
Abstract
Radiation-associated vascular changes most commonly present in the form of stenosis, thrombosis and occlusion. However, development of intracranial aneurysms secondary to radiation is far less common and often manifests with rupture. These aneurysms are difficult to treat and associated with high morbidity and mortality when ruptured compared with saccular aneurysms unrelated to radiation treatment. Both surgical and endovascular options are available for treatment of these aneurysms. We present a young patient with a radiation-induced intracranial pseudoaneurysm arising from the lenticulostriate branch of the left middle cerebral artery (MCA); this developed 1 year 4 months after 59.4 Gy of focused radiation to the suprasellar pilomyxoid astrocytoma. The patient successfully underwent endovascular glue embolization of the aneurysm and occlusion of the lenticulostriate artery after unsuccessful trapping of the aneurysm and occlusion of the parent artery using coils. She developed transient hemiparesis of the right side following the procedure, which was managed conservatively. We performed a complete review of the literature dealing with the radiation-induced intracranial aneurysms, their presentation, treatment and outcome.
Introduction
High-dose ionizing radiation has been increasingly used as a standard and effective treatment regimen for not only brain tumors but also for cerebral arteriovenous malformations (AVMs). With overall advances in medical care and increased life expectancy, the long-term side effects of radiation have become a major concern. Cerebrovascular complications secondary to radiation therapy are infrequent; they may include cavernous malformations and vasculopathy with vessel stenosis, occlusion or thrombosis. 1 Radiation-induced intracranial aneurysms are extremely rare with only 72 aneurysms in 45 patients so far reported, including the present case. These aneurysms are difficult to treat and associated with high morbidity and mortality when ruptured compared with saccular aneurysms unrelated to radiation treatment.2–10
