
Abstract
Background
In acute ischemic stroke patients with large-artery occlusion, uncertainties remain about whether clinically important outcomes are comparable between first-line contact aspiration and stent-retriever thrombectomy, although two trials have investigated whether one strategy should be preferred over another.
Purpose
The purpose of this article is to compare the efficacy and safety of first-line contact aspiration and stent-retriever thrombectomy in stroke patients with anterior circulation large-artery occlusion.
Methods
We undertook a systematic review of studies of patients treated for large-artery occlusion, with the latest devices of either strategy, within six hours of stroke onset. We determined rates of final complete reperfusion (defined as modified Thrombolysis In Cerebral Infarction score = 3), periprocedural complications and 90-day functional independence (defined as modified Rankin Scale (mRS) score 0–2), and excellent outcome (defined as mRS score 0–1) after contact aspiration and after stent-retriever thrombectomy using random-effects meta-analyses. Any differential effects in rates between the two strategies were assessed using random-effects meta-regressions.
Results
Fifteen studies (1817 patients) were included. There was no difference in rates of final complete reperfusion at the end of all endovascular procedures between contact aspiration and stent retrievers (51.1%, 95% confidence interval (CI) 39.3–62.9; vs 38.3%, 95% CI 28.6–48.0; pint = 0.14), 90-day functional independence (45.0%, 40.7–49.2; vs 52.4%, 47.7–57.1; pint = 0.45) and excellent outcome (32.1%, 25.7–38.5; vs 34.1%, 21.2–46.9; pint = 0.94). Rates of periprocedural complications did not differ between the two strategies.
Conclusions
Current data suggest no difference in efficacy and safety between first-line contact aspiration and stent-retriever thrombectomy in stroke patients with large-artery occlusion.
Introduction
The clinical benefit of mechanical thrombectomy in acute ischemic stroke patients with large-artery occlusion of the anterior circulation is well established.1,2 Because trials predominantly used stent-retriever devices, guidelines recommend their use. 3 In similar populations a more recent strategy, first-line contact aspiration, involving the use of a large-bore aspiration catheter, has been reported to achieve high reperfusion rates at a lower cost than first-line stent-retriever thrombectomy4–6 and histological findings in animals have suggested less damage to artery walls. 7
However, uncertainties remain about whether clinically important outcomes are comparable between first-line contact aspiration and stent-retriever use in acute stroke patients with anterior circulation large-artery occlusion, although two trials have investigated whether one strategy should be preferred over another.8,9 The Effect of Endovascular Contact Aspiration vs Stent Retriever on Revascularization in Patients with Acute Ischemic Stroke and Large Vessel Occlusion (ASTER) trial 8 failed to establish the superiority of first-line contact aspiration against stent-retriever use on final successful reperfusion rates; and it would therefore be wrong to assume that the two strategies have similar effects on reperfusion rates. Also, although the recent comparison of direct aspiration vs stent retriever as a first approach (Cardiovascular Outcomes for People Using Anticoagulation Strategies (COMPASS)) trial 9 showed the noninferiority of first-line contact aspiration to stent-retriever use with respect to good clinical outcome, findings should be interpreted with caution because 85% of the patients treated with stent retrievers received concomitant aspiration.
Systematic reviews can help to assess the existing evidence on the effects of interventions. However, the only published systematic review comparing reperfusion rates and clinical outcomes between the two strategies has left unanswered questions, mainly due to the inclusion of mixed populations. 10 The authors did not restrict inclusion to studies of patients with proximal anterior circulation occlusion, and studies combining patients with posterior and anterior circulation occlusions as well as those with distal occlusions were included. However, there is as yet no evidence that mechanical thrombectomy is beneficial in acute stroke patients with distal anterior circulation occlusion or in those with posterior circulation occlusion, and its use is not currently recommended. In addition, studies using different generations of catheters were included; however, catheters have evolved over time, with the use of the latest generation of devices carrying higher reperfusion rates.11–13 Finally, no upper time limit from stroke onset to endovascular treatment was defined in this review, although the benefit of mechanical thrombectomy is time related 14 and guidelines recommend its use in a specific time window. 3
In view of these uncertainties, we undertook a systematic review and meta-analysis to compare the efficacy and safety of contact-aspiration and stent-retriever thrombectomy as first-line therapy using the latest generation of devices, and to determine the risk factors for reperfusion failure after first-line technique alone in acute stroke patients with anterior circulation large-artery occlusion.
Methods
The data, analytic methods, and study materials have been made available to other researchers for purposes of reproducing the results or replicating the procedure. We declare that all supporting data are available within the article and its online supplementary files.
