
Abstract
We report a case of traumatic intracranial carotid artery pseudoaneurysm treated with an equine pericardium-covered stent. The patient was admitted to the Emergency Department after sustaining severe polytrauma in a motor vehicle accident. A cavernous carotid pseudoaneurysm was detected after an episode of massive epistaxis that required emergent nasal packing. Treatment with parent vessel sacrifice was ruled out after an unfavourable balloon test occlusion. We opted for an equine pericardium-covered stent as a means to immediately seal the wall defect in the setting of massive bleeding secondary to an unstable lesion. We describe the potential benefits and drawbacks of these prostheses and the technical difficulties encountered in this particular case. To our best knowledge, this is the first published case report on a post-traumatic intracranial internal carotid artery pseudoaneurysm successfully treated with an equine pericardium-covered stent.
Introduction
Massive epistaxis from a traumatic intracranial pseudoaneurysm is a rare but lethal condition. Emergency cases of massive exsanguinating haemorrhage may require parent vessel sacrifice. To our knowledge, this is the first published case of a post-traumatic internal carotid artery (ICA) pseudoaneurysm treated with an equine pericardium-covered stent.
Case presentation
A teenager was admitted to the Emergency Department after sustaining severe head trauma in a motor vehicle accident. At admission, an episode of massive epistaxis was treated with anterior nasal packing.
The initial computed tomography (CT) scan showed sulci effacement, subarachnoid haemorrhage and multiple parenchymal contusions. On bone window settings, the scan revealed multiple facial and skull base fractures, including the right carotid canal (Figure 1).
CT angiogram demonstrated the presence of an arterial outpouching from the medial aspect of the cavernous segment of the right ICA.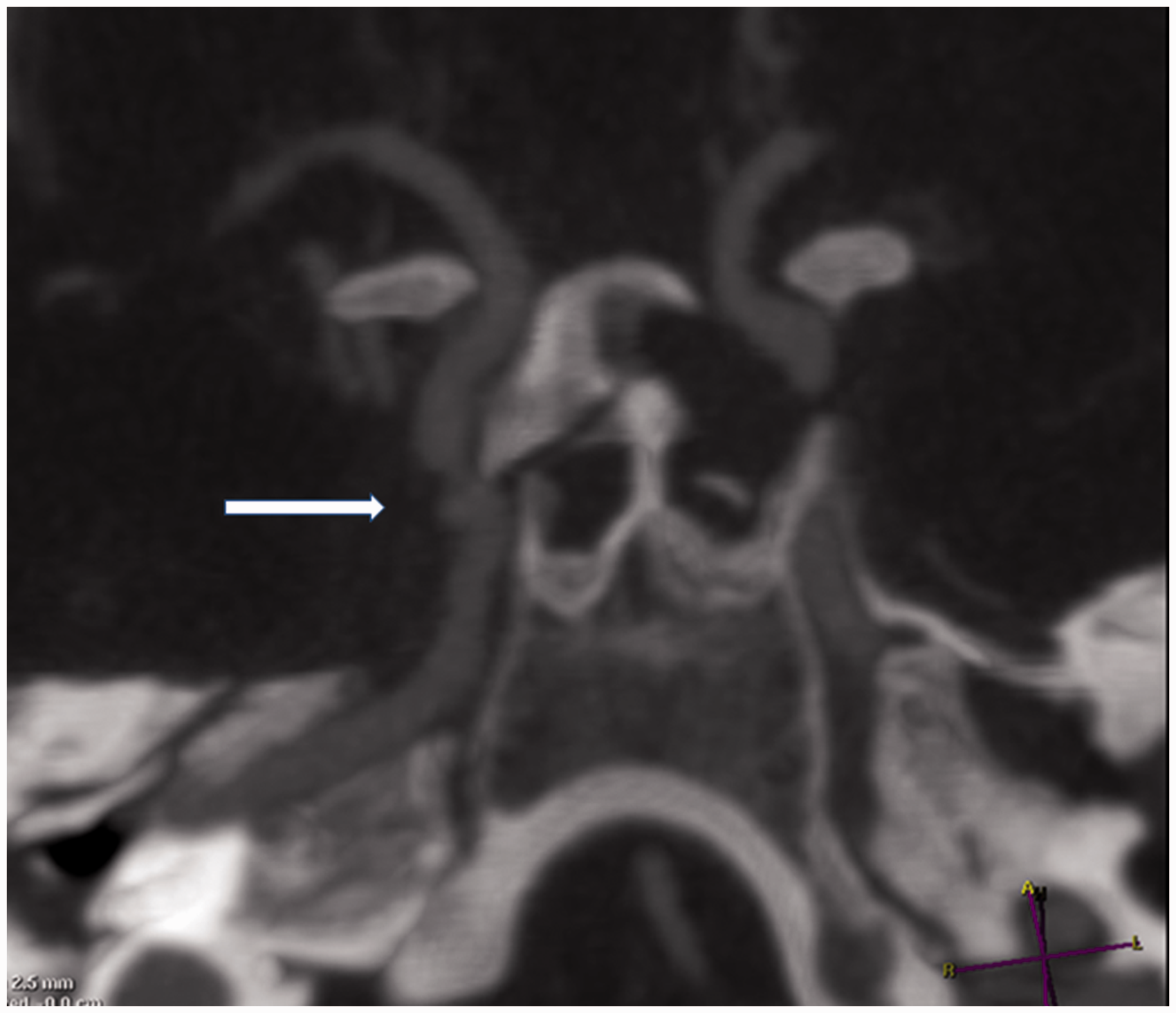
The CT angiogram demonstrated the presence of an arterial outpouching that protruded into the right sphenoid sinus and arose from the medial aspect of the cavernous segment, consistent with a post-traumatic ICA pseudoaneurysm.
The patient was moved to the angio suite for emergency digital subtraction angiography (DSA), which confirmed the presence of a cavernous segment ICA pseudoaneurysm (Figure 2). Results of a balloon anatomic occlusion test (BTO) were unfavourable, with poor collateral vessels and a delay >3 s in the venous phase on the right side.