We present a pediatric case of incidentally detected pseudoaneurysm of lenticulostriate artery, likely induced by stereotactic irradiation for pilomyxoid astrocytoma of the optic pathway, which was effectively treated with endovascular glue embolization.
Case presentation
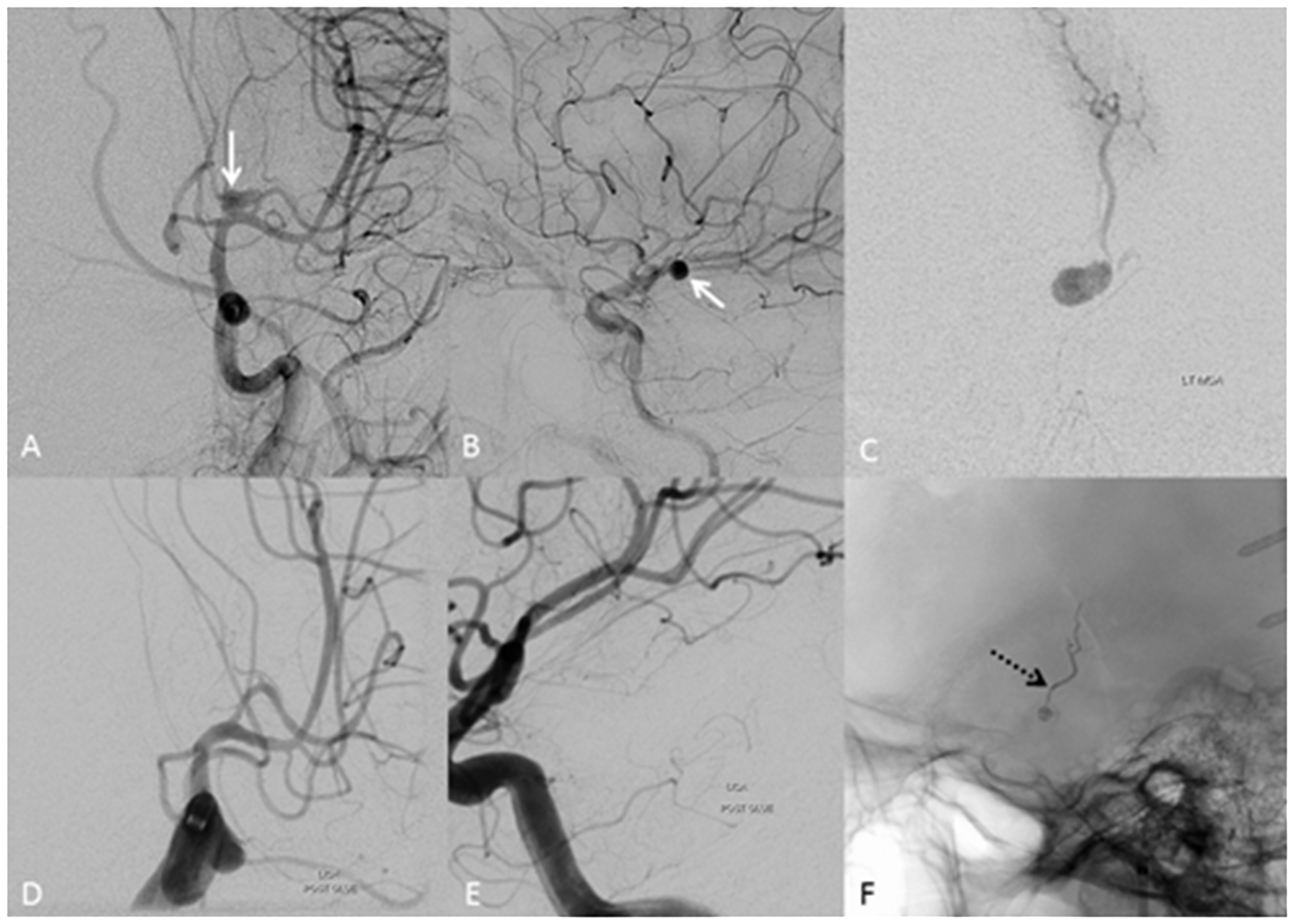
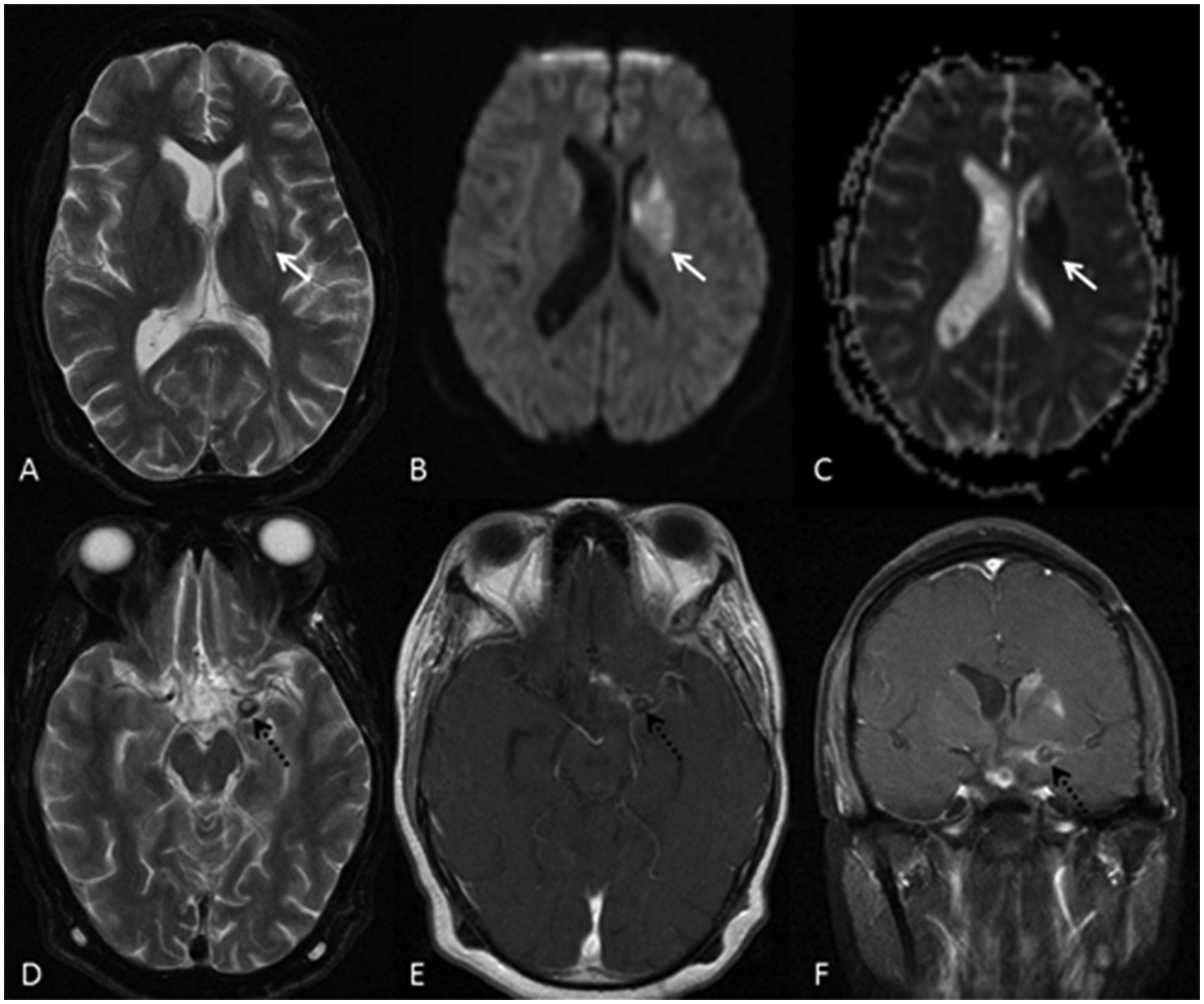
We present a young 14-year-old female who was diagnosed with a suprasellar mass involving the optic pathway 2 years ago while investigating for signs of increased intracranial pressure (ICP) and visual deterioration. She underwent ventriculoperitoneal shunt with partial resection and biopsy of the lesion 1 month after the diagnosis. The histopathological analysis of the tissue showed pilomyxoid astrocytoma of the optic pathway. She was initially prescribed two cycles of caroboplatin and vincristine as chemotherapy; however, her symptoms became worse. Subsequently, she received six cycles of volumetric-modulated arc therapy from December 2013 to February 2014 with a total dose of 59.4 Gy directed to the suprasellar lesion. She improved over time and the 1-year follow up MRI performed in January 2015 showed significant decrease in tumor size. A later follow up MRI performed in July 2015 showed further decrease in tumor size, with new sub-acute infarcts in the left basal ganglia and a suspected aneurysm from the superior M2 division of left middle cerebral artery (MCA) (Figure 1). The young age of the patient, the pseudo aneurysm morphology of the aneurysm and location of the aneurysm within the previously irradiated field suggested that this may represent a radiation-induced aneurysm. Cerebral infarction due to radiation-induced vasculopathy was diagnosed. Digital subtraction angiography was performed immediately, and this demonstrated a slow-filling 6 × 4 mm pseudo aneurysm from a lenticulostriate perforator arising from the superior M2 division of the left MCA (Figure 2). The case was extensively discussed in the multidisciplinary team meeting and the consensus favored endovascular embolization of the aneurysm, given the angiographic appearance and location in the pre-irradiated field. The aim of the endovascular procedure was to occlude the aneurysm as well as the parent artery