We report our study according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses. 15 We sought studies including ≥10 ischemic stroke patients with a large-artery occlusion in the anterior circulation (defined as distal internal carotid artery or proximal segments of the middle cerebral artery) and in whom endovascular treatment with first-line contact aspiration or first-line stent-retriever thrombectomy was initiated within six hours of stroke onset, as recommended. 16 In March 2018, in view of two recently published trials,17,18 the time window for mechanical thrombectomy was extended after the first six hours in the subgroup of patients fulfilling restrictive imaging criteria, as described in the trials. 19 However, as the two trials were published after the time of our electronic search strategy, authors of eligible studies were unlikely to have selected patients based on similar imaging criteria. Therefore, we did not change our selection criteria, which remain in line with the guidelines available at the time of our electronic search strategy.
We reduced bias and confounding due to secular trends in acute stroke management (including endovascular therapy devices and use of complementary mechanical techniques) by including only studies whose recruitment period was after January 2012, which corresponds to the introduction of the first-line contact-aspiration technique. 4 We also restricted our inclusion criteria to studies of patients treated with the second generation of stent retrievers (Solitaire FR, Covidien, Irvine, CA, USA, or Trevo, Stryker Neurovascular, Fremont, CA, USA), which have been shown to be superior to the Merci retriever for reperfusion and clinical outcomes,12,13 or those treated with large-bore aspiration catheters (5MAX, 5MAX ACE, ACE64, Penumbra, Alameda, CA, USA; SOFIA 5F or 6F, MicroVention, Tustin, CA, USA) because their larger diameter is estimated to enable greater aspiration flow rates than previous-generation aspiration catheters (with separator). 11 Studies of patients treated with concomitant contact aspiration and stent retriever were excluded. Studies of patients treated with the recent EmboTrap stent-retriever system were not included. Although some data from registries20–22 showed promising results, no comparative data are available on clinical outcomes between the EmboTrap system and Solitaire or Trevo stent retrievers. Studies of patients with anterior circulation occlusion and concomitant cervical carotid occlusion (tandem occlusion) were not excluded. Studies involving patients with anterior and posterior circulation occlusion in which information on anterior circulation could be extracted separately were included. Studies with delay of endovascular treatment not restricted to within six hours after stroke onset were included if data on patients treated within six hours after stroke onset were available separately.
We searched Medline and Embase on November 1, 2018, to identify studies of patients treated with stent retrievers using both the medical subject heading (MESH) and text words (“mechanical thrombectomy” OR “Trevo” OR “Solitaire” OR “endovascular treatment”) AND (“ischaemic stroke” OR “ischemic stroke”). To identify studies of patients treated with contact aspiration, we updated our previous systematic review 23 to November 1, 2018, using MESH and text words (“thrombo-aspiration” OR “penumbra system” OR “ADAPT” OR “SOFIA”) AND “stroke” in Medline and Embase; we restricted our inclusion criteria to patients with anterior circulation occlusion only, therefore the number of included studies was smaller than in our previous meta-analysis. After screening all titles and abstracts for potentially eligible studies, we screened the full texts and collected data using a prespecified data extraction file. We also added data from the prospective endovascular database from the Department of Interventional Neuroradiology (Lyon University Hospital, Lyon, France) of all stroke patients treated by mechanical thrombectomy between January 1, 2015 and December 31, 2016, after exclusion of those included in the ASTER trial. 8 If there were multiple publications from one cohort, we included only the publication with the largest amount of data relevant to this review. We did not restrict inclusion by study language or study design.
We extracted data on final successful reperfusion (defined as modified Thrombolysis In Cerebral Infarction (mTICI) score of 2b or 3) and complete reperfusion (mTICI = 3). The mTICI is a categorical scale to measure reperfusion after intraarterial treatment in stroke patients, with scores ranging from 0 (no reperfusion) to 3 (complete reperfusion), and a TICI score of 2b or 3 indicates successful reperfusion 24 (Supplementary Table 1). We also collected information on periprocedural complications (symptomatic intracranial hemorrhage (sICH), subarachnoid hemorrhage (SAH), downstream emboli in the same territory as the primary occlusion, emboli in a new territory (ENT), new cerebral infarct (defined as infarct confirmed by brain imaging involving a new territory), arterial dissection and vessel perforation) and 90-day functional independence (defined as a modified Rankin Scale (mRS) score of 0, 1 or 2), excellent outcome (defined as an mRS of score 0–1) and all-cause mortality. The mRS is a categorical scale to measure functional outcome in stroke patients, with scores ranging from 0 (no symptom) to 6 (death), and a score of 2 or less indicates functional independence. 25 Additionally, we extracted data on study design (retrospective, prospective observational study, randomized controlled trial), patients’ baseline characteristics (age, sex, previous hypertension, diabetes, atrial fibrillation and dyslipidemia, National Institutes of Health Stroke Scale (NIHSS) and Alberta Stroke Program Early Computed Tomography (ASPECT) scores pretreatment), clot location and length, stroke etiology, types of devices used and 90-day cause of death.
