
Abstract
Background
Although the embolization of lenticulostriate artery feeders is often warranted in the treatment of brain arteriovenous malformations, it is technically challenging due to steep and repeated angulations. Here, we describe our novel technique of navigating a flow-guided microcatheter into lenticulostriate artery feeders using the strong support provided by an S-shaped distal access catheter.
Methods
We reviewed our retrospective cohort of brain arteriovenous malformations, in which lenticulostriate artery feeders were attempted to embolize.
Result
During the study period, endovascular embolization was performed in 25 arteriovenous malformations cases. Of these, eight lenticulostriate artery feeders were present in six cases (24%). In two cases, lenticulostriate artery feeder catheterization was avoided from the beginning due to the small diameters of the feeders. After all, microcatheter navigation for lenticulostriate artery feeders were attempted in four cases with six lenticulostriate artery feeders. In all the six feeders, the S-shaped distal access catheter was successful in supporting the microcatheter to advance distally to the lenticulostriate artery feeders, even if other approaches were unsuccessful. Of the six catheterized lenticulostriate artery feeders, four were embolized. Symptomatic infarction in the lenticulostriate artery territory and mild vasospasm occurred in two cases each, but they did not result in permanent neurological deficits.
Conclusion
Although some potential complications need to be considered, the S-shaped distal access catheter technique appears to be an effective alternative approach to gaining access to difficult feeders of arteriovenous malformations.
Introduction
The treatment of high-grade brain arteriovenous malformations (AVM) is still challenging even in the multimodality treatment era.1–3 Some AVM have deep lenticulostriate artery (LSA) feeders, which are generally fragile and tortuous.4,5 The presence of deep feeders significantly increases surgical risks, and, thus, presurgical embolization is important.6–8
However, difficulties are associated with catheterizing the LSA. The LSA arises from the superoposterior aspect of the M1 segment of the middle cerebral artery (MCA) and then makes a sharp medial turn, followed by a sharp lateral turn before it enters the anterior perforated substance.9,10 These curves in the LSA are major obstacles to the advancement of microcatheters.
A “balloon-assisted microcatheter navigation” method has already been reported by a group with extensive experience of microcatheter navigation into LSA feeders. 11 In this method, a compliant balloon is inflated at the MCA just after the origin of the LSA. This balloon helps the microcatheter to advance deeply into LSA feeders. This method demonstrates that strong support is vital for the successful navigation of microcatheters.
We recently encountered some cases in which an S-shaped distal access catheter provided strong support for the navigation of a microcatheter into LSA feeders. The aim of the present study was to review our AVM cases in which LSA feeders were attempted to embolize and assess the utility of this technique.
Subjects and methods
This single-center retrospective study, which was performed to review the catheterization methods of LSA feeders in the embolization of brain AVM, was approved by the hospital ethics committee.
Brain AVM embolized in our hospital between April 2011 and January 2017 were candidates for this study. Angiograms before embolization were reviewed by at least two authors (SK and MS) and AVM with LSA feeders were included. The details of embolization were reviewed, with a focus on the catheterization technique used for LSA feeder navigation and associated complications.
Results
During the study period, a total of 44 embolization sessions were performed on 25 AVM cases consisting of 12 males and 13 females, with an average age of 36 (8–72 years). Of these 25 cases, 8 LSA feeders were present in 6 cases (24%).
In two of those cases, the diameter of LSA feeders was so small that the risk of embolization did not seem to outweigh the benefits. Thus, the operator had given up catheterizing them from the beginning. In the remaining four cases, the operator attempted to catheterize LSA feeders, for which attending physician strongly demanded to embolize before surgical resection or Gamma-knife radiosurgery. Two cases had two LSA feeders. After all, microcatheter navigation for LSA feeders were attempted in four cases with six LSA feeders during the study period (Table 1). The locations of AVM were in the frontal lobe in two cases, the basal ganglia in one, and the parietal lobe in one. Presentations were intracranial hemorrhage in three cases and seizure in one.
Summary of cases.

Embo: embolization; LSA: lenticulostriate artery; NBCA: n-butyl cyanoacrylate; Technique no. 1: balloon-assisted microcatheter navigation; technique no. 2: exchange method using S-shaped microcatheter; technique no. 3: S-shaped distal access catheter supported microcatheter navigation.