using either glue or microcoils. However, we considered coiling instead of glue embolization given the very small stump proximal to the pseudoaneurysm and the risk of intraprocedural reflux of glue into the M2 division. Under general anesthesia and systemic heparinization (3000 units), a 6-F groin sheath was placed in the right femoral artery. A 6-F Envoy DA multipurpose guiding catheter (Codman Neuro, Raynham, MA, USA) was placed in the left internal carotid artery (ICA), and a Headway DUO microcatheter (MicroVention Inc, Tustin, CA, USA) was navigated coaxially over a Traxcess 014 microguidewire (MicroVention Inc, Tustin, CA, USA) and positioned in the superior M2 division of the left MCA. Superselective angiograms were performed, which re-demonstrated the pseduoaneurysm arising from the lenticulostriate perforator of the left MCA. An attempt was made to advance the microcatheter into the perforator to deploy coils in the short proximal stump for parent artery occlusion; however, it was not possible due to acute angulation at the origin. Subsequently, we decided to proceed with glue embolization. A Sonic 1.2-F microcatheter (BALT Extrusion, Montmorency, France) was successfully advanced over a Hybrid 007 microguidewire (BALT Extrusion, Montmorency, France) into the lenticulostriate perforator under roadmap guidance and positioned within the aneurysm. We used a mixture of one-third Histocryl (BIBraun, Ann Arbor, MI, USA) and two-thirds Lipidol (Guerbet LLC, Bloomington, IN, USA) for obliteration of the aneurysm. The glue mixture filled the aneurysm as well as the perforator distal to the aneurysm. A control angiogram following glue injection demonstrated complete occlusion of the pseudoaneurysm as well as the lenticulostriate perforator (Figure 2). Post procedure, she developed hemiparesis of the right side and mild confusion. MRI performed the next day after glue embolization showed a new infarct in the left putamen (Figure 3). The patient was managed conservatively and discharged 2 days after the procedure to a children’s hospital for further care. She has completely recovered from her neuro deficit as of our last follow up at 2 years.
