
Abstract
Background
Emergent large vessel occlusive (ELVO) stroke secondary to underlying carotid occlusive disease is frequently encountered in endovascular ischemic stroke therapy and trials. Up to 29% of all cerebral vascular accidents are attributed to severe carotid occlusive disease, and recent interventional trials have demonstrated this occurrence in 18.6–32.2% of ELVO stroke. We present a novel technique using the stent retriever guide wire to expedite angioplasty and/or stent placement for associated carotid occlusive disease during mechanical thrombectomy of ELVO stroke. This technique utilizes the “waiting time” during stent retriever integration within the thrombus as an opportunity to initiate revascularization of the cervical carotid, using the deployed stent retriever guidewire as an ad hoc rapid exchange wire while the stentriever serves as a potential surrogate distal embolic protection device. We present 23 cases using this novel endovascular approach, which we have called the single-cross technique, as the cervical lesion is only traversed once during therapy.
Methods
A case series of 23 consecutive patients who underwent a novel endovascular technique for treating tandem ICA origin and intracranial occlusive lesions is presented. Endpoints measured were time to re-perfusion, rates of intracranial hemorrhage and clinical outcomes (mRS at 30 and 90 days).
Results
Average procedure time for revascularizing both the carotid and intracranial lesions was 52 min. A symptomatic ICH rate of 9% was observed. Seventy-four percent of patients had an mRS of 0–2 at follow-up.
Conclusions
The single-cross technique appears to be a safe and effective option for treating tandem occlusive lesions in the setting of ELVO.
Introduction
Recent outcomes datamized controlled trials demonstrated clear efficacy and benefit of mechanical thrombectomy in emergent large vessel occlusive (ELVO) stroke.1–7 Patients with hemodynamically significant carotid occlusive disease were frequently excluded from ELVO trials, 8 as they represent a more complex disease process, potentially requiring multiple concurrent interventions which could complicate outcome analysis.
While data from the early thrombectomy trials are limited, tandem lesions were encountered in 17% of enrolled patients in the endovascular treatment for small core and proximal occlusion ischemic stroke trial, with similar clinical outcomes to their non-tandem counterparts, 9 although the authors did acknowledge a high variability in the treatment of the tandem lesions patients and commented on the need for future studies. The highly effective reperfusion evaluated in multiple endovascular stroke trials meta-analysis suggested that patients with anterior circulation tandem lesions and ELVO experienced similar benefits when compared to patients with ELVO alone, although the former group of patients was poorly represented and conclusive recommendations could not be made on the basis of the available studies. 10
The coexistence of severe extracranial carotid disease and tandem intracranial thrombosis is a highly complex disease process and presents the neurointerventionalist with a therapeutic dilemma. The primary goal is to recanalize the occluded intracranial arterial tree. However, even if definitive treatment (stent or endarterectomy) of the associated cervical lesion can be deferred, with initial navigation solely to permit the intracranial thrombectomy procedure (restoring collateral flow), a cervical flow limiting stenosis or occlusion creates therapeutic issues which may increase procedural time and complications.
Options for treatment of intracranial ELVO with concomitant cervical occlusive disease include:
1. Angioplasty and/or stenting of cervical lesion first followed by completion of intracranial thrombectomy procedure 2. Intracranial thrombectomy first (if able to navigate the cervical carotid occlusive disease) with revascularization of cervical carotid following completion of the intracranial procedure 3. Intracranial thrombectomy from another approach (e.g. retrograde via a PCOM, via ACOM) 4. Intracranial thrombectomy alone, with medical management of the cervical carotid occlusive disease.
Acute stent placement in the extracranial carotid artery has been shown to have an acceptable risk profile in the management of tandem lesions.
11
A recent meta-analysis of data (largely retrospective) of ELVO stroke with tandem occlusions revealed similar clinical outcomes in patients undergoing initial treatment of their intracranial versus cervical disease.
12
While each option may have relative benefits and drawbacks, it may not be feasible to defer treatment of the cervical carotid occlusive disease, for fear of recurrent thromboembolic event or hypoperfusion injury.
We propose a novel and efficient technique capitalizing on the “waiting time” required for clot integration into a stent retriever. This technique allows an opportunity to utilize the deployed stent retriever wire not only as an ad hoc rapid exchange guidewire, but also to serve as surrogate distal embolic protection device (EPD) during passage of a balloon guide catheter (BCG) or large bore catheter beyond the cervical lesion. This “single-cross” technique obviates the need for multiple passes of a wire through a symptomatic cervical lesion, reducing the potential for dissections and/or further distal emboli of symptomatic plaque.
Technique
After a standard diagnostic arteriogram is performed and the target lesion(s) is identified, an exchange is performed to bring a large diameter 8–9 French long sheath into the common carotid artery (CCA) (e.g. Arrowflex® Teleflex, Shuttle® Cook Inc.). Traditionally, the use of a long sheath is required for carotid stent deployment, if deemed necessary. More recently, advancements with larger-bore BGCs have reduced the need for long sheaths, as they have sufficient lumen diameters to accommodate carotid stenting systems. The use long sheaths may still be advantageous in cases of tortuous anatomy for support purposes. Figure 1 summarizes the workflow.
