
Abstract
Background
Fusiform dissecting aneurysms involving the dominant vertebral artery with poor collaterals are challenging to treat. The purpose of this study was to present an initial experience with a fill and tunnel technique for reconstructive endovascular treatment of these conditions.
Methods
A total of 13 patients, 11 men and 2 women, each with a fusiform vertebral artery dissecting aneurysm not amenable to internal trapping of the parent artery, underwent reconstructive endovascular treatment using a fill and tunnel technique between January 2012 and December 2015. The safety, feasibility, and clinical and angiographic outcomes of these procedures were retrospectively evaluated.
Results
The average maximum diameter of the fusiform aneurysms was 12.1 mm. Five were ruptured. Three aneurysms were treated with a single stent and the remaining 10 aneurysms required double-stent placement. Treatment was technically successful in all 13 patients, achieving complete occlusion (n = 10, 76.9%) and near-complete occlusion (n = 3, 23.1%). No procedure-related complications occurred in any patient. There were no delayed thromboembolic or hemorrhagic complications during the follow-up period (mean, 19.0 months). Angiographic follow-ups (mean, 9.1 months) showed stable occlusion in 90.9% (10/11) and asymptomatic in-stent occlusion in one patient (9.1%, 1/11). At the end of the observation period (mean, 19.0 months), all patients had excellent clinical outcomes (modified Rankin Scale (mRS) 0, 92.3%, 12/13), except one (mRS 4), resulting from poor preoperative status.
Conclusions
This retrospective study demonstrated that endovascular reconstruction using a fill-and-tunnel technique was a technically safe, feasible, and clinically effective treatment method for fusiform vertebral artery dissecting aneurysms with ipsilateral dominance.
Introduction
Intradural vertebral artery (VA) dissection has been recognized as an important cause of subarachnoid hemorrhage (SAH) and ischemic stroke affecting young or middle-aged adults and may result in aneurysmal dilatation, also called VA dissecting aneurysm (VADA). 1 In particular, ruptured VADAs have a high rate of early rebleeding with catastrophic outcomes. 2 Treatment by internal trapping of the dissected segment of the parent artery is usually performed and is one of the most reliable techniques to prevent rebleeding.3–6 However, this procedure is not suitable for fusiform VADAs that involve the dominant VA with poor collaterals. 7 Endovascular reconstruction using coils and stents could be a feasible alternative treatment under these special conditions. To date, various endovascular techniques have been applied to achieve parent artery preservation and aneurysm exclusion from the circulation simultaneously.7–15 However, no study has answered the question of which endovascular technique is the most useful for endovascular reconstruction under these conditions. Moreover, there have been no randomized studies comparing the efficacy of endovascular techniques and several retrospective studies have been conducted with small numbers of patients, short-term follow-up, and no standardization of endovascular techniques. In the present series, to achieve complete aneurysm exclusion and parent artery preservation, we attempted to treat fusiform VADAs with a fill-and-tunnel technique (FT). Our aim was to evaluate the efficacy of FT using coils and stents for the endovascular reconstructive treatment of fusiform VADAs with ipsilateral dominance by reviewing patients’ clinical and radiological data.
Methods
Study plan
We performed a review of the clinical and radiological records of all patients during a 48-month period from January 2012 to December 2015, in a prospective registry of patients who underwent FT for the treatment of fusiform VADAs with ipsilateral dominance. FT was attempted in almost all fusiform aneurysms that were expected to be difficult to treat using conventional surgical or endovascular techniques. However, only patients harboring ruptured or unruptured fusiform VADA were included in this study. VADAs involving the origin of the dominant posterior inferior cerebellar artery were excluded from this study because this condition was approached using a different treatment strategy. The treatment strategy applied to posterior inferior cerebellar artery-involved VADAs included occipital artery-posterior inferior cerebellar artery bypass followed by internal trapping of the aneurysm and occipital artery-posterior inferior cerebellar artery bypass followed by reconstructive treatment using FT. Medical data were collected prospectively in accordance with our protocol and reviewed retrospectively with approval from the institutional review board. Owing to the retrospective nature of this study, the requirement for consent was waived by the local institutional review board.
General information on endovascular treatment
In general, endovascular treatment was administered as soon as possible after SAH, regardless of the clinical condition of the patient. All patients without SAH received a dual-antiplatelet medication including 75 mg of clopidogrel and 100 mg of acetylsalicylic acid (ASA) each day for five days before the procedure. For patients who presented with SAH, dual-antiplatelet premedication was not prescribed because of the risk of rebleeding. All procedures were performed via the unilateral or bilateral transfemoral approach under intravenous sedation with full anticoagulation accomplished by the use of intravenous heparin. The activated clotting time was maintained at two to three times the baseline measurement throughout the procedure.