Critical appraisal for assessing the quality of studies was based on the RoBANS tool 26 for nonrandomized studies and on the Cochrane Collaboration tool 27 for randomized studies. Additionally, assessment of the risk of bias was undertaken at the study level based on study design, methods of ascertainment for posttreatment reperfusion (i.e. whether an independent core lab was used) and requirement for center experience in endovascular treatment. We used funnel plots to assess the risk of bias across studies.
Statistical analysis
Rates of successful (mTICI of 2b or 3) and complete (mTICI = 3) reperfusion, after first-line technique alone and after all endovascular procedures, which included the use of rescue therapy in cases of unsuccessful reperfusion after first-line technique alone, were calculated using random-effects model meta-analyses. 28 Rates of periprocedural complications and 90-day outcomes after each strategy were calculated using similar methods. Because the stent-retriever strategy can be performed with and without flow arrest using a proximal balloon, we also determined the rates of reperfusion and 90-day outcomes in sensitivity analyses restricted to the studies using the flow-arrest technique, which is estimated to carry higher reperfusion rate and minimize thrombus fragmentation.29,30 We investigated any differences in reperfusion rates after each strategy based on study design (randomized or nonrandomized), presence of an independent core lab assessment and requirement of center experience in mechanical thrombectomy using random-effects meta-regressions and reported p values (pint) obtained from random-effects meta-regressions analyses. 31 We assessed differential effects between contact aspiration and stent-retriever thrombectomy using random-effects meta-regressions. To investigate any potential for selection biases, we explored differences in baseline patient characteristics by endovascular strategies using similar analyses. In addition, we determined the associations between baseline age, NIHSS score, clot location, stroke etiology and bridging therapy use and reperfusion failure (defined as mTICI < 2b) after first-line strategy alone. Statistical heterogeneity between studies was assessed and quantified with the I2 index. 32 Statistical analyses were performed in R version 3.1.3 and Review Manager version 5.3.
No ethical approval for research was required for this systematic review.
Results
A total of 7197 unique titles were identified from the electronic search strategy of stent-retriever thrombectomy and from the update of our previous systematic review on contact aspiration. After abstract screening and full-text assessment,4,8,33–44 14 studies were included in the meta-analysis. Then, we added data from our prospective registry, leading to the final inclusion of 15 studies (1817 patients, Figure 1, Supplementary Tables 2–4 and Appendix 1). Information on patients treated with contact aspiration was available in nine4,8,33–37,43 studies (one randomized controlled trial, five retrospective observational studies and three prospective observational studies, including our prospective registry) and with stent retriever in eight8,38–41,44,45 (six randomized controlled trials, one prospective observational studies and our registry). In one study
44
involving patients treated with stent retriever or contact aspiration, we included only those treated with stent retrievers because of overlaps in patients treated with contact aspiration with another study.
43
Because several types of stent retrievers were used in the participants of the MR CLEAN trial,
45
we included only those treated with Trevo or Solitaire stent retrievers.
42
The list and reasons for exclusion of studies that had evaluated the efficacy or safety of contact aspiration or stent-retriever thrombectomy are provided in Supplementary Appendix 2.