Procedural flow chart summarizing the single-cross technique.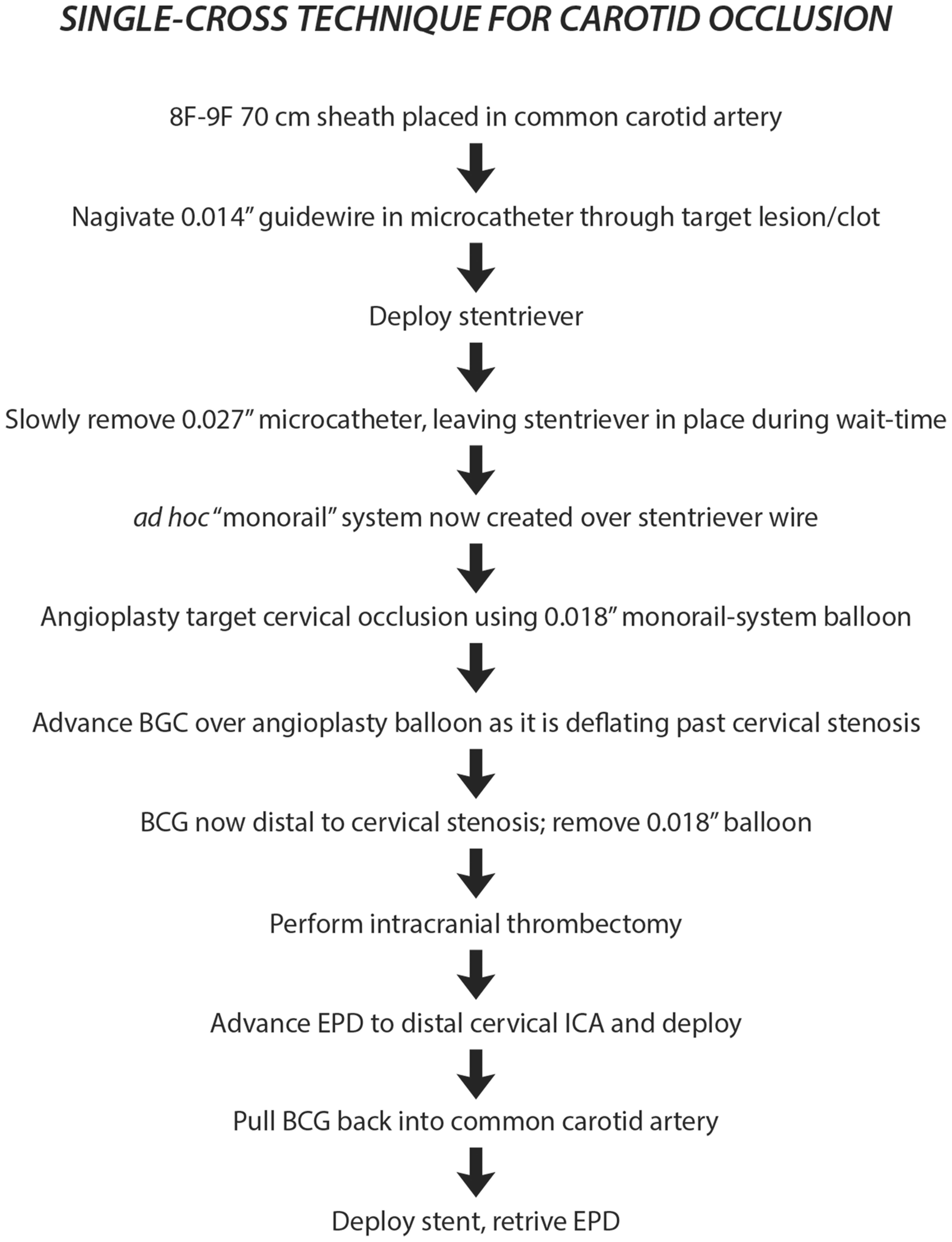
At this point, a stent retriever compatible microcatheter (e.g. Marksman™ Medtronic, Orion™ Medtronic, Excelsior XT-27® Stryker Neurovascular) is advanced through a 8-9F BGC (with or without long sheath), and navigated over a 0.14″ microwire (e.g. Transend® EX, Stryker Neurovascular) to the petrous carotid and a gentle microcatheter injection is performed to document intraluminal placement of the microcatheter (particularly in cases of carotid occlusion), and to assess clot burden/location to target stent retriever deployment. After the intracranial anatomy was defined, the target lesion (MCA and/or intracranial ICA lesion) is crossed using standard over-the-wire technique, and a microcatheter injection is repeated to document appropriate intraluminal placement distal to the clot. One of the longer stent retrievers (i.e. 4 × 40 mm Solitaire™ Medtronic, 4 × 30 mm Trevo™ Stryker Neurovascular) is then deployed in routine fashion, with care taken to engage not only the MCA thrombus, but also to cover the ACA and PCOM origins.
During the “wait period,” typically 5 min or so, to allow for clot integration and brain reperfusion, attention is turned to the carotid lesion. The microcatheter is gently removed from the patient, leaving the stent retriever in place. The radial force of the stent retriever will stabilize its position within the intracranial vasculature during microcatheter removal. A 0.018″ rapid exchange system balloon (e.g. Sterling™ Boston Scientific) is advanced over the stent retriever wire to the target cervical carotid lesion and angioplasty is performed. After the angioplasty is performed, the BGC is advanced over the deflated balloon into the high cervical internal carotid region. This is an important and somewhat subtle technical nuance that is essential to the success of the procedure in our experience. Advancing the BGC during balloon deflation facilitates distal BGC placement by minimizing “mismatch” of the lumens and acts as a proxy introducer given its stiff proximal shaft. We have found that using longer length balloons (i.e. 40–60 mm length) ensures not only adequate coverage for carotid lesions of unknown length (in the case of carotid occlusions), but also facilitates distal placement of the BGC/large bore catheter.
Additionally, our experience has been that in all M1 segment MCA and intracranial ICA occlusions, the length of the stent retrievers will suffice to cover the anterior cerebral and posterior communicating artery origins, theoretically preventing embolization of large particulate and/or clot (associated with active carotid lesions) into these regions during angioplasty and passage of BGC/large bore catheter.
With distal placement of the BGC or large bore catheter, the thrombectomy procedure can proceed in standard fashion. Following removal of the stent retriever, and after achieving desired intracranial reperfusion, further assessment of the cervical carotid occlusive disease can be performed. Our preferred method is to advance a traditional carotid EPD (i.e. Emboshield® NAV 6 Abbott) through the BGC (still positioned in the high cervical ICA), and then deploy the EPD in the high cervical ICA, prior to retracting the BGC into the CCA. Deploying the EPD in this manner maintains access across the cervical lesion and eliminates “re-crossing” the lesion with the EPD wire. Of note, there is adequate wall apposition of the deployed EPD to render its position “stable” in the distal ICA during retraction of the BGC. If there is a concern about stability of the EPD, one could use commercially available exchange length EPD compatible wires (e.g. BareWire® workhorse, Abbott Vascular, USA).
With the EPD deployed in the distal cervical ICA, angiography and assessment of the post-angioplasty carotid lesion can now be performed through the BGC or long sheath. If there is residual flow limiting stenosis or high-risk features, further intervention (additional angioplasty, stent) can be performed over the EPD in traditional fashion.
There may be instances where balloon angioplasty or thrombectomy alone (with restoration of collateral flow) may suffice as the initial treatment, and this may not be apparent until after the thrombectomy. While the majority of tandem lesions do undergo stent placement at the cervical lesion (as in our technical note), meta-analysis of tandem lesions indicates no difference in outcomes with stenting versus angioplasty alone. 12 Additionally, this technique of deploying the EPD in the distal cervical ICA prior to retracting the BCG back across the ostial lesion protects against embolization of clot material that may be present between the vessel wall and the BCG.
