
Abstract
Introduction
The endovascular coiling of small ruptured aneurysms with difficult geometries presents a significant treatment challenge. We report our initial experience and the technical details of dual microcatheter coil embolizations that were applied in these difficult lesions.
Method and results
Eighty-five small aneurysms (<7 mm) that exhibited difficult configurations, such as a wide neck or an important branch vessel arising from the fundus, were successfully treated using a dual microcatheter technique. The packing attenuation, adverse events during the procedures, and angiographic occlusions from 21 very small aneurysm (≤3 mm) were recorded and compared with our coiling results of 64 small aneurysms (>3 mm, <7 mm). There were no significant differences in intraprocedural ruptures or procedure-related thromboembolisms between the two groups. At the last post-procedure clinical follow-up, a good clinical outcome (an modified Rankin Scale (mRS) of 0–2) was observed in 18 of the patients (85.7%). The recanalization rates at follow-up were significantly lower in the very small aneurysm group compared to the small aneurysm group (p < 0.05) and the mean packing density in the very small aneurysm group was significantly higher compared to the small aneurysm group (35.2% vs 24.8%, p < 0.05).
Conclusion
The dual technique was feasible, safe, and effective for coil embolization of aneurysms with difficult configurations and, in particular, it provided an alternative option for treating very small aneurysms.
Introduction
The endovascular treatment of aneurysms with unfavorable configurations, such as a wide neck and major branches incorporated within the aneurysm’s fundus, continues to be technically challenging because of the difficulty of stabilizing the microcatheter tips in these aneurysms to achieve a stable coil frame.
For several years, the dual microcatheter technique has been reported for the coil embolization of cerebral aneurysms with complicated configurations to create a stable coil frame using two coils to brace each other. 1 To the best of our knowledge, using the dual microcatheter technique in the treatment of small aneurysms, especially for very small aneurysms (diameter ≤ 3 mm), has not been reported widely. We present here our early experience with using double microcatheters in the treatment of small and very small aneurysms with difficult configurations.