Flowchart.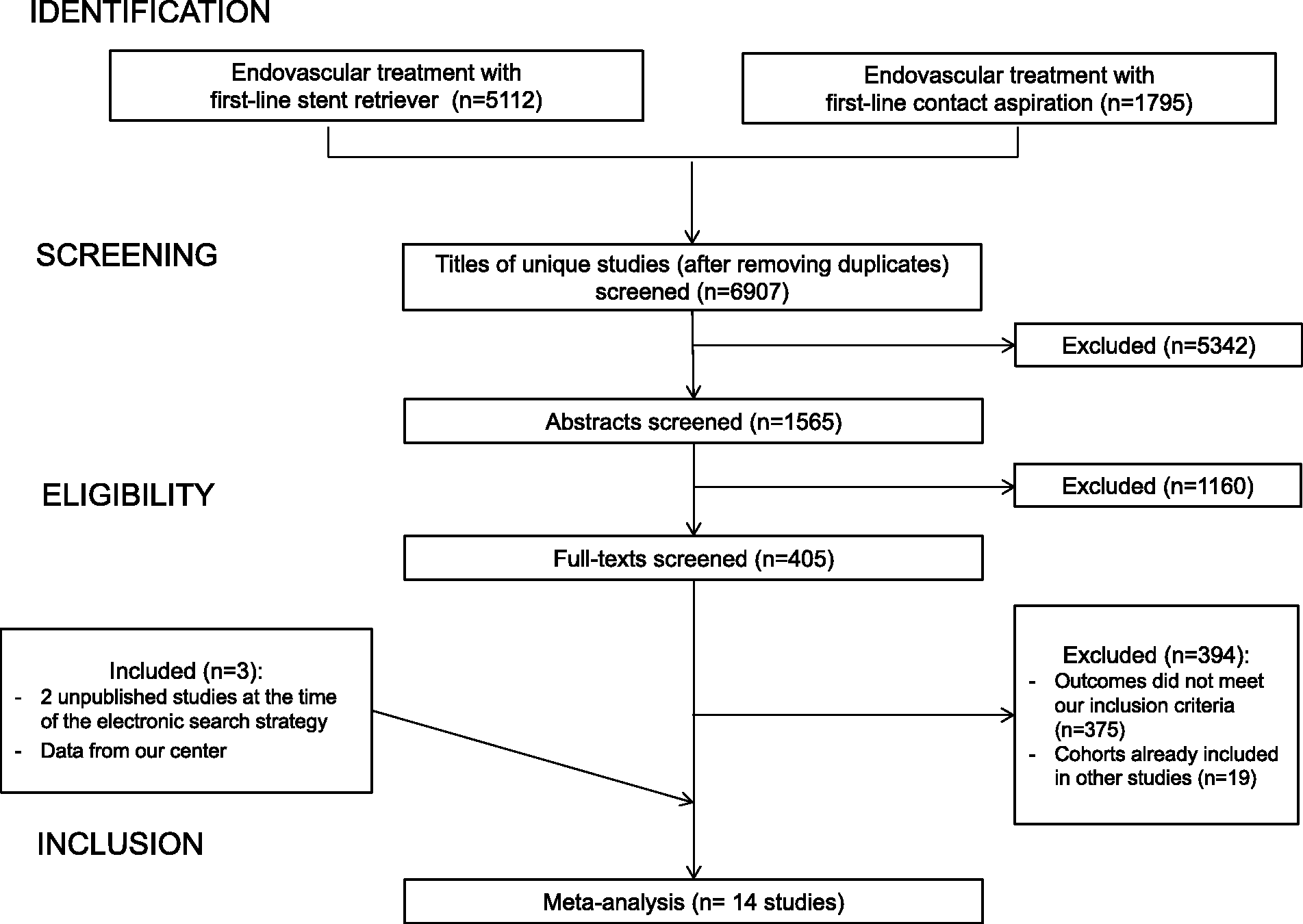
Low risk of bias was found in randomized and nonrandomized studies (Supplementary Tables 5 and 6). The number of passes required with the first-line catheters before switching to rescue treatment was defined in only two studies 8 (including ours), with a minimal number of three passes. sICH definitions used in individual studies are reported in Supplementary Table 7.
Baseline patient characteristics.