Illustrative case
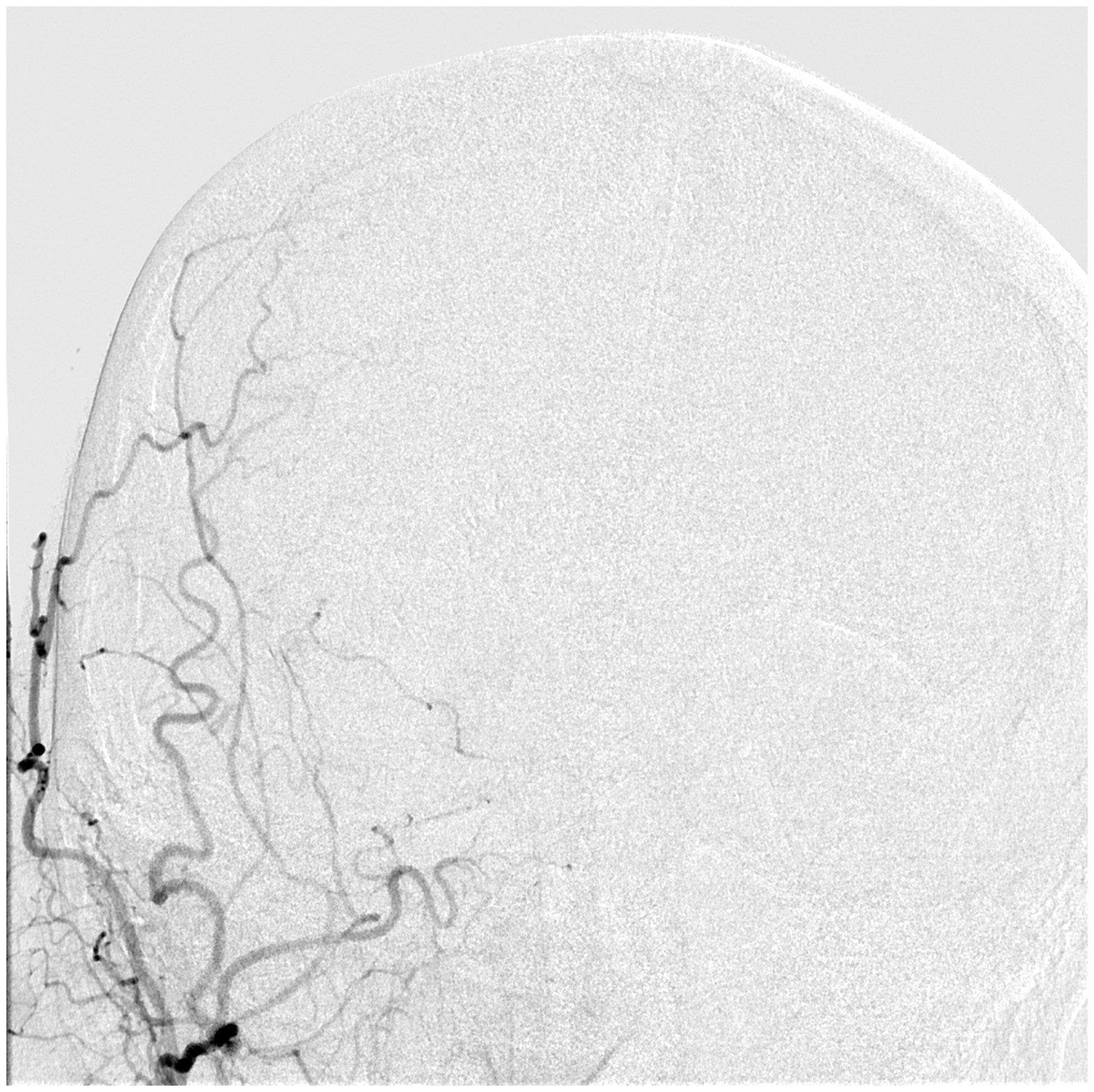
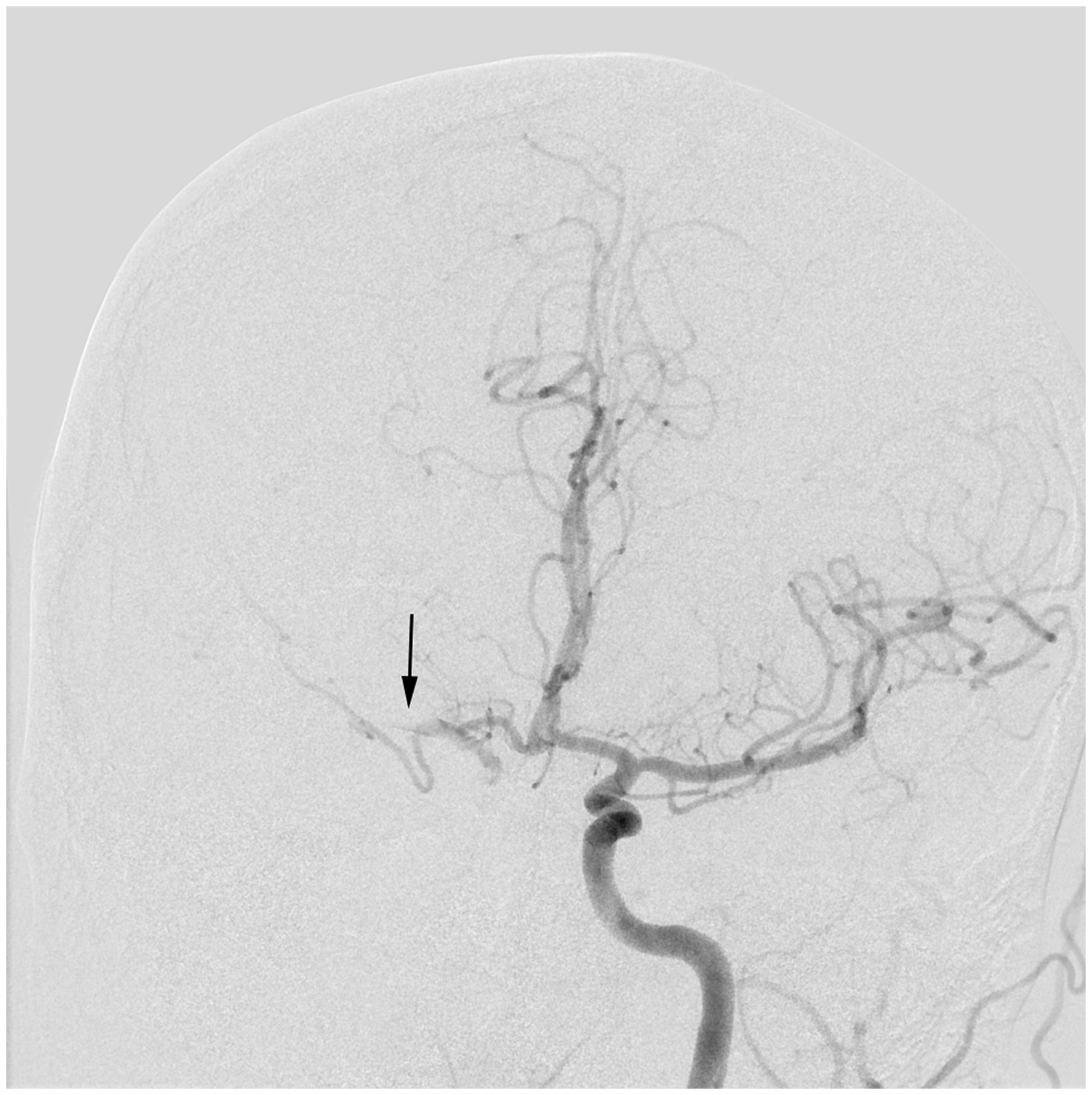
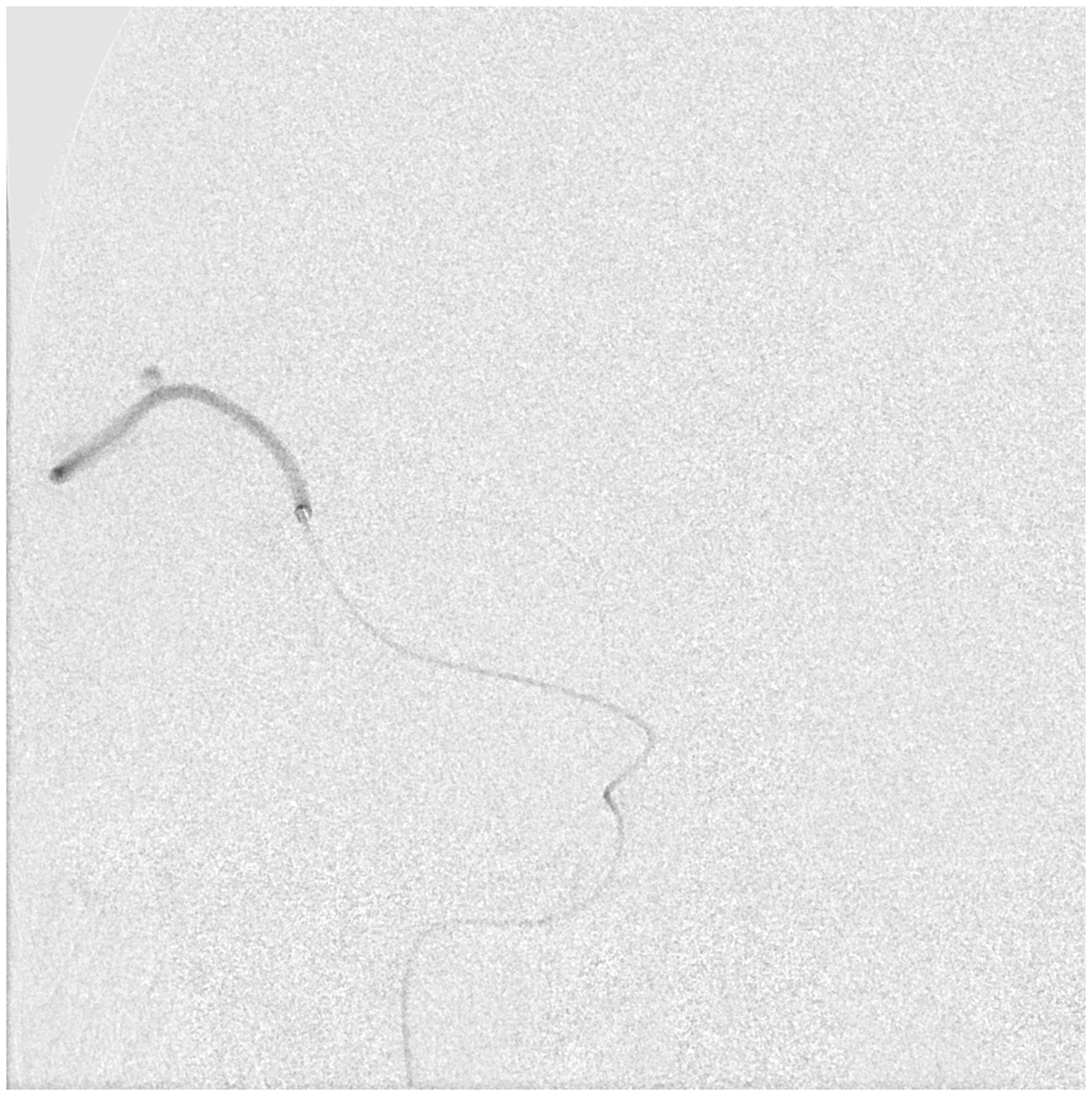
A patient in late 40s with a history of smoking and hypertension presented as a “wake up” stroke with dysarthria, dense left hemiplegia, and an initial NIHSS of 16. Given the unknown time of onset, the patient was not a candidate for intravenous tPA therapy. The patient had a non-contrast CT head demonstrating a “dense” right MCA sign and ASPECTS of 10. Emergent angiography demonstrated acute occlusion of cervical right ICA at the CCA bifurcation (Figure 2), typical of atherosclerotic disease, with no appreciable flow to the intracranial vasculature (Figure 3). Contralateral left carotid angiography revealed patent ACOM with collateral flow to the left ACA vascular territory, but with a distal embolus occluding the M1 segment of the right MCA vascular territory (Figure 4).
Right common carotid artery injection showing occlusion of the proximal RICA. Right common carotid artery injection showing no appreciable intracranial flow. Contralateral carotid angiogram demonstrating a patent ACom with R MCA occlusion.
