
Abstract
Background
Significant advances have been reported recently in the genetic and mechanistic characterization of extracranial venous malformations. However, intracranial purely venous malformations (icVM) analogous to those outside the CNS have not been systematically described.
Purpose
We sought to ascertain whether such an entity as icVM could in fact be identified, distinct from previously described CNS venous anomalies and analogous to extracranial venous malformations.
Methods
Our prospectively collected pediatric cerebrovascular database was reviewed to identify patients with icVM; 1458 consecutive angiograms and/or angiographic interventions performed on 706 children at our institution from October, 2006 through May, 2019 were evaluated, in addition to outside imaging studies on 192 additional patients sent to our Vascular Anomalies Center for cerebrovascular review during the same time period. Thus, the cohort consisted of 898 children.
Results
Nineteen of 898 patients (2.1%) were found to harbor icVM, including 9 (47.3%) with sinus pericranii, 15 (78.9%) with associated large, complex extracranial venous malformations, and 3 (15.7%) with neurocognitive delay. There was no intracranial hemorrhage or venous hypertension seen in the cohort. Asymptomatic venous thrombosis in the superior sagittal sinus was seen in three patients.
Conclusion
Venous malformations, both extracranial and icVM, share many characteristics that are distinct from developmental venous anomalies. icVM were not associated with venous hypertension. The underlying genetic mutations involved in the development of icVM, germ-line or somatic, remain to be elucidated, but may very well involve shared mechanisms and pathways with extracranial venous malformations.
Keywords
Introduction
Venous malformations (VMs, Figure 1) are slow-flow vascular anomalies originally characterized within a system proposed by Mulliken and Glowacki in 1982, 1 and subsequently updated in the 2015 ISSVA classification of vascular anomalies. 2 The ISSVA classification prominently features VM outside the CNS, with both isolated and syndromic variants identified; several genetic mutations have recently been implicated in these various VM subtypes. However, for the brain, the ISSVA classification includes only brain arteriovenous and capillary anomalies (AVM, AVF, and cavernous malformations, respectively); intracranial purely venous malformations analogous to those outside the CNS have not been systematically described. Developmental venous anomalies and sinus pericranii are better characterized as variant venous drainage patterns rather than true vascular malformations, and are morphologically quite dissimilar from extra-CNS VMs. We sought to ascertain whether true brain venous malformations (icVM) could in fact be found. As such, we systematically reviewed a large cerebrovascular database at our international referral center, with the goal of characterizing the clinical and radiographic features of such lesions.
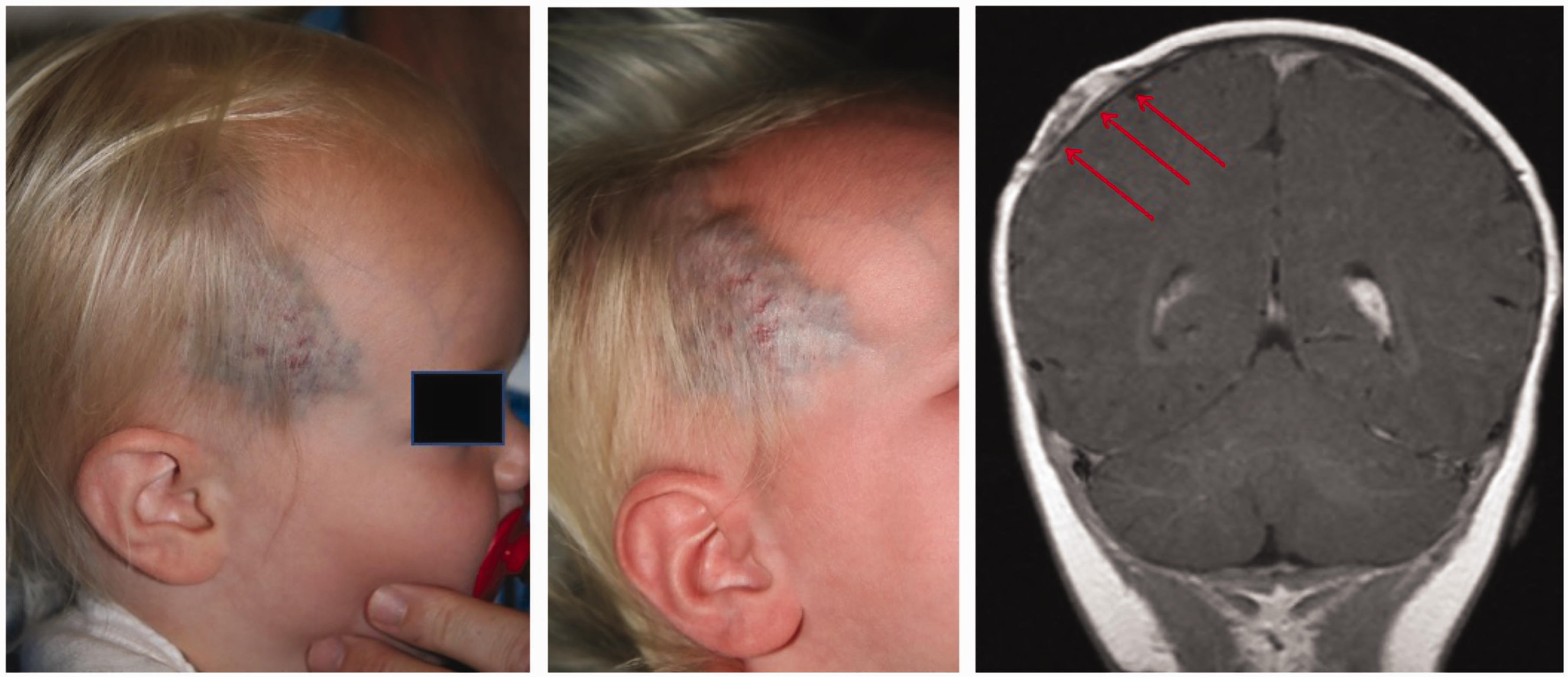
Supra-auricular temporalis region extracranial VM. Note the multilobulated, mass-like, non-cylindrical morphology characteristic of VM.