Materials and methods
Patients and aneurysms
Endovascular treatment of 21 ruptured tiny aneurysms.
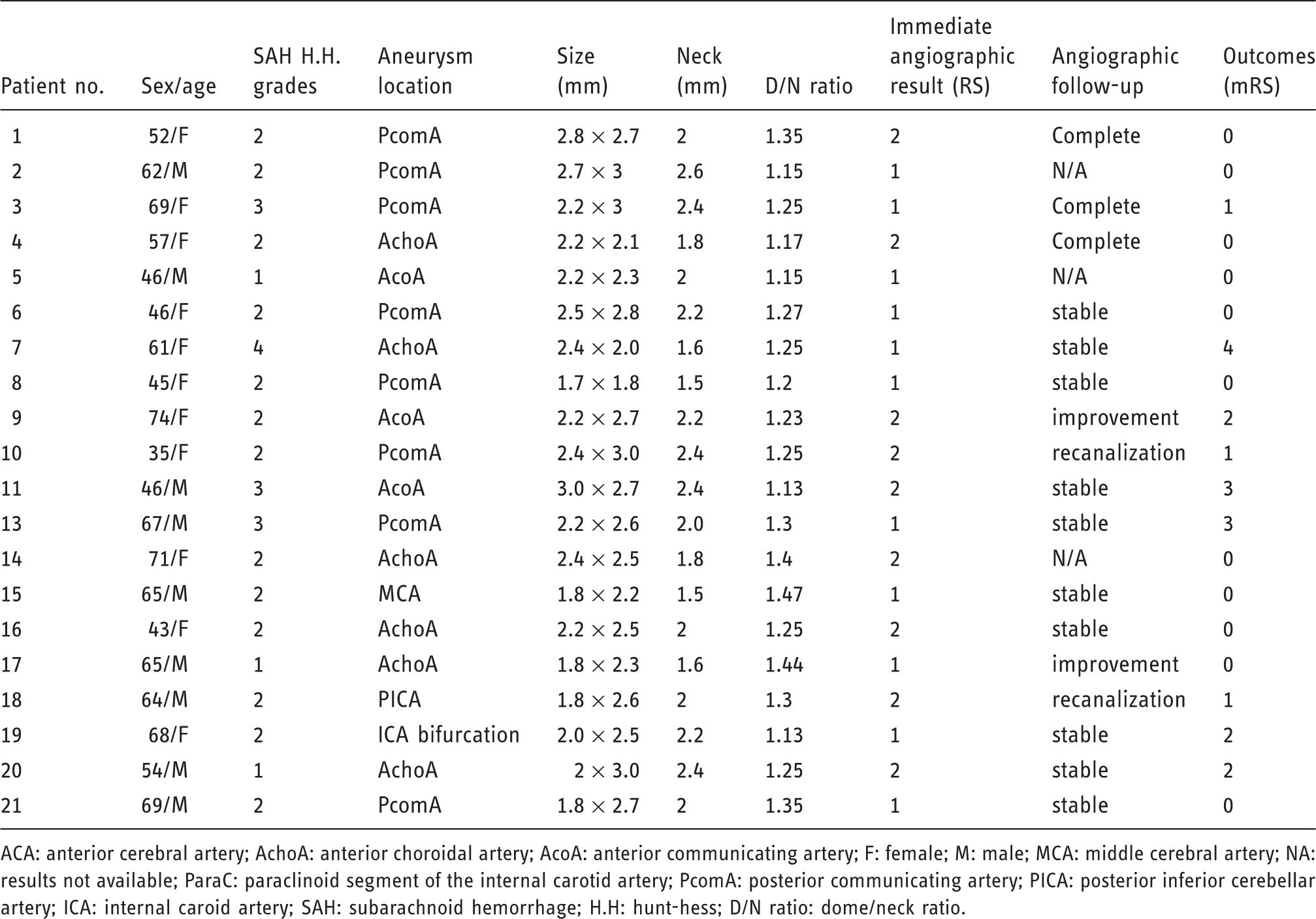
ACA: anterior cerebral artery; AchoA: anterior choroidal artery; AcoA: anterior communicating artery; F: female; M: male; MCA: middle cerebral artery; NA: results not available; ParaC: paraclinoid segment of the internal carotid artery; PcomA: posterior communicating artery; PICA: posterior inferior cerebellar artery; ICA: internal caroid artery; SAH: subarachnoid hemorrhage; H.H: hunt-hess; D/N ratio: dome/neck ratio.
The aneurysm volume was calculated by assuming that aneurysms are ellipsoid according to the following equation:
2

The coil volume was calculated according to the cylinder volume formula:

The information on the coil was provided in the manufacturer’s specifications. The packing attenuation was calculated as the ratio of the coil volume to the aneurysm volume.
Techniques
All of the cases were judged to be suitable for an endovascular coil embolization by the consensus of the neurosurgeons and neurointerventionalists, or involved patients who refused surgery. The strategies for the implementation of the double catheter technique were the following:
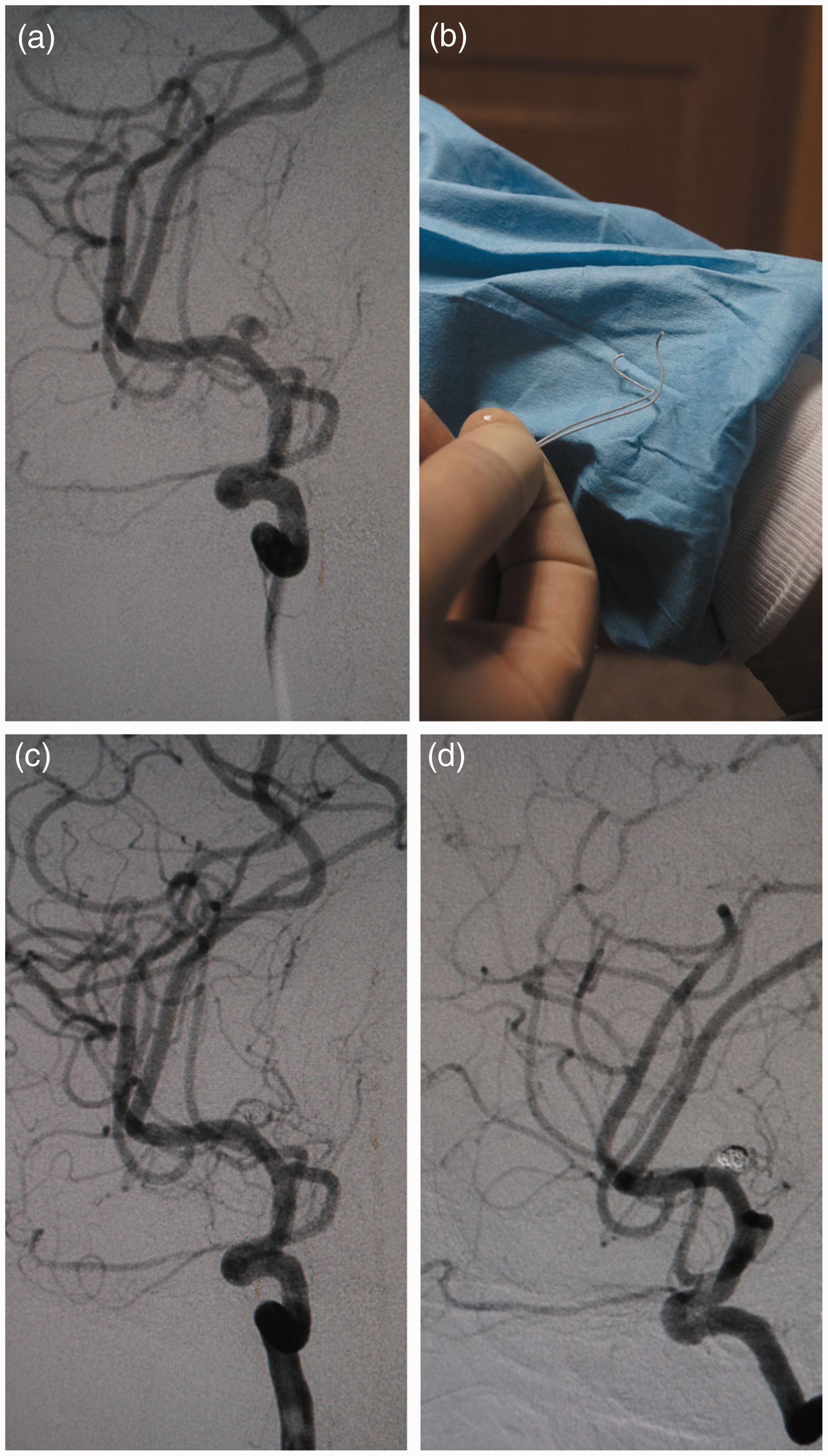
One microcatheter was used at first in an attempt to advance the microcatheter, but either a stable coil mass could not be formed or the microcatheter was displaced, after which the second microcatheter had to be advanced. The microcatheter was implanted into the appropriate location in the dome, and then another microcatheter was implanted into the distal branch of the parent artery. If under the aegis of the microcatheter positioned in the parent vessel the coil could not successfully constitute the basket, then the microcatheter was retracted and implanted into the sac of the aneurysm. The two microcatheters were designed to adapt to a wide-necked configuration or to protect an important branch vessel (Figure 1).