(a) Axial FLAIR, (b) coronal T2W and (C) coronal post contrast T1W MRI images demonstrate the optic pathway glioma in the suprasellar region (dotted black arrow) and the left middle cerebral artery (MCA) aneurysm (white solid arrow). (d) 3D Time of Flight (TOF) axial source image. (e and f) TOF maximum intensity projections reveal the faintly visible small aneurysm from the left MCA. (a and b) Oblique projections of diagnostic cerebral angiogram show the small aneurysm from the superior division of the left MCA. (c) Superselective angiogram with contrast injection through the microcatheter reveals the pseudoaneurysm arising from a lenticulostriate branch of the left MCA. (d and e) Post glue embolization angiograms demonstrate no obvious residual aneurysm. (f) Fluro image of the head shows the glue cast in the aneurysm and the lenticulostriate artery. Post procedure follow up MRI. (a) Axial T2W, (b) axial diffusion weighted images and (c) axial apparent diffusion coefficient map MRI images of the brain show acute ischemic infarct in the left putamen (white arrow). (d) Axial T2W, (e) axial post contrast T1W and (f) coronal post contrast T1W MRI images of the brain demonstrate the thrombosed aneurysm.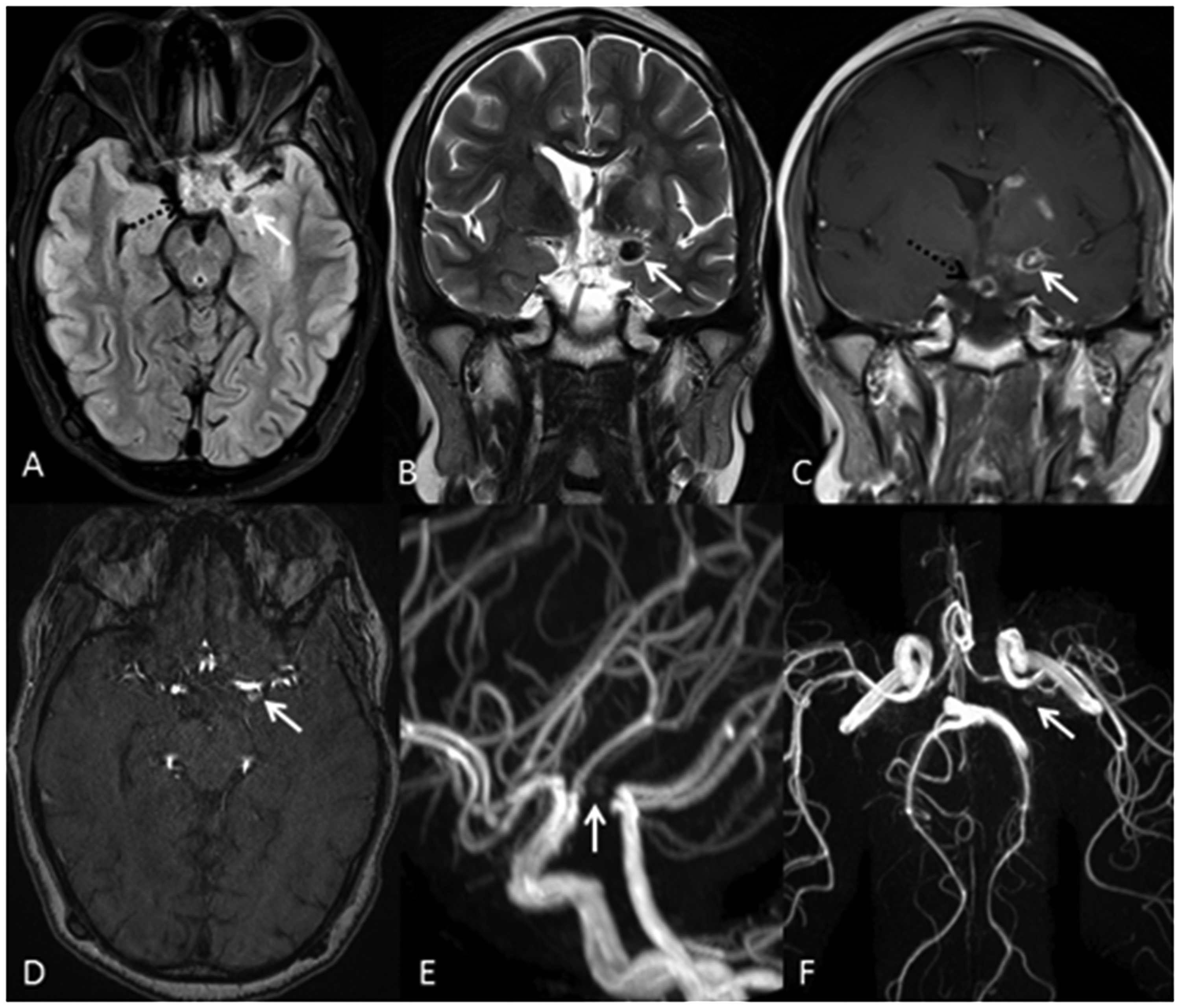
Discussion