Methods
Institutional review board approval was obtained for the current study. Our prospectively collected pediatric cerebrovascular database was retrospectively reviewed. The database contains detailed clinical and radiographic information on every patient at our institution who undergoes a neurointerventional procedure, along with a synopsis of all angiographic findings and interventions, entered at the time of the procedure by the senior author. Retrospective review of the database thus allows for efficient screening of a large population of pediatric cerebrovascular patients for the purposes of a research study, identifying among them cohorts with particular features of interest, who then undergo re-analysis of the imaging; 1458 consecutive angiograms or angiographic interventions performed on 706 children at our institution from October, 2006 to May, 2019 were included for evaluation in this study, along with accompanying MR and CT scans. In addition, outside imaging studies on 192 additional patients, sent to our Vascular Anomalies Center for review during the same time period and flagged as harboring cerebrovascular abnormalities, were also included for evaluation, resulting in 898 total patients included in the review. Only patients with ages in the range of fetus to 18 years were included. Lesions characterized by arteriovenous shunting, purely arterial anomalies, cavernous malformations, capillary telangiectasias, developmental venous anomalies corresponding to previously described morphology, and sinus pericranii without anomalous intracranial venous morphology were excluded.
Intracranial venous malformations (icVM) were defined as mass-like, non-cylindrical collections of venous structures shown to be in clear anatomic continuity with the superficial or deep venous system of the brain or the dural sinuses, with flow characterized as venous in its angiographic, enhancement phase or pulse sequence characteristic, and lack of pulsation artifact on MRI; specific morphologic subtypes of icVM are described below. Architecture of icVM did not evidence the dilated medullary veins converging centripetally into a large venous collector and from there into the superficial or deep venous system, that is characteristic of DVA. The medical records and radiographic imaging of patients harboring such lesions were reviewed for demographic information, clinical presentation and course, associated conditions, neurodevelopmental status, lesional morphology, and drainage characteristics, and accessible genetic information was collected for each patient from chart review. Vascular imaging of the identified cohort was then reviewed by the authors (two endovascular neurosurgical fellows and one interventional neuroradiology fellow, in addition to the senior author). Where available, follow-up imaging was also reviewed in order to assess longitudinal changes in the icVMs, with the follow-up period tabulated.
Results
After excluding cases with arteriovenous shunting, developmental venous anomalies harboring previously described morphology, and sinus pericranii without additional intracranial venous malformation, 19 (2.1%) of 898 patients were designated as having pure intracranial venous malformations (Figures 2 to 7, Table 1). These anomalies, with features analogous to extracranial VM (Table 2), were categorized morphologically into globoid (Figure 7), fusiform (Figure 6), and falcine (Figures 2 and 4); the falcine subtype was seen on fetal imaging as well, subsequently confirmed on postnatal MR (Figure 3). For the cohort with diagnosis of icVM, patient age at diagnosis ranged from 6 months gestational age to 13 years old (mean age = 9.1 years), including 12 males and 7 females.
Imaging, clinical, and demographic characteristics of the icVM cohort.
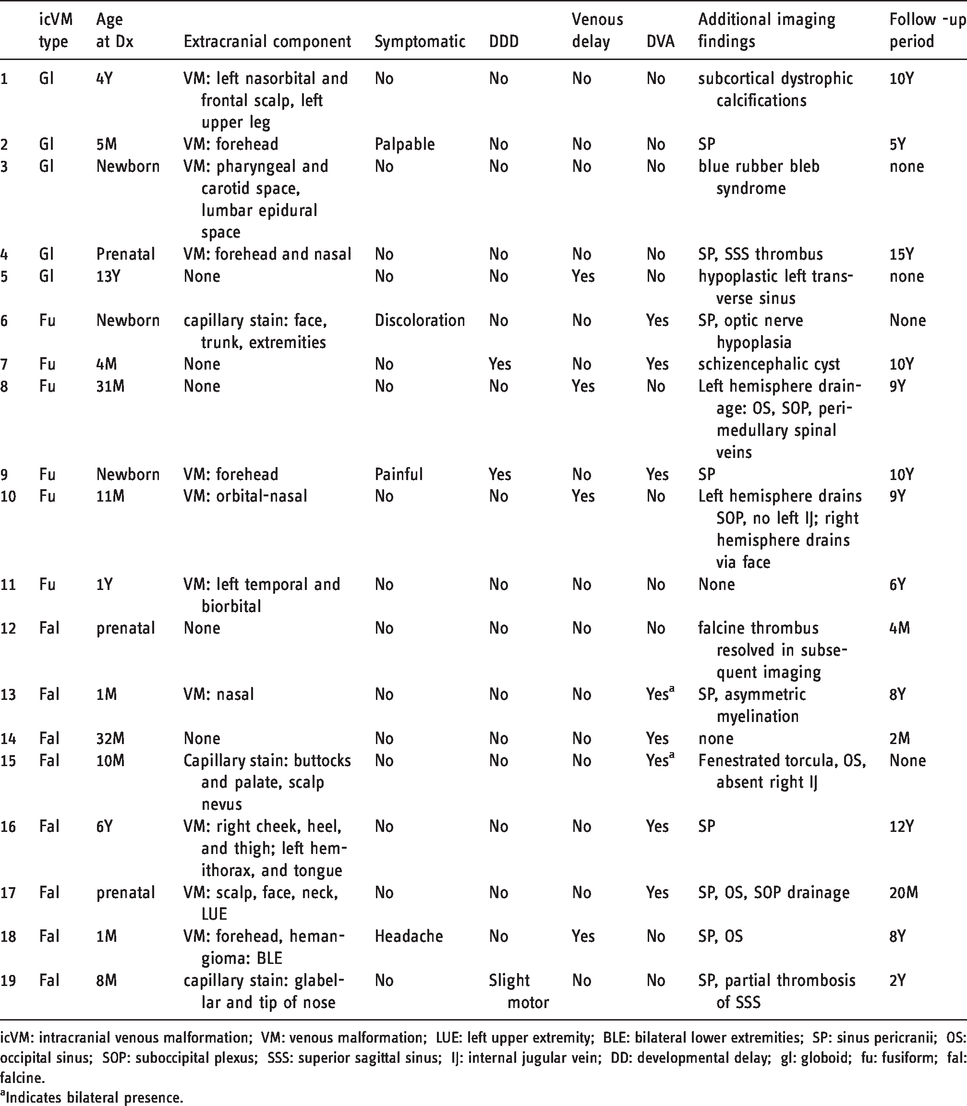
icVM: intracranial venous malformation; VM: venous malformation; LUE: left upper extremity; BLE: bilateral lower extremities; SP: sinus pericranii; OS: occipital sinus; SOP: suboccipital plexus; SSS: superior sagittal sinus; IJ: internal jugular vein; DD: developmental delay; gl: globoid; fu: fusiform; fal: falcine.