Endovascular procedures
Endovascular procedures were performed by a single operator (MS) under local anesthesia and continuous sedation (Cases 1 and 3) or general anesthesia (Cases 2 and 4). After a sheath introducer was inserted into the right femoral artery, a bolus of heparin was injected intravenously. An 8-Fr balloon guiding catheter (Optimo Temporary Occlusion Balloon, Tokai Medical Products, Inc., Aichi, Japan) was navigated into the internal carotid artery ipsilateral to AVM, and continuous irrigation with heparinized saline (10 units of heparin per 1 ml saline) was started. We used the balloon guiding catheter to control the flow of embolic materials during their injection.
There was no predetermined protocol for LSA feeder catheterization. Three techniques were retrospectively recognized.
Technique no. 1: balloon-assisted microcatheter navigation
As reported previously by Mendes et al. 11 , with a double lumen compliant balloon (Scepter XC 4 × 11 mm, Microvention, Inc., Tustin, CA, USA) inflated just after the origin of LSA feeders, the navigation of a flow-directed microcatheter, Marathon (Medtronic, Dublin, Ireland) or Magic 1.5F (Balt Extrusion Sas, Montmorency, France), into LSA feeders was attempted using a 0.010-inch microguidewire (Tenrou S-10, Kaneka Medix Corporation, Osaka, Japan).
Technique no. 2: exchange method using S-shaped microcatheter
The tip of the Excelsior SL-10 Pre-shaped S microcatheter (Stryker Neurovascular, Fremont, CA, USA) generally turns upward in the M1 segment of the MCA. Using this characteristic, the tip of the microcatheter was engaged at the origin of LSA feeders. To obtain additional support, a compliant balloon (Scepter XC 4 × 11 mm) was inflated at the origin of LSA feeders to fix the microcatheter. With this support, a long 0.010-inch microguidewire (Chikai 10-300 cm, Asahi Intecc Co., Ltd., Aichi, Japan) was navigated as far as possible. An exchange of the S-shaped microcatheter with a Marathon or Magic 1.5F microcatheter along the fixed microguidewire was attempted.
Technique no. 3: S-shaped distal access catheter technique
The tip of the distal access catheter (Fubuki 4.2Fr, Asahi Intecc Co., Ltd.) was manually bent to make two small sharp curves taking the form of an “S” (Figure 1) using a heat gun (GHG 660 LCD Professional, Bosch, Gerlingen, Germany). The temperature of the heat gun was set to 130°C. To avoid the catheter damage due to overheating, the temperature applied to the distal access catheter was sensed with the operator’s hand holding the catheter. On average, heating for 20 s was repeated twice. After heating, the catheter was left for several minutes at room temperature to stabilize the shape. This S-shaped distal access catheter turned upward at the distal part of the M1 segment. The catheter was then gently pulled back with a continuous slow injection until the LSA feeder was opacified. With this catheter engaged at the orifice of the LSA, a flow-guided microcatheter, either Marathon or Magic 1.5F, was navigated as distally as possible. The distal access catheter provided an enough support for the microcatheter to advance more deeply into LSA feeders.