All patients received subcutaneous administration of 2850 IU of low-molecular heparin (Fraxiparin, GlaxoSmithKline, Marly-le-Roi Cedex, France) twice or three times per day, for a duration of three days postoperatively according to our protocol of stent-assisted coiling. After the procedure, all patients with SAH were prescribed dual-antiplatelet medication, which consisted of a loading dose of 300 mg of clopidogrel and 300 mg of ASA. In all patients, dual-antiplatelet drugs, which consisted of clopidogrel (75 mg) and ASA (100 mg) each day, were also maintained for at least six months. A clopidogrel resistance test was performed approximately 24 hours after drug administration in all cases according to our protocol for stent-assisted coiling. In patients who were poor responders to clopidogrel, as indicated by the VerifyNow P2Y12 assay, cilostazol was added to the treatment regimen.
Fill-and-tunnel technique
The femoral artery was first accessed using a 6 Fr 80 cm long Shuttle sheath (Cook, Bloomington, IN, USA), and a 6 F Envoy guiding catheter (Cordis, Miami Lakes, FL, USA) was navigated into the distal second segment of the affected VA. A microcatheter was navigated to a branch of the posterior cerebral artery using a guidewire, which was exchanged with a 300-cm-long exchange wire. The microcatheter was retrieved, and a self-expandable stent (Neuroform 3; Boston Scientific, Fremont, CA) was advanced over the prepositioned exchange wire and positioned to cover the entire dissection segment and left undeployed. The appropriate stent size was selected (available diameters were 3.0–4.5 mm and lengths were 15–30 mm) so the stent diameter was 0.5 mm larger than the parent vessel diameter and the ends of the device would extend at least 5 mm beyond the neck of the aneurysm on each side. A microcatheter for coil delivery was placed into the aneurysm sac using a guidewire and the coiling began. Because the coil delivery catheter was not jailed to the vessel wall, it remained freely maneuverable during the procedure and permitted circumferential