
Abstract
Background
Anterior communicating artery aneurysms are the second most common type of intracranial aneurysm and have a high incidence of rupture. Intraprocedural rupture can lead to a high mortality and morbidity rate, representing a major challenge in emergency endovascular treatment of ruptured anterior communicating artery aneurysms.
Methods
We performed a retrospective review of 344 consecutive patients with emergency endovascular treatment of ruptured anterior communicating artery aneurysms. Patients were grouped into intraprocedural rupture and non-intraprocedural rupture groups according to whether intraprocedural rupture occurred. Demographic and clinical factors, vessel-related factors and therapy-related factors were compared between the two groups.
Results
Intraprocedural rupture occurred in 11 patients (3.2%). Univariate analysis showed that hypertension, the occurrence of vasospasm, aneurysm size, aneurysm angle and a high aspect ratio value were significantly associated with intraprocedural rupture (P < 0.05). Multivariate analysis showed that hypertension odds ratio (OR, 9.799; P = 0.007), the occurrence of vasospasm (OR, 10.121; P = 0.002) and a high aspect ratio value (OR, 10.571; P = 0.006) were independent risk factors for intraprocedural rupture.
Conclusions
A history of hypertension, the occurrence of vasospasm and a high aspect ratio value are independent risk factors for intraprocedural rupture among patients with ruptured anterior communicating artery aneurysms.
Keywords
Introduction
Intracranial Aneurysms (IAs) have an overall prevalence of up to 3.2% 1 in the adult population worldwide and the incidence continues to increase yearly. Spontaneous subarachnoid haemorrhage (SAH) usually arises from the rupture and bleeding of an IA and is a devastating and potentially life-threatening disease. IAs tend to occur at bifurcations and vessel curvatures and anterior communicating artery aneurysms (ACoAAs) are the second most common type of IA and have a high incidence of rupture. 2 Recent advancements in techniques and devices have made a great number of ACoAAs a suitable target for treatment with endovascular coil embolization. 3 According to the International Subarachnoid Aneurysm Trial, endovascular therapy for ACoAAs yields a better clinical outcome than traditional microsurgical clipping treatment in patients with ruptured aneurysms. 4
Despite the remarkable evolution of endovascular therapy for IAs, this intervention is inherently associated with serious complications, even at experienced centres. Intraprocedural rupture (IPR) is one of the most devastating complications with high mortality and morbidity rates, and is inevitably encountered by the majority of neurosurgeons, even at high volume experienced centres. The present study demonstrated that the incidence of IPR ranges from 2.8% to 5.2%, and the risk of functional impairments and death related to IPR can reach 63%. 1 Therefore, early diagnosis and preoperative assessment of risk factors associated with IPR for ACoAAs can lead to the prevention of deteriorated clinical outcomes. Unfortunately, the risk factors for IPR remain unclear and have not been completely investigated in previous studies. There are many possible mechanisms and risk factors associated with IPR, but the findings from previous studies are contradictory.5,6 Most previous studies investigated the potential risk factors for IPR by merging both ruptured and unruptured aneurysms and overlooked the differences in the natural courses between the two. In addition, ignorance of the differences in the locations and timing of treatment may be responsible for these conflicting results.
Thus, to avoid patient-related bias and provide an ideal internal control for variables, such as morphological features, the aim of this study was to investigate the role of demographic and clinical factors, vessel-related factors, and therapy-related factors in patients undergoing IPR as well as to identify the independent risk factors related to IPR in the emergency endovascular treatment of ruptured anterior communicating artery aneurismal haemorrhage from a large population sample.
Materials and methods
This study was a retrospective single-centre analysis approved by the ethics committee of the First Affiliated Hospital of Dalian Medical University. All patients provided written informed consent before inclusion in the database.
Patients selection
All consecutive patients in our institutional database who presented with a diagnosis of aneurismal SAH and ACoAAs on computed tomography angiography between January 2010 and December 2019 were included in our study. The exclusion criteria were as follows: (1) non-endovascular treatment; (2) timing of treatment >48 h; (3) non-aneurismal subarachnoid haemorrhage or inability to identify which aneurysm ruptured; (4) patients with ruptured IAs undergoing conservative or aneurysm clipping treatment and (5) incomplete clinical date or angiographic imaging.