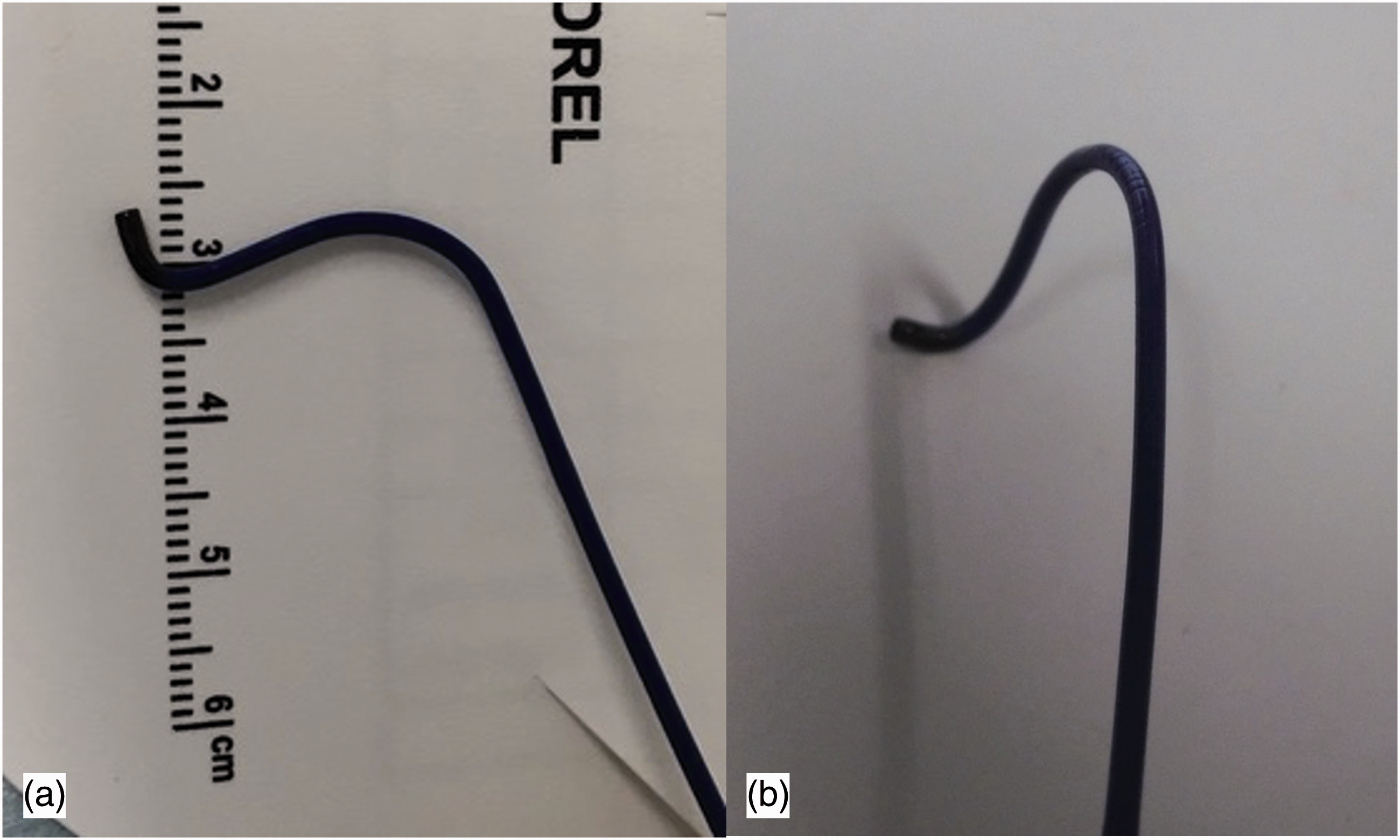
Shaping of distal access catheter for the catheterization of LSA feeders. (a) S-shaped distal access catheter for the distal LSA feeder in Case 2. (b) Reshaping of the catheter for the proximal LSA feeder in Case 2. Note that a stronger and slightly more anterior bend was shaped for the proximal feeder.
Provocation tests were performed with the local injection of pentobarbituric acid 50 mg prior to injection the liquid embolic material from LSA. Clinical examination was performed when the patient was under conscious sedation, and motor-evoked potentials were monitored when the patient was under general anesthesia. Of the six LSA feeders tested, two positive feeders were not embolized.
N-butyl cyanoacrylate (NBCA) diluted at 17, 20, or 25% was injected into three feeders and Onyx 18 (Medtronic) into one for embolization.
In the first two cases, techniques no. 1 and/or no. 2 were initially attempted but were not successful. Although the tip of the microguidewire or microcatheter was successfully inserted into the origins of the LSA feeders, they did not advance beyond the angulations of the feeders. We then changed our strategy to use technique no. 3, and the microcatheter was successfully navigated into LSA feeders distally. In the latter two cases, technique no. 3 was used from the beginning, and the microcatheter was successfully navigated into LSA feeders.
Representative case
A 63-year-old male (Case 2) with large right parietal AVM presented with intraventricular hemorrhage (Figure 2(a)). Embolization was indicated before the surgical removal of AVM. Two LSA feeders were detected, one that originated from the superoposterior aspect of the MCA and the other from the superoanterior aspect (Figure 2(b)).
