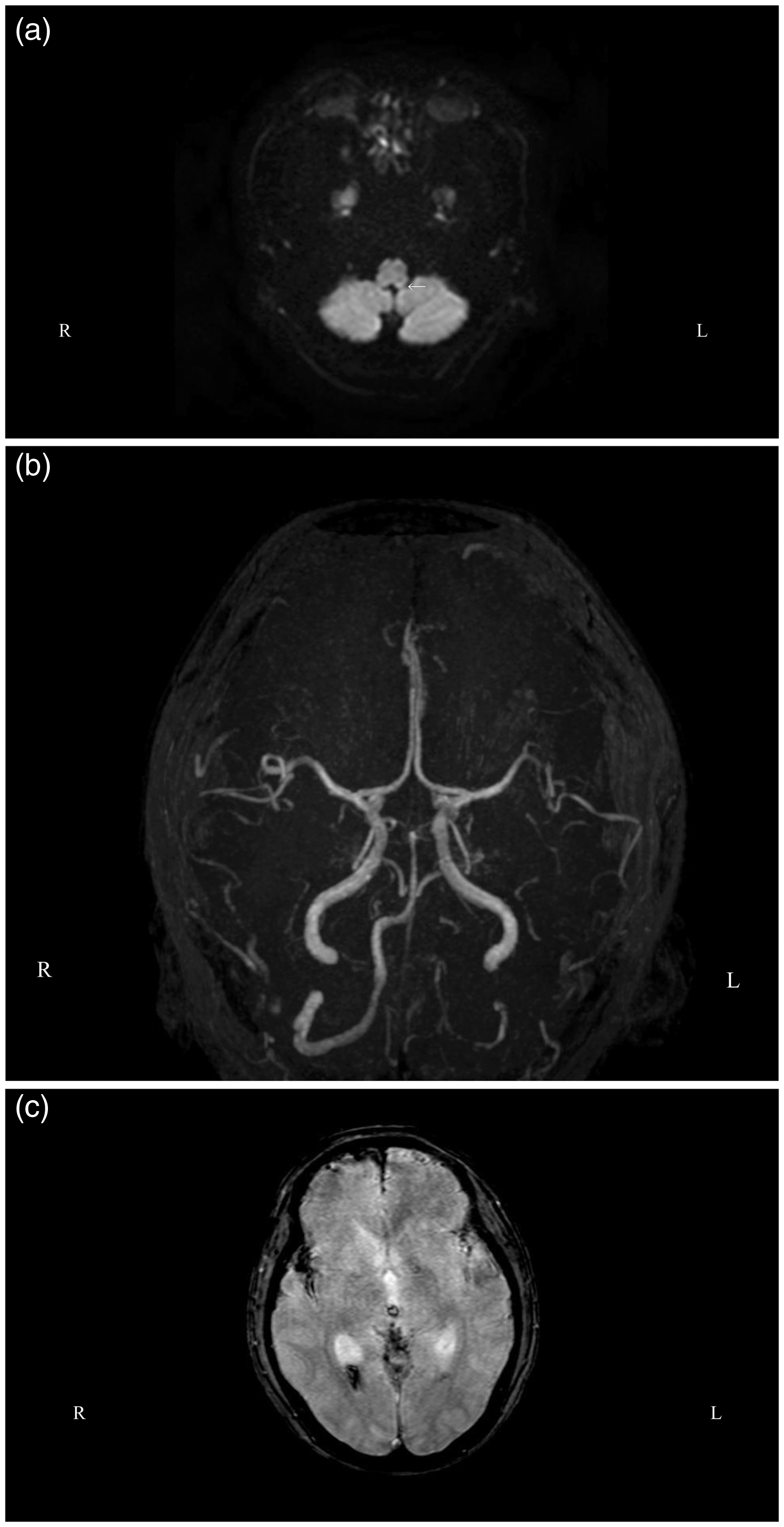
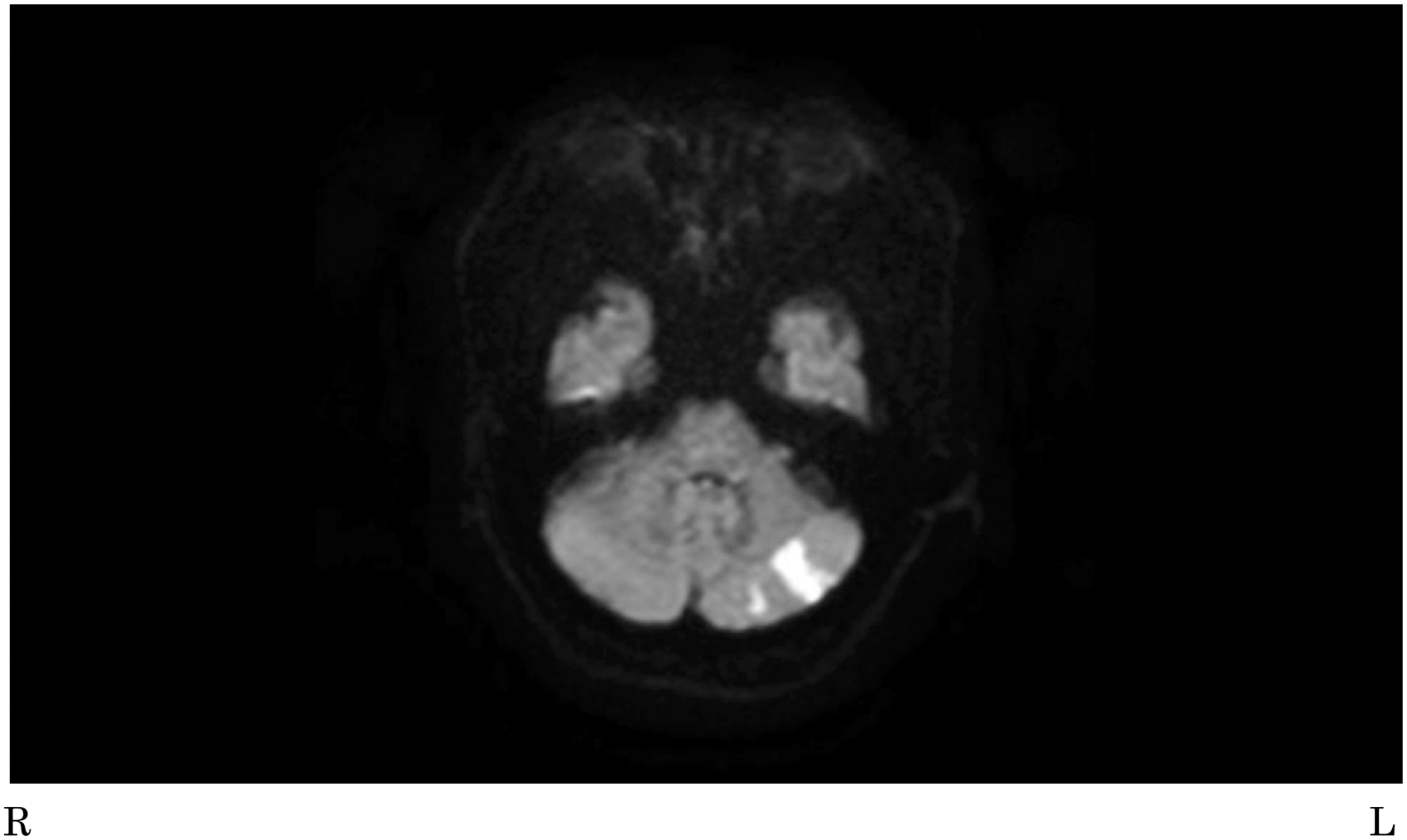
MRI showed diffuse SAH with intraventricular hemorrhage in addition to the infarction of the left medulla (Figure 1(c)). Brain four-vessel digital subtraction angiography confirmed the diagnosis of dissection of the left vertebral artery (Figure 2(a) and (b)). Further, it revealed the double origin of the PICA and that the dissecting lesion largely involved an intracranial origin of the PICA, but not an extracranial origin. Internal trapping was chosen to treat the dissecting lesion as the extracranial channel was expected to supply the PICA territory. The procedure was performed under local anesthesia. The left vertebral artery was catheterized with a 5Fr-guiding catheter through the right femoral artery. A microcatheter was placed into the dissecting lesion, and nine coils were deployed to occlude the lesion. Postoperative angiogram showed patency of the left PICA through the proximal origin (Figure 2(c)). Although postoperative MRI showed small infarcts in the PICA territory probably due to emboli during the procedure (Figure 3), she almost fully recovered except for wooziness and left the hospital to return home. The follow-up angiography at six months after the procedure showed occlusion of intracranial vertebral artery and patency of the extracranial origin of PICA.