Endovascular procedure and IPR definition
All procedures were performed after discussion and consensus among two experienced interventional neurosurgeons. A loading dose of 450 mg clopidogrel was administered before 2 h of emergency stent deployment. 7 All patients were treated under general anaesthesia and systemic heparinization. After femoral sheath placement, digital subtraction angiography (DSA) was performed in patients harbouring unruptured aneurysms to confirm the target location preciously. Then, the guiding catheter was navigated into the target artery and all aneurysms were embolized with detachable coils with or without assistance of balloons or stents. IPR was defined as a microguidewire, microcatheter or coil located beyond the confines of the aneurysm wall as assessed by angiography. If an IPR occurred, heparin was reversed with protamine immediately, and coiling was completed as rapidly as possible, as presented in an illustrative case (Figure 1).

Representative case of a 47-year-old female with a ruptured intracranial aneurysm at the right ACoA. (A) The patient was admitted to hospital with a sudden headache and CT scan demonstrates subarachnoid haemorrhage. (B) Three-dimensional volume rendering by CT angiography demonstrated the aneurysm arising from ACoA. (C) DSA showed a regular aneurysm with narrow neck. (D) Perforation with contrast extravasation occurred after the superselective microcatheterization of the aneurysm. (E) Immediate coil embolization was undertaken and the cessation of contrast leakage can be observed on angiography. (F) Postoperative angiography depicted contrast media retention in the lateral ventricle.
Date collection
Demographic and clinical factors, vessel-related factors and therapy-related factors were collected.8,9 Demographic and clinical factors included age, sex, previous hypertension, diabetes, coronary artery disease, smoking status and preoperative neurological status (Hunt-Hess grade). Vessel-related factors include occurrence of vasospasm (defined as arterial thinning or prolonged contrast media retention in circulation during interventional operation) and aneurismal morphology features. The latter was assessed using three-dimensional DSA images that were retrieved from the archives at the Philips Integris 3D-RA Release 4.2 workstation (Figure 2) and included size (maximum distance between the neck and dome of an aneurysm), neck width (neck size >4 mm or dome/neck ratio <1.5 is defined as wide neck), shape (irregular aneurysms were defined as aneurysms with daughter sacs or a lobulated shape), flow angle (defined as the angle between the maximum height