A 65-year-old male patient with a middle cerebral artery aneurysm: (a) DSA revealed a very small aneurysm incorporating a branch artery; (b) two microcatheters were used, the tip portion of two microcatheters after steaming showed a “S” shape; (c) after the insertion of the final coil, digital substract angiography (DSA) revealed complete occlusion with the patency of the branch artery; (d) a follow-up angiogram obtained 12 months post-treatment demonstrated stable occlusion.
The endovascular procedures were performed under general anesthesia on a commercially available monoplane angiography unit using a common femoral approach. During the coiling of the aneurysms, 3000 U of heparin was administered intravenously before the insertion of the microcatheter; subsequently, 1000 U/h. Standard frontal and lateral projections, working projections, and 3D-RA were performed to assess the characteristics of the aneurysm. The height and width of the aneurysm’s dome and the size of the aneurysm’s neck were measured from the various 3D imaging views to determine if it was possible for the coil to be deployed as a stable basket. A hemostatic valve with three ports was connected to the guiding catheter (6 F) that had been prepared to contain one of the two microcatheters. The guiding catheter was positioned in the desired location. After the first microcatheter was positioned, an extremely soft bare platinum coil (Hypersoft helical coil, MicroVention, Inc., Aliso Viejo, California, USA) or a 3D coil (Axium3D, Covidien, Mansfield, Massachusetts, USA) was first attempted to be embedded into the aneurysm to form a relatively stable frame. The inserted coil was not detached temporarily. The second microcatheter was advanced, and then the second coil, which usually had a smaller size or was a morphological variant, was inserted. Subsequently, the two coils were enlaced and mutually supported each other to constitute a frame basket. If the result of framing was unsatisfactory, one of the two coils or both of the coils could be retrieved and re-inserted separately. After a stable frame was acquired, one of the two coils was detached, and the next coil was advanced. This process was continued alternately until the aneurysms were coiled as densely as possible and it was not possible to deploy any more coils.