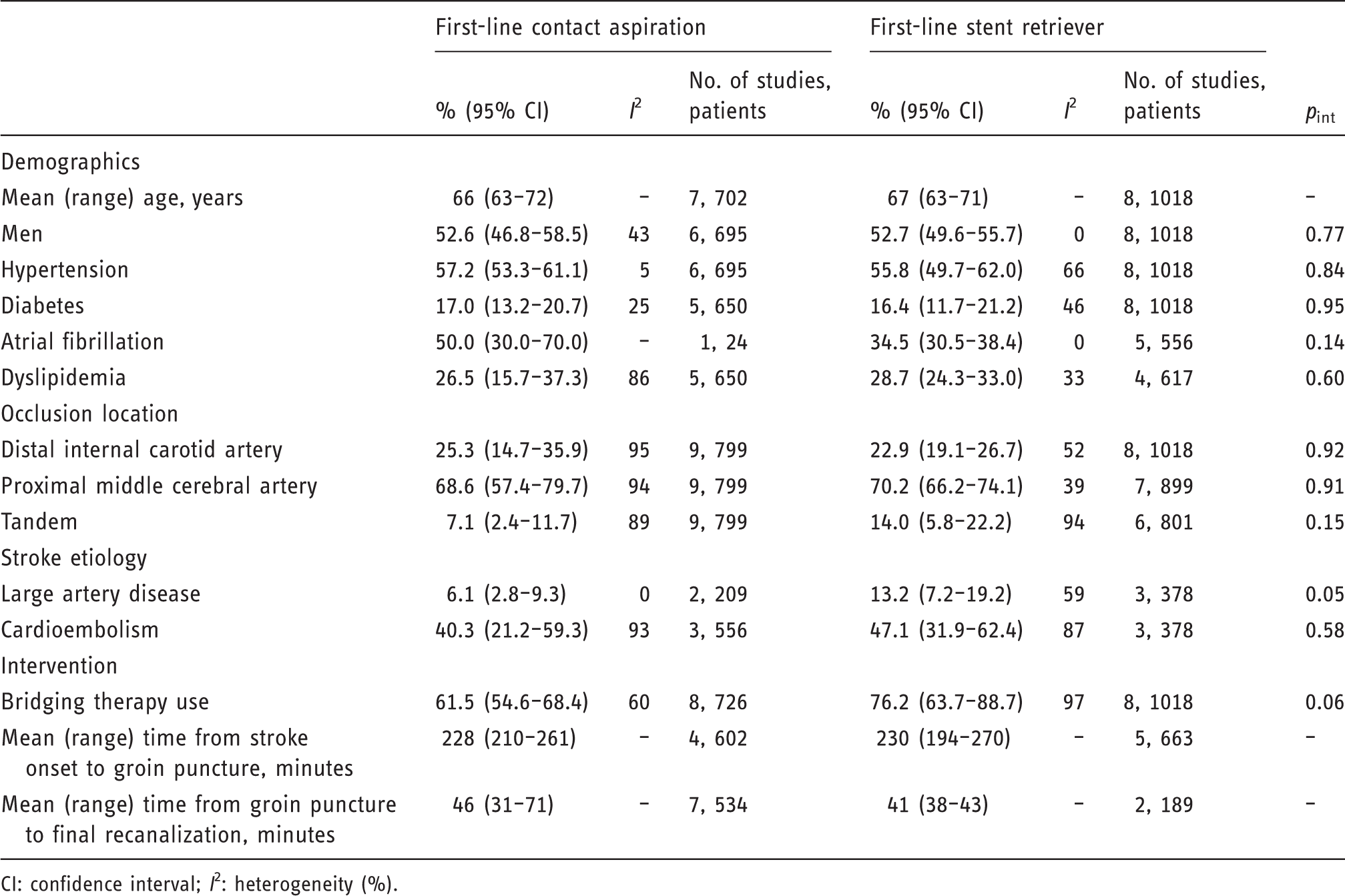
CI: confidence interval; I2: heterogeneity (%).
Meta-analyses of the outcomes between contact aspiration and stent retriever as first-line therapy.
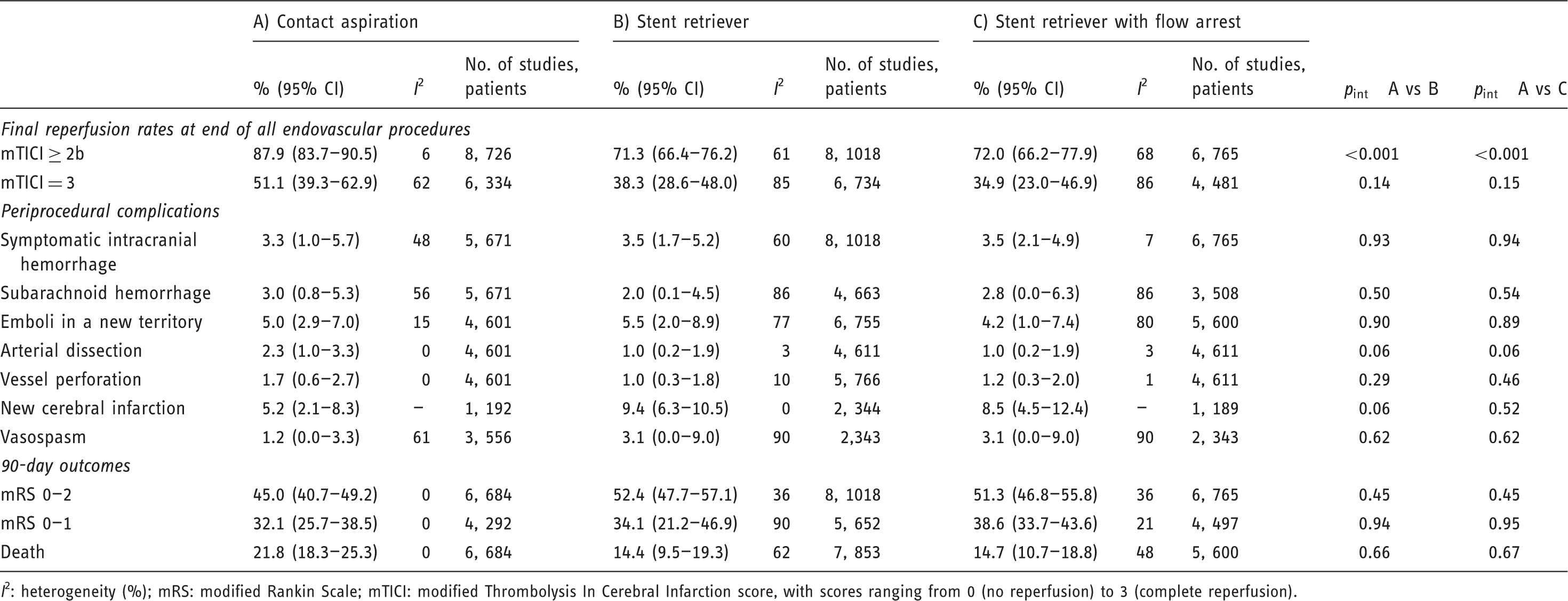
I2: heterogeneity (%); mRS: modified Rankin Scale; mTICI: modified Thrombolysis In Cerebral Infarction score, with scores ranging from 0 (no reperfusion) to 3 (complete reperfusion).
After first-line stent retriever, the pooled rate of final successful reperfusion at the end of all endovascular procedures was 71.3% (95% CI 66.4–76.2, Table 2) and those of complete reperfusion was 38.3% (28.6–48.0), with no difference based on study design (pint = 0.88 and pint = 0.62, respectively), presence of an independent core lab assessment (pint = 0.97 and pint = 0.31, respectively) or requirement of center experience in mechanical thrombectomy (pint = 0.12 and pint = 0.95, respectively). After first-line stent retriever alone, the pooled rate of successful reperfusion was 67.7% and a rescue therapy was used in 23.8% in the only study reporting data (Supplementary Table 4).
The rate of each periprocedural complication was less than 10% (Table 2), with no difference based on requirement of center experience (pint = 0.31 for sICH, pint = 0.10 for SAH, pint = 0.11 for ENT, pint = 0.34 for arterial dissection, and pint = 0.14 for vessel perforation). No study reported information on new emboli in the same territory. At 90 days, pooled rates were 52.4% (95% CI 47.8–57.1) for functional independence, 34.1% (95% CI 21.2–46.9) for excellent outcome and 14.4% (95% CI 9.5–19.3) for death, with no study reporting information on cause of death (Table 2). Funnel plots of the rates of final reperfusion and 90-day outcome were symmetrical, suggesting no publication bias (Supplementary Figure 2).
Compared to stent-retriever use, the pooled rate of final successful reperfusion at the end of all endovascular procedures was significantly higher after contact aspiration (pint < 0.001) but there was no difference in the rates of final complete reperfusion (pint = 0.08), periprocedural complications and 90-day outcomes (Table 2). The additional analyses comparing studies of stent retrievers with flow arrest and those of contact aspiration did not change the findings, the rate of final successful reperfusion at the end of all endovascular procedures being significantly higher after contact aspiration (pint < 0.001), with no difference in the rates of final complete reperfusion, periprocedural complications and 90-day outcomes (Table 2).
After first-line contact aspiration alone, neither age, NIHSS score, clot location or bridging therapy use was associated with reperfusion failure (Figure 2, Supplementary Figures 3–8). Information on stroke etiology was available in only two studies,8,43 which reported no association with reperfusion failure. After first-line stent retriever alone, no study reported data on reperfusion in the prespecified subgroups.