of the aneurysm and the main blood vessel), aneurysm angle (defined as the angle between the aneurysm neck and maximum height of the aneurysm), aspect ratio (AR, maximum vertical height of the aneurysm/neck width) and size ratio (SR, maximum height of the aneurysm/parent vessel diameter). All of these measurement methods have been defined and depicted in previous studies.10–12 Therapy-related factors include treatment modality (coiling only or balloon/stents- assisted coiling) and occlusion density (judged according to the grading system proposed by Roy et al. 13 and classified as complete occlusion (complete obliteration), subtotal occlusion (residual neck) and inadequate occlusion (residual aneurysm)).
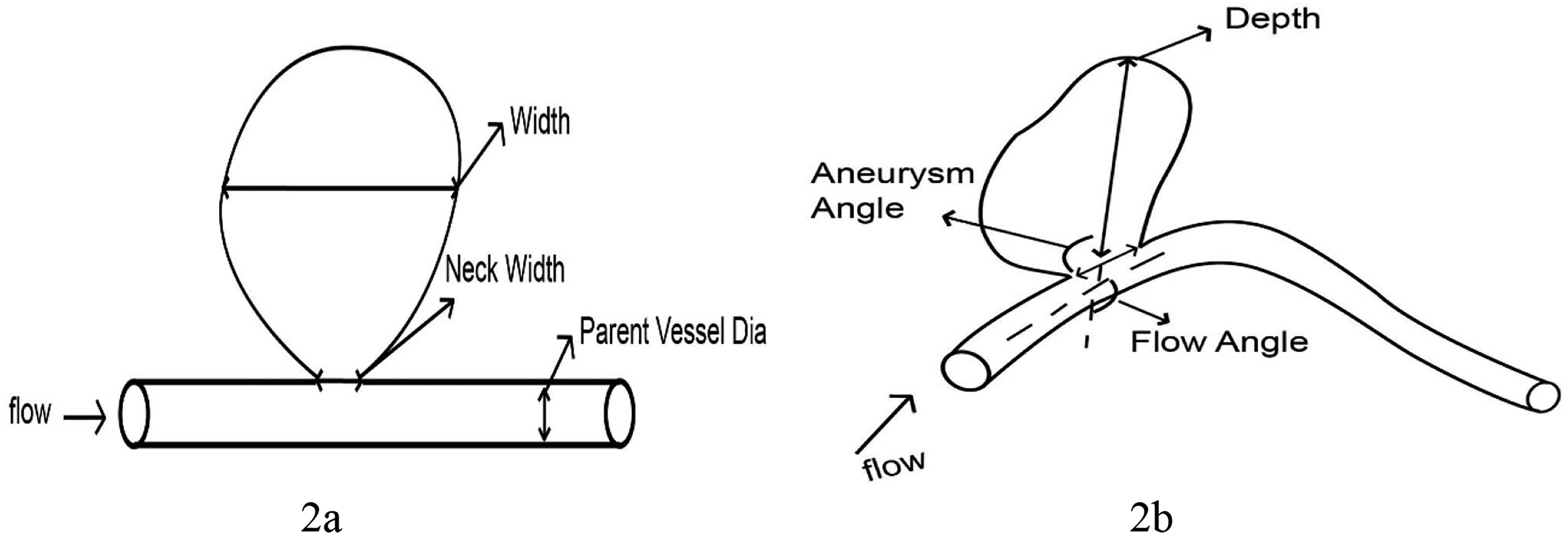
Measurement definitions: neck width is defined as the maximum cross-sectional diameter of the neck of the aneurysm; depth is defined as the longest diameter between the neck and the dome; width is defined as maximum diameter perpendicular to depth; aneurysm angle is defined as the angle between the aneurysm neck and depth of the aneurysm; flow angle is defined as the angle between the vector of depth and the vector of the centre line of the parent artery.
Statistical analysis
We performed univariate and multivariate analyses using the SPSS software package, version 22.0 (IBM, Armonk, New York). Categorical variables were expressed as numbers and percentages and continuous variables were reported as the mean values ± standard deviation. The chi-square test or Fisher’s exact test was used for categorical variables. Regarding continuous variables, Student’s t-test was used for normally distributed date and the Mann–Whitney U test was used for nonnormally distributed data. Univariate analysis was performed to identify the potential variables associated with IPR. All variables with significance at P < 0.1 on univariate analysis were included in multivariate logistic regression analysis to explore the independent risk factors for IPR. P < 0.05 was considered statistically significant. The clinically relevant cut-off point when the value reached its maximum was defined with receiver operating characteristic curves.
Results
Patient characteristics
Ultimately, 344 patients met the inclusion criteria and were enrolled in the study. All the included patients were categorized into IPR and non-IPR groups according to whether IPR occurred. Of the 344 patients, IPR occurred in 11 cases, for a rate of 3.2%. A summary of individual cases is depicted in Table 1.
Details of 11 cases with intraprocedural rupture (IPR).
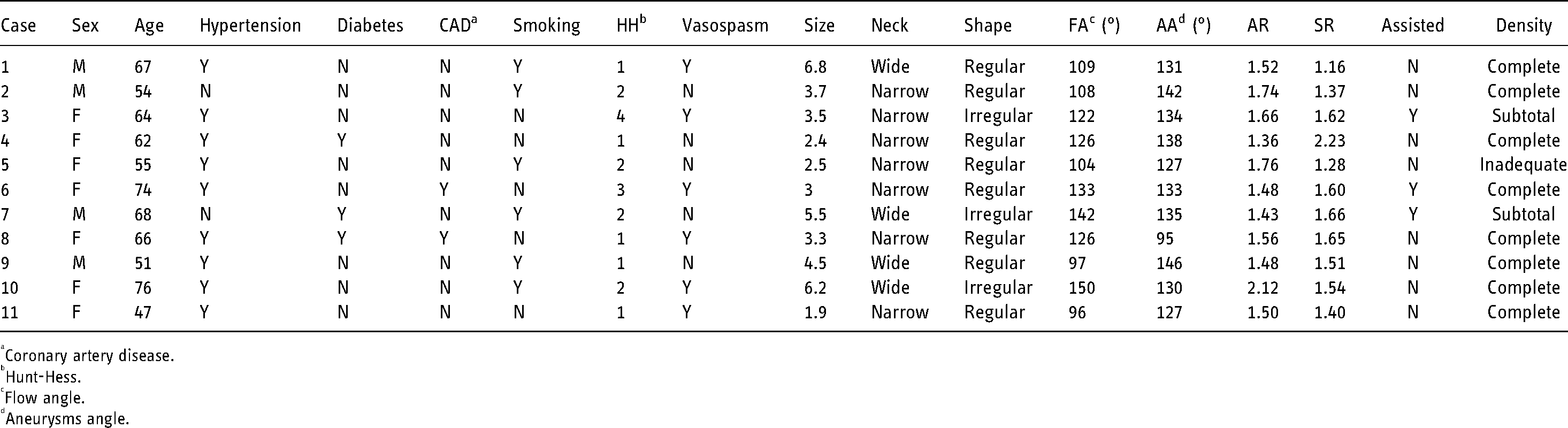
Coronary artery disease.