coil packing. The stent was fully deployed when the homogeneous coil was properly packed in the sac or flow stagnation of the parent artery was detected. If the patency of the parent artery was not secured on a control angiogram, placement of the overlapping stents or ballooning within a stent could be easily attempted using the prepositioned exchange wire. Alternatively, in the event that the coil packing density was unsatisfactory on a control angiography, coiling could be continued using the jailed microcatheter because a coil-delivery catheter will be jailed naturally just after the first stenting. In this case, a second stent was positioned slightly proximal to the first stent just before additional coiling and left undeployed. The second stent was fully deployed when dense coil packing was achieved, and it allowed for the correction of possible coil prolapse by pushing the coil loop back into the sac or by sticking it between the two stents. The procedure is shown in Figures 1 and 2.
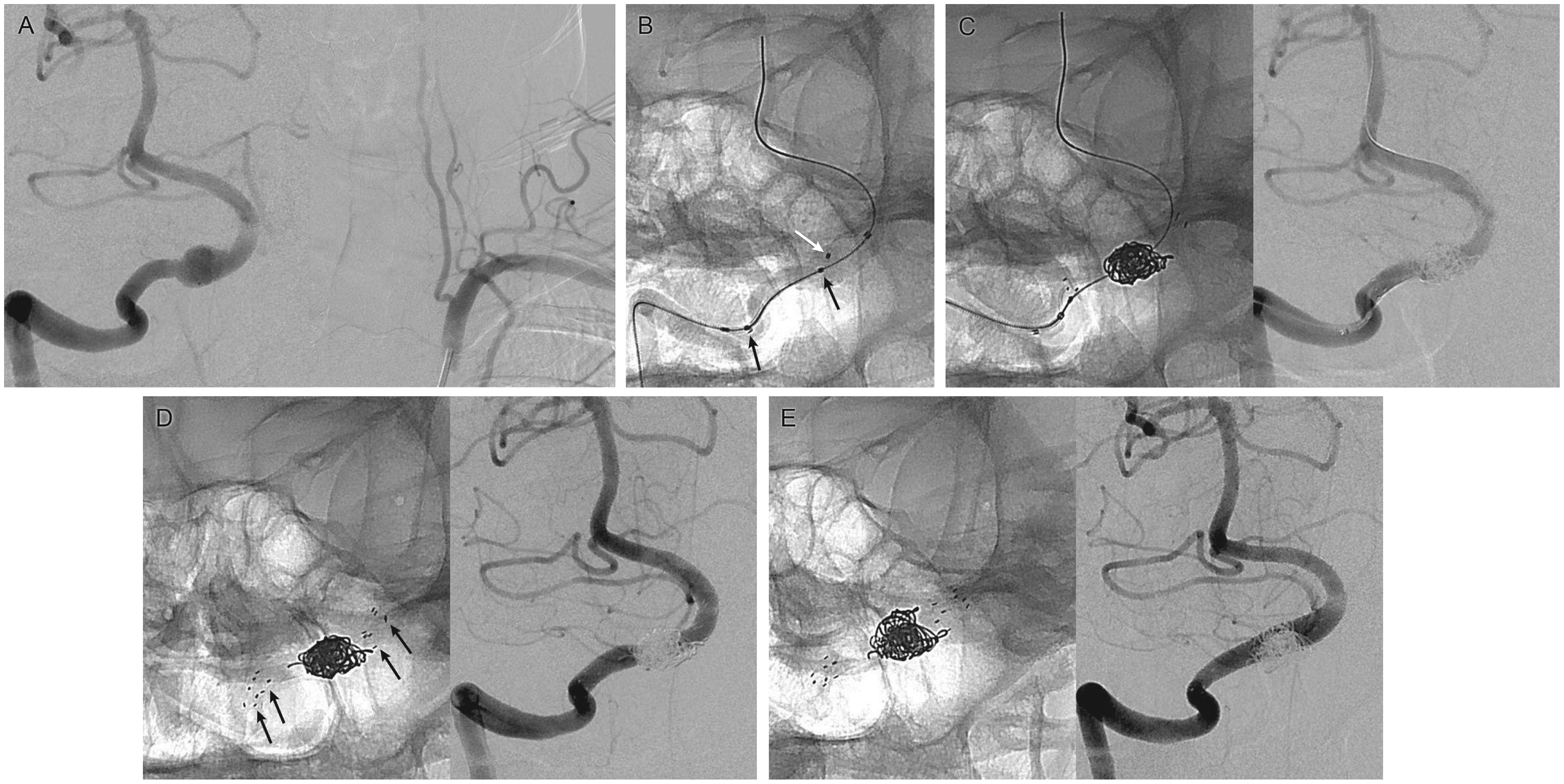
Patient 7. Serial schematic illustrations and angiographic images of whole tunneling technique procedure. (a) Right vertebral artery angiogram demonstrating a fusiform vertebral artery dissecting aneurysm with ipsilateral dominance. (b) The Neuroform 3 stent is first advanced over the prepositioned exchange wire, and positioned to cover the entire segment of the dissection, and left undeployed. A microcatheter for coil delivery is placed into the aneurysm sac using a guidewire. (c) Circumferential coil packing continues until homogeneous coil packing in the sac is achieved or the flow stagnation of the parent artery is detected. (d) The stent is fully deployed, and it allows arterial wall reconstruction materialized by the stent constraining the coil mesh inside the sac. (e) Immediate postprocedure angiogram showing complete obliteration of the aneurysmal dilatation with a patent parent artery. Patient 2. (a) Right and left vertebral artery angiograms demonstrating a fusiform aneurysm of the right distal