
Abstract
Background
Segmental arterial mediolysis (SAM) is an uncommon or underdiagnosed arteriopathy that presents with life-threatening hemorrhage. SAM can affect the intracranial, spinal, and visceral arteries, with reported cases of concomitant intracranial and visceral hemorrhage.
Case description
We present the case of a 61-year-old male with concurrent subarachnoid and intraperitoneal hemorrhage caused by simultaneously bleeding posterior spinal artery and splenic artery pseudoaneurysms. The posterior spinal artery pseudoaneurysms were treated with selective injection of polyvinyl alcohol particles into the posterior spinal artery, while the splenic artery pseudoaneurysm was treated with Gelfoam embolization. The constellation of imaging, clinical, and laboratory features led to a presumptive diagnosis of SAM, which remains the only reported cause of concurrent neurovascular and visceral artery aneurysm rupture.
Conclusion
SAM is a key diagnostic consideration in cases of concomitant intracranial, spinal, and visceral artery aneurysm rupture.
Keywords
Introduction
Segmental arterial mediolysis (SAM) is an uncommon arteriopathy characterized by life-threatening hemorrhage in the abdominal cavity, retroperitoneum, and skull base. 1 First described in 1976, SAM results in non-inflammatory lysis of the arterial media, with resultant arterial instability and risk for hemorrhagic sequelae or aneurysm formation.2,3 Recently, SAM has been reported as a rare cause of concomitant intracranial and visceral artery aneurysm rupture.
Case report
A 61-year-old Caucasian male with a past medical history of Reiter’s syndrome, obstructive sleep apnea, nicotine abuse, and alcohol abuse presented to the Emergency Department (ED) for evaluation of acute-on-chronic neck pain, lower extremity pain and weakness, and confusion. The patient became acutely agitated in the ED, with worsening mentation. Noncontrast head computed tomography (CT) was performed, which demonstrated acute extra-axial blood products about the caudal brainstem and visualized cervical spine (Figure 1(a)). The patient was emergently transferred to the medical intensive care unit with onset of hypotension and tachycardia. He was intubated for airway protection, and a central line was placed. Neurological and neurosurgical consultations were obtained.
Initial imaging evaluation. (a) Noncontrast head computed tomography (CT) at the time of initial evaluation demonstrates subarachnoid hemorrhage in the upper cervical spine. (b) T1-weighted sagittal magnetic resonance imaging of the lumbar spine demonstrates intermediate to high signal of the cerebrospinal fluid consistent with spinal subarachnoid hemorrhage as well. (c) CT of the abdomen and pelvis with intravenous contrast demonstrates pseudoaneurysms of the short gastric artery (arrow) and a large amount of intraperitoneal blood surrounding the spleen.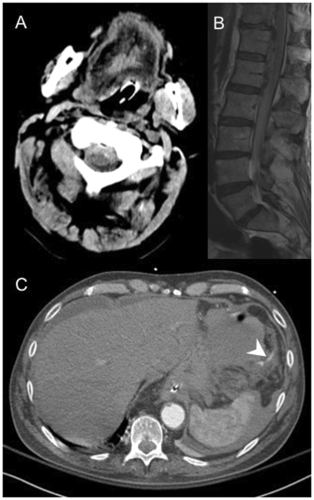
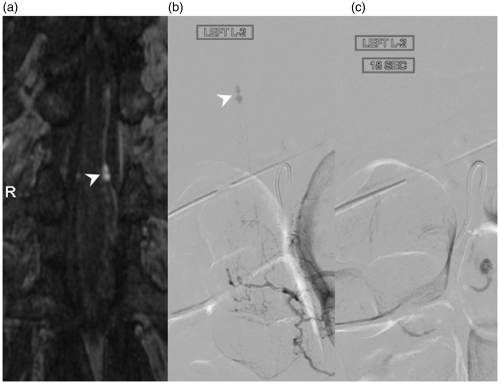
CT angiography of the head and neck was negative for aneurysm or dissection. Magnetic resonance imaging of the spinal column revealed subarachnoid and subdural blood products throughout the cervical, thoracic, and lumbar spine (Figure 1(b)), with multiple posterior spinal artery aneurysms. Catheter angiography was recommended for further evaluation. Immediately prior to the spinal angiogram, the patient experienced a continued hemoglobin drop. An emergent CT angiogram of the abdomen and pelvis was performed, which demonstrated blood products throughout the abdomen and pelvis, with active extravasation from a splenic artery pseudoaneurysm, and the patient was triaged to vascular interventional radiology for an urgent catheter angiogram (Figure 1(c)). Splenic artery angiogram demonstrated active extravasation from multiple splenic artery pseudoaneurysms, which were successfully treated with Gelfoam embolization (Figure 2). Following stabilization of his hemoglobin, the patient was brought to spinal angiography the next day. Spinal angiography demonstrated a pseudoaneurysm arising from the posterior spinal artery at the level of L2 which was successful embolized with PVA particles (150 µm; Figure 3). Cerebral angiography was negative for an intracranial source of hemorrhage.