Hunt-Hess.
Flow angle.
Aneurysms angle.
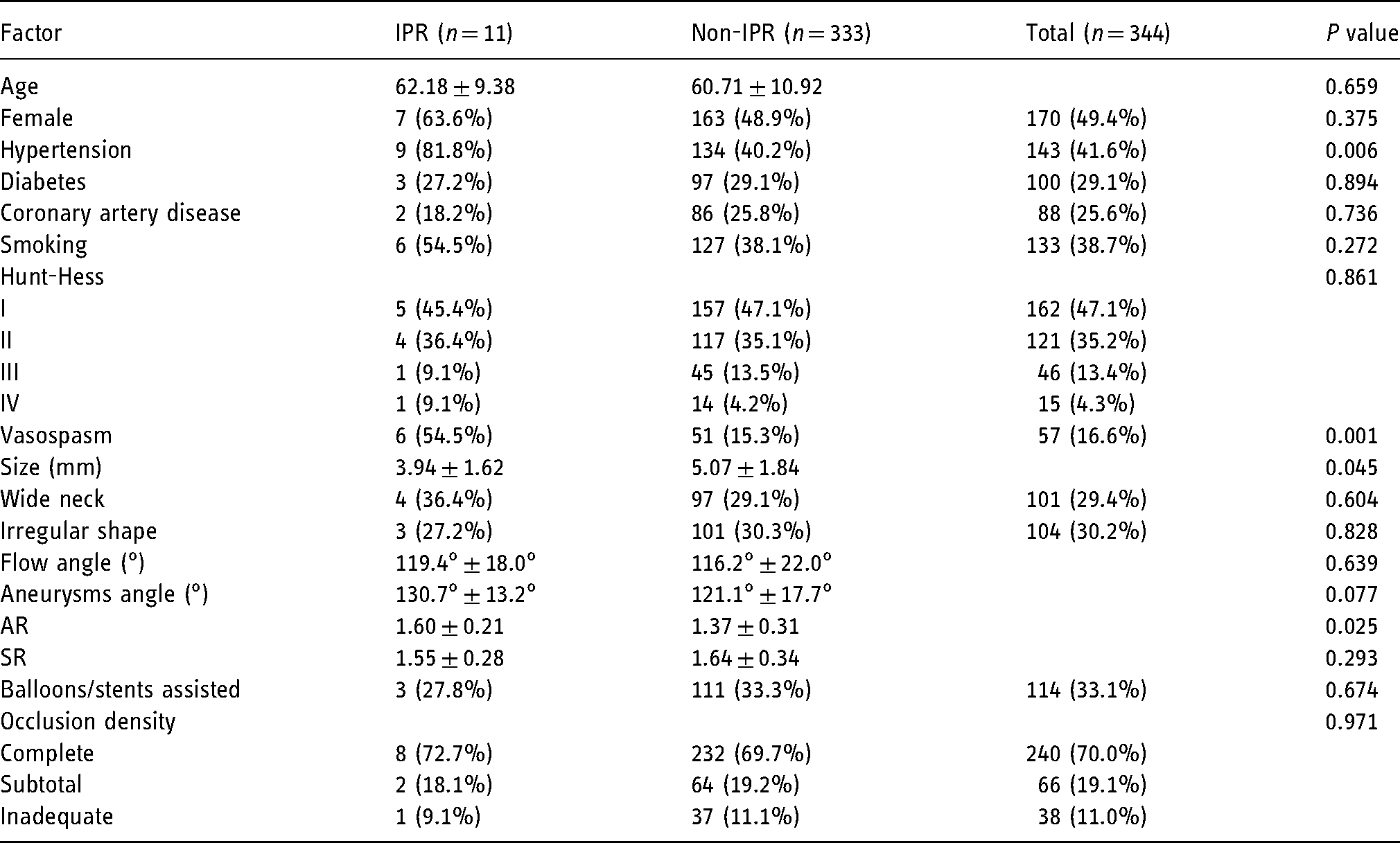
Of the 344 patients, the average ages of the non-IPR group and IPR group were 62.18 ± 9.38 and 60.71 ± 10.92 years, respectively. The non-IPR and IPR groups included 163 (48.9%) and 7 (63.6%) female patients, respectively. Of 344 patients in the study, 143 patients (41.6%) were hypertensive, 100 patients (29.1%) had diabetes, 88 patients (25.6%) had coronary artery disease and 133 patients (38.7%) were smokers. The ∼82.3% of the patients were classified as having a good clinical grade at admission (Hunt and Hess grades 1 and 2). In total, the mean aneurysm size was 5.0 ± 1.8 mm, mean aneurysm angle was 121.45° ± 17.67°, mean flow angle was 116.31° ± 21.86°, mean AR was 1.37 ± 0.34 and SR was 1.64 ± 0.33. A total of 114 patients (33.1%) were treated with balloon/stent-assisted coiling. In total, 240 patients (70.0%) made a dense embolization. Detailed demographic and clinical factors, vessel-related factors and therapy-related factors in the IPR and non-IPR groups are listed in Table 2.