vertebral artery with ipsilateral dominance. (b) Unsubtracted X-ray (same projection as Figure 2(a)) showing the coil delivery microcatheter tip (white arrow) inside the aneurysm sac. The nondeployed stent (black arrows) is still within its delivery catheter. (c) Unsubtracted (left) and subtracted (right) images acquired immediately after a circumferential coil packing and first stent deployment reveal an unsatisfactory packing density. (d) Unsubtracted (left) and subtracted (right) images obtained finally after additional coiling through the jailed microcatheter and second stent deployment demonstrate complete obliteration of the aneurysm with a well-preserved parent artery. Black arrows indicate radiopaque markers of the two overlapping Neuroform 3 stents. (e) The 13-month follow-up angiogram demonstrating complete obliteration of the aneurysm sac with smooth reconstruction of the involved segment of the right vertebral artery.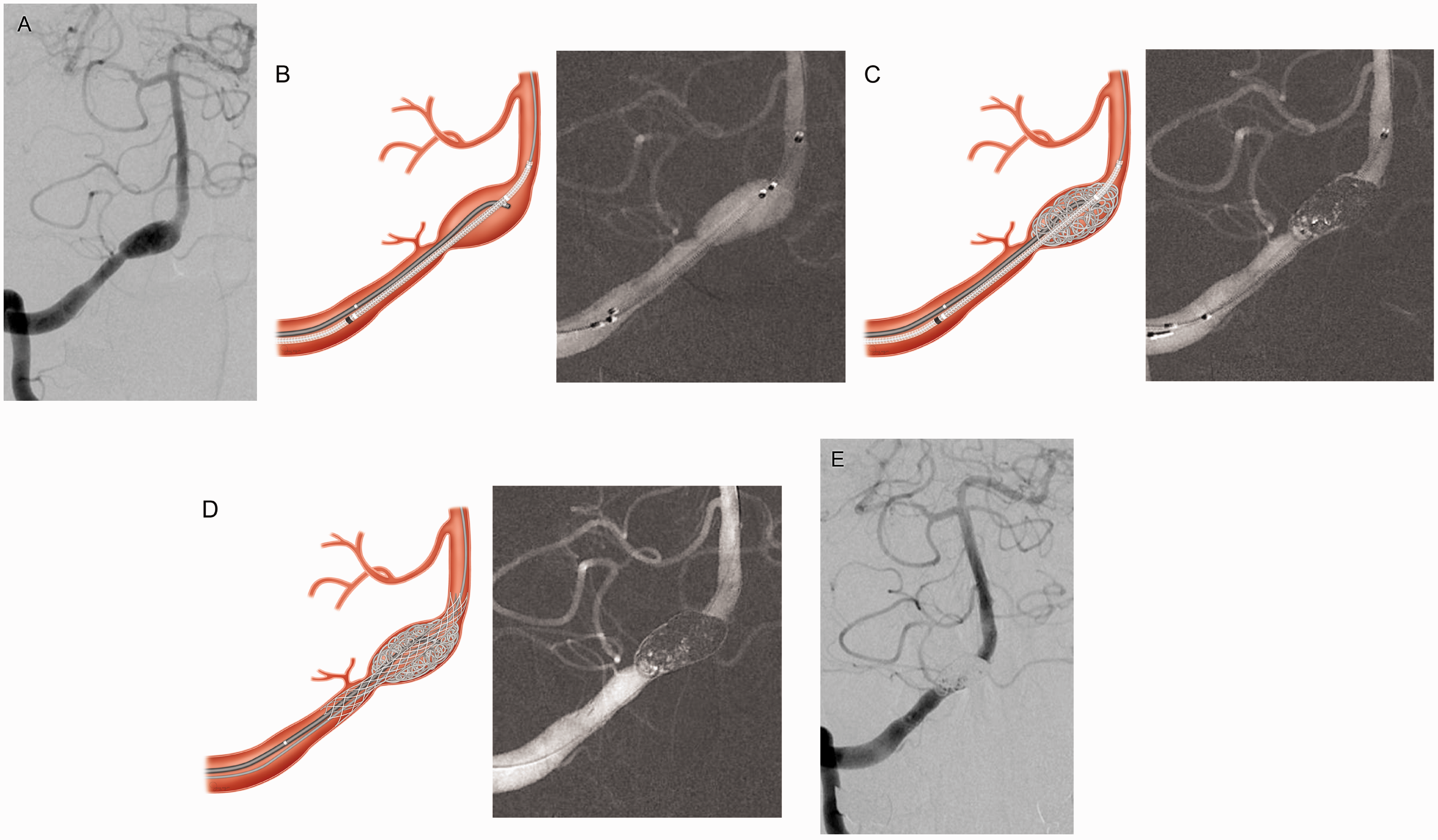
Analysis
Immediate and follow-up angiographic results were categorized into three groups based on the Raymond classification. 16 Recanalization was defined as the worsening of a classification: complete occlusion to neck remnant, neck remnant to aneurysm remnant, or complete occlusion to aneurysm remnant. Significant in-stent stenosis was defined as a greater than 50% narrowing or complete occlusion of the parent vessel at the time of follow-up. Radiologic assessments were conducted by two independent blinded authors (J.K.K. and T.H.L.) with 10 to 15 years of experience in neurointervention. Clinical results were assessed upon discharge from the hospital, or at the last clinical visit, using the modified Rankin Scale (mRS). Complications were defined as all adverse events related to the procedure and were evaluated retrospectively using medical and operative reports.
Results
Patient characteristics and treatment outcomes of tunneling technique for a fusiform VADA.
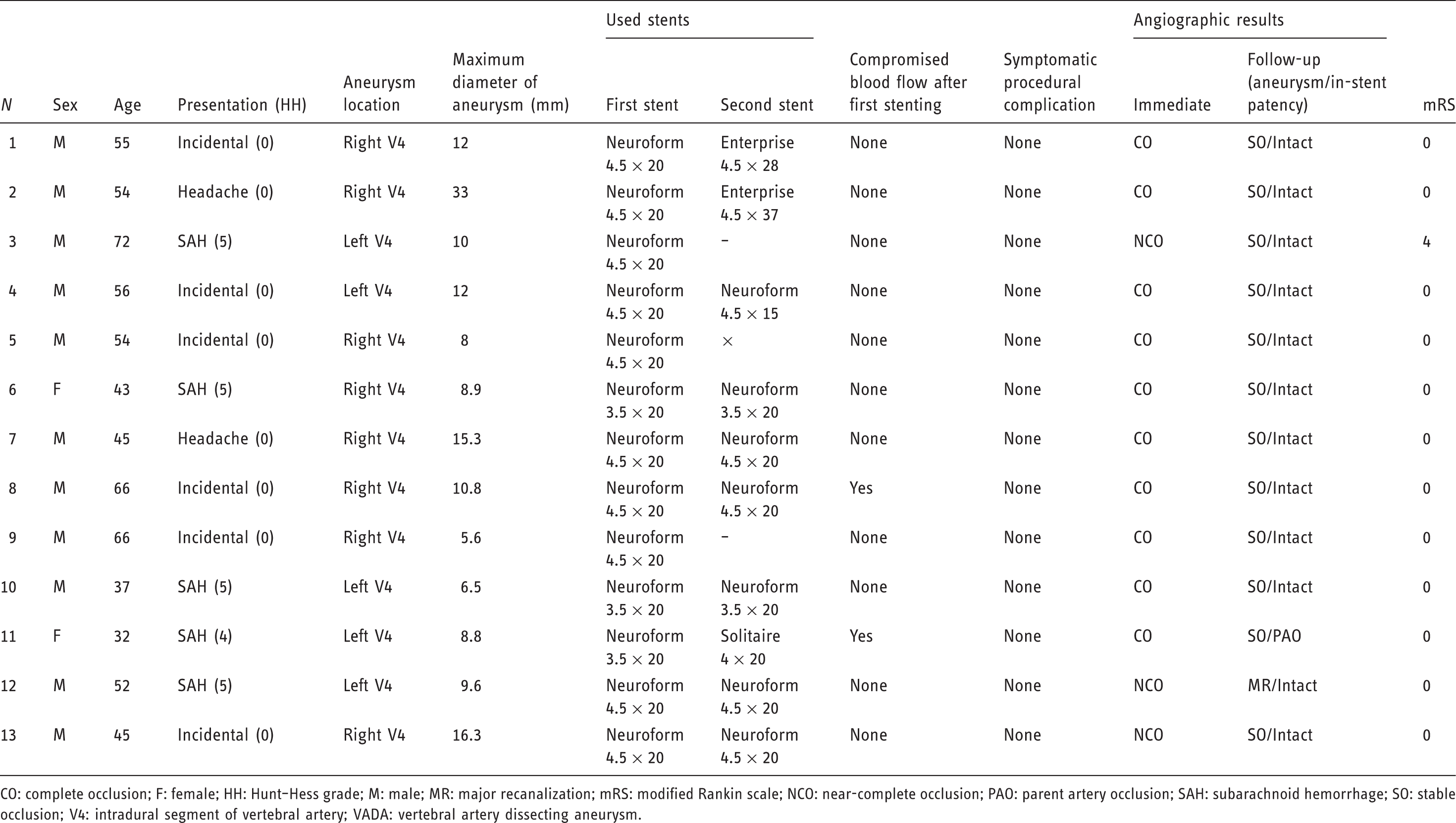
