
Abstract
Background and objective
To determine the risk factors for recurrence after endovascular embolization of posterior communicating artery aneurysms (PcomA).
Methods
We retrospectively analyzed a cohort of 163 patients harboring 172 PocmAs who were treated with endovascular embolization from January 2019 to December 2020. The patients were divided into recurrence and stable groups depending on outcome. Univariate and logistic regression analyses were performed to determine the potential risk factors of recurrence during follow-up.
Results
Of the total 163 patients harboring 172 aneurysms, 107 were treated with simple coil occlusion and 65 were treated with stent-assisted coil embolization. There were significant differences in aneurysm sizes and use of non-stent-assisted coil embolizations between the groups (P < 0.05). The incidence of saccular aneurysm and Raymond grade were significantly higher in the recurrent group than in the stable group (P < 0.01). After variable selection, Raymond grade, aneurysm size, saccular aneurysm and non-stent-assisted coil embolization were included in further analysis. Binary logistic regression analysis revealed significant associations with non-stent-assisted coil embolization (P = 0.007), packing density (P < 0.001) and Raymond grades II (P < 0.001) and III (P = 0.002).
Conclusion
Non-stent-assisted coil embolization, as well as packing density and Raymond grades II grade III are associated with recurrence after endovascular treatment of PcomA.
Keywords
Introduction
Posterior communicating artery aneurysm (PcomA) occurs in approximately 25% of all patients with aneurysms. 1 Currently, the treatment for PcomA involves microsurgical clipping. With the development of novel devices and minimally invasive surgery, endovascular treatment has become important for the treatment of intracranial aneurysms. Despite the fact that endovascular therapy has improved patient outcomes and has produced lower mortality than microsurgical clipping, the postoperative recurrence rate of 30% remains a difficult problem. 2 A number of studies have determined that the size of aneurysm, occurrence of rupture, Hunt-Hess grade, packing density, saccular aneurysm, and presence of stent often affect long-term stability post-embolization.3–5 Nevertheless, the risk factors for PcomA recurrence post-embolization remain unclear. This single-center retrospective review was designed to determine potential risk factors for recurrence of PcomA.