Splenic angiogram. (a) Preoperative splenic angiogram demonstrates multiple pseudoaneurysms arising from branches of the splenic artery, as well as active extravasation. (b) Post-embolization splenic angiogram demonstrates complete cessation of active extravasation, with multiple wedge-shaped perfusion defects in the spleen. Posterior spinal artery aneurysms. (a) Gadolinium bolus spinal magnetic resonance angiography demonstrates focal aneurysmal dilatation of the radicular segment of the posterior spinal artery. (b) Selective injection of the left L2 lumbar artery demonstrates two focal spinal pseudoaneurysms of the radicular segment of the posterior spinal artery. (c) Following selective injection of PVA particles into the posterior spinal artery, the posterior spinal artery pseudoaneurysms no longer fill.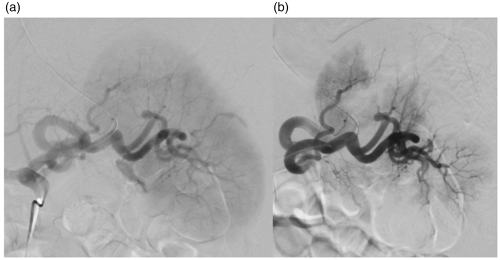
Extensive laboratory analysis was undertaken with negative myeloperoxidase, proteinase-3, anti-cyclic citrullinated peptide, and immunoglobulin G phospholipid antibodies. Erythrocyte sedimentation rate and C-reactive protein were mildly elevated. Anti-nuclear antibody was negative. Repeat visceral angiography performed four months later demonstrated no evidence of vasculitis. Repeat spinal angiography two months later demonstrated complete occlusion of the previously treated spinal pseudoaneurysms. Ten months following presentation, the patient made a complete neurological recovery. He has had no recurrent hemorrhage.
After extensive workup, differential considerations included vasculitis, SAM, and underlying infection. Review of the patients imaging and laboratory analysis was unrevealing for a vasculitic or infectious etiology. SAM remains the presumptive diagnosis, as it is the only reported cause of hemorrhage from intra-abdominal and neurovascular aneurysms.
Discussion
SAM is an uncommon and underdiagnosed vascular disease with substantial acute-phase mortality. 1 The pathogenesis of SAM is not well delineated, but prior studies have suggested that it is a noninflammatory and nonatherosclerotic arteriopathy. 3 Pathological analysis of vascular beds affected by SAM demonstrate vacuolization and lysis of the outer arterial media, smooth-muscle degeneration, and serration of the internal elastic lamina. These changes result in focal gaps in the arterial wall, causing dissecting pseudoaneurysms. There is currently some debate as to whether SAM is a systemic or non-systemic disease. However, given the fact that a number of cases have been reported to affect multiple vascular beds, many authors favor a systemic cause. 1
Due to significant overlap in imaging appearance with similar vasculopathies and subclinical presentation, diagnosis relies on careful imaging and laboratory and clinical correlation. The imaging findings of SAM include arterial dilation, single aneurysm, multiple aneurysms, intramural hematoma, arterial stenosis, and arterial occlusion.1,4 Celiac artery and branch-vessel involvement has been reported in 46–80% of cases.1,4,5 Superior mesenteric, inferior mesenteric, and renal arterial involvement is also common.1,4–9
There have been at least eight previously reported cases of SAM affecting both visceral and neurovascular beds.4–15 In all of the previously reported cases, hemorrhages of the neurovascular and visceral vasculature occurred within one week of each other, and in most cases surgical or endovascular management was required to stabilize the patient. Our case is unique in that it is the first reported case of SAM affecting the spinal vasculature and is one of the only cases in which endovascular interventions were performed for both visceral and neurovascular complications.
Ideal treatment strategies for managing posterior spinal arterial aneurysms are controversial. 16 The majority of published studies focus on surgical management of these lesions. However, there are several case reports examining the role of endovascular management. 17 Because the posterior spinal arteries are small and difficult to catheterize selectively with most microcatheters, the vast majority of lesions discussed in the literature were treated with proximal embolization alone. Proximal embolization techniques that have been reported include proximal coil embolization,17,18 PVA particle embolization, 16 and liquid embolization with glue or Onyx®. 19 One major disadvantage of PVA particle embolization or liquid embolic agent embolization is that it is difficult to control the flow of the embolic agent, so there is a potential risk of embolizing territories beyond the affected vessel. This is particularly true in the region of the conus where there are rich anastomoses between the posterior spinal arteries and anterior spinal artery. Coil embolization, while presumably safer, does not result in occlusion of the aneurysm itself, but rather the origin of the posterior spinal artery. Thus, there is always a risk of reconstitution of the aneurysm from rich posterior spinal arterial anastomoses. Ultimately, a review of the literature suggests that there is no defined endovascular treatment strategy for these lesions and that ideal treatment strategies should be considered on a case-by-case basis. In our case, embolization with particles was performed over coiling, as we sought to have some penetration of embolic material to the level of the pseudoaneurysm in order to prevent another devastating subarachnoid hemorrhage from aneurysm re-rupture/reconstitution. Particles were chosen over liquid embolic agents due to the fact that we felt uncomfortable embolizing the posterior spinal artery with our microcatheter in a wedged position, especially given that the posterior spinal artery was supplying the conus basket.
Because of the rarity of SAM, ideal management strategies have yet to be established. In the acute phase, supportive measures are needed to manage bleeding and neurological complications. Vascular imaging including computed tomography angiography, magnetic resonance angiography, and conventional angiography can be used to diagnose and monitor pseudoaneurysms associated with the disease. Both surgical and endovascular therapies can be considered for treatment of the visceral and neurovascular aneurysms and have had similar reported success rates. Long-term management strategies include blood-pressure management, smoking cessation, and continued imaging follow-up to evaluate for the presence of new lesions.
Conclusions
In conclusion, we present a unique case of SAM affecting both visceral and neurovascular beds. The splenic artery and posterior spinal artery pseudoaneurysms were both managed endovascularly, and the patient has made a complete recovery with no recurrent bleeding. SAM is a key diagnostic consideration in cases of concomitant intracranial, spinal, and visceral artery aneurysm rupture.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.