CO: complete occlusion; F: female; HH: Hunt–Hess grade; M: male; MR: major recanalization; mRS: modified Rankin scale; NCO: near-complete occlusion; PAO: parent artery occlusion; SAH: subarachnoid hemorrhage; SO: stable occlusion; V4: intradural segment of vertebral artery; VADA: vertebral artery dissecting aneurysm.
FT using coils and stents was technically successful in all 13 VADAs. Three aneurysms were treated with a single stent and the remaining 10 aneurysms required double-stent placement (stent-within-stent). A Neuroform 3 stent was chosen as the first stent in all cases. In the two cases in which compromised blood flow was recognized immediately after the first stenting, an in-stent-balloon angioplasty was performed with tirofiban injection (Figure 3). Well-preserved flow of the parent arteries was confirmed at the end of each procedure. All procedure times were an average of 1.5 hours. No procedure-related symptomatic complication occurred in any patient, and the 30-day major adverse events (major stroke and death) rate was 0%.
Patient 8. (a) Right and left vertebral artery angiograms demonstrating a fusiform aneurysm of the right distal vertebral artery with ipsilateral dominance. (b) Unsubtracted (left) and subtracted (right) images obtained immediately after the first stenting show a compromised distal blood flow. (c) Unsubtracted (left) and subtracted (right) images obtained finally after in-stent-balloon angioplasty with tirofiban injection and second stent deployment demonstrate complete obliteration of the aneurysm with a well-preserved parent artery.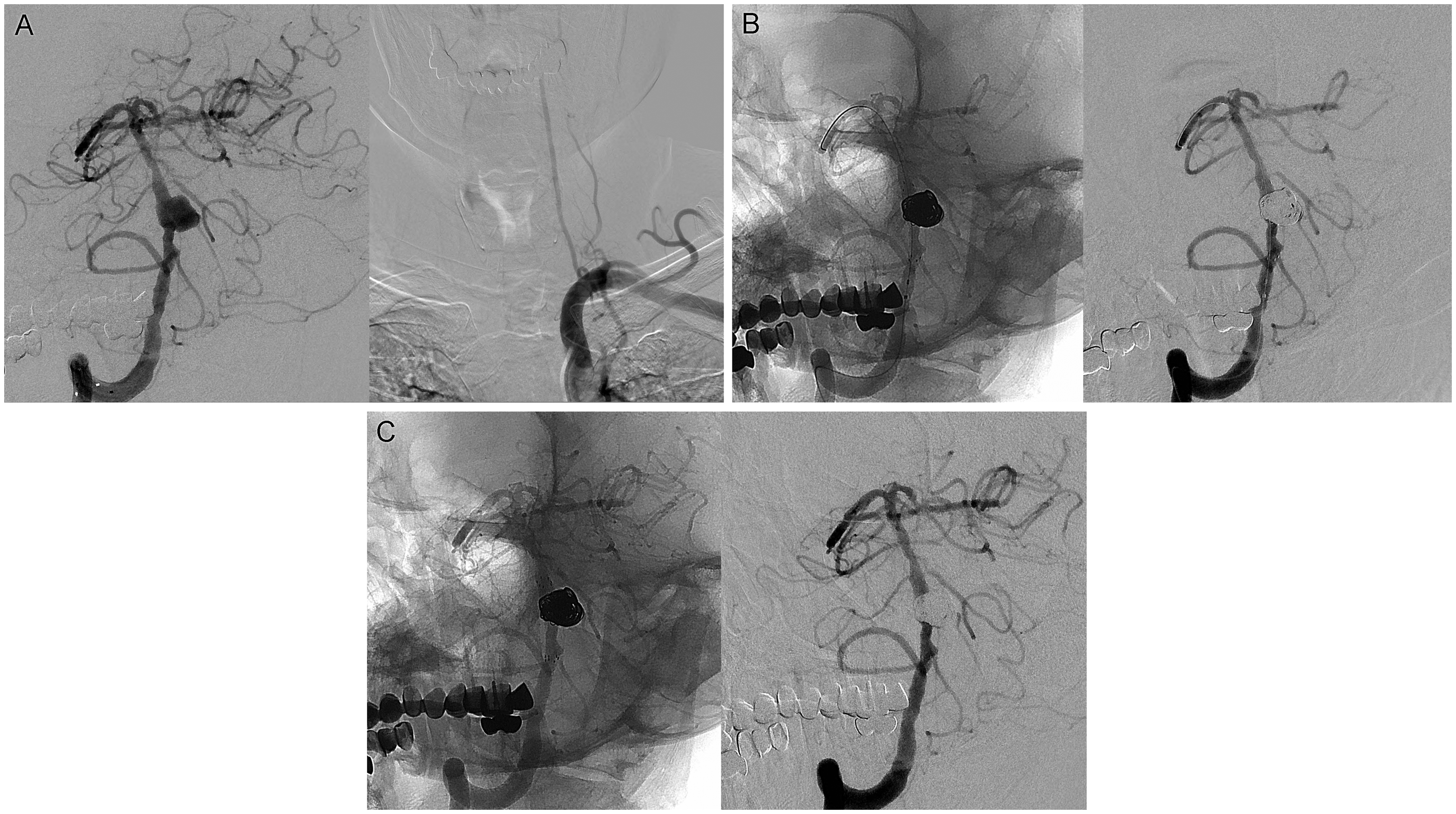
Immediate postprocedural angiographic results included complete occlusion in 10 cases (76.9%) and near-complete occlusion in three patients (23.1%). Conventional angiography follow-up was obtained in 11 patients at intervals ranging from two to 24 months (mean, 9.1 months). Ten of the 11 aneurysms revealed a stable occlusion. One patient who had suffered an SAH showed a major recanalization in an eight-month follow-up angiography. Additional flow diversion with a (PED, Covidien, Irvine, CA, USA) was