DSA (PA and L) confirmed the presence of a cavernous segment ICA pseudoaneurysm.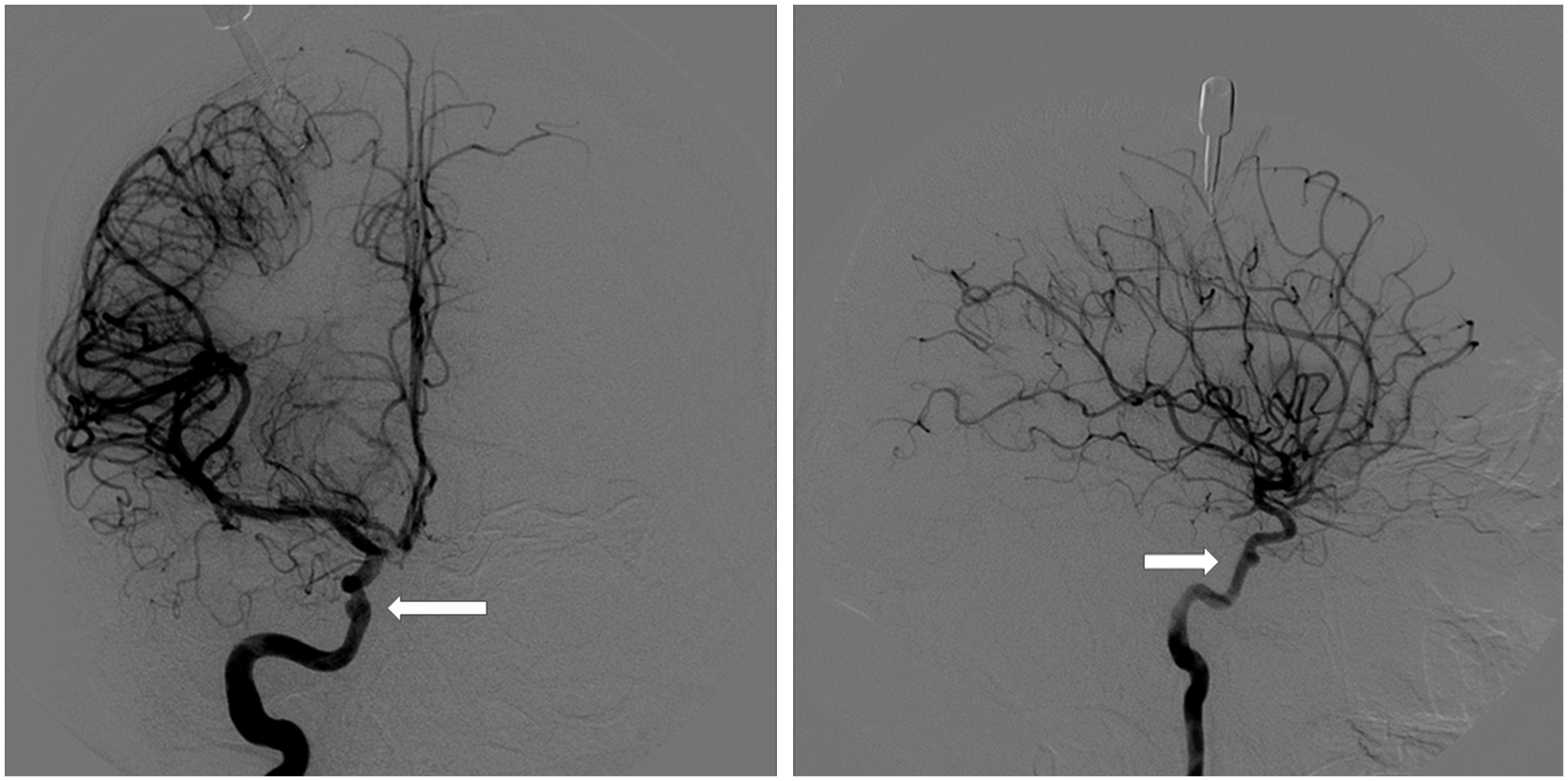
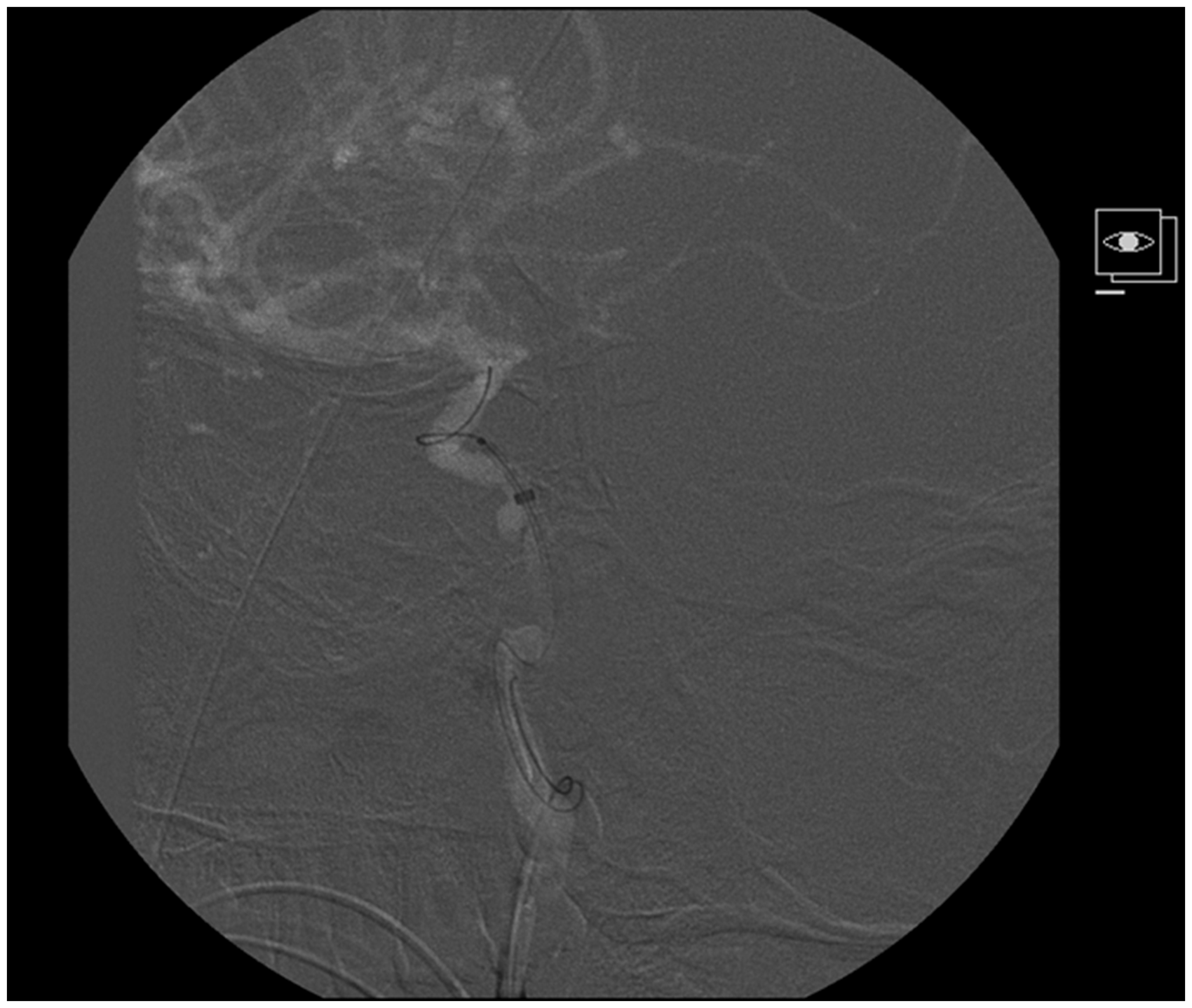
We opted for a reconstructive technique with a covered balloon-expandable stent, pre-treating the patient with clopidogrel (300 mg gastric loading dose). A right femoral approach was adopted, using an 80 cm Neuron 88 guiding catheter (Penumbra Inc., San Leandro, CA, USA). A 105 cm Navien 072 catheter (Covidien Vascular Therapies, Mansfield, MA, USA) with 0.014 Synchro guidewire (Boston Scientific Corp., Fremont, CA, USA) was navigated until reaching the petrous segment. A pericardium-covered stent (4–18 mm) (Aneugraft Nx, ITGI Medical limited, Or Akiva, Israel) was advanced over the wire; however, after repeated attempts, distal progression proved impossible (Figure 3).
A pericardium-covered stent (4–18 mm) (Aneugraft Nx, ITGI Medical limited, Or Akiva, Israel) was advanced over the wire; however, after repeated attempts, distal progression proved impossible.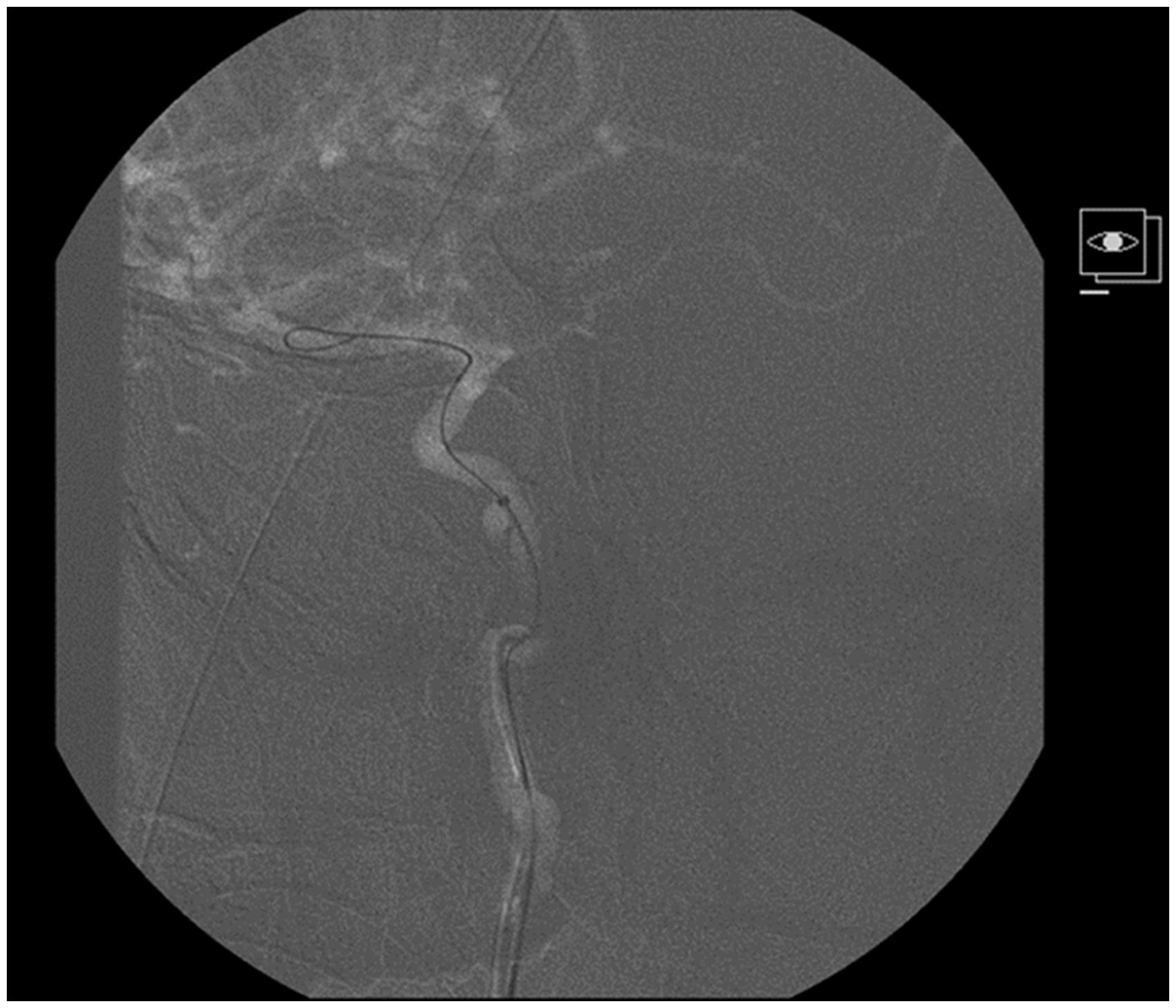
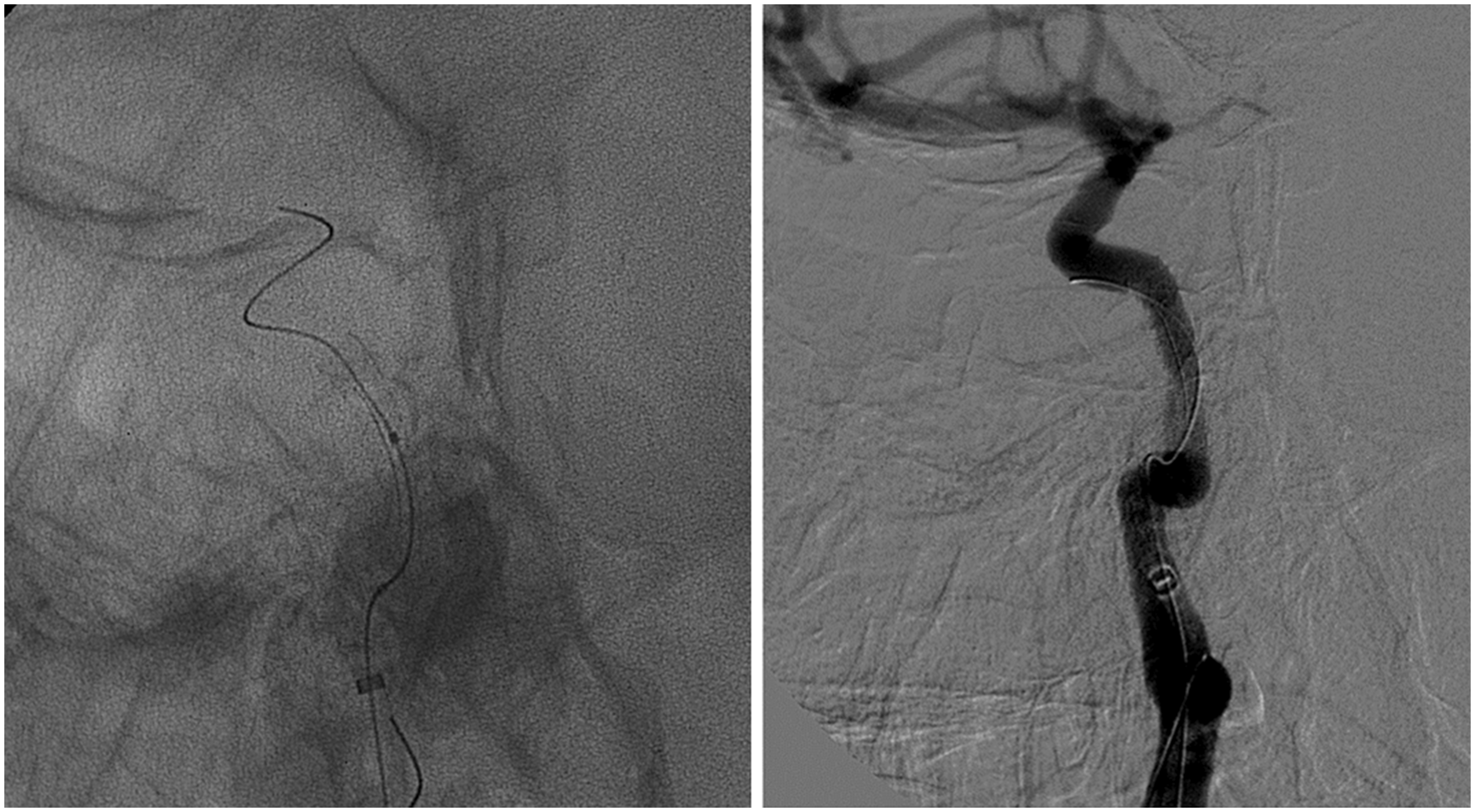