Forest plots of the meta-analyses of potential risk factors of reperfusion failure (mTICI < 2b) after first-line contact aspiration alone.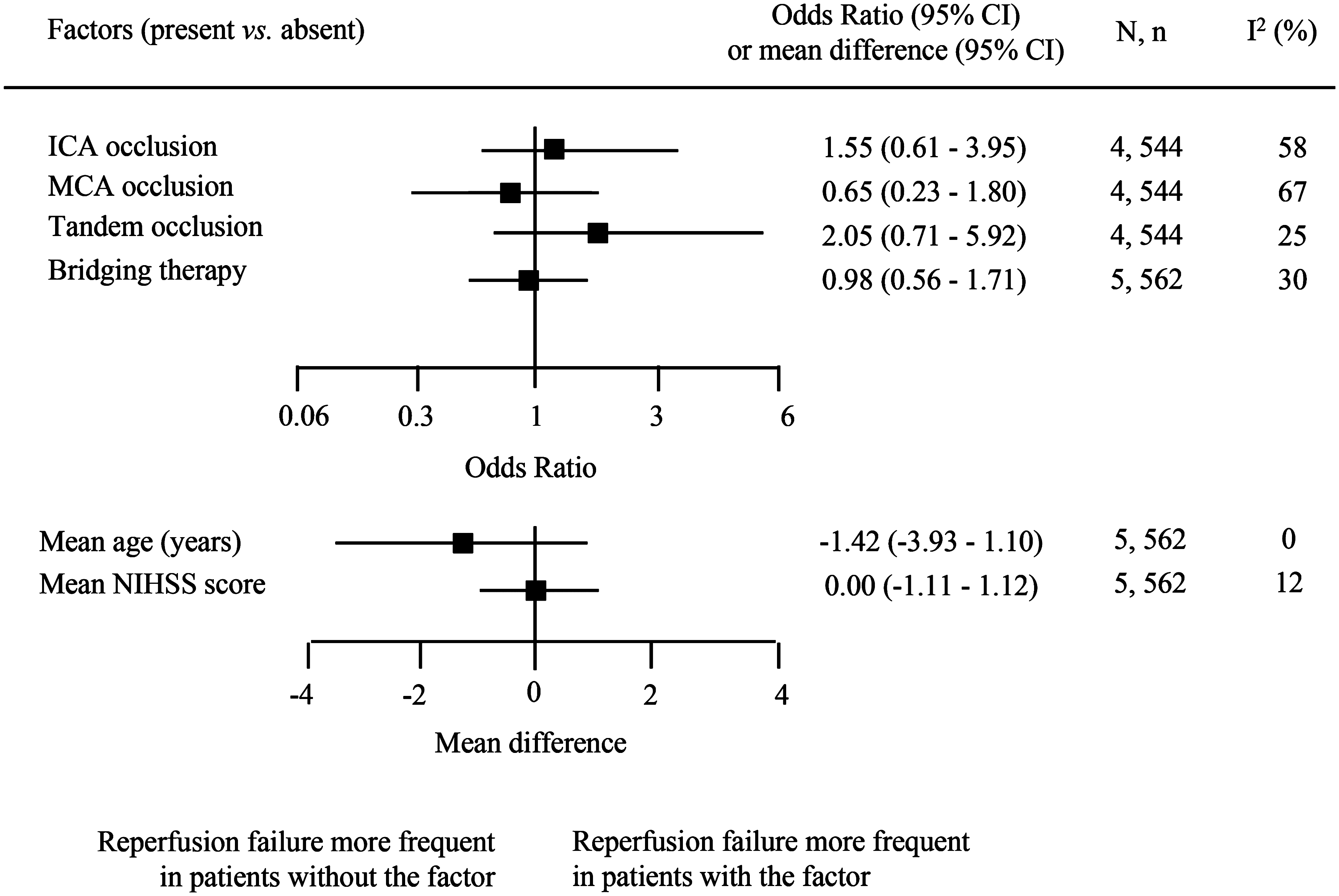
Discussion
In this meta-analysis of acute stroke patients with anterior circulation large-artery occlusion, although the final successful reperfusion rate at the end of all endovascular procedures was significantly higher after first-line contact aspiration than after stent-retriever thrombectomy, the rate of final complete reperfusion and of functional independence did not differ between the two strategies. There is increasing evidence that complete reperfusion (mTICI = 3) may more accurately predict good clinical outcome than the combined criteria of successful reperfusion (mTICI of 2b or 3),46–49 and this may partly explain the findings.
Despite variability in selection criteria among studies as well as in study design, current data suggest no difference in the clinical and safety profiles of contact aspiration and stent-retriever thrombectomy as first-line strategy with the latest generation of devices. Although randomized controlled trials provide the highest level of evidence, the necessity of a noninferiority trial here is questionable. Sample size calculation of noninferiority trials depends on the choice of the margin of noninferiority, and sample size is usually larger than for superiority trials. Assuming a rate of successful reperfusion of 85% with aspiration and of 70% with stent retriever and a margin of noninferiority of five percentage points, with a power of 90% and a significance level of 5%, a trial assessing the noninferiority of contact aspiration against stent retriever would require 1550 patients in each group, which is larger than all previous trials.