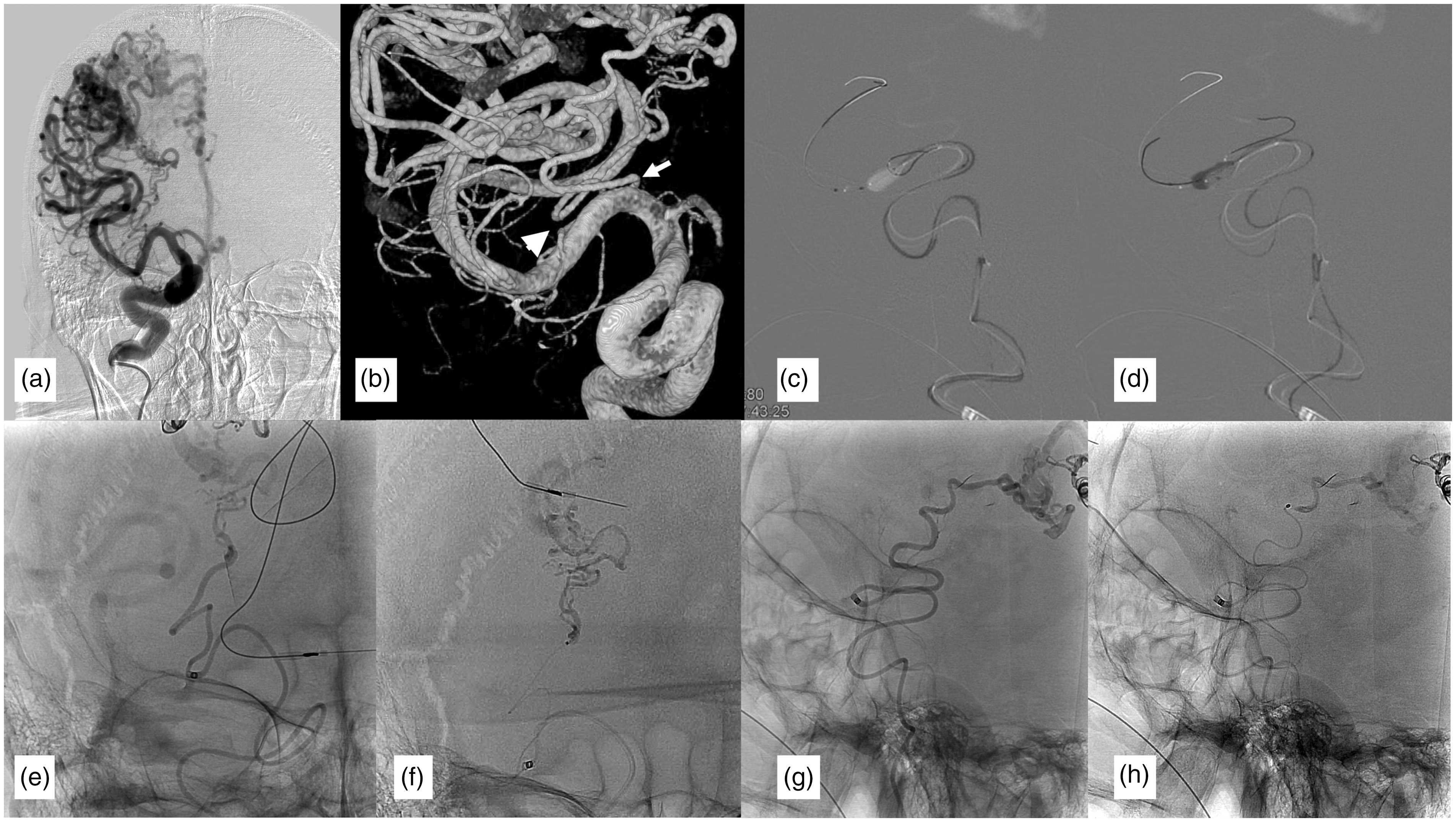
Microcatheter navigation to the LSA feeder in Case 2. (a) Anteroposterior view of a right internal carotid angiogram showing the parietal AVM with LSA feeders. (b) 3D rotational angiogram showing two LSA feeders, one proximal superoanterior (white arrow), and one distal superoanterior feeder (white arrowhead). (c) Navigation of the microcatheter with the balloon-assisted technique (technique no. 1) was attempted, but unsuccessful. (d) Navigation of the microguidewire from the S-shaped microcatheter was also attempted (technique no. 2); however, microcatheter exchange was not successful. (e) Non-subtracted image of the injection from the S-shaped distal access catheter. Note that the tip of the intermediate catheter engaged the orifice of the LSA, providing maximum support for microcatheter navigation. (f) A microcatheter (Marathon) was successfully advanced deep into the LSA feeder from this intermediate catheter. However, the embolization from this microcatheter was avoided because the provocation test was positive. (g) After re-shaping the distal access catheter, it was positioned at the origin of the proximal LSA feeder. (h) A microcatheter was advanced deep into the feeder from this catheter and NBCA was injected.