Radiation-induced vasculopathy is well known and effects both small and large vessels within the field of treatment. 11 Multiple mechanisms have been implicated in the biological tissue injury, which include DNA damage, cellular apoptosis, deregulation of interactions between surviving cells, and hypoxia caused by vascular damage. Selective induction of inflammatory cascade has also been proposed, including the release of cytokines and growth factors necessary for tissue healing. 12 Thrombo-occlusion, stenosis and moya moya changes are the most common cerebrovascular manifestations after cranial radiation.9,11,13 The incidence of radiation-associated intracranial aneurysms is much rarer; however, the underlying pathogenesis appears to be identical. Histopathologically, a combination of findings can be noted in radiation-affected vessels such as fibrosis, necrosis and fibrin deposition in the vessel wall, accelerated atherosclerotic changes in the intima, inflammation and disruption of endothelial cell linings, likely contributing factors in aneurysm formation.3,9,10,13,14 The known histological alterations in the cerebrovasculature after radiation with constant shear stress of blood flow likely precipitate the formation of aneurysms and also increase the risk of rupture.1,4,7,15–17 The first reported case of radiation-induced aneurysm involving bilateral ICAs was in 1975 by Bole et al. 18
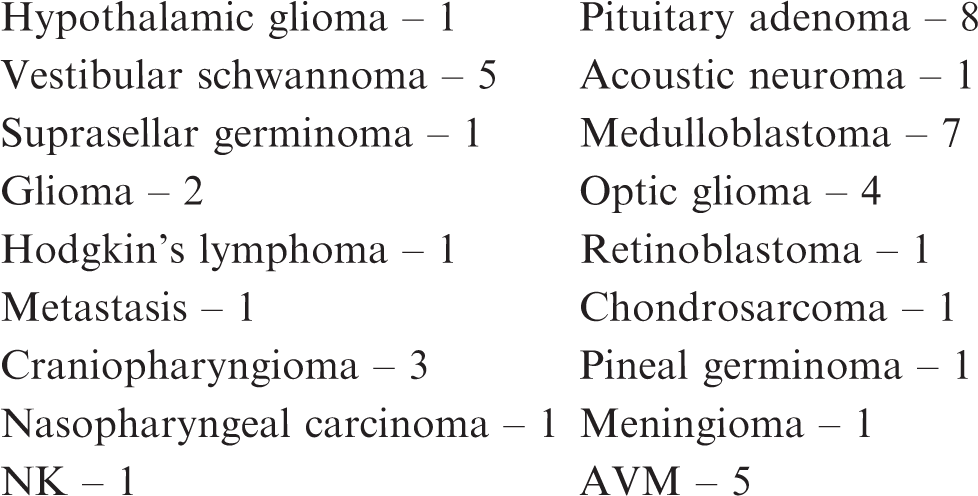
Reported literature on radiation-induced intracranial aneurysms.