Univariate analysis of individual factors related to intraprocedural rupture (IPR).
IPR risk factors
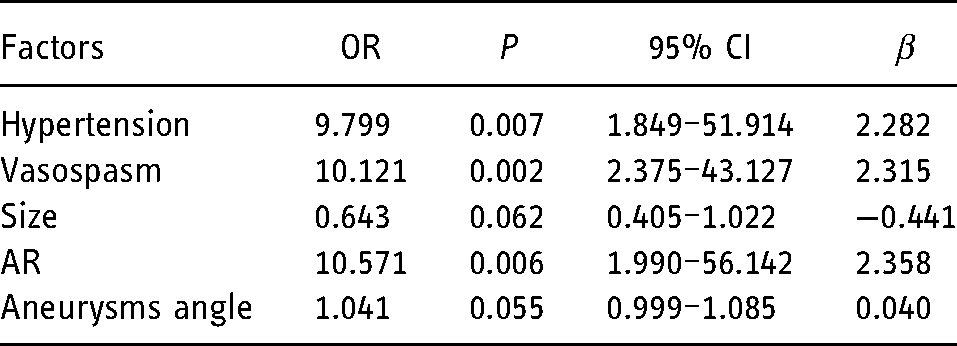
In the univariate analysis of factors associated with IPR, hypertension, occurrence of vasospasm during the operation, aneurysm size, aneurysm angle and AR value in the IPR group were significantly different from those in the non-IPR group and were included in the multivariable analysis. A forward conditional logistic regression analysis is given in Table 3. The model showed that hypertension odds ratio (OR, 9.799; P = 0.007), the occurrence of vasospasm (OR, 10.121; P = 0.002) and a high AR value (OR, 10.571; P = 0.006) increased the risk of IPR. The threshold value of AR was 1.425 (Figure 3) and the area under curve value for the variable was 0.797 (95% CI, 0.738–0.857).