aIndicates bilateral presence.
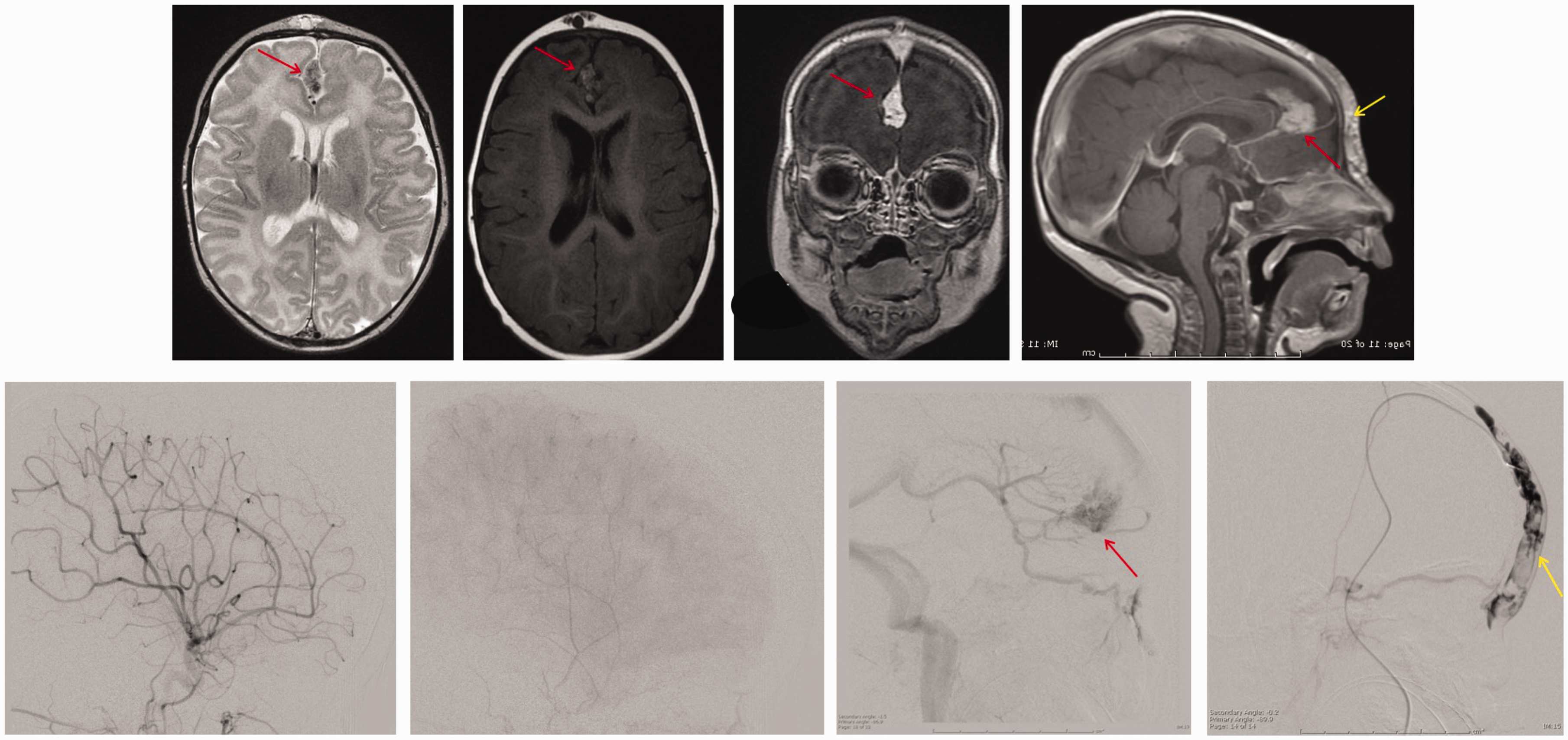
icVM within the leaflets of the falx (red arrows). The patient additionally has a basal ganglia DVA which empties into the icVM, as well as a glabellar extracranial VM (yellow arrows), which is not in communication with the icVM. Upper panels, left to right: axial T2, T1, and coronal and sagittal post-contrast acquisitions show intense enhancement concordant with venous malformation. Lower panels, left to right: lateral views of arterial, capillary, and venous phases of injection of the left internal carotid artery, and direct injection of the glabellar VM. Note absence of visualization of the icVM on arterial or venous phases, as well as absence of drainage of the icVM out to the glabella and non-drainage of the glabellar VM into the icVM.