Technique no. 1 was initially attempted. A 0.010-inch microguidewire was inserted at the origin of the superoposterior LSA feeder (Figure 2(c)) and the advancement of a Marathon microcatheter along it was attempted with Scepter XC balloon inflated. However, the microcatheter and guidewire did not advance along the feeder and bent into the distal MCA.
The tip of the S-shaped SL10 microcatheter was engaged into the LSA feeder (Technique no. 2). Scepter XC balloon was also inflated at the origin of the feeder to increase the back-up power. With this support, the microguidewire advanced past the second angulation of the LSA feeder (Figure 2(d)). However, the SL10 microcatheter did not advance along the 0.010-inch guidewire. Thus, we attempted to exchange the SL10 microcatheter with the Marathon microcatheter; however, the exchange maneuver was unsuccessful. This second attempt gave us a hint that an S-shaped catheter might provide sufficient support for the microcatheter to be advanced deep into LSA feeders.
In the third attempt, the tip of a distal access catheter (Fubuki 4.2Fr) was bent with a heat gun into the shape of an “S” (Figure 1(a)). This S-shaped intermediate catheter was navigated into the MCA and its tip was engaged at the origin of the superoposterior LSA feeder (Figure 2(e)). The support was sufficiently strong for the Marathon microcatheter to advance deeply into this feeder (Figure 2(f)). However, the provocation test resulted in the disappearance of motor-evoked potentials and, thus, glue was not injected into this feeder.
It was not possible to access the superoanterior LSA feeder with the same S-shaped distal access catheter, and the tip was reshaped to turn anteriorly after the upward convex MCA (Figure 1(b)). With this reshaped catheter, the origin of the proximally originating LSA feeder was engaged (Figure 2(g)) and the Magic 1.5F microcatheter advanced deeply (Figure 2(h)). After a negative provocation test, 0.44 ml of 20% NBCA was injected. After confirming successful devascularization from LSA feeders, the endovascular procedure was completed without complications.
Infarction in the LSA territory
In all the four cases, magnetic resonance imaging (MRI) was performed within one week of embolization. Newly formed infarctions in the LSA territory were detected in three cases: one was asymptomatic (Case 3), whereas the other two were symptomatic (Cases 1 and 4).
In Case 1, two infarctions in the centrum semiovale appeared after embolization. The anterior infarction was attributed to embolization because it was continuous with the glue (Figure 3(a) and (b)). The posterior infarction was separate from the glue and was attributed to flow arrest caused by wedging of the intermediate catheter into the origin of the LSA (Figure 3(c)). These infarctions caused mild weakness of the right hand, which completely resolved in one week. In Case 3, a small asymptomatic infarction that was continuous with the glue appeared. In Case 4, a moderate infarction appeared in the right centrum semiovale that was continuous with the glue (Figure 3(d) and (e)). It was responsible for left hemiparesis, which completely resolved in one week.
