
Abstract
Management of intracranial stenosis remains controversial. Stenting for intracranial stenosis has been associated with high complication and restenosis rates. Morbidity may be related to the intracranial microcatheter exchange that is required in stent placement after the angioplasty. We present a technique in which we deploy an Neuroform Atlas stent through the lumen of a Gateway balloon microcatheter in order to avoid intracranial microcatheter exchange and the associated morbidity. We discuss advantages and pitfalls of this novel technique.
Introduction
Management of intracranial stenosis remains controversial. Although intracranial stenting initially showed promise, the Stenting and Aggressive Medical Management for Preventing Recurrent Stroke in Intracranial Stenosis (SAMMPRIS) trial in 2011 revealed a high 30-day stroke or death rate in stented patients (14.7%) compared to medically managed patients (5.8%). 1
Procedural morbidity may be related to the intracranial microcatheter exchange for stent placement after the angioplasty. We present a technique of deploying an Atlas stent through the lumen of a Gateway balloon microcatheter (Boston Scientific, Marlborough, Massachusetts) in order to avoid intracranial microcatheter exchange and the associated morbidity. We discuss advantages and pitfalls of this novel technique.
Technique
A female between the age of 50 and 60 with bilateral severe internal carotid artery (ICA) stenosis had her first stroke 11 months prior with right leg and arm weakness and was found to have infarcts in the left caudate nucleus and bilateral watershed areas (Figure 1). CTA revealed bilateral supraclinoid ICA stenosis. She was placed on aspirin, clopidogrel, and rosuvastatin. Eight months after the initial stroke she started to have transient right side weakness, approximately twice a week, with three episodes of bilateral leg weakness, leading to fall or near fall. Follow-up MRI showed increased foci of FLAIR hyperintensity in bilateral centrum semiovale, consistent with subacute watershed infarcts. Angiogram confirmed severe stenosis of bilateral supraclinoid ICAs with some pial collaterals from bilateral posterior cerebral arteries to bilateral anterior cerebral and middle cerebral artery territories. An anterior communicating artery was present. Given recurrent symptoms while on optimal medical therapy she was offered angioplasty and stenting for severe bilateral supraclinoid ICA stenosis (Figures 2 and 3) Verbal and written consent to publish de-identified images, history, and treatment course was obtained from the patient.
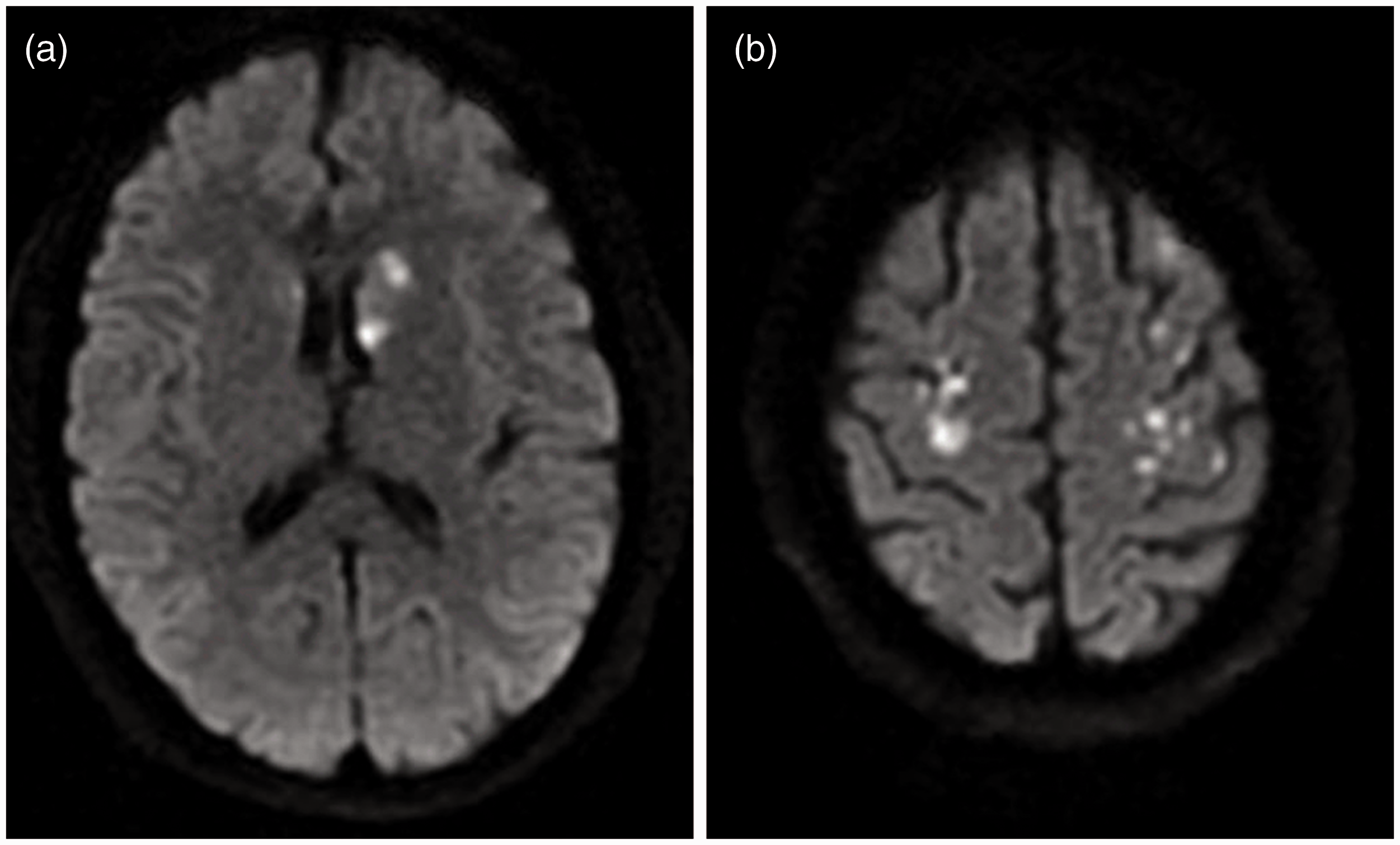
Presenting DWI images. (a) Acute infarcts in left caudate nucleus. (b) Bilateral watershed infarcts with some possible embolic infarcts.
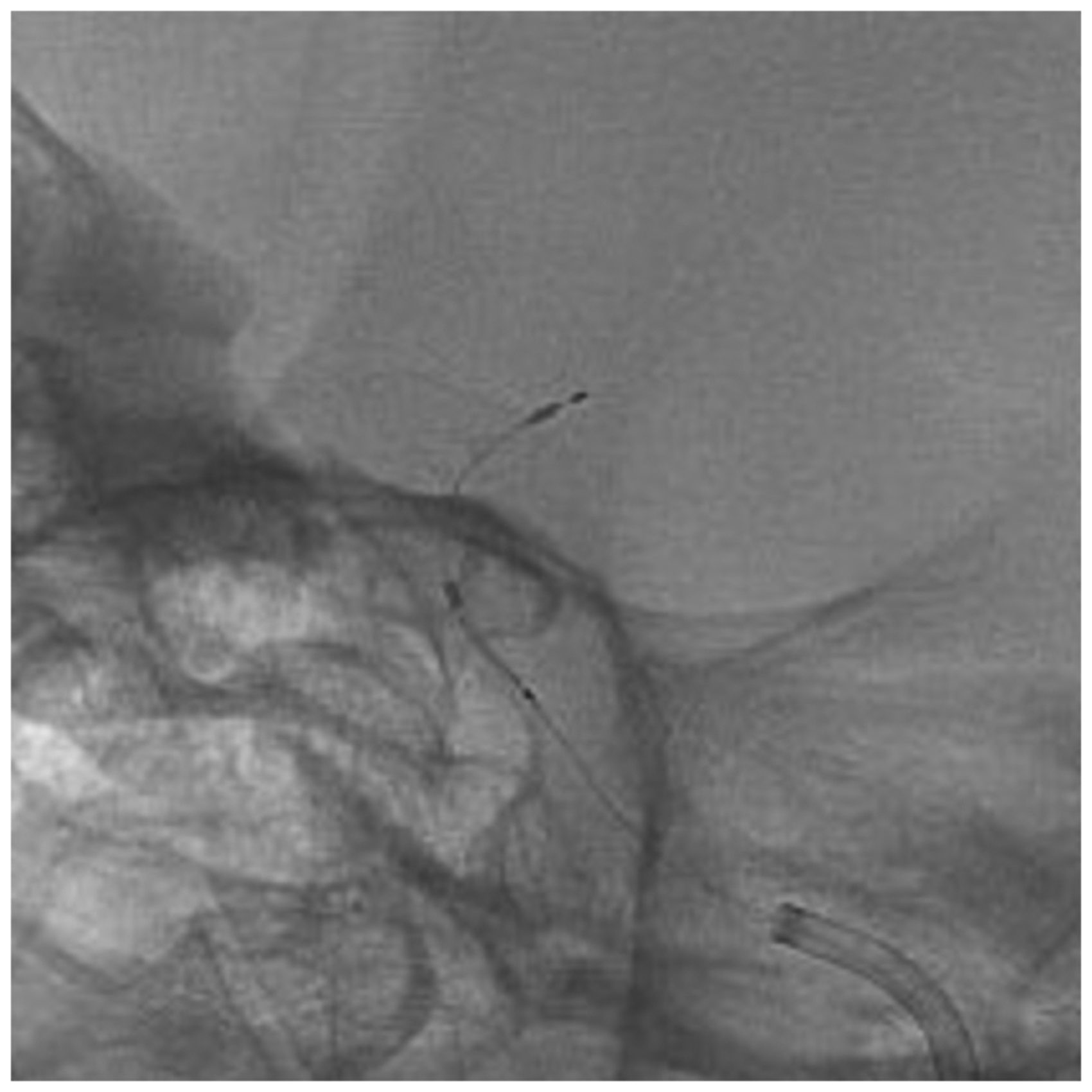