In a second attempt, a 3MAX catheter (Penumbra Inc., San Leandro, CA, USA) was employed coaxially within the Navien 072, enabling its advance (Figure 4). The 3MAX was removed and the stent was navigated to its final selected position. The Navien was then withdrawn, using a pullback standard manoeuvre with the pericardium-covered stent, which remained in stable position across the pseudoaneurysm neck (Figure 5). Inflation to 10 atm was required for successful deployment. The patient received 250 mg intravenous aspirin after the deployment. Control DSA during the procedure confirmed ICA patency with no aneurysm filling (Figure 6). There was no procedure-related complication and no further episode of recurrent epistaxis.
In a second attempt, a 3MAX catheter (Penumbra Inc., San Leandro, CA, USA) was employed coaxially within the Navien 072, enabling its advance. The Navien was then withdrawn, using a pullback standard manoeuvre with the pericardium-covered stent, which remained in stable position across the pseudoaneurysm neck. Inflation to 10 atm was required for successful deployment. Control DSA during the procedure confirmed ICA patency with no aneurysm filling.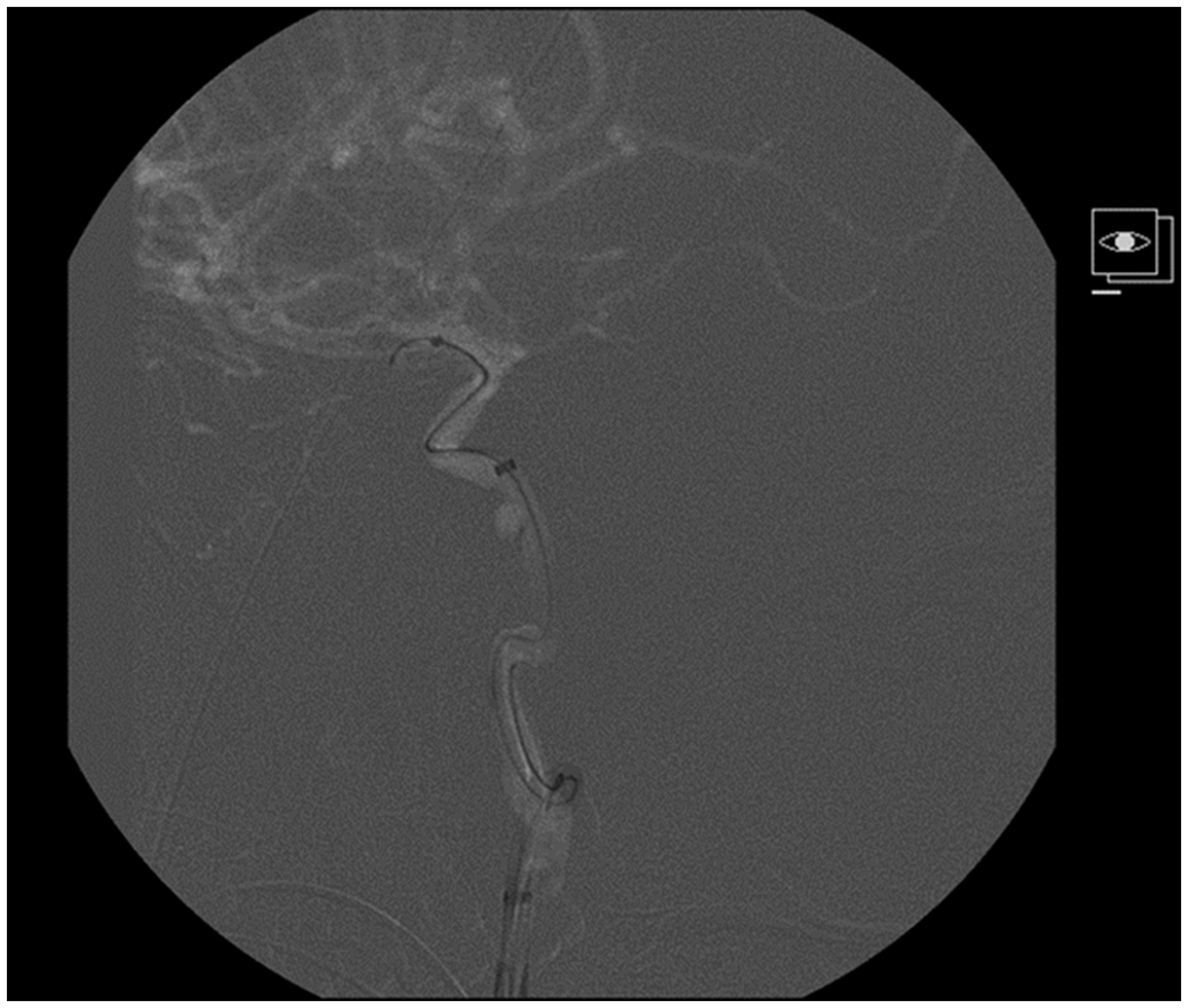
Discussion