performed successfully (Patient 12). Parent arteries with stenting were patent with no evidence of definite intimal hyperplasia or in-stent stenosis, except in one case. This patient had asymptomatic in-stent occlusion that was discovered six months later on routine follow-up angiography. Additional therapy was declined after sufficient collaterals had been confirmed (Figure 4). In five patients with SAH, one patient was discharged with an mRS score of 4 as a direct consequence of the initial SAH. The remaining 12 patients had excellent clinical outcomes (mRS 0) without rebleeding during the follow-up period of six to 28 months (mean, 19.0 months).
Patient 11. (a) Initial right and left vertebral angiograms reveal a ruptured dissecting aneurysm on the left distal vertebral artery and a hypoplasia on the right distal vertebral artery (black arrows). (b) Unsubtracted (left) and subtracted (right) images obtained finally after stent-assisted coiling demonstrate complete obliteration of the aneurysm with a preserved parent artery. (c) The six-month routine follow-up angiograms show early termination of the left vertebral artery at the posterior inferior cerebellar artery, indicating in-stent occlusion and an enlargement of the right distal vertebral artery (black arrows) with a sufficient distal blood flow.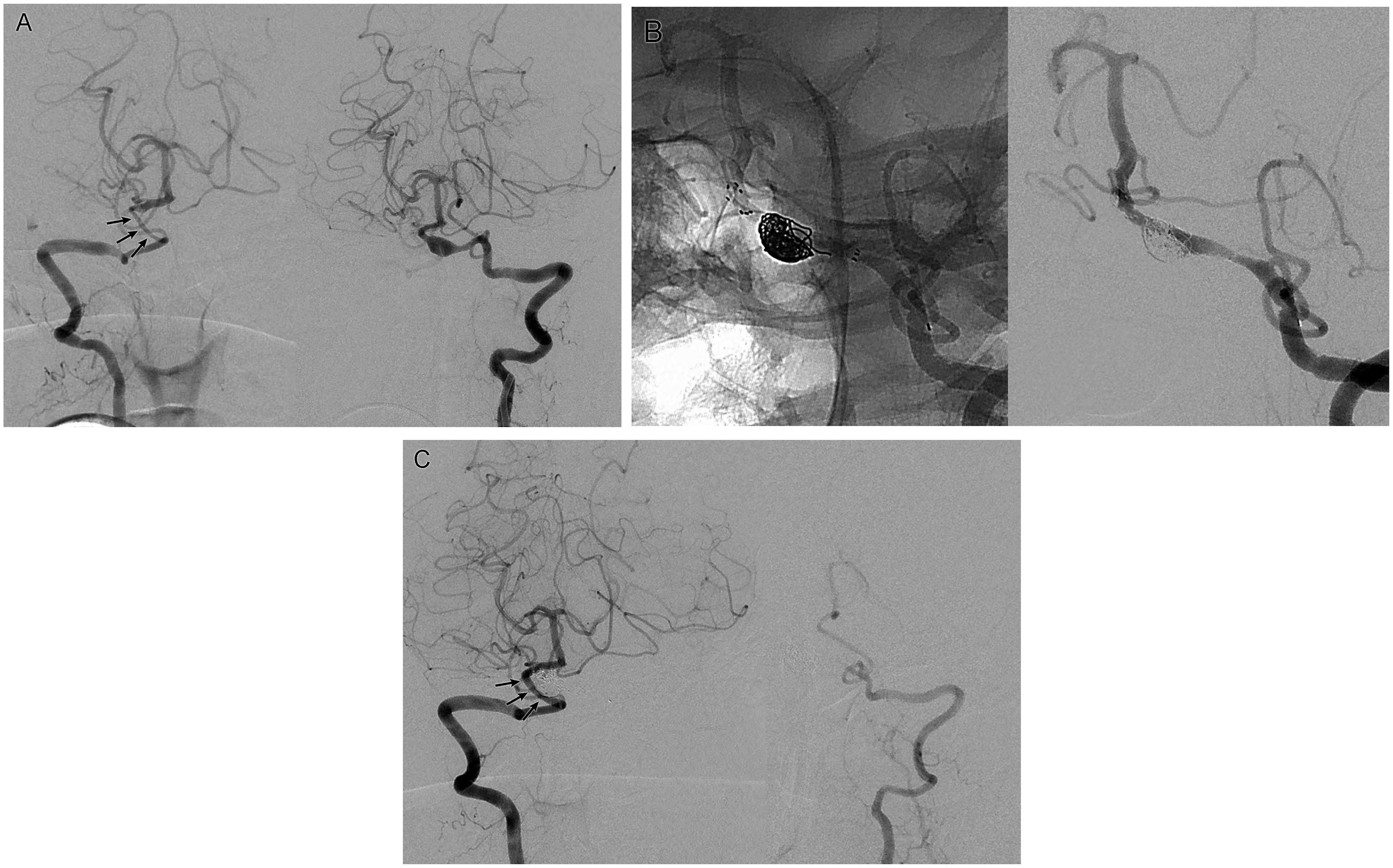
Discussion
It is technically challenging to treat a fusiform intracranial aneurysm without a defined neck region excluding from the parent artery. This obstinate situation is often encountered in VADAs. Internal trapping of the dilated segment of the parent artery is one of the most reliable techniques to prevent rupture or rebleeding.3–6 However, this procedure is not suitable for treating fusiform VADAs involving the dominant VA with poor collaterals. With recent improvements in endovascular devices, reconstructive treatments using stents and/or coils have increasingly emerged in these special conditions.6–9,11,12 To date, various endovascular techniques have been applied for the simultaneous preservation of the parent artery and aneurysm exclusion from the circulation, including stent-assisted coiling (SAC), the use of stents alone, flow diversion, and covered stent placement.3–6,12,14,17–24