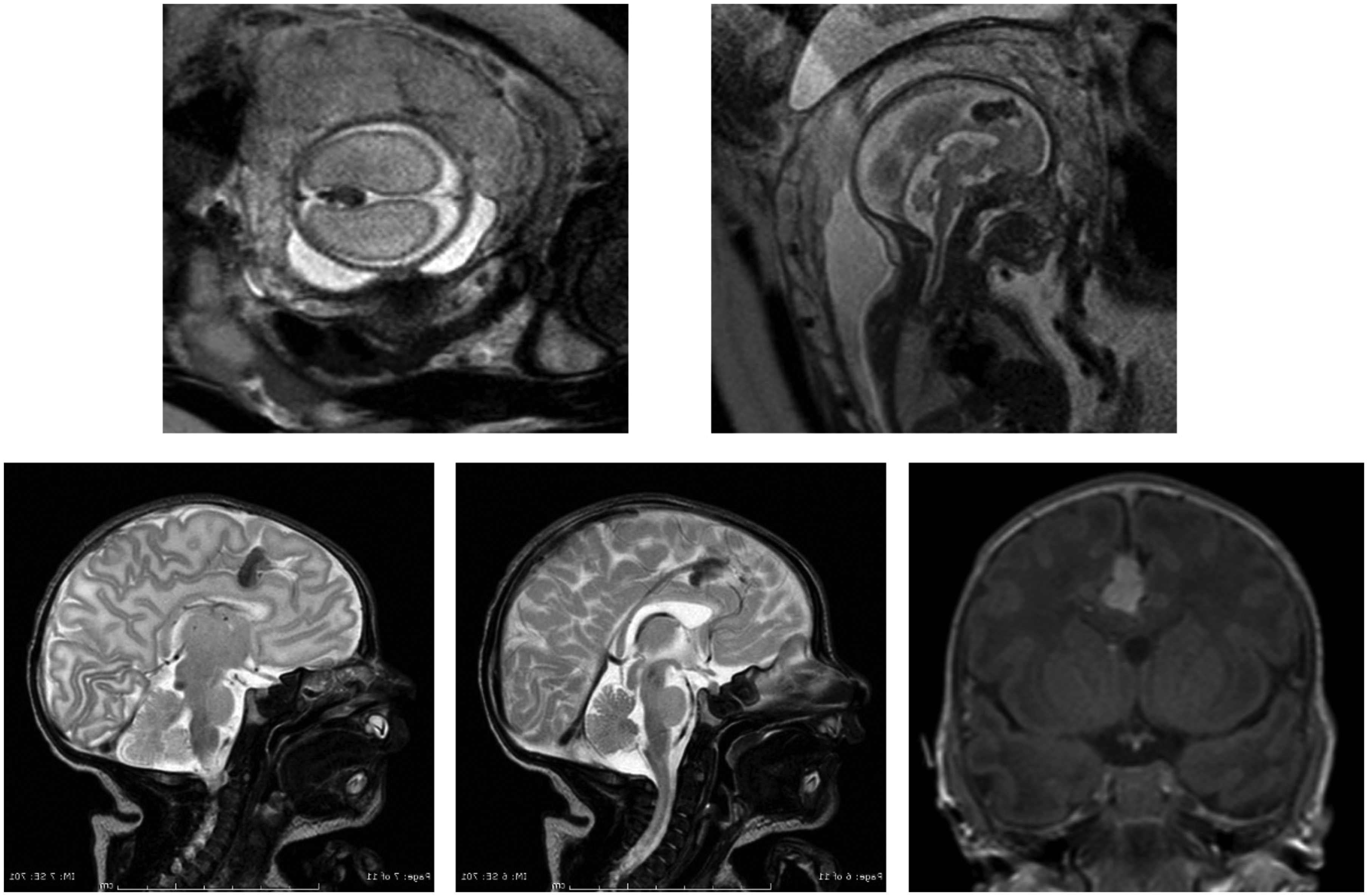
Falcine icVM diagnosed on fetal MRI (upper two panels), along with postnatal MRI follow-up (bottom panels, sagittal T2 and coronal post-contrast T1). Note the posterior drainage of the icVM into the inferior sagittal sinus.
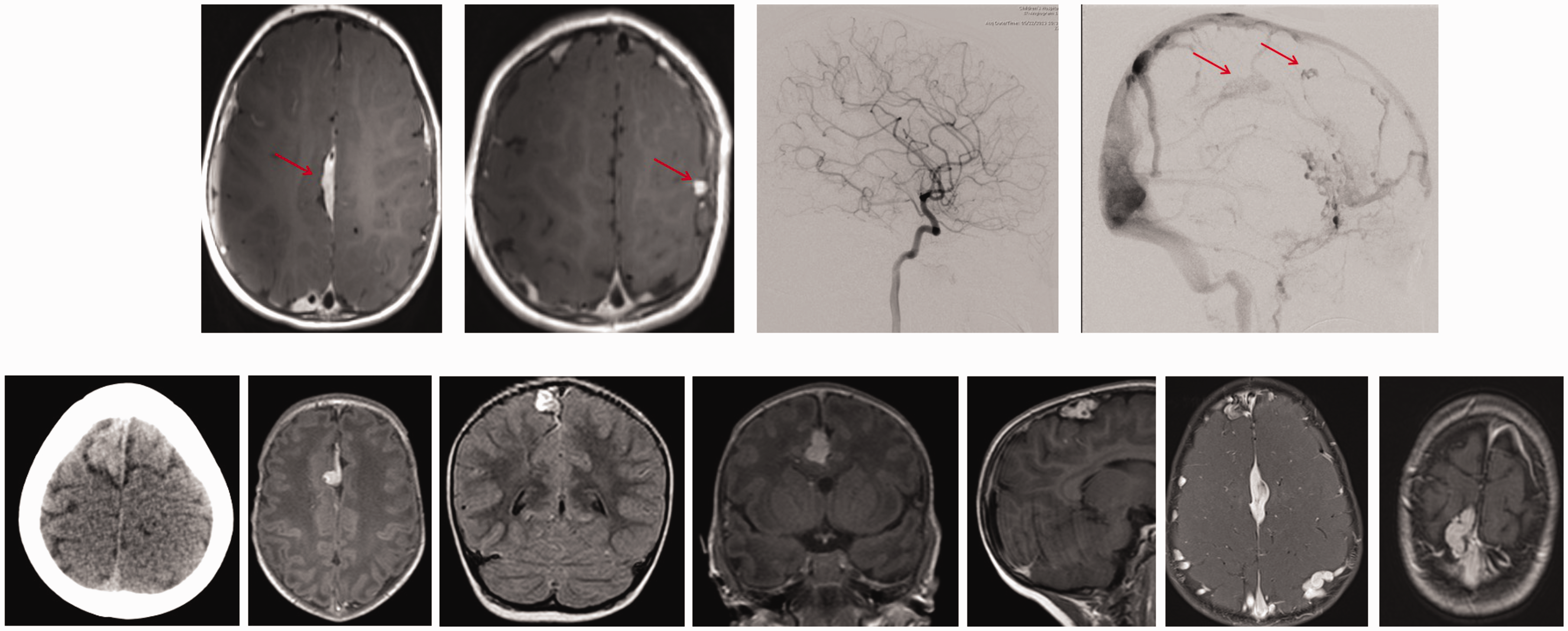
Several examples of interhemispheric icVM, ranging from far anterior to posterior. Top row: axial post-contrast MR images demonstrating an interhemispheric and left lateral icVM (left panels, red arrows), and lateral views of arterial and venous phases of injection of the left internal carotid artery in the same patient (right panels). Note absence of visualization of the icVM on the arterial phase of the angiogram, with visualization of contiguity with clear venous structures on the venous phase, Bottom row: Examples of interhemispheric icVM in different patients, ranging from far anterior to posterior. Note the characteristic compressible, multilobulated mass-like morphology, with vein-like enhancement and continuity with an adjacent venous structure.