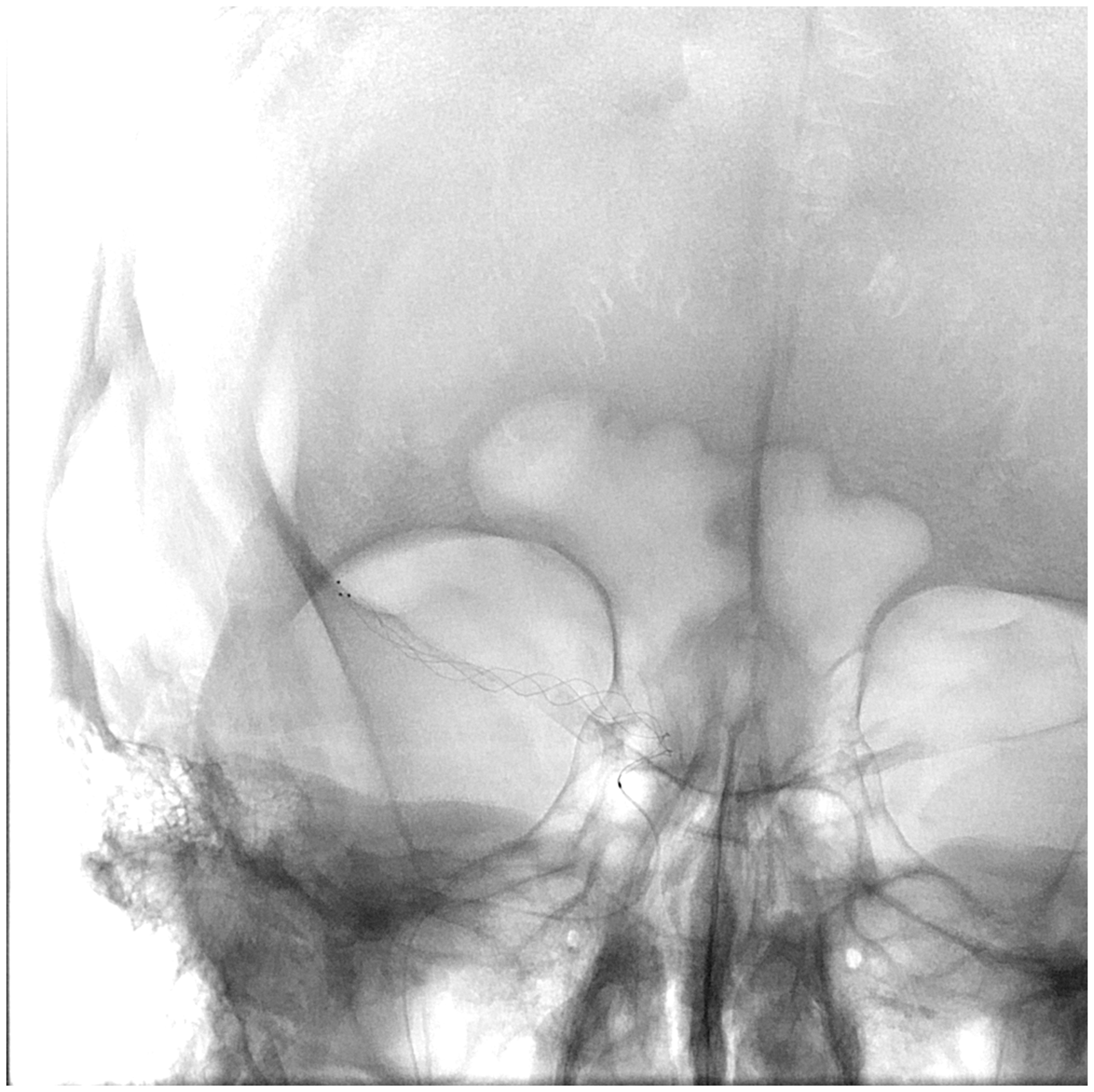
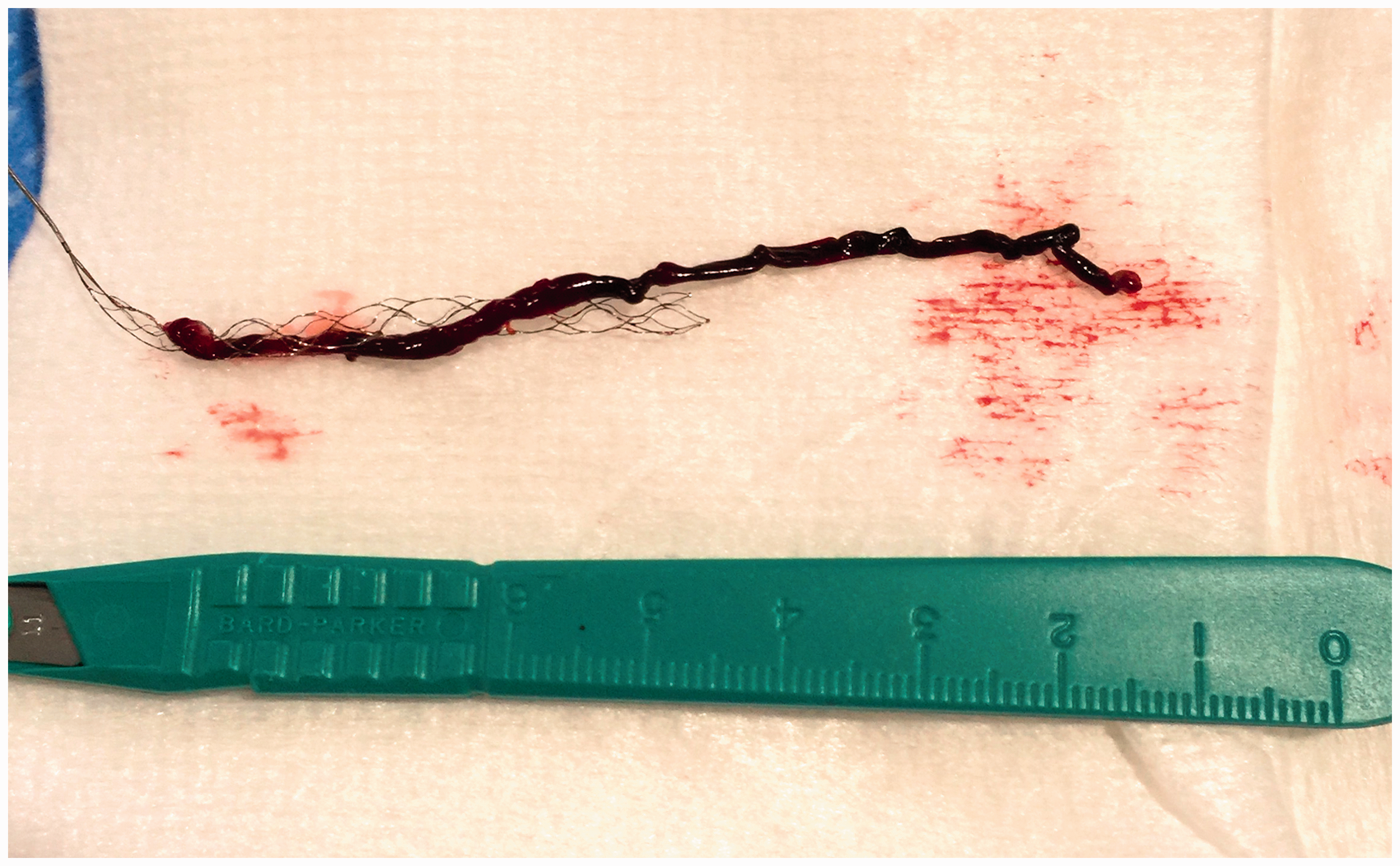
A 5-French diagnostic catheter was exchanged over a 0.035″ Rosen wire for an 8 F Arrowflex® sheath, which was positioned in the distal right CCA. An 8F BGC was then advanced to the tip of the long sheath. A 0.027″ microcatheter was then advanced over a 0.014″ microwire past the ICA occlusion into the cavernous ICA. Microcatheter injection confirmed placement within the cavernous ICA and occlusive thrombus within the M1 segment of the right MCA (Figure 5). The microcatheter was then advanced over the microwire past the thrombus into a dominant M2 branch of the MCA (Figure 6). A 4 × 30 mm Trevo® stent retriever mechanical thrombectomy device was then deployed across the M1 occlusion, with care taken to ensure coverage of the ACA and PCOM origins (Figure 7). The microcatheter was then removed, and a 4 × 60 mm Sterling™ balloon was advanced over the stent retriever wire and angioplasty at the ICA occlusion was