Clinical and angiographic follow-up
The clinical outcomes at the last follow-ups were reviewed by two independent neurologists using a modified Rankin Scale (mRS) score. The angiographic occlusion at the end of the procedure was classified using a three-point Raymond score (RS) as follows: RS 1 was considered to be the complete obliteration of the sac and neck of the aneurysm, RS 2 was defined by a lack of contrast filling in the aneurysm sac but the presence of contrast filling in the neck remnant, and RS 3 was defined by the contrast filling of the sac. 3 The angiographic follow-up results were evaluated by the RS as described above. Any increase in the contrast filling compared with the previous angiographic results was considered to indicate recanalization.
Comparison with data of small aneurysms (>3 mm, <7 mm)
The D/N ratio, procedural aneurysm perforations, packing density, recanalization and retreatment rates were compared with very small aneurysms (≤3 mm). Categorical data between the groups were compared using a contingency table. Continuous data were statistically analyzed using the unpaired t-test for normally distributed variables and using the Mann–Whitney U-test for non-normally distributed variables. Values of p < 0.05 were considered statistically significant. SPSS software (version 13; SPSS Inc., Chicago, Illinois, USA) was used to perform the analysis.
Results
Outcomes data for very small aneurysms treated with the dual catheter technique
Technical success was defined as the desirable positioning of the two microcatheters and a stable basket established by two coils. All of the treatments were successfully completed in 21 very small aneurysms. There were no perforated aneurysms or procedure-related thromboembolisms in this series. Only one patient harboring a tiny AcoA aneurysm experienced a coil loop prolapse. Loop herniation was observed in the end of the final coil but did not affect the patency of the anterior cerebral artery and thus did not result in a thromboembolism in the parent artery.
The mean packing density was 35.2%, and the range was 24.6–41.2%. The immediate angiographic outcome was assessed by the authors based on the RS. An RS 1 was achieved in 12 of the aneurysms (57.1%) and an RS 2 was achieved in nine of the aneurysms (42.9%); an RS 3 was not achieved in this study.
All of the patients survived the hospital admission period. Seventeen (81.0%) of the patients experienced good outcomes (mRS 0–2) at the time of discharge. At the last post-procedure clinical follow-up, a good clinical outcome was observed in 18 of the patients (85.7%). There was no rebleeding observed during the follow-up period. An angiography follow-up was performed in 18 of 21 patients within 10–18 months after the procedure. Two case exhibited angiographic improvement, 14 cases exhibited stable occlusions (Figure 1), and two cases exhibited recanalization. The recanalization resulted from the slight compression of the coil, and it was not necessary to retreat these patients due to very little residual intra-aneurysmal flow.