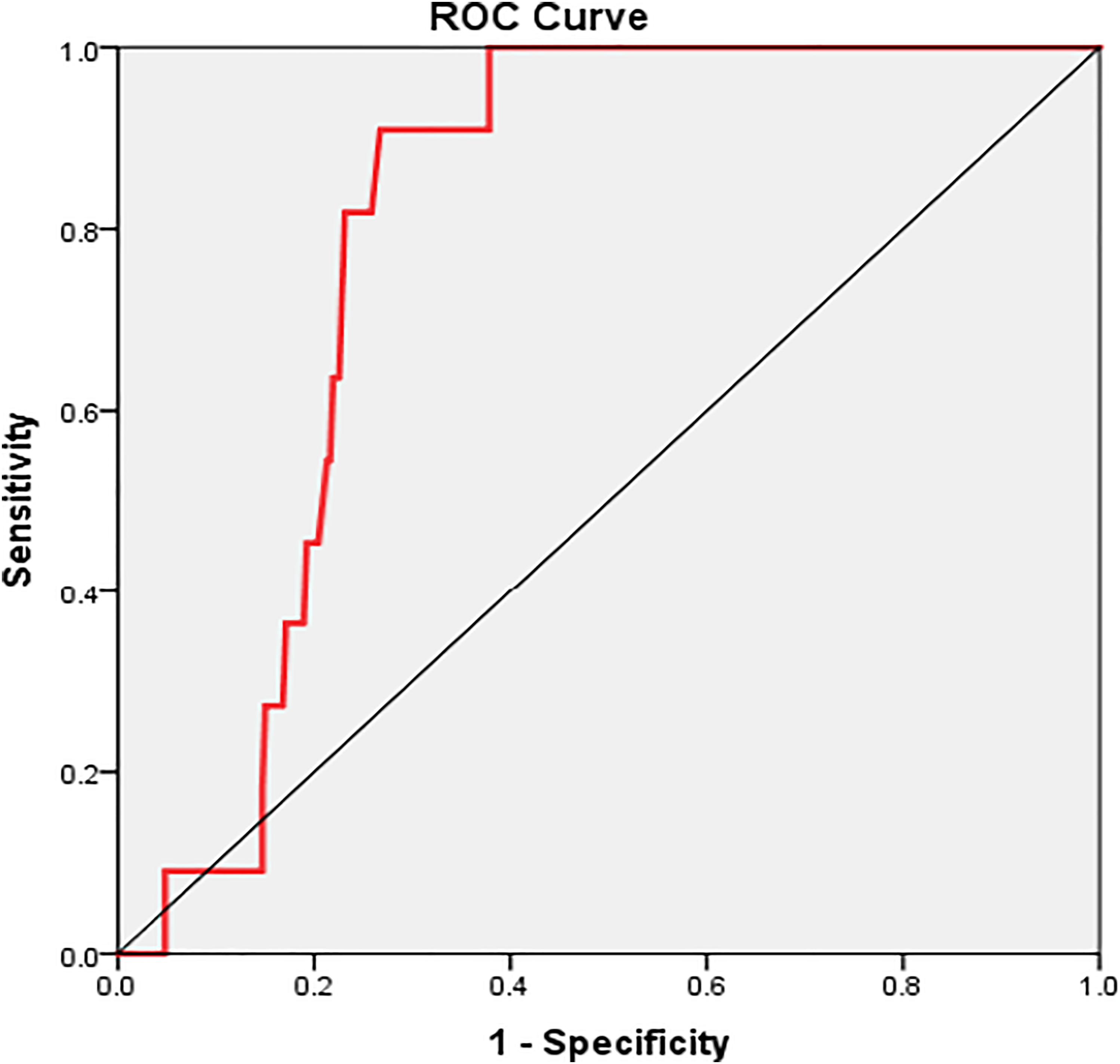
The area under the ROC curve for the AR was 0.797 and the cut-off point for AR was 1.425. ROC: receiver operating characteristic; AR: aspect ratio.
Multivariate analysis of factors associated with intraprocedural rupture (IPR).
Discussion
Endovascular therapy has been a preferred treatment option for ruptured aneurysms and the benefits of endovascular coiling for ruptured ACoAAs have been clearly addressed in previous studies. 2 However, adverse effects associated with embolization remain inevitable and should be highlighted. Few studies have investigated the risk factors for IPR of ruptured aneurysms at specific sites with a sufficient number of cases. In this study, we provided a large sample-based analysis and investigated ruptured ACoAAs. Multivariate analysis revealed that hypertension (OR, 9.799; P = 0.007), vasospasm (OR, 10.121; P = 0.002) and AR value (OR, 10.571; P = 0.006) were independent risk factors for ruptured ACoAAs. No statistically significant differences in other factors were noted. This is the first study to directly investigate the risk factors for ruptured ACoAAs.
Hypertension is the most common clinical chronic disease and the most important risk factor resulting in cerebrovascular disease. 14 Previous studies have shown that hypertension is closely related to the occurrence of IAs. However, the relationship between hypertension and IPR remains controversial. In our study, we found statistical significance between the hypertension and IPR groups rather than between other demographic and clinical factors and IPR. Generally, chronically elevated blood pressure increases the difficulty of intraoperative blood pressure management for anaesthesiologists. In addition, long-term hypertension may cause pathological changes in the patient's cerebral blood vessels, such as arteriosclerosis, accelerated hardening of the cerebral blood vessels with less elasticity and irritation of a vulnerable site of the aneurysm. 14 In addition, stiff vasculature will aggravate the spasm response of cerebral blood vessels, making it more difficult to operate on the microcatheter and microguidewire during the operation, causing perforation.