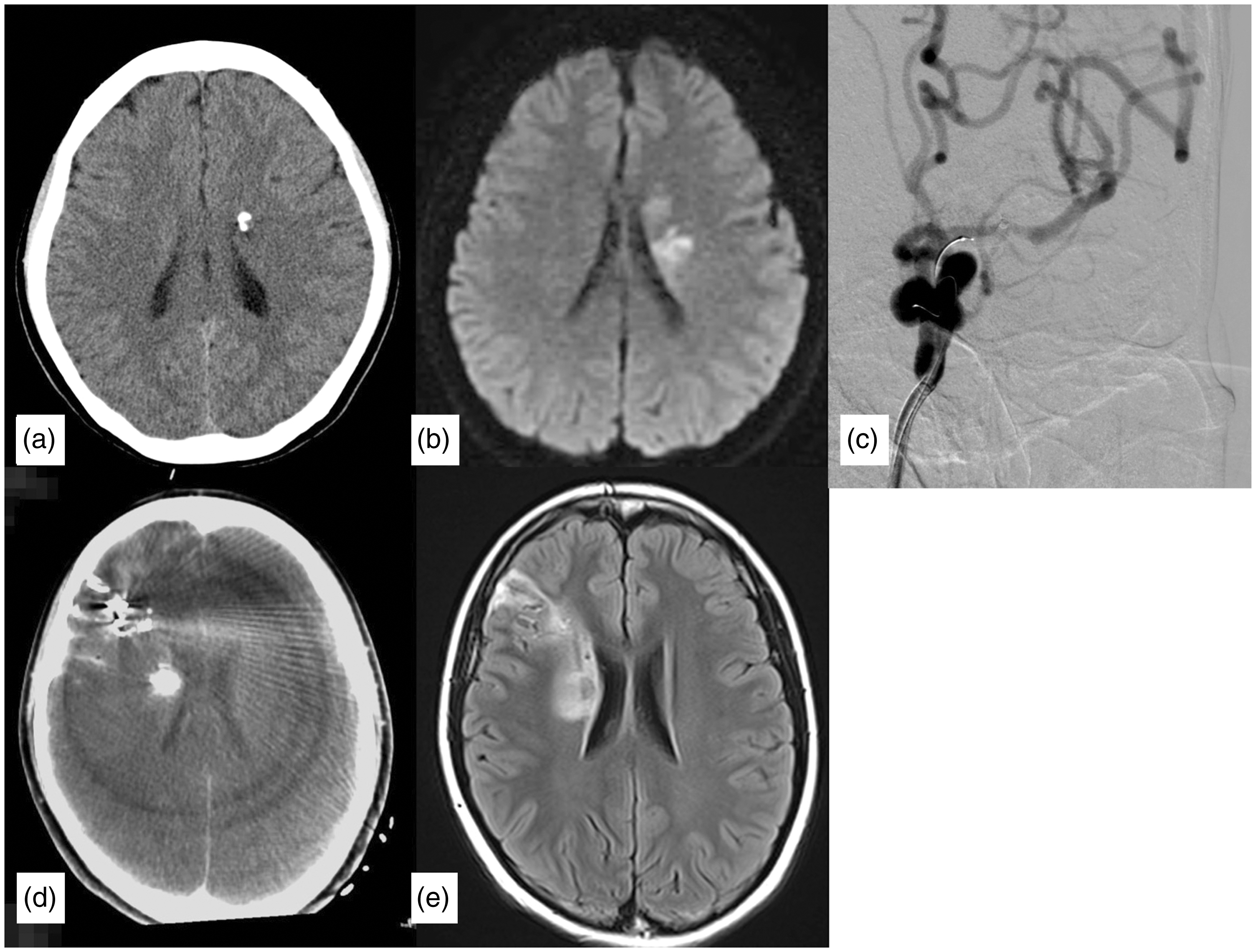
Ischemic complications of LSA feeder embolization. Case 1. Cerebral CT scan after embolization showing the distribution of the embolizing material (a) and an MRI diffusion-weighted image showing two separate infarctions (b). The anterior infarction was adjacent to the embolizing material and, thus, was attributed to embolization. The other infarction contributed to the arrest of flow in the LSA during intermediate catheter engagement (c), which was retrospectively detected with the injection from the guiding catheter during embolization. Case 4. CT scan showing the distribution of glue (d) and MRI showing ischemia adjacent to glue (e). Subarachnoid hemorrhage was also observed and attributed to microcatheter navigation into the cortical feeder during the same embolization session.
Perforation, dissection, and spasm of intracranial arteries
In Case 4, minor subarachnoid hemorrhage, limited to the cortical sulci near the nidus, was detected on computed tomography after embolization (Figure 3(d)). It was attributed to the perforation of other cortical arteries embolized in the same session and was responsible for a minor headache lasting for a few days without neurological sequalae.
Arterial dissection was not detected on angiograms obtained after embolization. Vasospasm at the M1 segment was noted in two cases. Stenosis was 43% in Case 1 (Figure 4) and 23% in Case 3. In both cases, stenosis was not responsible for flow restrictions. Thus, a vasodilator was not injected. This vasospasm resolved spontaneously on MRI acquired four days after embolization.