Anterolateral view (a) and lateral view (b) of left vertebral artery angiogram showed irregularity of left vertebral artery and double origin of left posterior inferior cerebellar artery (PICA) from intradural (long arrow) and extradural (short arrow) supply. Postprocedural angiogram showed complete occlusion of the dissecting lesion and left PICA was visualized through the caudal channel (c). Diffusion weighted image of postoperative magnetic resonance imaging showed high signal lesions in the territory of the posterior inferior cerebellar artery, suggesting fresh infarcts due to distal emboli during the procedure.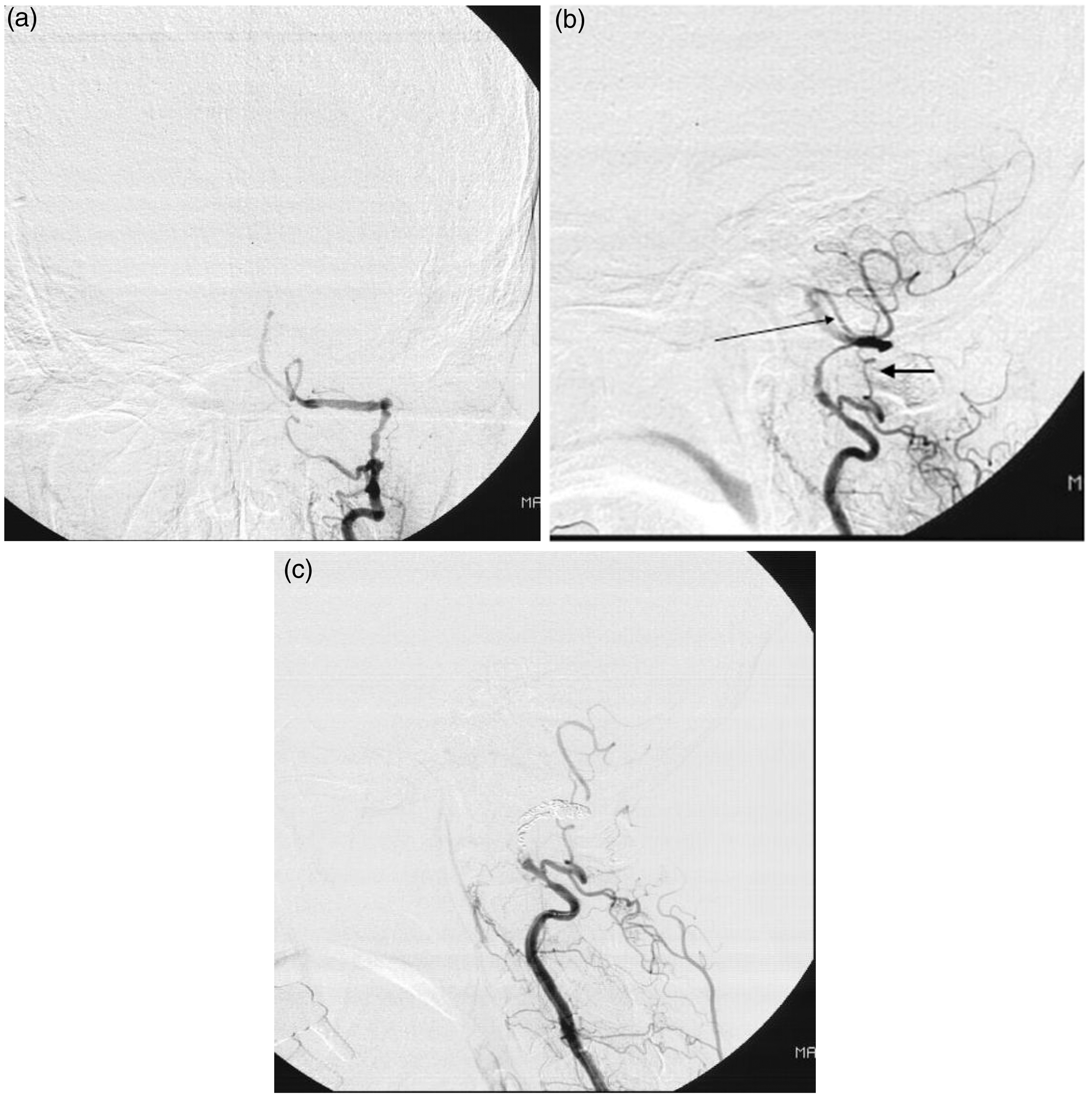
Discussion
Characteristics of dissecting vertebral artery/posterior inferior cerebellar artery aneurysms associated with double origin of the posterior inferior cerebellar artery.