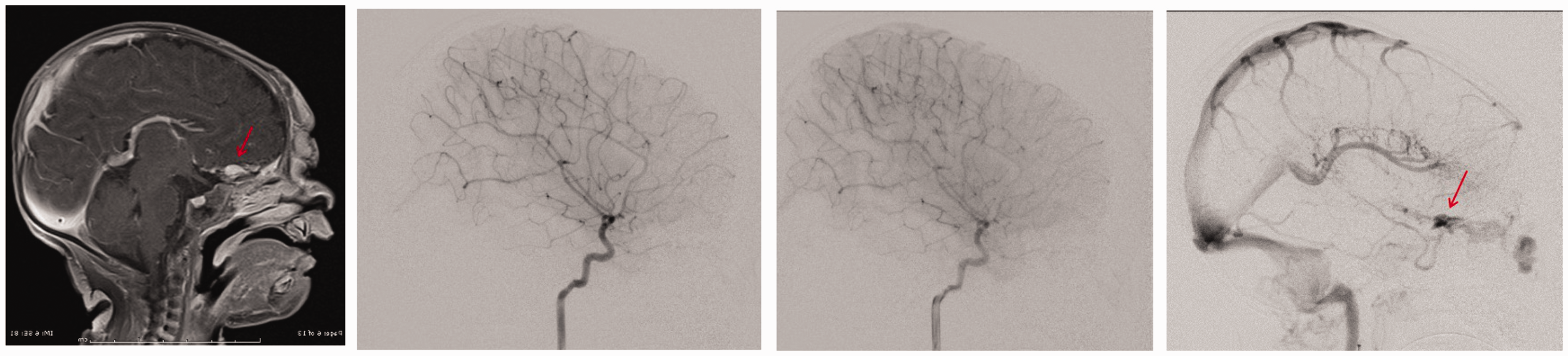
Basal frontal midline icVM (red arrows) on post-contrast sagittal MR (left panel). Right panels show arterial, capillary, and venous phases of a lateral view of the right internal carotid injection. Note non-visualization of the icVM on arterial and capillary phases and the contiguity of the icVM in this cases with a glabellar VM, with non-contiguity of the icVM with a DVA draining into an enlarged internal cerebral vein.
Of 19 patients harboring icVM, 9 (47.3%) had sinus pericranii along with icVM, 15 (78.9%) had associated large, complex extracranial venous malformations, and 3 (15.7%) exhibited neurocognitive delay. No patient had imaging evidence of dilated venous collaterals or diffuse “pseudophlebitic” venous clustering to suggest intracranial venous hypertension. There was no intracranial hemorrhage, neither clinically nor radiographically evident, in any patient in this cohort. Asymptomatic venous thrombosis in the superior sagittal sinus was seen in three patients, with evidence of partial recanalization in two and complete resolution in one patient, who was diagnosed prenatally on MRI. In patients in whom longitudinal imaging studies were available, there was usually no appreciable change over time in the caliber of the icVM relative to adjacent vascular structures, with the exception of one case that demonstrated waxing and waning in size of the malformation, as can be seen for extracranial VM (Figure 6). In addition to the icVM anomalous morphology, 4 of 19 cases showed delayed venous emptying of the malformation; in all the others, both opacification and emptying of the malformation were in phase with adjacent venous structures. Table 3 summarizes associated imaging and clinical features for each of the morphological subtypes of icVM. There was no arteriovenous shunting seen in any case (per the exclusion criteria). In no patient did the icVM spontaneously thrombose or disappear.
Top row: non-midline fusiform icVM, the right-sided example within a schizencephalic cleft. Bottom row: frontal angiographic views of a left internal carotid injection, showing non-visualization of the icVM on arterial and capillary phase images. The venous phase image on the extreme right was acquired several years after the image to its left, demonstrating the dynamic caliber of the icVM over time, neither shrinking nor growing in monotonic fashion; this dynamic appearance over time excludes interpretation of this lesion as being due to venous outlet stenosis with progressive pre-stenotic venous dilatation.
Associated findings and intracranial venous anomaly morphology, categorized as globoid, fusiform, and falcine.
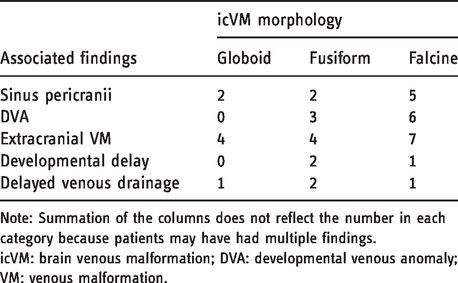
Note: Summation of the columns does not reflect the number in each category because patients may have had multiple findings.
icVM: brain venous malformation; DVA: developmental venous anomaly; VM: venous malformation.