Stent deployment through balloon catheter. The distal markers of the stent is seen just inside the tip of the microcatheter, which is approximately 3 mm beyond the distal balloon marker, ready to be deployed in the left supraclinoid ICA.
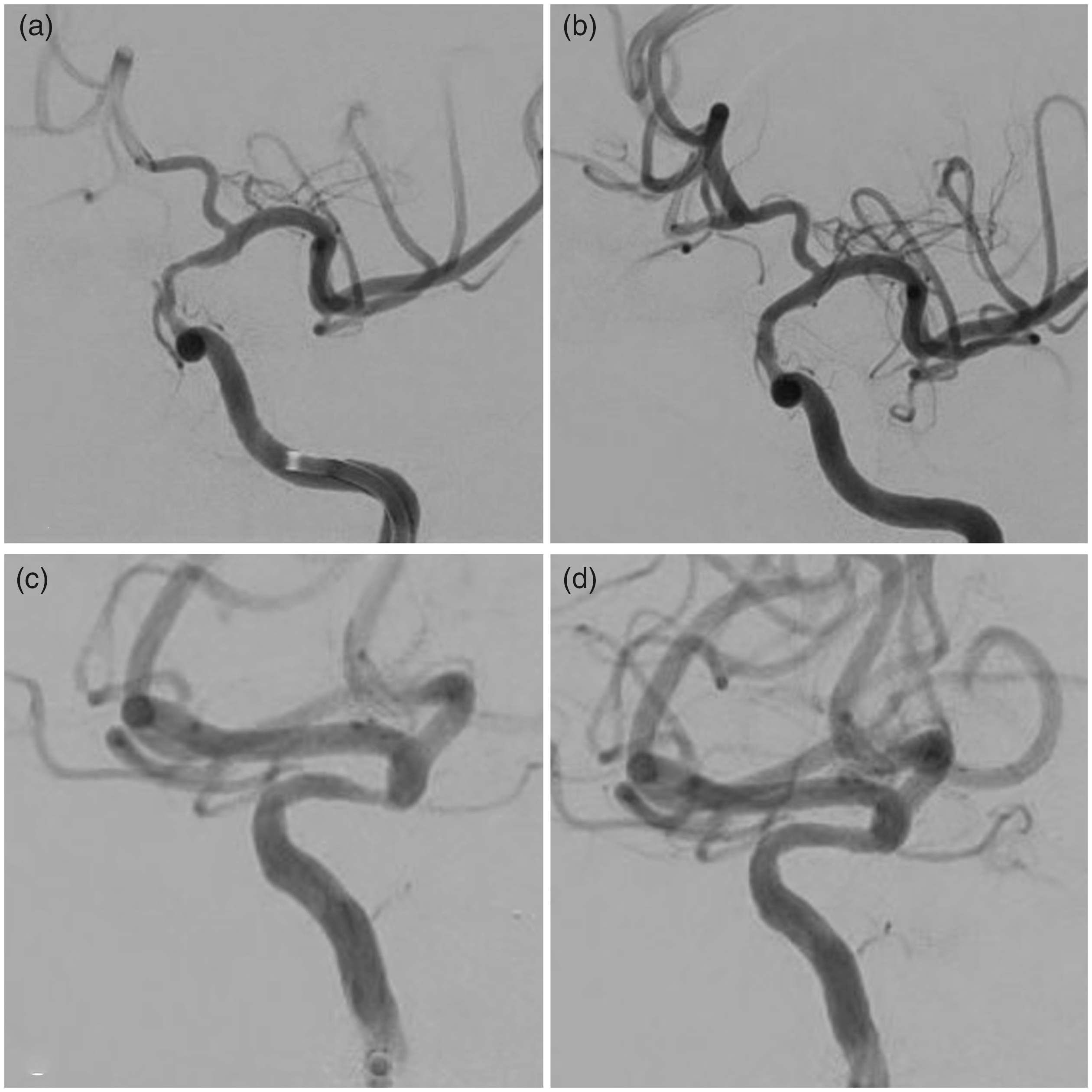
Angioplasty and stenting of bilateral supraclinoid ICA stenosis. (a) A 14.6 mm segment of 80% stenosis in the supraclinoid left ICA. (b) Markedly improved caliber and distal flow of supraclinoid left ICA on the follow-up angiogram two weeks later, which are even better than on the immediate post-stenting angiogram. The normal segment of left ICA measures 2.6 mm. (c) An 8.2 mm segment of >70% stenosis in the supraclinoid right ICA. (b) Less than 30% residual stenosis in the supraclinoid right ICA after angioplasty and stenting.
She first underwent stenting of the left ICA as her last symptom was transient right arm and leg weakness and the left side stenosis was more severe than the right side. We did not stent both sides in one setting for the concern of post-procedural hyperperfusion. To stent the left ICA lesion, a 6 French long sheath was advanced into the origin of left ICA and an intermediate catheter was placed into the petrous segment of the left ICA. A 2.5x15mm Gateway balloon catheter was navigated through the stenosis into the supraclinoid ICA segment over a 014 wire. After balloon position was confirmed, the balloon (with a nominal pressure of 6 atmospheres) was inflated to 3 atmospheres over 1 minute . The stenosis was fully dilated at this pressure without any residual waist. A 3x24 Atlas stent was advanced through the balloon catheter after deflation and was deployed in the supraclinoid ICA without difficulty. Post-stenting angiogram showed improvement of stenosis from 80% to 46%. Follow-up angiogram two weeks later showed further improvement of stented supraclinoid left ICA with <30% residual stenosis.
The patient had no further neurological symptoms and returned two weeks later for follow up angiogram and stenting of the right ICA stenosis. A 4x24mm Atlas stent was deployed into the supraclinoid right ICA through a 2.5x15mm Gateway balloon after angioplasty. Post-stent angiogram showed improvement of the right ICA stenosis.
Discussion
The SAMMPRIS trial exclusively used the Wingspan Stent System which was the only FDA approved stent for intracranial stenosis in 2011. The Wingspan Stent System requires an intracranial microcatheter exchange, which can lead to vessel injury. Four of the ten symptomatic hemorrhages (1.8% of stented patients) in the trial were attributed to guidewire perforation. 1 We aim to diminish the risk of guidewire perforation as well as operative time by eliminating the cumbersome microcatheter exchange step altogether and deploying the stent through a compatible balloon microcatheter. We have successfully used this technique in three additional patients without difficulty.