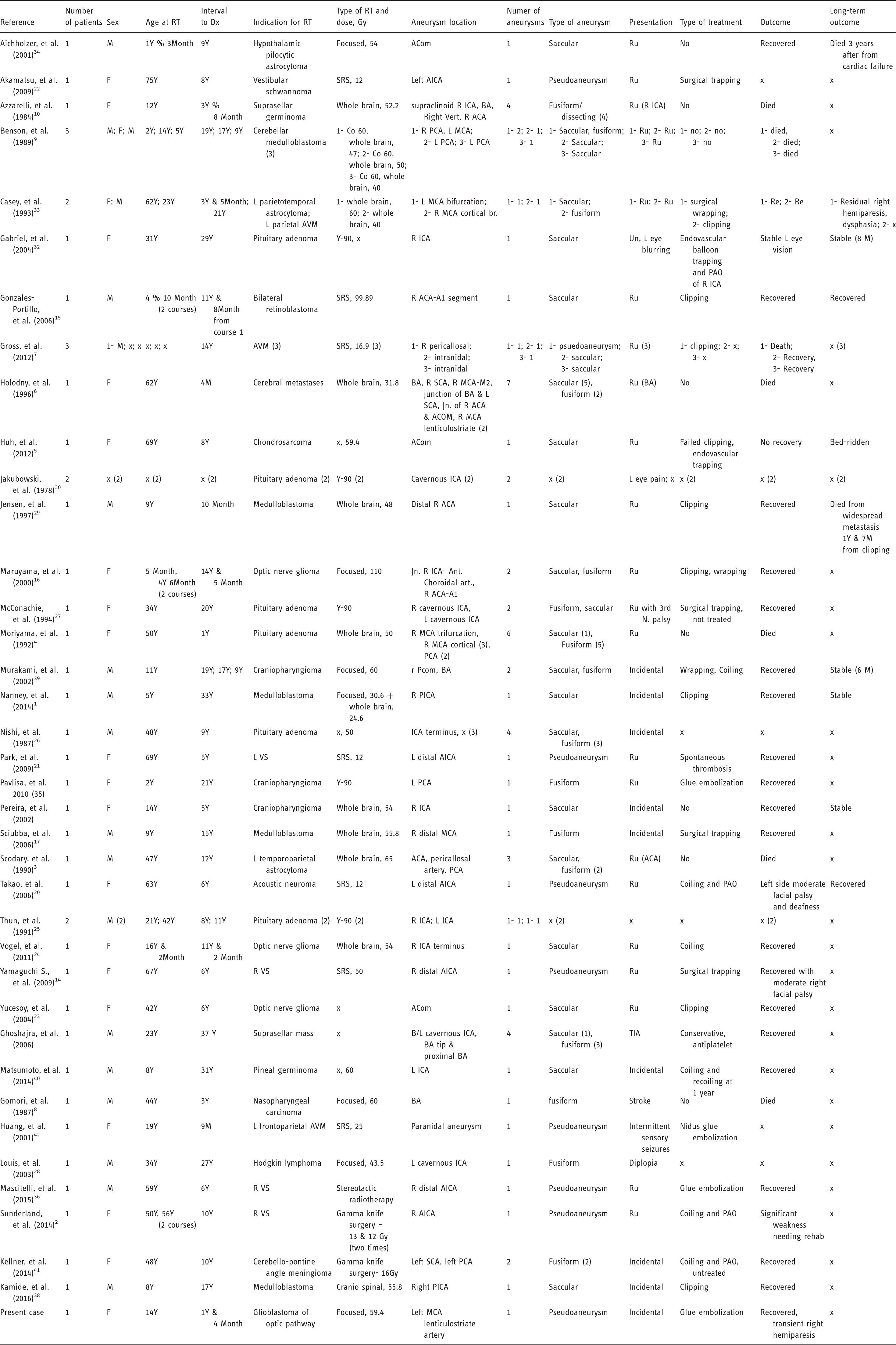
RT: radiotherapy; Dx: diagnosis; Gy: Gray, R: right; L: left; M: male; F: female; Y: year; x: Unknown; Y-90: yttrium-90; SRS: stereotactic radiosurgery; Ru: rupture, Un: unruptured; Re: recovered; BA: basilar artery; ACA: anterior cerebral artery; ICA: internal carotid artery; MCA: middle cerebral artery; PCA: posterior cerebral artery; AICA: anterior inferior cerebellar artery; SCA: superior cerebellar artery; PCom: posterior communicating artery; ACom: anterior communicating artery; PICA: posterior inferior cerebellar artery; AICA: anterior inferior cerebellar artery; AVM: arteriovenous malformation; TIA: transient ischemic attack; VS: vestibular schwannoma; PAO: parent artery occlusion.