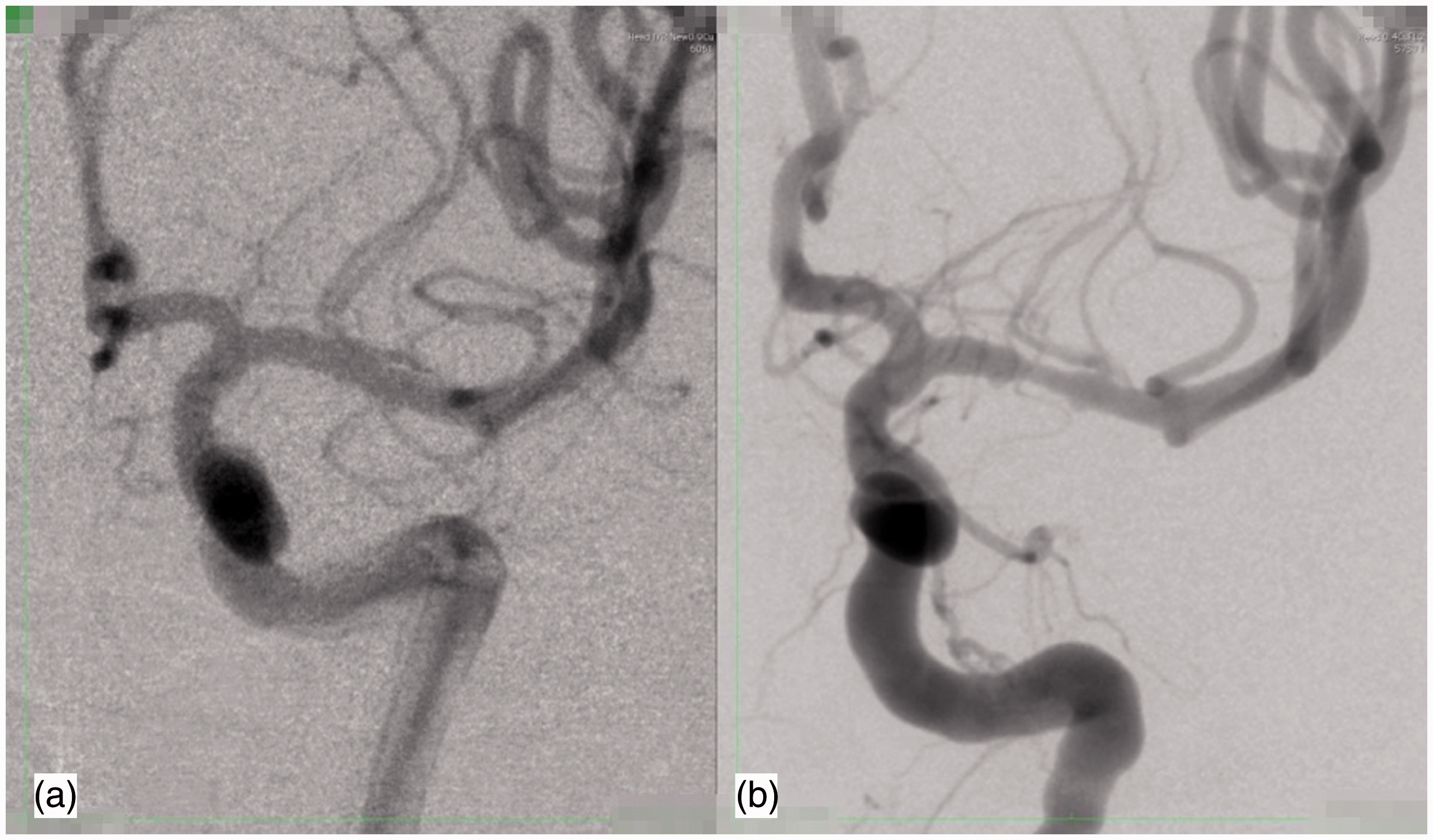
Mechanical spasm caused by the distal access catheter. Left internal carotid angiogram before (a) and after (b) embolization from LSA feeders. The diameter of the M1 segment showed 43% narrowing.