performed (Figure 8). During balloon deflation, the BGC was advanced over the balloon into the upper cervical ICA (Figure 9). After the remainder of the 5 min “wait period,” the stent retriever was removed using temporary balloon occlusion technique and vigorous aspiration of the BGC. A large thrombus was successfully removed (Figure 10), and angiography through the BGC reveals restoration of normal flow (TICI 3) to the right MCA vascular territory (Figure 11). A large NAV
6
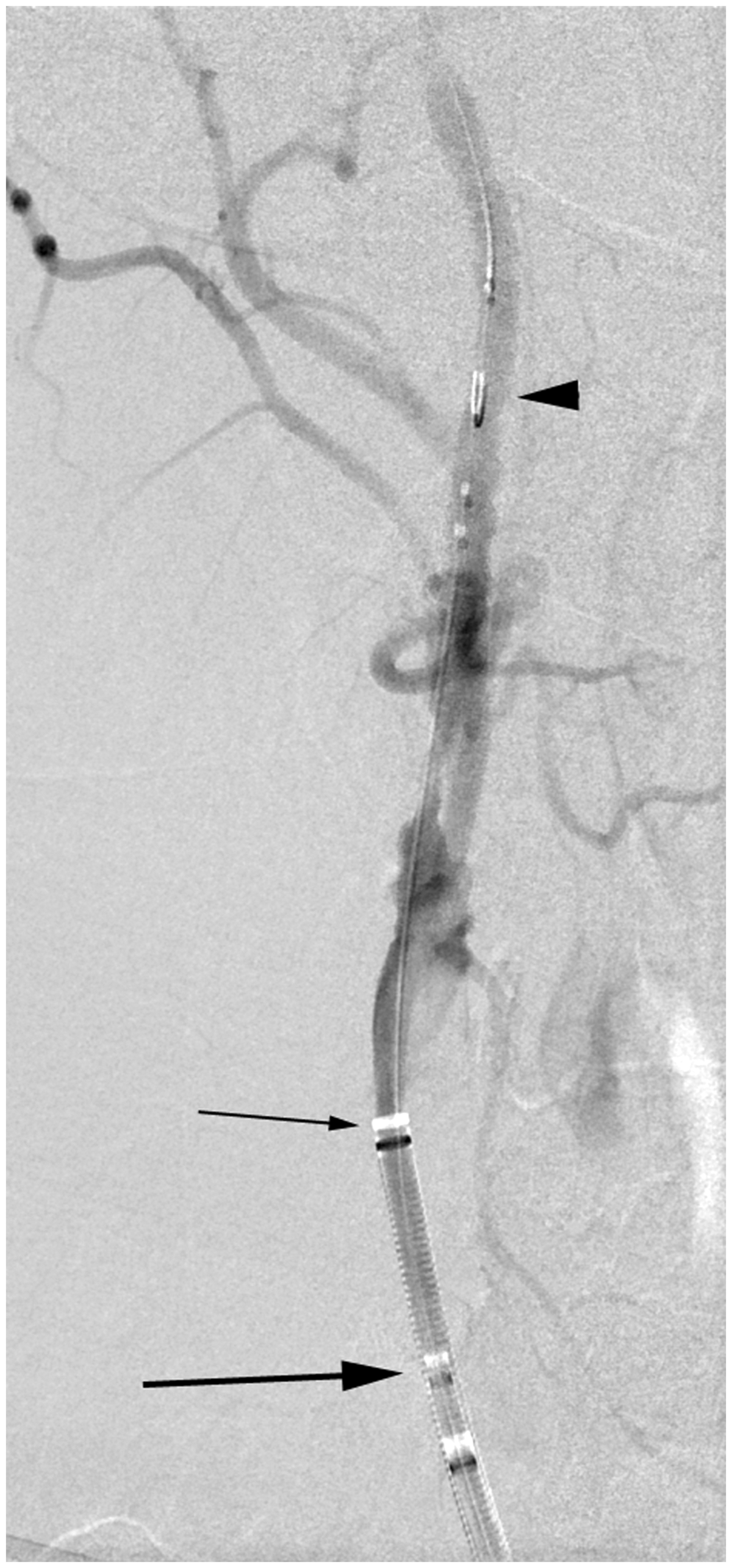
distal EPD device was then advanced through the BGC and positioned in the distal cervical ICA, followed by removal of the BGC (Figure 12). Angiography through the long sheath reveals irregular thrombus at the site of ICA occlusion, and thus the decision to proceed with stenting was deemed appropriate. A Carotid WALLSTENT™ (Boston Scientific, MA, USA) was then advanced over the EPD and deployed across the ICA stenosis and the stent was post-dilated with a 5 mm balloon (Figure 13).