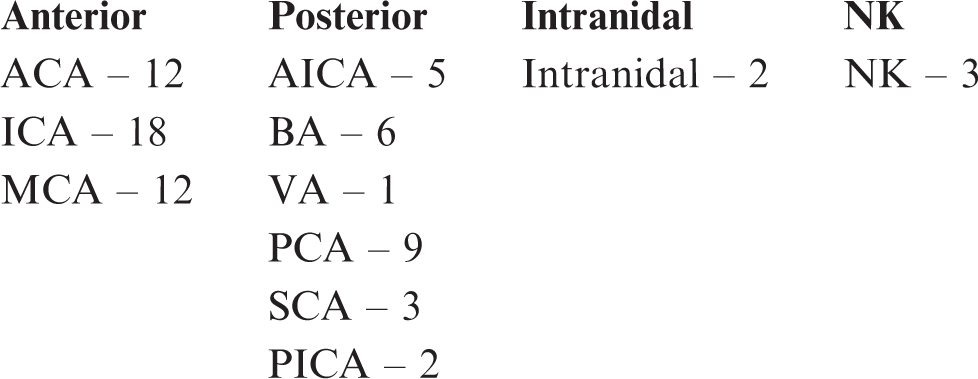
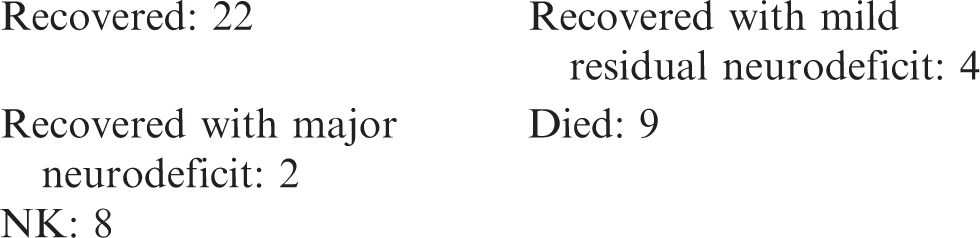
As per our review of the literature, the anterior circulation was the favored location, constituting 56% of radiation-induced aneurysms.3–6,9,10,15–17,23–34 With regards to morphology of the aneurysms, both saccular (40%) and fusiform (42%) aneurysms were almost equal in incidence, 11% were pseudoaneurysms and 7% were not defined in the literature. The majority of patients presented with rupture of these aneurysms and intracranial hemorrhage, constituting 58% of the total.2–7,9,10,14–16,20–24,27,29,33–36 Only 20% including the current case were incidental and were found during work up for other symptoms. The cause is still unclear; however, it could be a combined effect of multiple factors, such as radiation-induced vessel wall inflammatory changes leading to necrosis and fibrosis and tumor invasion of the vessel wall, making these aneurysms more biologically unstable. 1 According to the current review, the higher incidence of fusiform and pseudoaneurysms may also explain the increased risk of rupture and intracranial bleed. Various previous studies have reported very high mortality (42–67%) from rupture of radiation-induced aneurysms.14,15,29 However, in the present review the risk of morbidity (15%) and mortality (30%) from ruptured radiation-induced aneurysms is lower than the general population with aneurysmal subarachnoid hemorrhage. 37
Given the more unstable nature and higher risk of rupture, special attention should be given to appropriate management of intracranial aneurysms secondary to radiation treatment. 14 Once the diagnosis is made there should not be delay in treating these lesions. Various treatment options have been proposed in the literature. The treatment strategy should be planned based on various observations such as presence of pseudoaneurysms or dissecting aneurysms with the fragile nature of aneurysm wall needing parent artery occlusion. The underlying radiation vasculitis with stenotic vessels may further complicate the procedure. The lack of long-term outcome data of these aneurysms post treatment is also a worrying fact. Therefore, a watchful follow up is needed in long-term surviving patients to specifically look for recurrence of the treated aneurysm and de novo aneurysm formation.