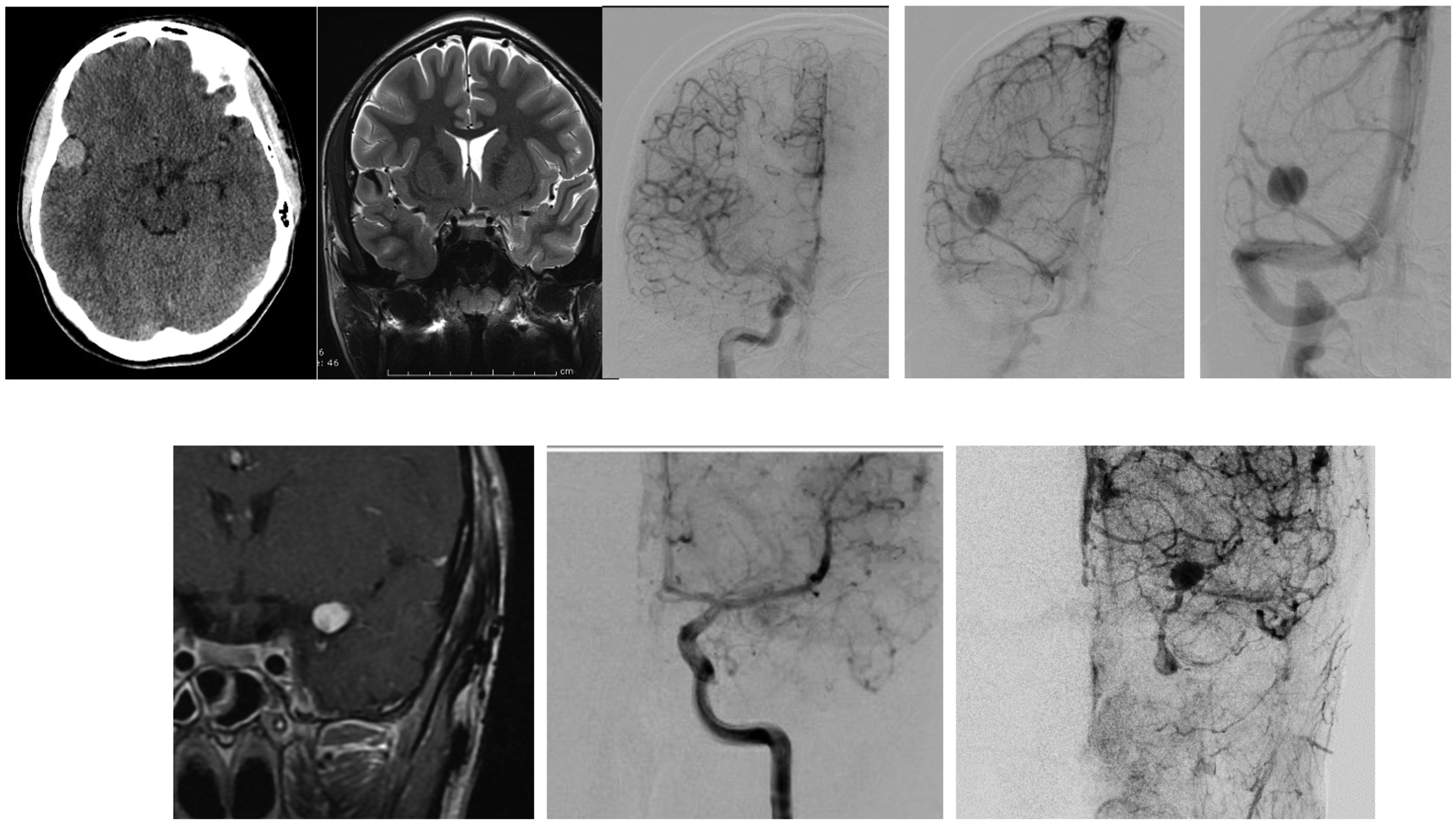
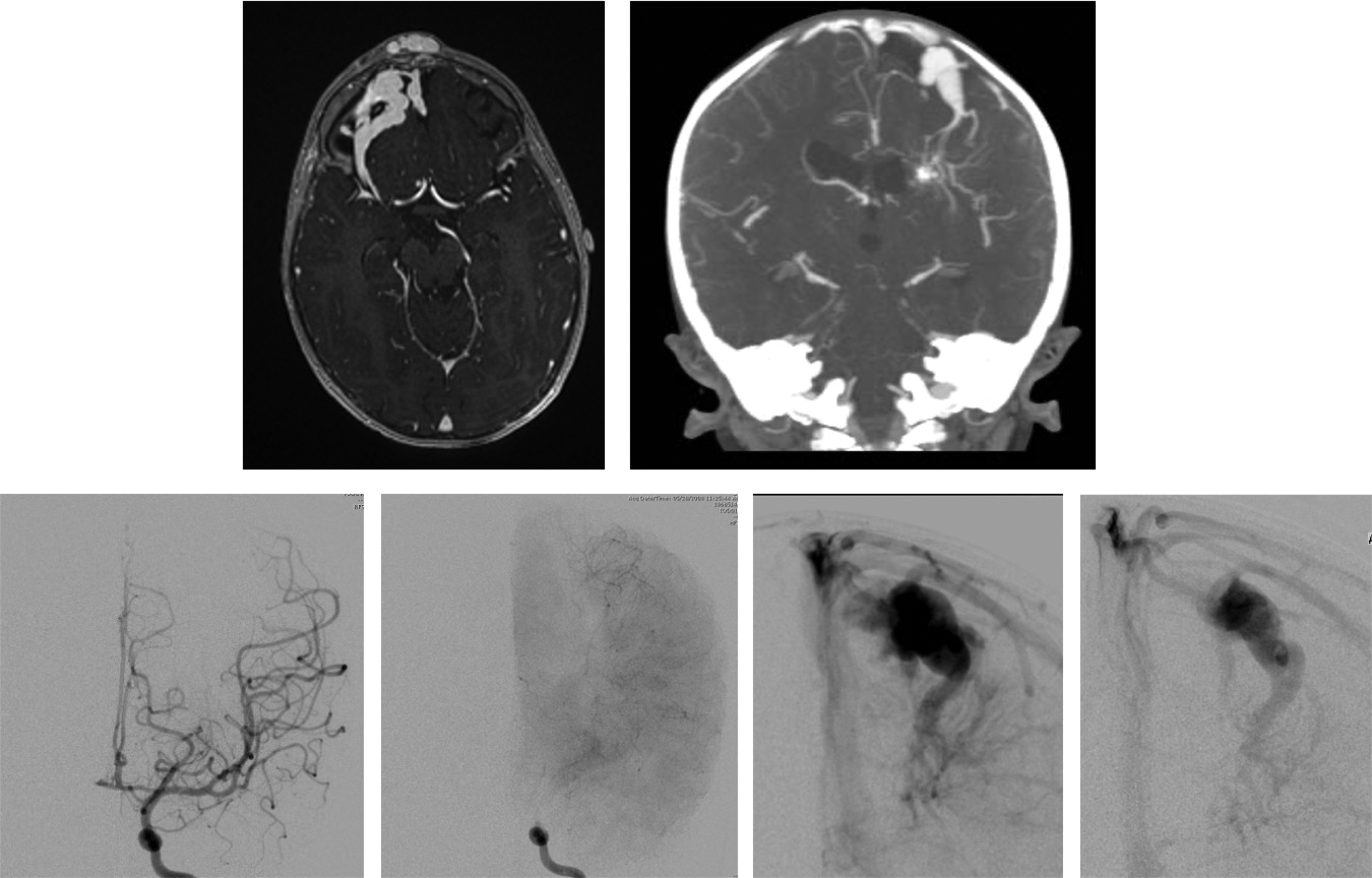
Globoid icVM morphology appearance on CT, MR, and angiography. Top row images are from one patient and bottom row images from another. Catheter angiography demonstrates the opacification in the venous phase, with delayed emptying.
In eight patients, the icVM lay subjacent to the extracranial VM; of these eight, five demonstrated communication between intracranial and extracranial VM via sinus pericranii or cavernous sinus drainage. In the six patients with extracranial venous malformations off midline, the icVM was always ipsilateral to the extracranial anomaly; three of these six icVM were subjacent to the extracranial. Multiple bilateral extracranial venous malformations were identified in six patients. Table 1 summarizes the icVM clinical and radiographic features we found for the cohort of 19 patients.
Discussion
The term “developmental venous anomaly” (DVA) was coined to stress its non-pathological status. 3 While the identification and characterization of the DVA were an important landmark, this entity does not describe the brain venous malformations we characterize here, which are similar in many ways to those encountered outside of the brain (see Table 3). icM constituted ∼2% of the total cohort of cerebrovascular anomaly patients reviewed at our tertiary academic referral center. Interestingly, none of the patients exhibited angiographic or other imaging evidence of intracranial venous hypertension or hemorrhage.
Within the icVM cohort, true DVA, sinus pericranii, and persistent falcine sinuses were found in 45%, 45% and 0% of the cohort, respectively. These three previously described venous variant conditions will be discussed in turn below. Extracranial venous malformations are also discussed, in order to highlight significant recent identification of associated genetic markers, which may prove relevant as well to icVM.
DVA