Many previous studies have reported that the occurrence of cerebral vasospasm significantly increases the rupture risk of aneurysms and affects the prognosis of patients with intracranial ruptured aneurysms. 15 ACoAAs are generally small in diameter and more susceptible to vasospasm. Thus, we compared the incidence of vasospasm between the IPR and non-IPR groups. We found that the occurrence of cerebral vasospasm significantly increased the incidence rate of IPR in ruptured ACoAAs. When vasospasm occurs in the parent artery, it can cause an abrupt, marked decrease in the diameter of blood vessels. With the accumulation of tension, it is difficult for the surgeon to accurately control the direction and strength of the microguidewire and microcatheter, thus increasing the risk of IPR. This conclusion reminds us that once intraoperative vasospasm occurs, full attention must be paid to the release of tension on the microcatheter and avoid aggravation of vasospasm. If necessary, intravascular administration of drugs, such as nimodipine, can be used to alleviate the degree of vasospasm.
AR is an important morphological parameter and a high AR represents a higher tortuosity of IAs. Many previous studies suspected that AR was associated with the occurrence of the IPR. 16 However, these studies focussed on multiple locations and no consensus threshold value was reached. In our study, we found a statistical trend among the IPR and non-IPR groups. Specifically, the AR value was significantly higher in the IPR group and a height of AR value ≥1.425 was a better predictor of rupture in the operation of ACoAAs. From a haemodynamic perspective, complex and varied wall shear stress caused by a high AR value plays an important and crucial role in endothelial proliferation and apoptosis, which is associated with atherosclerotic lesions and elastin degradation, thus weakening the arterial wall and facilitating rupture. 16 In addition, as the neck of the aneurysm becomes relatively narrow, blood stasis in the aneurysm will aggravate the hypoxia and inflammatory reaction of the aneurysm wall, which increases the risk of IPR. 17
Several risk factors, such as size, shape, aneurysm angle and therapy factors, were reported to be related to the occurrence of IPR. Mitchell found that small aneurysms (<4 mm) were more prone to rupture during surgery after measuring the diameter of more than 600 cases of intraoperative ruptured aneurysms. 18 In our study, the size of aneurysms was highly associated with IPR in univariate analyses, but this factor did not achieve significance in multivariate regression analysis. This might be attributed to insufficient statistical power in the IPR group (n = 11) and that statistics may be influenced by other factors, such as shape or neck width. Irregular aneurysm shape leads to disturbance in hemodynamic, making it an underlying factor of aneurysm rupture. However, Fan did not observe a significant correlation between IPR and irregular shapes, which was consistent with our study. 19 Generally, the increasing aneurysm angle resulted in greater wall shear stress inside the dome. In our study, the aneurysm angle did not correlate with rupture, which was consistent with the conclusion of Ye et al. 20 Ye found that the aneurysm angle can help predict the formation of ACoAAs but not rupture.
Therapy-related factors include occlusion density and treatment modality. Ihn et al. 21 found that overpacking of the aneurysms, oversized and stiff coils are responsible for a higher rate of IPR. The technique of stent-assisted endovascular embolization of ACoAAs has been proposed to improve the occlusion rate and decrease the number of coils. It was reported that stent or flow diverter placement was a protective factor against IPR. 22 In our study, we found no significant difference in therapy-related factors between the two groups. This finding may be attributed to the fact that the surgeons participating in this study have abundant clinical experience in embolization degree and operation method selection.
There are some limitations in our study. Firstly, our study employed a retrospective design using a single-centre database. Considering the low incidence rate of IPR, there is clearly a need for prospective, multicentre and large-scale trials in the future. Secondly, this database did not include the types of stents, use of intermediate catheters, history of subarachnoid haemorrhage, or use of vasodilators during surgery. These factors were potentially unmeasured confounders in this research. Additionally, we only considered ruptured ACoAAs in this study, which might have biased the selection of patients, and the results are potentially not applicable to other sites of IAs.
Conclusions
In this case-control model, we observed that ruptured ACoAAs with a history of hypertension, occurrence of vasospasm and a high AR value were independent risk factors for IPR during emergency treatment and more attention should be given to aneurysms with the abovementioned characteristics during clinical practice.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.