Microcatheter angiogram from the right petrous ICA confirming MCA occlusion. Microwire angiogram from dominant M2. 4 × 30 mm Trevo® deployed across the M1 thrombus covering origins of the PCom and ACom arteries. 4 × 60 mm Sterling™ balloon was advanced over the stent retriever wire and angioplasty at the ICA occlusion was performed. During balloon deflation, the BGC was advanced over the balloon into the upper cervical ICA. Large thrombus was removed. TICI 3 flow through R MCA. A large NAV6 distal EPD device was then advanced through the BGC and positioned in the distal cervical ICA, followed by removal of the BGC. A Carotid WALLSTENT™ (Boston Scientific, MA, USA) was then advanced over the EPD and deployed across the ICA stenosis and the stent was post-dilated with a 5 mm balloon.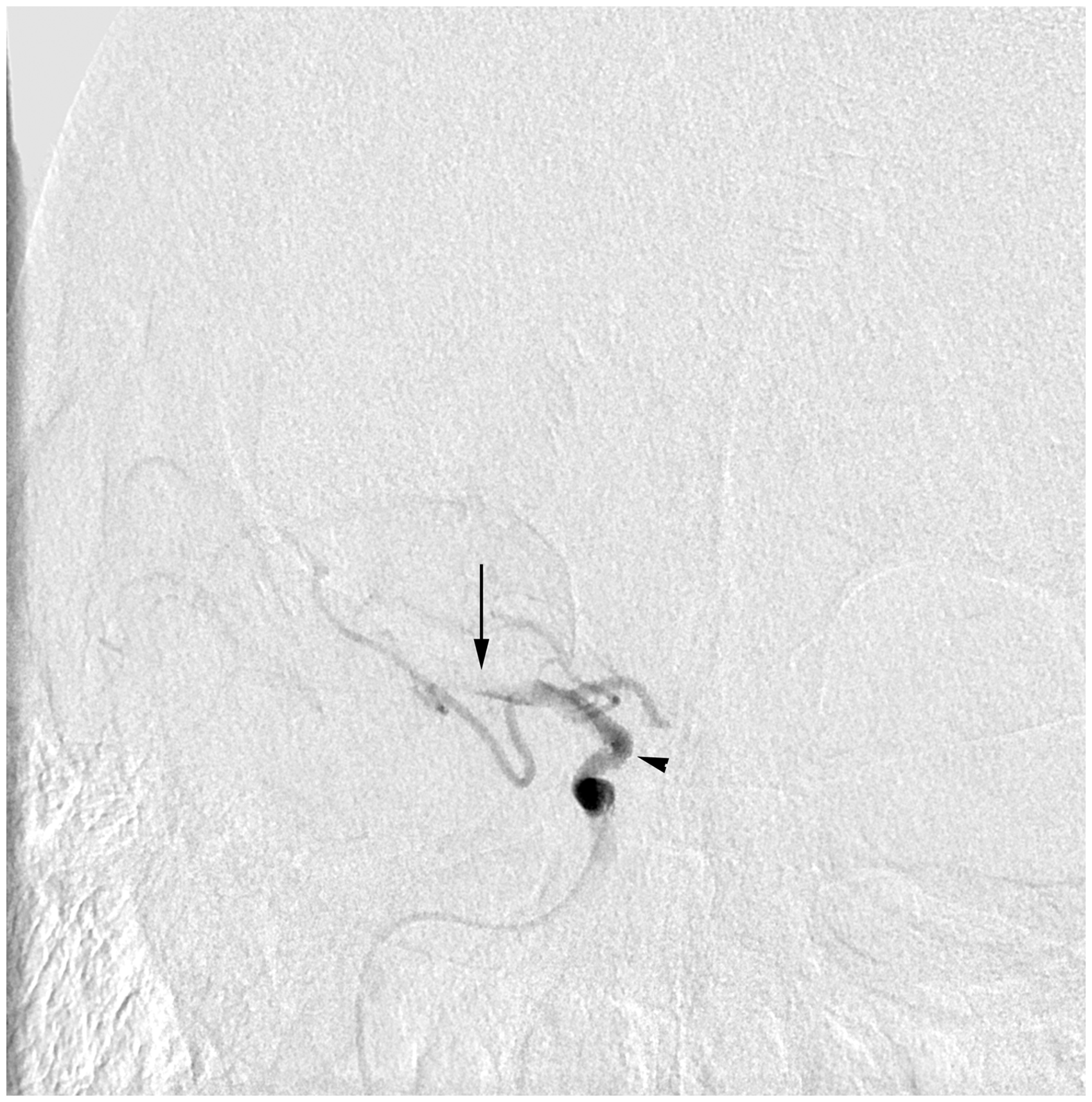




The patient was given an intravenous bolus of, and started on maintenance drip of eptifibatide. The patient passed a dysphagia screen 45 min later, and was given a 60 mg PO bolus of prasugrel and 325 mg PO aspirin. The eptifibatide drip was discontinued 2 h after the PO bolus of antiplatelet medications. The patient was discharged home the next day (mRS 0) and was continued on dual antiplatelet regimen thereafter.
Discussion
In patients with ELVO stroke and tandem lesion, it is a complex decision to revascularize the cervical carotid before or after thrombectomy, and/or offer endovascular treatment at all. This is partially due to the variability in treatment these patients have received in large prospective thrombectomy trials. Consensus appears to be emerging that emergency treatment of both intracranial and extracranial lesions is safe and probably improved clinical outcomes. In this patient population, the interplay of the clinical exam, anticoagulation, and anti-platelet regiments combined with the potential for long and more complex procedure propels an already high-risk population towards a propensity for a poor clinical outcome. Carotid stenting with antithrombotic agents has been shown to yield superior recanalization rates when compared to thrombectomy alone. 13
It is clear, however, that failed intracranial revascularization ensures a poor outcome, and it is this very population that may benefit from increased collateral circulation provided by emergent cervical recanalizaiton.
We have found that this technique significantly expedites the process of revascularization of LVO strokes with concomitant carotid occlusive disease. Our average procedure time, from groin access to groin closure was 52 min for these complex procedures (27–96 min). In 23/24 (96%) of the patients, our technique provided a “single-pass” of the BGC into the distal cervical ICA, and this was achieved in less than the 5 min “waiting period.”
We chose to report total procedure time (i.e. groin access to groin closure). This decision was made to eliminate ambiguity as to when re-perfusion is re-established. After thrombectomy, full intracranial recanalization may be re-established, but there still may be a flow-limiting or even occlusive lesion that remains in the extracranial carotid. By reporting the full procedure time, we can standardize the reported times across this heterogeneous patient population.
Stenting of the carotid artery over the stentriever wire has been described previously. Behme et al. presented a case report of a single individual who they successfully treated with a stent over a thrombectomy wire. 14 The thrombectomy device in this case report was small (4 × 20 mm Trevo) and the authors do not comment on whether or not the ACA was protected. There is no commentary provided as to the location of the BCG, although a “solumbra” technique was employed by use of a 6F SophiaPlus aspiration catheter, advanced to the carotid terminus.
Sultan-Qurraie et al. describe a similar technique for the treatment of concomitant carotid and intracranial large vessel occlusions 15 although there are some important distinctions to be made between these two techniques. First of all, their SEIMLesS technique recommends advancing the BCG as distally as possible, but it is not reported whether they attempted or were successful in their five-patient retrospective group. We believe that “drafting” the BCG behind the angioplasty balloon as it is deflating is essential for advancing the BCG to the skull base. Distal BCG placement is a first principle of mechanical thrombectomy. The SEIMLesS group re-demonstrated our finding that concomitant versus sequential treatment appears to result in faster treatment times. We would also emphasize that stentriever selection is essential to ensure coverage of the ACA. The SEIMLesS group “strive[s]” to achieve this as well, but does not include this essential point as a part of their protocol.
Another key point the SEIMLesS authors make is to use the BCG inflated in the CCA as a proximal flow arrest device. The patients who present with tandem occlusions often have chronic, high-grade ICA stenoses with intracranial collaterals fed by the ECA and a high hypoperfusion index. In our experience, occluding the common carotid artery can exacerbate cerebral ischemia in these patients and should be avoided if possible.
We had one patient in whom the BGC would not pass the carotid lesion despite using the angioplasty technique described here, as the cervical carotid lesion was “heavily calcified” and would not permit passage of BGC into the distal cervical ICA. In this instance, we had to address the cervical lesion first with angioplasty and stent placement, and while the patient did have a good clinical outcome (mRS 0), the procedure time was substantially longer (117 min).