Comparison with the small aneurysms data (>3 mm, <7 mm)
Comparison of demographic characteristics and results of coil embolization in both small and very small aneurysms group.
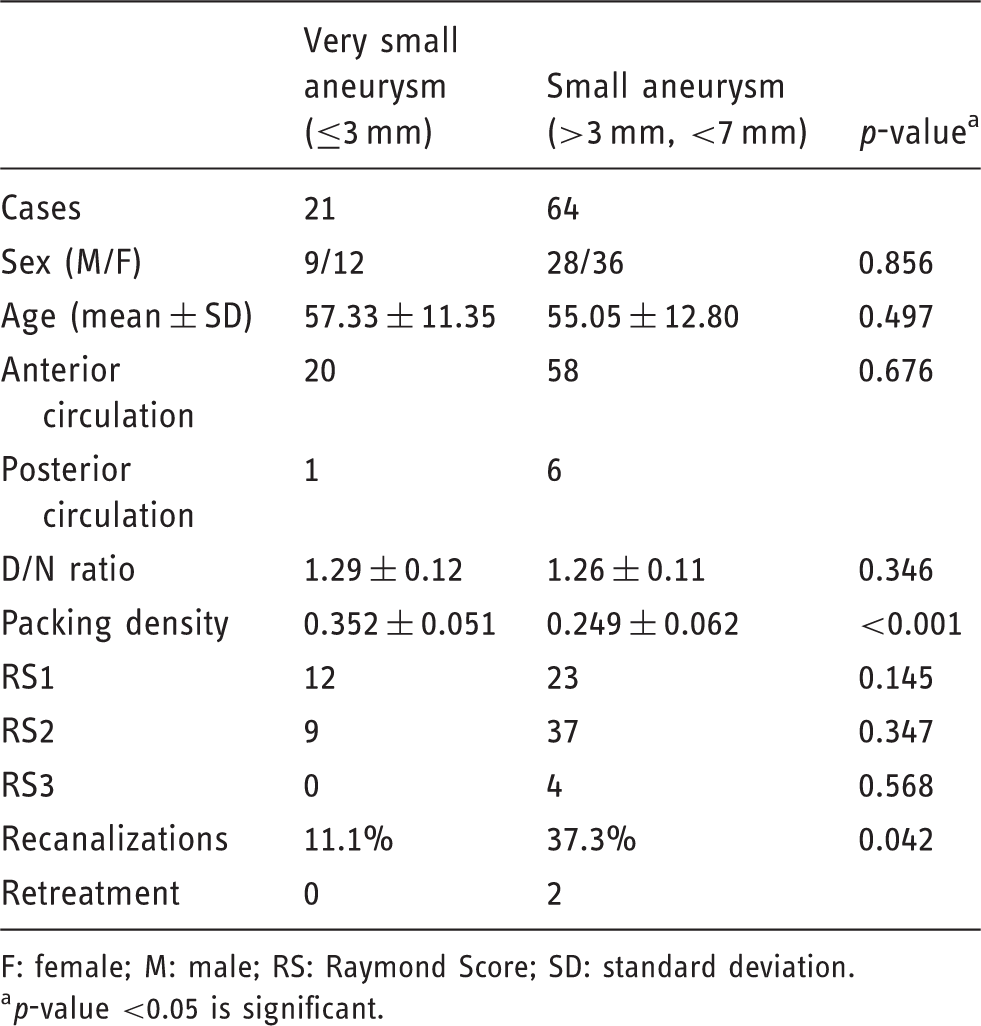
F: female; M: male; RS: Raymond Score; SD: standard deviation.
p-value <0.05 is significant.
Loop herniation was observed in four cases. In three cases with an aneurysm (>3 mm, <7 mm), a stent was deployed during the procedure as a “rescue measure.” The thromboembolism in the parent artery was observed in two cases. Aneurysm perforation occurred in two cases in the aneurysms (>3 mm, <7 mm) group.
The mean packing density in the very small aneurysm group (35.2%) was significantly higher than that in the small aneurysm group (24.8%).
There was no significant difference in the clinical outcomes between the very small aneurysm group and the small aneurysm group. Clinical follow-up was available for 60 of 64 patients and ranged from eight to 17 months in the small aneurysm group. Fifty-six of 64 patients had an mRS of 0–2.
In the small aneurysm group, immediate angiographic results revealed that the rates of complete obliteration (RS1), neck remnant (RS2), and residual aneurysm (RS1) were 12.5% (23 of 64), 62.5% (37 of 64), and 25.0% (four of 64), respectively. The initial complete occlusion rates were slightly higher in the very small aneurysm groups than in the small aneurysm groups, but this difference was not statistically significant.
An angiography follow-up was available in 59 cases, 25 of which exhibited angiographic recanalization. Recanalization rates at follow-up were significantly greater in the small aneurysm group than in the very small aneurysm group (42.3%, χ2 = 4.144, p = 0.042) (Table 2, Figure 2) Retreatment was performed in two aneurysms that exhibited recanalization in the small aneurysm group.
A 54-year-old male patient with a ruptured anterior communicating aneurysm; (a) angiography revealing a small wide-necked anterior communicating aneurysm (3.5 × 4.1 mm); (b) two microcatheters were positioned into the appropriate location of the aneurysmal dome and a more stable coil configuration was achieved with the addition of a second coil advanced alternately with the first coil; (c) the postembolization angiogram demonstrated complete occlusion; (d) follow-up angiogram (11 months) demonstrated significant recanalization of the aneurysm. The aneurysm was not retreated.