As detailed by Lasjaunias et al., 3 in addition to the characteristic morphology, DVAs consistently (1) drain normal cerebral tissue, (2) are associated with absence of a “normal” venous pathway to drain the territory, (3) drain into a normal extraparenchymal venous collector, and (4) opacify angiographically in the same angiographic phase as normal veins. DVAs have been associated with cavernomas, 4 de novo development of capillary telangiectasias within the DVA region, 5 diffuse enhancement 6 or increased cerebral blood volume 7 within their fields, other diffuse vascular pathologies, including head and neck venous/lymphatic malformations, 8 hereditary hemorrhagic telangiectasia, and sinus pericranii, and other entities 9 ; symptomatic variants of DVA have been described as well. 10 It has been hypothesized that DVAs are dysplastic vessels resulting from anomalous development at the level of the capillary bed. 9 Indeed, DVA-like channels have been recognized to occur in patients with Sturge-Weber syndrome, 3 in whom fundamental capillary abnormalities are a hallmark feature of the disease process attributed to a somatic mutation in GNAQ. 11
Sinus pericranii
Sinus pericranii (SP) occur when venous drainage of the brain bypasses the dural venous sinuses in favor of extracranial venous pathways via transcranial diploic channels. Most such drainage is non-obligate, i.e. alternative, intracranial venous drainage is available for the brain region in question, such SP can be therapeutically occluded safely. Most sinus pericranii are asymptomatic, 12 and in our population most often were found incidentally or on workup for associated venous malformation of the head or face. Classification schemes have been proposed on the basis of various hypothetical types and etiologies of SP, 13 only some of which contain vascular endothelium on histology. 14 It has been suggested that the association of SP with craniosynostosis and intracranial hypertension points the way towards a possible etiology, at least in some cases. 15 An association between SP and DVA has been well established. 15 , 16 Most importantly, SP are frequently associated with, and often in direct communication with, extracranial scalp or glabellar venous malformations, as was seen in five out of nine patients in our cohort with SP. In some cases such as these, there is obligate venous drainage from a DVA via SP into the extracranial VM, and the VM cannot be safely sclerosed or occluded without compromising brain venous drainage.