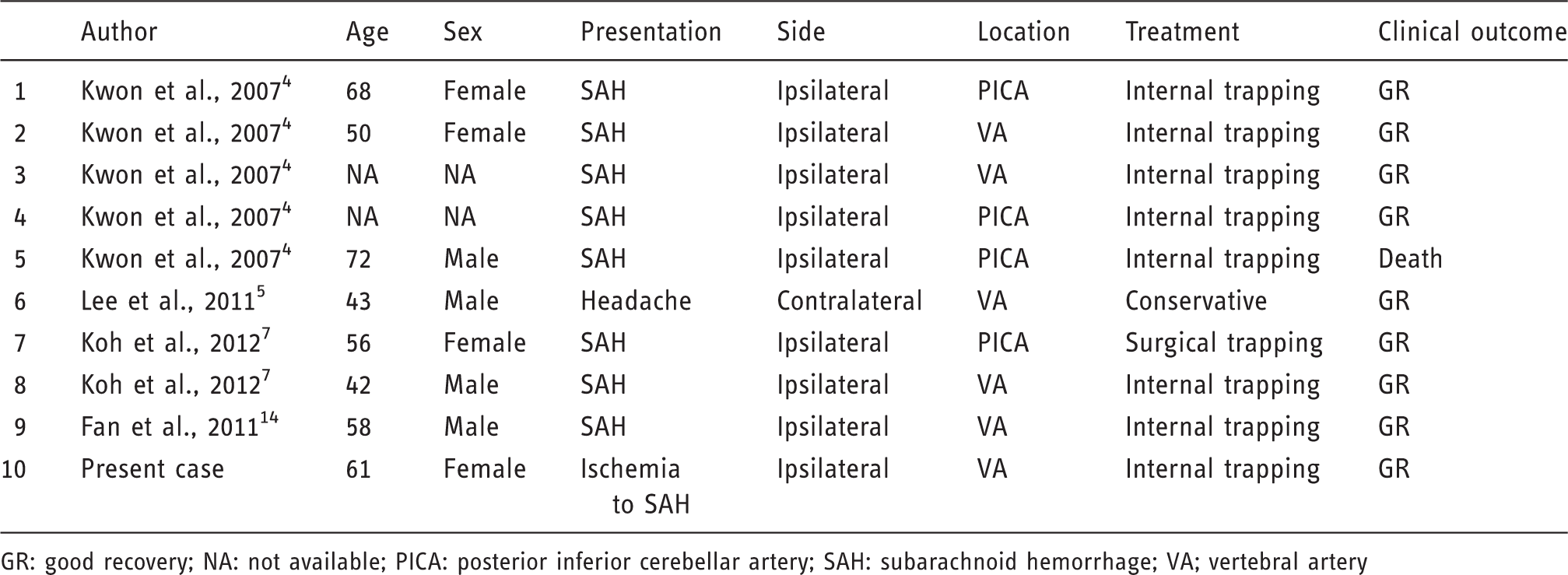
GR: good recovery; NA: not available; PICA: posterior inferior cerebellar artery; SAH: subarachnoid hemorrhage; VA; vertebral artery
The clinical course and prognosis of VADA are variable: it may present as a ruptured form, causing SAH, or as an unruptured form associated with ischemia or local symptoms. In the ruptured case, early surgical intervention is critical because of a high incidence of rebleeding and poor prognosis after rebleeding.15–18 By contrast, the management of symptomatic intracranial unruptured (siu) VADA remains controversial. On one hand, the rate of recurrent ischemic attacks is low,8,10 although several cases of siu VADA causing subsequent SAH have been reported.19–24 To our knowledge, this is the first report of a patient with VADA associated with DOPICA who originally had ischemia and subsequently suffered from SAH. In fact, the rate of subsequent SAH of siu VADA in the Japanese population is as high as 3.4%, 25 although that of non-Japanese populations was quite low. 10 Naito et al. suggested endovascular treatment for patients with VADA with relatively large or growing aneurysmal dilatations, and described the difficulty of predicting subsequent SAH in patients with siu VADA by angiographic findings. 19
The major advance of endovascular treatment with coils has made the treatment of VADA safer and easier, even in the acute phase of SAH.26,27 Endovascular techniques of VADA can be divided into deconstructive and reconstructive. 28 A deconstructive procedure can be safely performed if vital arterial branches are not involved in the segment of the vessel to be treated. However, the dissected segment cannot be occluded in patients with VADA involving PICA. That is why the treatment of VADA in them remains difficult, with a reported procedure-related morbidity of 16.7%. 29 Reconstructive procedures should be performed using stent placement including stent-assisted coiling and flow diverter stent, when we have to preserve the parent artery. The risk of bleeding with conservative management and the risk of ischemic complications associated with endovascular treatment using deconstructive or reconstructive techniques should be carefully considered in determining the indications of VADA in each case. As far as we know, all patients who had ipsilateral vertebral artery/PICA dissecting aneurysms associated with DOPICA on the ipsilateral side eventually had SAH. It is possible that this reflects a publication bias, as DOPICA can be overlooked in unruptured VADA; cerebral angiography is not routinely performed in unruptured cases. However, the risk of ischemic complications in the treatment of VADA associated with DOPICA can be reduced by preserving the extracranially originating PICA. Accordingly, early endovascular internal trapping should be considered when the risk of subsequent hemorrhage cannot be ignored for a long lesion, such as that in our case, in the management of intracranial vertebral artery or PICA dissecting aneurysms.
Conclusion
DOPICA is a relatively rare anomaly and may present a risk factor for subsequent aneurysm development and rupture. Early endovascular intervention should be considered even in the treatment of unruptured intracranial DAVA associated with DOPICA, when it can be performed safely.
Footnotes
Acknowledgement
The patient has consented to submission of this case report to the journal.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.