Post-traumatic ICA pseudoaneurysms are life-threatening and require prompt intervention, given a mortality rate as high as 50%. 1
The different endovascular approaches adopted for this purpose can be divided between deconstructive and reconstructive techniques.
In deconstructive techniques, arterial sacrifice requires a detailed assessment of the collateral circulation, because it is usually impossible to conduct a clinical test in acute cases. However, even if the balloon test occlusion is tolerated, this is not a guarantee that symptoms will not develop. In addition, patients with clinical conditions such as subarachnoid haemorrhage or severe trauma that produce intracranial hypertension during their clinical course are not good candidates for deconstructive techniques in acute phase.
In reconstructive stent-assisted techniques, double antiplatelet therapy is required, and there is a risk of rebleeding if complete occlusion is not achieved, especially in very unstable lesions such as traumatic pseudoaneurysms.
In the present case, the collateral flow was poor during BTO, and parent vessel occlusion was ruled out. A reconstructive technique with an equine pericardium-covered stent was selected because of its capability to immediately seal the defect in the wall in a clinical setting of massive bleeding. Aneugraft Nx is a coaxial (0.014” lumen guidewire) balloon-expandable equine pericardium-covered stent with a platinum wire marker that defines the portion covered by the pericardium. A pressure of 5 atm was considered necessary to achieve a stent expansion diameter matching that of the vessel.
Methods such as conventional overlapping stenting or flow diverter use have previously been reported.2,3 Polytetrafluoroethylene (PTFE)-covered stents or endograft prostheses could also have been selected, 4 but we used this equine pericardium-covered stent because it was readily available at the time and has CE approval for intracranial indications. Pericardium-covered stents have also been used in extracranial circulation, mainly in interventional cardiology studies, and there is a case report of its utilization for a mycotic intracranial aneurysm. 5
In our case, the main drawback was the device-limited trackability, which required navigation across the lesion with a distal access system (Navien 072) after a first failed attempt to navigate the stent from a proximal position. The deployment pressure finally required was higher (10 atm), and there was a risk of intradural vessel rupture. Careful measurements for device size selection and a slow inflation are critical aspects with this device. Diameters range from 2.5 mm to 4.0 mm. Bare metal stent length and pericardium sleeve length range from 13 to 18 mm and from 5 to 11.2 mm, respectively. Nominal pressure is 5 atm and rated burst pressure is 14 atm.
Introduction of the type of endovascular stent used in the present case increases the risk of additional injury to the vessel wall and may result in stent thrombosis. These covered stents are relatively inflexible and carry a risk of later complications (e.g. dissection or delayed intimal hyperplasia), especially when deployed in tortuous arterial segments, leading to early restenosis. Although the stent was placed in a straight segment in our patient, follow-up DSA angiograms are warranted in all cases.
Conclusion
To our knowledge, this is the first published case report on a post-traumatic intracranial ICA pseudoaneurysm successfully treated with an equine pericardium-covered stent, which appears to be an effective option for parent vessel reconstruction.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.