While the efficacy of the stent retriever as a surrogate EPD is challenging to evaluate in a retrospective case series, the technique would also permit angioplasty of the cervical carotid lesion utilizing proximal BGC for flow arrest and aspiration if desired. There was no evidence of ACA or PCA infarct in any patient on 24 h follow-up imaging (by either CT or MRI). Follow-up angiography following completion of the procedure (with the patient in still in the angiography suite), demonstrated a new embolus to the ACA or PCA in only one patient (4%). This represented a pericallosal ACA branch (A3 segment) embolus, which was not clinically evident or identifiable as an infarct on subsequent CT scan. This patient also received intravenous tPA, and we suspect there was subsequent lysis of the thrombus. Satisfactory reperfusion was achieved with TICI 2b-3 flow in all patients (100%). We have found that this technique simplifies many decision points during what initially may be viewed as a “complex” case. If one is dealing with a more sub-acute or chronic cervical occlusion presenting with a “stump” embolus, the support of “dual” proximal catheters/sheaths allows for remarkable stability and support.
The antiplatelet regimen for these patients requires significant consideration. Fourteen (61%) patients received full-dose intravenous tPA prior to the intervention. Fourteen (61%) patients received an intravenous bolus of eptifibatide in the angiography suite, with eight of these patients also having received IV tPA therapy. Seventeen (74%) of the patients received loading doses of dual antiplatelet therapy (clopidogrel or prasugrul and aspirin) within 2 h post procedure of which eight had received IV tPA. Seven patients (30%) received all of the following: intravenous tPA, eptifibatide bolus, and within 2 h post procedure a loading dose of dual antiplatelet therapy.
Patient demographic and device usage data.
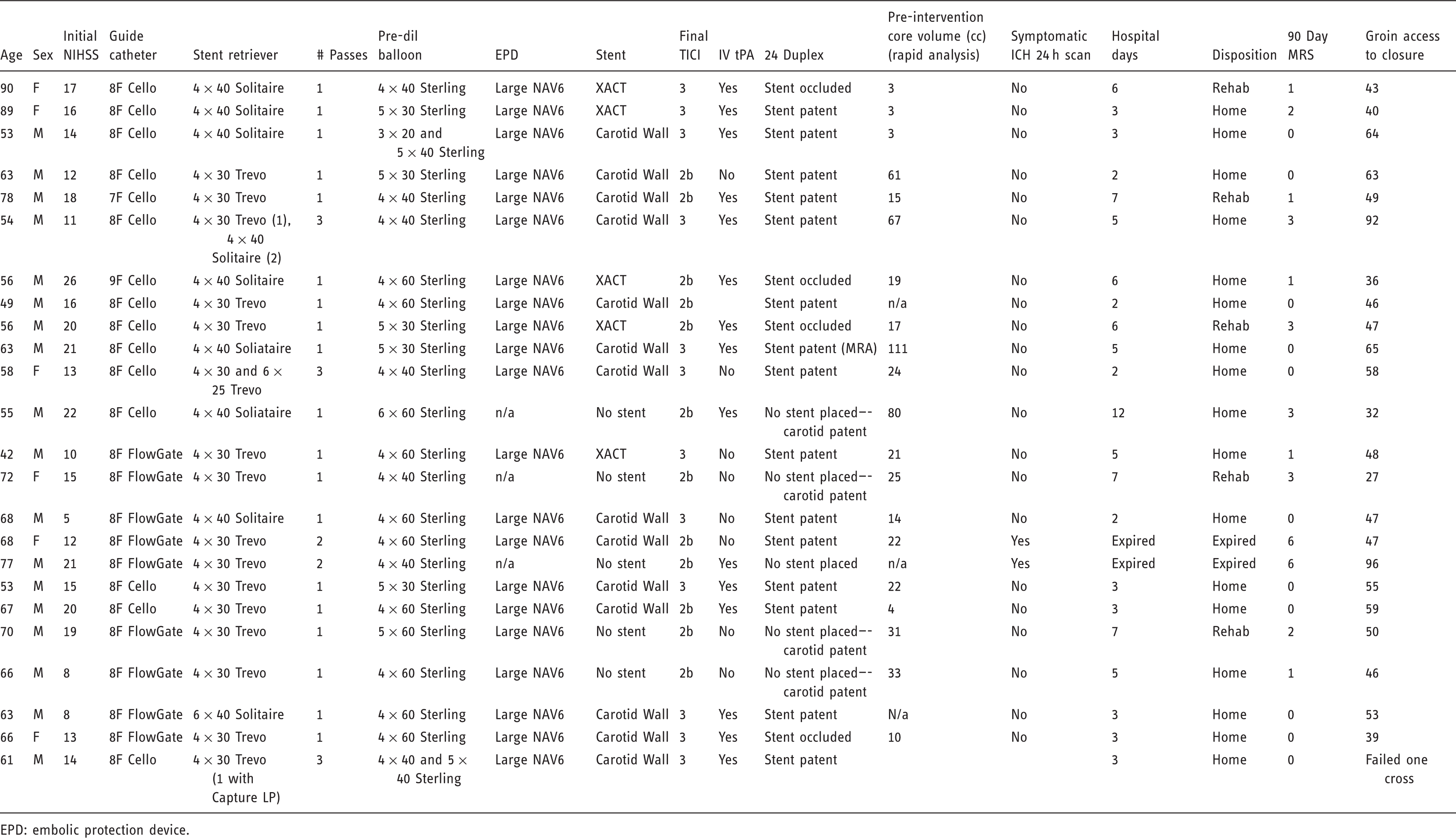
EPD: embolic protection device.
All patients had meticulous management of blood pressure following reestablishment of flow, with target systolic pressures strictly less than 140 mmHg.
Carotid duplex examinations were performed the next day in all patients. Of the 18 patients who received a stent, 4 (22%) had in-stent occlusion. Three of these four acute stent occlusions had 90 mRS of 0 or 1 (one patient only had 30-day follow-up and was mRS of 1). One of the patients with re-occlusion did not receive any antiplatelet therapy for 24 h (the first patient in the series). In future, studies are needed to truly understand the best antiplatelet regimes for these complex patients.
While this represents a small, retrospective case series of a complex clinical problem, we were able to achieve excellent clinical outcomes comparable to recent stroke trials. The rate of death and sICH are low (9%) in this complex patient population. The procedure is efficient, allowing for the treatment of two potentially lethal disease processes in a fast and efficient manner. The clinical outcome for this cohort is very good; all but 1 patient has 90-day follow-up, with 17 (74%) patients having an mRS 0–2. The most recent patient in our series has only 30-day follow-up, with an mRS of 1.
The other technical pitfall of this technique revolves around the compatibility of the guide catheters, balloons, stents, and microwires. The stent retriever wires (Solitaire & Trevo) are slightly larger than traditional 0.014 in. microwires, and are not compatible with traditional carotid angioplasty balloons/stents. But it is feasible that future renditions of these devices will take into account this scenario and develop more readily compatible versions, further simplifying these seemingly complex clinical presentations. Additionally, there may be other devices available outside the United States (Aperio, pReset) that offer a wider range of interoperability.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.