A new strategy for mechanical thrombectomy combines the use of aspiration with the stent-retriever catheter (triaxial system) as concomitant aspiration is hypothesized to promote entrapment of the clot within the stent retriever. Data on clinical outcomes with this combined approach are scarce and mainly come from uncontrolled, small, retrospective studies or case reports.33,50–52 Whether this system is associated with additional benefit compared to the first-line use of either technique alone remains uncertain, and a randomized trial comparing the use of contact aspiration combined with stent retrievers vs stent-retriever use alone is ongoing. 53 Reperfusion rates after contact aspiration and stent retrievers are high, and randomized controlled trials aiming to assess the superiority of the combined contact aspiration and stent-retriever approach against the first-line strategy alone would therefore require a very large sample size to have sufficient statistical power.
Assessing the optimal thrombectomy method based on patients’ clinical features and/or thrombus characteristics might help to improve acute management of stroke. However, we found that subgroups of patients who are unlikely to achieve a successful reperfusion after first-line strategy alone, and for whom the combined approach might be justified, are not readily identifiable at present. Also, further research with imaging analyses aiming to detect which technique is less prone to thrombus fragmentation, which leads to downstream emboli as well as emboli in new territories, is needed.
Although we consider our findings to be valid, our study has limitations. First, our results were heterogeneous but this is commonly observed in meta-analyses of absolute risks because of the population case mix and we used a random-effects model to take this into account. Second, study designs between the two strategies were not well balanced. However, the inclusion of a higher number of randomized controlled trials in patients treated with stent retrievers than in those treated with contact aspiration was expected. While several randomized controlled trials have been published in stroke patients treated with stent retrievers, only two have been published in those treated with contact aspiration, of which one met our inclusion criteria. Randomized controlled trials tend to select more healthy patients and to involve more experienced operators than observational studies. However, we found no difference in reperfusion rates and clinical outcomes after either strategy based on study design or whether experience in mechanical thrombectomy was required, although meta-regressions cannot rule out ecological biases. 31 Despite a higher number of randomized controlled trials in the studies of stent retriever than in those of contact aspiration, which might have overestimated the likelihood of good outcomes with stent retriever compared to contact aspiration, the rates of functional independence, excellent outcome and periprocedural complications did not differ between the two strategies. Third, the prevalence of stroke due to large-artery disease was higher in studies of patients treated with stent retrievers than in those treated with contact aspiration; however, there is no evidence in the literature for a difference in the efficacy of thrombectomy based on stroke etiology by either technique and this is therefore unlikely to have biased the findings. Fourth, there might have been a learning curve effect with the initiation of thrombectomy with contact aspiration, and it is possible that the recanalization rates reported in the first publications were lower than those reported in the more recent publications. However, it is also possible that publication biases occurred with the publication of more positive studies than negative studies when the technique was initiated. Whether this has influenced the recanalization rates and clinical outcomes after contact aspiration remains uncertain. Additionally, we were unable to compare reperfusion rates between the two first-line techniques alone because only one study reported data on the use of rescue therapy after reperfusion failure with stent retriever alone. It is also possible that the higher successful reperfusion rate observed after contact aspiration than stent retrievers was due to the use of rescue therapy. Finally, the finding on the rate of sICH needs to be interpreted with caution because of the variation in definitions of sICH among studies.
Conclusion
In acute ischemic stroke patients with anterior circulation large-artery occlusion, currently available data on the efficacy and safety after contact aspiration and after stent-retriever thrombectomy as first-line strategy suggest no difference between the two groups. Data on risk factors for reperfusion failure after either first-line technique alone remain scarce.
Supplemental Material
Supplemental material for First-line contact aspiration vs stent-retriever thrombectomy in acute ischemic stroke patients with large-artery occlusion in the anterior circulation: Systematic review and meta-analysis
Supplemental Material for First-line contact aspiration vs stent-retriever thrombectomy in acute ischemic stroke patients with large-artery occlusion in the anterior circulation: Systematic review and meta-analysis by Marion Boulanger, Bertrand Lapergue, Francis Turjman, Emmanuel Touzé, René Anxionnat, Serge Bracard, Michel Piotin and Benjamin Gory in Interventional Neuroradiology
Footnotes
Acknowledgments
Author contributions include the following: Collected data and participated in study design: M.B. and B.G. Performed statistical analysis: M.B. Interpreted the results: M.B., B.G. and E.T. Drafted the manuscript: M.B. Edited/reviewed the manuscript: B.L., F.T., E.T., R.A., S.B., M.P. and B.G.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.