Covered stents have been proposed but their placement is limited by their inflexibility, insufficient data for long-term efficacy, and occlusion of the side branches and perforators arising from the covered segment, which may result in a catastrophic ischemic event.18,20,23
Flow diversion using high density and low porosity to modify the flow between the parent vessel and the aneurysmal sac has also been proposed. In this technique, alteration of flow induces embolization of the aneurysm with reconstruction of the parent vessel by the device.25,26 This is often the goal when treating fusiform and giant aneurysms. However, patients with posterior circulation aneurysms are at a higher risk for ischemia, particularly perforator infarction.27,28 A recent study demonstrated poor outcomes for patients presenting with large or giant fusiform aneurysms treated with flow diverters. 28 Nevertheless, use of the flow diverter has been shown to be an attractive alternative for the treatment of dissecting aneurysms. In the present study, flow diverters were excluded from consideration because they were “off-label” for insurance in the majority of our series.
The use of stents that are not specifically designed for flow diversion alone without coils is also an attractive option for the treatment of fusiform aneurysms. Stent-alone treatments can alter hemodynamics and create favorable flow conditions to enhance thrombosis.12,29 Placement of multiple stents across the neck of an aneurysm has been shown angiographically to profoundly reduce aneurysmal inflow to the aneurysm. 22 Although a couple of case series have reported good results, most of them dealt with unruptured VADAs. Since immediate aneurysm obliteration is often not accomplished, even in multiple overlapping stents, these techniques may be insufficient to prevent rebleeding of a ruptured VADA.