Persistent embryonic sinuses and venous sinus development
The superior sagittal sinus arises from the cranial aspect of the sagittal plexus, which is seen in developing embryos at the 20 mm stage (eight to nine weeks), 17 while the inferior sagittal sinus and straight sinus arise from the caudal aspect of the sagittal plexus as smaller channels involute.17–19 The sagittal plexus is enveloped by an primitive falx cerebri, 17 within whose leaflets lies the falcine sinus, connecting the vein of Galen and superior sagittal sinus. Involution of the falcine sinus usually occurs before birth, 17 , 18 and where it does not, some hypothesize that persistence is compensation for dysfunction in the development of the straight sinus. 20 , 21 Most commonly, persistent falcine sinus is seen in the setting of vein of Galen malformations (though not invariably in that setting). 17 , 18 , 20 However, association of persistent falcine sinus with many other abnormalities has been described as well, including brain AVMs, Apert syndrome, occipital encephalocele, Chiari malformations, agenesis of the corpus callosum, and osteogenesis imperfecta. 18 , 20
Tischfield et al. were recently the first to elucidate the genetic pathway related to the development of the cerebral venous sinuses. For arteriovenous differentiation, it has been shown that endothelial cell fate results from expression of pre-programmed genes within the involved cells themselves, with an additional differentiation developmental effect of flow through the developing vessels.22–25 In contrast, Tischfield et al. demonstrated that development of the venous sinuses results from paracrine effects from adjacent cranial and dural structures. Thus, rather than the vascular-developmental genes previously described, the mutation inducing venous sinus anomalies identified was in Twist1, which results in loss of Bmp2/4 expression in preosteoblasts in the mesoderm and dura, in turn resulting in skull and venous sinus defects in mice. 26 Human subjects with Twist1 mutations show segmental aplasia of one transverse sinus or sagittal sinus, as well as papilledema and enlarged optic nerve sheaths suggestive of increased intracranial pressures.
In terms of clinical implications for icVM, either those invested within the dural leaflets such as the falx or those whose downstream drainage sinus was hypoplastic due to the paracrine developmental effects described, such a configuration might result in intracranial venous hypertension, whereas an identical icVM with a patent downstream sinus might be clinically silent (as were all the icVM cases in our cohort).
Extracranial venous malformations
Extracranial venous malformations have been extensively described in terms of clinical manifestations, pathophysiology, imaging workup, treatment, prognosis, and increasingly, genetic markers. Extracranial VM are manifest as discrete lesions or as diffuse regional abnormalities, can be relatively isolated from or closely associated with the adjacent regional venous drainage, often exhibit sidedness when multiple, and may be associated with multifocal or diffuse conditions, such as blue rubber bleb nevus syndrome or multiple cutaneous and mucosal venous malformations (VMCM). 1 , 27
Genetic mutations in the TEK gene on chromosome 9p, encoding the endothelial cell tyrosine kinase receptor TIE2 have been implicated in the pathogenesis of venous malformations, both in familial germ-line form and as somatic mutations in up to 50% of sporadic cases.28–31 TIE2 mutations result in a gain of function, causing downstream activation of mTOR, signaling increased cellular growth and proliferation. Interestingly, another branch in the same genetic pathway involves PIK3CA mutations, which are found in 54% of VM (as well as in CLOVES and other overgrowth syndromes). 32 Promising early results suggest that some overgrowth patients with PIK3CA mutations might be effectively treated with rapamycin, an mTOR inhibitor. 33 Whether any of these mutations are found either in the germ-line or in the involved tissue of icVM patients remains to be seen. However, given that single mutations can result in both extracranial and intracranial arteriovenous lesions, 34 , 35 it would be surprising if the above genes implicated in extracranial VM were found not to be involved in icVM as well. Moreover, there is a long-standing observation documenting a clear association between DVA and extracranial VM and lymphatic malformation,7,36 with a more recent report showing these to be ipsilateral in 83% of cases and to involve the same metamere in 75%, 37 further buttressing the likelihood of a common genetic/developmental etiology.
Conclusion
We describe here intracranial pure venous malformations (icVM), which share many of the recognized features of extracranial venous malformations. Hallmark characteristics of icVM include: (i) patulous, dysplastic, non-cylindrical morphology (globoid, fusiform, or falcine), (ii) clear connection to the superficial or deep venous system of the brain or the dural sinuses, (iii) delayed venous emptying, (iv) ipsilateral location when associated with extracranial anomalies, and (iv) absence radiographic evidence of venous hypertension. No patient in our cohort manifested intracranial hemorrhage or clinically significant thrombosis. In no patient did the icVM spontaneously thrombose or disappear.
Venous malformations, both extracranial and icVM, share many characteristics that are distinct from DVAs, as summarized in Table 2. Our experience suggests that venous hypertension is not the cause of icVM, given that none of our cases manifested clinical or radiographic evidence of such. Rather, as has recently been shown for numerous other types of vascular anomalies, germ-line or somatic mutations are a likelier etiology. The underlying genetic pathways involved in the development of icVM remain to be elucidated, but may very well involve shared mechanisms and pathways with the extracranial venous malformations.
Comparison of characteristics of extracranial VM, intracranial VM, and DVAs.
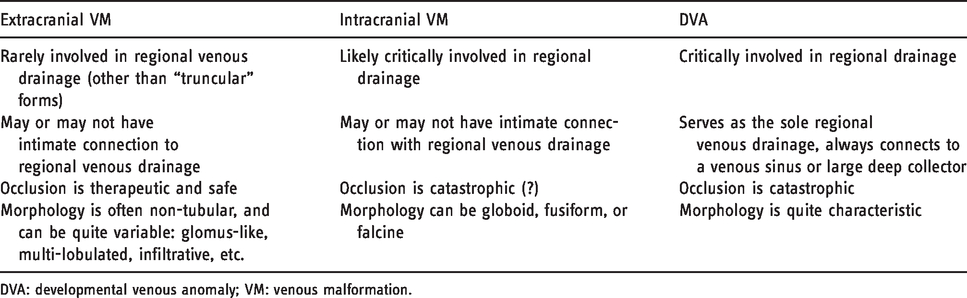
DVA: developmental venous anomaly; VM: venous malformation.
Footnotes
Acknowledgments
We would like to thank the staff at the Vascular Anomalies Center as well as the Cerebrovascular Surgery and Interventions Center at Boston Children’s Hospital for their academic and clinical collaboration, without which this study would not have been possible.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.