Discussion
Despite advances in both devices and techniques, many small aneurysms are treated by coiling embolizations. 4 However, it is still considered to be very challenging to treat these lesions with wide necks or important branch vessels originating from the fundus, particularly for tiny aneurysms. Although the adjunctive stent technique may be considered an alternative for complex aneurysms, the structural features of conventional stents, such as their available sizes, unfavorable flexibility and high porosity, may not be optimal for facilitating the embolization of tiny aneurysms. 5 Since Baxter et al. reported a double microcatheter technique used to treat wide-necked aneurysms in 1998, 6 a few studies have revealed better results for the technique.7,8
The major advantage of the dual microcatheter technique is that the coil does not have to be detached, thereby allowing subsequent coiling through another microcatheter to achieve a stable coil frame. Previous studies demonstrated that a major limitation of the endovascular treatment of tiny aneurysms is the high likelihood of intraoperative rupture. In our series, there were no procedural ruptures in the very small aneurysms and no significant difference in the procedural ruptures between the very small aneurysms and the small aneurysms. The following technical factor is closely associated with the successful application of the dual microcatheter technique.
First, a steady guiding catheter is vitally important for a successful embolization. To achieve optimal control of the microcatheters, the steady guidance of the catheter at as great a distant is necessary for the sufficient sustenance of the devices, especially in the tortuous supra-aortic vessel system. In some cases, a 90.0 cm 6-Fr long introducer accommodating the 6F catheter was advanced to improve the microcatheter’s stability. Sceond, precise shaping of the two microcatheters' tips that conforms to the aneurysm’s configuration was a key factor in safely accomplishing the embolization of the tiny aneurysms, Good shaping can reduce the resistance of the microcatheter during its navigation and reduce the risk of intraprocedural rupture.
Finally, the coil itself also plays a key role in stable framing and good packing. In this series, a very bare platinum coil was preferred as the framing coil in most cases, although this coil has been routinely used as a filling or final coil. The soft coil was initially designed to improve the handling properties and reduce the risk of aneurysm ruptures. 9
Although the dual microcatheter technique had been proven safe and effective, a previous study reported that the major limitation of the dual microcatheter technique is decreased packing density and increased recurrence rate. In the present study, we retrospectively compared the very small aneurysms group (≤3 mm) to the small aneurysms group (>3 mm, <7 mm), both of which were treated with the dual microcatheters technique. Recanalization rates in the very small aneurysms were lower relative to both the small aneurysms group and the previous historical series about dual microcatheters technique. 7
There are several reasons that may explain the low recanalization rates. First, in the current study, we achieved a desirable packing rate that was higher than the optimal value (20–33%).10,11 The packing rate in very small aneurysms treated with dual microcatheters was higher than that in the small aneurysms.
Given the high risk of intraprocedural ruptures of tiny aneurysms, the loose packing of one or two undersized coils is often used during the coiling of tiny aneurysms. 12 Although several studies have reported aneurysms with incomplete occlusions, the immediate angiography did not reveal increased recanalization in the angiographic follow-up, 13 the packing density was considered to be the most important factor related to changes in the intra-aneurysmal hemodynamics and decreases in the likelihood of recanalization. 14 The optimal packing in this study was related to a number of factors. First, based on the calculation formula of packing density, the size of the aneurysms is inversely proportional to the packing density. The smaller volume of the tiny aneurysm was closely related to the high packing density. Second, for the construction of the stable coil mass, the microcatheter, undetached coil itself, or both can serve as a mechanical scaffold for temporarily protecting the coils from protruding into the important branch vessel. This protective role may also be more important in tiny aneurysms because the microcatheter covers a higher proportion of the space around the neck than it dose in a larger one. Third, the very soft and small bare platinum coil used in this study possibly packed more of the small dead space and attained a more desirable distribution. The results are consistent with the experimental results in which the use of smaller and softer coils led to more complete filling of the aneurysm sac in the silicon aneurysm model. 15
Except for the packing density, the same coil possibly caused more significant hemodynamic changes compared with the larger aneurysms. Indeed, several studies have reported that tiny aneurysms with incomplete occlusions in the immediate angiography progressed to complete occlusion in the angiographic follow-up. 16
There was a low risk of procedure-related complications in the current study. In the very small aneurysm group, we encountered the twisted locking of the two microcatheters in only one case. This problem was finally resolved by retrieving both of the coils and the microcatheters and advancing the devices once more. However, the potential risks of an intraprocedural rupture, thromboembolic complications, coil stretching, or other complications were not negligible. The selection of the cases and the manipulation of the endovascular devices in the operation remained cautious in this small series.
Conclusion
In conclusion, most aneurysms were successfully and safely treated by a dual microcatheter technique in the present study. There was no increased periprocedural event rates and there were lower recanalization rates in the very small aneurysms compared with the small aneurysms in our study. The dual microcatheter technique should be considered as an alternative option in very small aneuyrysms.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.