Discussion
We herein described our initial experience of the distal access catheter shaping technique, in which an S-shaped intermediate catheter provided strong support at the origin of the LSA for the navigation of a microcatheter deeply into the LSA feeders of brain AVM. This technique provided successful microcatheter access to LSA feeders in all cases, even when other techniques failed. No perforation or dissection occurred. However, the distal access catheter may cause vasospasm at the M1 segment of the MCA and alter blood flow to cause infarctions in the territory of the LSA. Distal access catheters were previously shown to facilitate the access of a microcatheter.12–14 However, to the best of our knowledge, this is the first study to demonstrate that reshaping of the distal access catheter augmented its support for accessing LSA feeders of AVM.
Potential benefits of our technique
In the balloon-assisted microcatheterization technique (technique no. 1), difficulties are sometimes associated with placing the balloon exactly at the origin of the LSA because antegrade flow of the MCA may move the balloon during its inflation. Intracranial exchange of the microcatheter is necessary when the pre-shaped S microcatheter is used (technique no. 2), which is technically difficult and is associated with a risk of fatal complications. 15
Indirect options may also be employed to embolize difficult feeder(s) such as embolizing the nidal compartment and deep feeder in a retrospective manner from a catheter that has been navigated into an accessible feeder. Several techniques, including the pressure cooker technique and dual-lumen balloon-assisted technique, have been shown to facilitate the penetration of Onyx.16,17 Furthermore, the intermittent balloon occlusion technique enhances the penetration of Onyx by reducing back pressure. 18 Although these techniques are useful, they are not applicable to some cases in which the goal of endovascular treatment is the partial or targeted embolization of deep feeders.19,20
Among the distal access catheters available in our country in the study period, we chose Fubuki 4.2Fr (Asahi Intecc Co., Ltd.). To support flow-guided microcatheters, distal access catheters have to maintain their shape firmly. Fubuki 4.2Fr has braiding reinforcement structure inside, and it is considered easier to form and maintain the tip shape than other distal access catheter. If the diameters of catheters are larger, it will be difficult to form S-shape in M1, and, if catheters are smaller, the support will be weaker. A slightly smaller combination of flow-guided microcatheters and distal access catheters would be more desirable.
The technique of supporting a flow-guided microcatheter with a shaped distal access catheter may be useful for inserting a catheter into a narrow vessel that branches from a large vessel at a steep angle such as inferolateral trunk and meningohypophyseal trunk of internal carotid artery.
Potential risks and cautions
There are some concerns regarding the microcatheter navigation using S-shaped distal access catheters. First, the S-shaped catheter may place a physical stress on the MCA. In our series, mild vasospasm was detected in two of the four cases. If the S-shaped tip places a stronger physical stress on the intracranial artery, dissection or life-threatening perforation of the artery may occur. Although the prevalence of this mechanical complication in the MCA currently remains unclear, careful attention is needed during positioning of the intermediate catheter.
Second, the engagement of distal access catheters may cause ischemia. It is important to be careful not to block the antegrade blood flow of the LSA for long periods of time when the catheter is at the origin of the LSA.
Moreover, the navigation to the distal part of LSA does not always guarantee safe embolization without ischemic lesions. Even when microcatheters are navigated deeply into LSA feeders, vital tissue may be present between the tip of microcatheter and the nidus of AVM. In our cases, two of the six LSA feeders were positive for the provocation tests even the microcatheters were deeply advanced just before the nidus, and in another two feeders, the injections of embolic materials into LSA feeders caused symptomatic infarctions. Although the final clinical outcome was not severe in our patients, the rate of ischemic complication was quite high, and the indications for embolization from the LSA feeder must be determined with caution, especially in unruptured case.
General anesthesia with motor-evoked potential monitoring would be preferable to local anesthesia because it provides better control of the liquid embolic material by immobilizing patients.
Limitations
The major limitation of the present study is the small number of cases examined. The accumulation of further cases will facilitate assessments of the benefits and potential risks of this technique and it will be possible to compare our technique with others.
Conclusions
We herein reported our initial experience of a technique for navigating a flow-guided microcatheter into LSA feeders of brain AVM using an S-shaped distal access catheter. Although some potential complications need to be considered, this technique appears to be an effective alternative approach to gaining access to difficult feeders.
Footnotes
Authors' contribution
Conceptulization: MS; Investigation: SK, OI, MS, SM, HN, HH; Methodology: MS; Supervision: NS, HN; Writing-Original draft preparation: SK; Writing-Review and Editing: MS. All authors discussed the results and contributed to the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Ethical Committee of The University of Tokyo (approval number, 2231).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.