SAC seems to be the most widely used technique in the world as a reconstructive option for ruptured VADAs.2,5,7,9–11 When combined with the placement of coils within the aneurysm, stents allow for greater packing density within the aneurysmal sac, serve as a scaffold for endothelial growth, and support coils within wide-necked aneurysms to preserve the patency of the parent vessel. Nevertheless, recurrence or rebleeding of VADAs after SAC has often been reported. 30 Because of the very fragile nature of the ruptured aneurysm wall, the lesion’s typical irregular or fusiform contour, and/or branch vessel involvement, it is sometimes difficult to completely obliterate the VADA, even using conventional SAC, which may affect recurrence after embolization. When SAC is performed for the treatment of intracranial aneurysms, the technique of catheter tip placement into the aneurysm sac can be divided into two methods, the catheter jailing technique and through-the-stent’s-strut technique.31,32 If these two methods were applied to fusiform aneurysms like VADAs, it would be difficult to achieve satisfactory results because of the following drawbacks. First, since the catheter jailing technique does not offer a possibility to modify the microcatheter position within an aneurysm, the circumferential coil packing essential to the treatment of fusiform aneurysms is further limited. Second, it does not permit a passive kick-back movement of the coil delivery catheter during dense coil packing, which results in a higher risk of coil perforation. Third, since coil herniation through the stent strut into the parent artery cannot be observed during the procedure, these conventional techniques do not guarantee the patency of the parent artery. As a novel method for overcoming these drawbacks of the conventional techniques, FT was used to treat VADAs, including fusiform intracranial aneurysms at other locations, and excellent clinical and angiographic results were observed. FT has several advantages compared with the previous techniques. Unlike previous techniques requiring coil delivery microcatheter to be fixed in the aneurysm sac, FT provides the chance for circumferential coil packing while maintaining a higher degree of microcatheter flexibility and maneuverability during coil deployment. In other words, this technique gives the practitioner a much broader range of working positions, facilitating a compartmental approach. This can be critical to matching the coil mass geometry with that of the lesion, enabling optimum packing while retaining the control needed to maintain the patency of the parent artery. As a result, this technique improves the packing density in the aneurysms and protects from rebleeding. We prefer the use of an open-cell stent, specifically the Neuroform 3 Stent Delivery System (previous version), in FT for the following reasons. Placement of the overlapping stents or ballooning within a stent requires fewer steps because the microwire is left in place for loading subsequent stents or balloons, providing a key advantage over the Neuroform 3 design. In addition, this microwire can be used as a guidewire, which allows quick access to additional devices when distal complications occur.
In our study, 13 patients with VADAs were identified over the past four years. Endovascular reconstruction using FT was successfully performed, achieving complete occlusion (10/13) and near-complete occlusion (3/13). No procedure-related complications occurred in any patient. There were no delayed thromboembolic or hemorrhagic complications during the follow-up period (mean, 19 months). Angiographic follow-up (mean, 9.1 months) showed stable occlusion in 90.9% (10/11) and asymptomatic in-stent occlusion in one patient (9.1%, 1/11). At the end of the observation period (mean, 19 months), all patients had excellent clinical outcomes (mRS 0, 92.3%, 12/13), except one (mRS 4), resulting from poor preoperative status. According to a recent meta-analysis of reconstructive treatments for VADAs, the immediate occlusion rate was 53.0% and the long-term occlusion rate was 81.0%. 33 Perioperative morbidity and mortality were 4.0% and 92% of patients achieved good long-term clinical outcomes. The angiographic recurrence rate was 5.0%, with a retreatment rate of 3.0%. Although the small number of our cases makes direct comparison difficult, the present study showed comparable or superior results in most areas compared to previous ones, especially in angiographic results. All kinds of device-assisted coiling techniques can lead to prolonged procedure times and complex processes. However, FT seems to provide high packing density, preservation of the parent artery patency, and also shortened overall procedure time. To the best of our knowledge, this is the first description of the use of FT. FT might be effective for the endovascular reconstructive treatment of VADAs with ipsilateral dominance, which is difficult to treat using conventional methods.
Limitations
Our study had some limitations. First, the number of patients enrolled in this study was too small to evaluate the statistical significance of our procedure. Second, it was hard to make an assessment of coil compaction and in-stent stenosis because the tracking period was not very long. Third, some important points, such as the proper timing of stent deployment and the optimal packing density, were ambiguous. Therefore, further studies with a larger patient cohort and a longer follow-up period are needed to elucidate the efficacy and longevity of this treatment.
Conclusions
This retrospective study demonstrated that endovascular reconstruction using FT was a technically safe, feasible, and clinically effective treatment method for fusiform VADAs with ipsilateral dominance. Further studies with more patients and a longer follow-up period will be helpful to elucidate the efficacy and longevity of this treatment.
Footnotes
Acknowledgment
Author contributions include the following: J.K.K. and T.H.L. were primarily responsible for study design, collecting data and drafting the manuscript. C.H.C. and S.W.L. contributed significantly to this report by critically reading the manuscript and providing many helpful suggestions. All authors read and approved this manuscript to be submitted for publication to this journal.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a 2018 Pusan National University Research Grant.