The Atlas stent is a self-expanding, open-cell nitinol stent that is designed to be delivered through the Excelsior SL-10 (0.0165 inches internal diameter) or Excelsior XT-17 (0.017 inches ID). We found that the Atlas stent can be advanced smoothly through the Gateway balloon catheter, which has a similar internal diameter of 0.0165 inches. The key technical maneuver is to sever the distal 3mm of the introducer sheath of the Atlas stent with a scalpel such that the introducer fits just into the hub of the Gateway catheter. A small gap may exist between the end of the introducer sheath and the hub of Gateway catheter, but the stent can still be loaded into the catheter with a slight push. Without this modification, the tapered introducer advances too far into the Gateway catheter, causing compression of the introducer sheath and thus restraining the passage of the stent into the catheter (Figure 4).

(a) The black stent within the clear introducer is stuck in the hub of the gateway balloon catheter (black arrow). (b) When the stent is removed from the hub, it is apparent that the stent is stopped 2mm short of the tip of the introducer sheath (black arrow). (c) The tip of the introducer sheath is cut off with a scalpel to allow the stent to pass through when placed in the Gateway hub.
The Wingspan stent system has been reported to have an in-stent re-stenosis rate ranging from 24.2% to as high as 45.2% in younger patients.2–4 The Wingspan stent has a strong radial force (0.0116 Newtons/millimeter (mm)) compared to self-expanding stents such as the Enterprise stent and the Atlas stent (∼0.0082 Newtons/mm), which may contribute to in-stent stenosis by stimulating inflammation and intimal hyperplasia. 5 A lower radial force may be sufficient to prevent elastic recoil after angioplasty while avoiding vessel wall inflammation caused by excessive outward radial force. 6 Follow-up angiogram in this case confirmed that the radial force of Atlas stent was sufficient to continue improving vessel caliber after the procedure. The Enterprise stent has been used in patients with intracranial atherosclerosis with lower re-stenosis rates ranging from 2.94% to 24.7%; however the Atlas stent has yet to be investigated.7,8
Cuellar et al. reported use of the Atlas stent through the Coyote ES OTW angioplasty balloon which is a balloon designed for peripheral vascular use and is available in lengths 20mm to 40mm. 9 The Gateway balloon is better suited for this purpose as it is specifically designed for intracranial use and is available in lengths 9mm to 15mm. We have found that a balloon length of 15mm maximum is usually adequate to treat the area of severe stenosis and also decreases the risk of traction injury to distal branch perforators that can occur from straightening a longer curved segment.
One feature to be aware of is that the balloon catheter may kink and prevent stent deployment if it is not deflated prior to advancing the stent through the balloon segment. Inflation stiffens the balloon, making this segment inflexible, and thus predisposing the catheter to kinking when the stent is pushed against the balloon. One may consider advancing the stent to the cavernous segment during balloon inflation to save procedure time or overcome severe proximal tortuosity, and then deflate the balloon before the final stage of stent deployment.
Another feature to consider is that the distal marker of the Gateway balloon marks the end of the balloon but is several millimeters proximal to the end of the microcatheter. The distance from the marker to the end of the catheter is approximately 11mm for the 1.5mm balloon and 5mm for balloons 2mm and larger. Therefore the distal point of stent deployment should be estimated at the end of the microcatheter rather than at the distal radiopaque balloon marker. We place the distal balloon marker at the distal end of the stenosis in order to ensure that the stent covers just beyond the distal diseased segment when it is deployed.
Conclusion
We present a novel technique in which we deploy the Atlas stent through the Gateway balloon catheter for treatment of intracranial stenosis which avoids intracranial microcatheter exchange.
Footnotes
Authors’ Contribution
All authors made a substantial contribution to the design and drafting of the manuscript. All authors contributed to and approved the final revisions of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written and verbal consent to publish images, history, and treatment course was obtained from the patient.