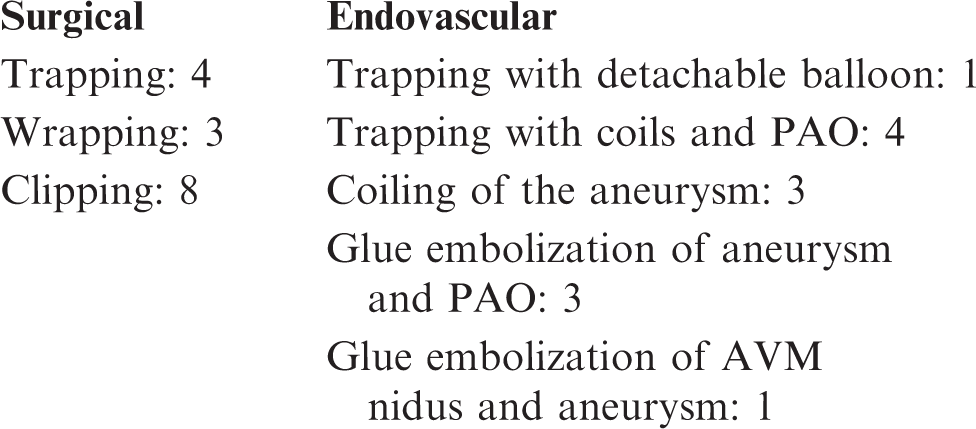
The ideal treatment of radiation-induced aneurysms remains debatable. The choice of treatment may include surgical as well as endovascular methods. The surgical options consist of direct microsurgical clipping and aneurysm trapping with or without bypass. Direct endovascular coiling, parent vessel occlusion with coils or liquid embolic agents or parent vessel remodeling with flow diversion strategies are the currently available endovascular options. Pseudoaneurysms and fusiform dissecting aneurysms need special attention due to the fragile aneurysmal wall and should be treated with surgical or endovascular trapping with or without bypass. So far, most radiation-induced aneurysms have been treated surgically; eight with clipping,1,7,15,16,23,29,33,38 four with trapping14,17,22,27 and three with wrapping.16,33,39 Endovascular treatment is useful in surgically inaccessible aneurysms. Twelve cases including the present case were treated with the endovascular approach: coiling of the aneurysm in three patients,24,39,40 trapping with coils and parent artery occlusion (PAO) in four patients,2,5,20,41 trapping with detachable balloons in one, 32 glue embolization of the AVM nidus and aneurysm in one, 42 and glue embolization of the aneurysm in three patients including the present case have been performed.35,36 One patient had failed clipping of the aneurysm and later on had successful coiling of the aneurysm and trapping of the parent artery. 5 In one patient there was spontaneous thrombosis of the ruptured pseudoaneurysm of the distal anterior inferior cerebellar artery (AICA) 21 and another patient with multiple unruptured radiation-induced aneurysms was managed conservatively with antiplatelets. 31 One patient recovered completely without treatment from spontaneous thrombosis of the radiation induced ICA bifurcation aneurysm.43 Our case is unique as this is the first case of endovascular glue embolization of a radiation-induced pseudoaneurysm from the left MCA lenticulostritate perforator with occlusion of the perforator. The initial plan was to trap the pseudoaneurysm and the proximal arterial stump using coils; however, it was impossible to navigate the microcatheter into the small perforator for coiling. Thereafter, glue embolization was successfully performed using a smaller microcatheter. The present case emphasizes the challenges of endovascular approach to aneurysms located in such small arteries. The previous cases of glue embolization were performed in relatively bigger arteries such as the AICA and posterior cerebral artery (PCA). Several factors should be kept in mind while preparing for such treatment: radiation-induced aneurysms are more fragile and prone to rupture; presence of radiation vasculitis with stenosis of the vessels may pose a serious challenge in navigating the microcatheters and wires and also increases the chances of thromboembolism; and lack of long-term data on recanalization of these aneurysms post treatment necessitates close follow up.
Summary of radiation-induced intracranial aneurysms


No treatment and died: 9 (1 died 3 years after from cardiac failure)
No treatment: 4 (2 spontaneous thrombosis)
Conservative treatment with antiplatelets: 1 NK: 7
Abbreviations – ACA: anterior cerebral artery; ICA: internal carotid artery; MCA: middle cerebral artery; AICA: anterior inferior cerebellar artery; BA: basilar artery, VA: vertebral artery; PCA: posterior cerebral artery; SCA: superior cerebellar artery; PICA: posterior inferior cerebellar artery; NK: not known.
Conclusion
Intracranial aneurysms secondary to cranial radiation are rare compared with other common manifestations such as vascular stenosis, occlusion and thrombosis. These aneurysms are usually associated with high risk of rupture and mortality due to the fragile nature of the aneurysm wall. There should be utmost urgency and low threshold in treating these aneurysms once detected. Both endovascular and surgical options have been successfully used for the treatment of radiation-induced aneurysms. The long-term outcome and recurrence rate is still unknown, thus such cases need special attention and regular follow up post treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.