Materials and methods
Study participants were recruited from the Department of Neurosurgery, The First Affiliated Hospital of Wannan Medical College. The study was performed in accordance with the Declaration of Helsinki. This study was approved by our Institutional Review Board, which waived the requirement for written informed consent.
Patients and aneurysm characteristics
From January 2019 to December 2020, we enrolled 193 patients (209 PcomAs) who underwent endovascular embolization. The study end point was the timing of recanalization during follow-up, 30 patients were excluded (16 cases with 20 aneurysms were lost follow-up, 8 cases with 10 aneurysms were vegetative states and 6 cases with 7 aneurysms were deaths). Ultimately, 163 patients with 172 aneurysms and met inclusion criteria. As shown in Figure 1. Inclusion criteria were as follows: (1) diagnosis of PcomA using angiography; (2) complete clinical history data and follow-up more than 6 months. Exclusion criteria were as follows: (1) no PcomA; (2) lack of completed clinical history data or loss to follow-up; and (3) non-endovascular treatment. Morphological data were obtained using digital subtraction angiography (DSA). Aneurysm size was categorized as small (<7 mm) or large (≥7 mm) according to previous experience. 6 An aneurysm was considered to have a wide neck if its size was ≥4 mm and/or if the D/R (dome-to-neck ratio) was <2. 7 On admission, patients with Hunt-Hess grades of 0–3 were classified as lower grade, and those with Hunt-Hess grades of 4–5 score were classified as high grade.8,9 Computerized tomography (CT) findings suggestive of subarachnoid hemorrhage or detection by lumbar puncture of hemorrhagic cerebrospinal fluid defined ruptured aneurysms. Abnormal protrusions in the aneurysm wall are defined as saccular aneurysms. Those aneurysms appeared again while complete occlusion after 3 month and/or residual aneurysm size had increased after incomplete occlusion were regard as recurrent aneurysm. 10
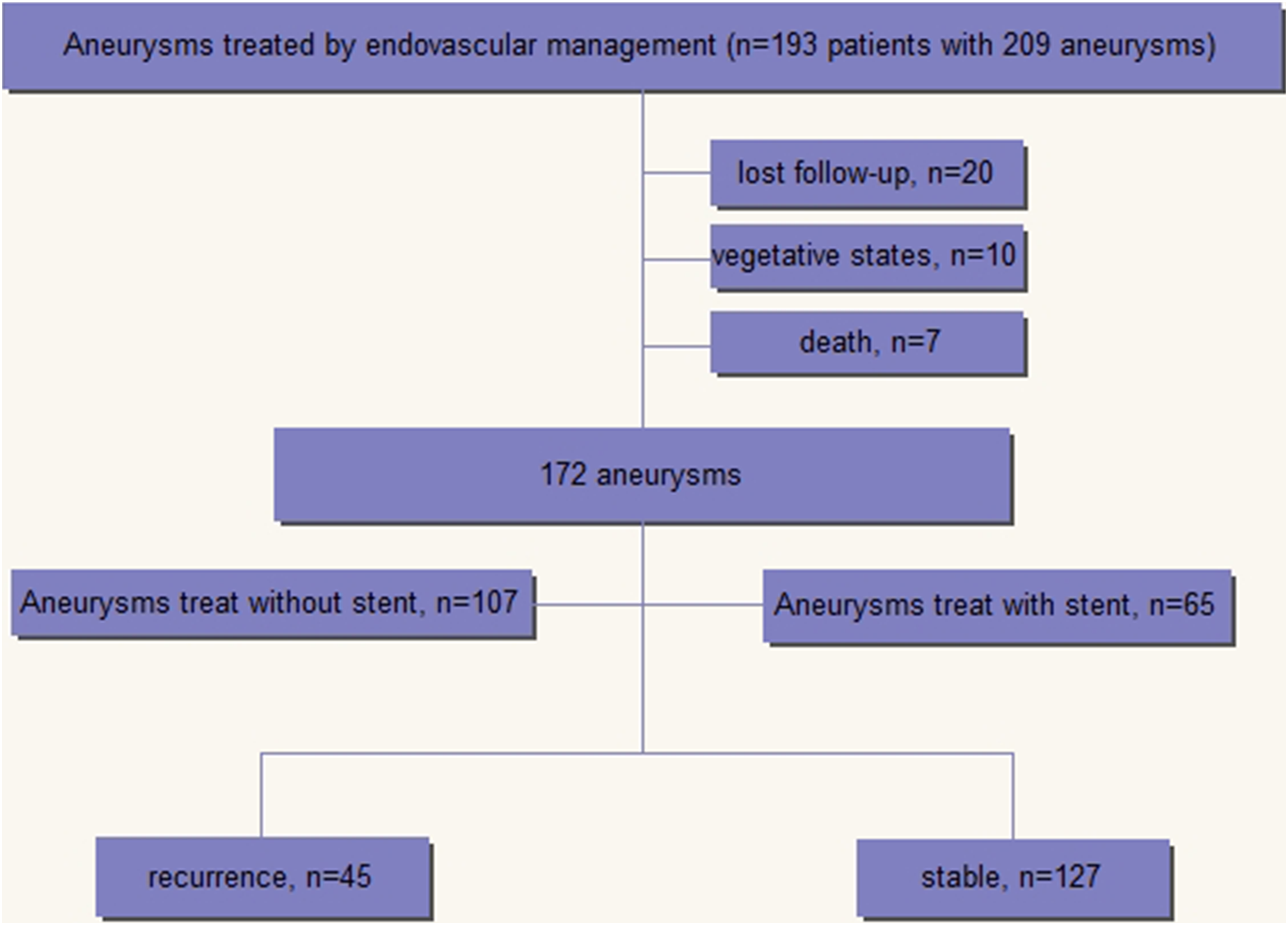
Flow chart shows overall study process.
Endovascular procedure and pharmacologic therapy
All patients were operated on under general anesthesia and received heparin intra-operatively (80 U/kg) to maintain activated clotting times 2–3 times the baseline value. A 6-F guiding catheter was introduced through a femoral sheath into the carotid artery. All procedures were performed on a biplane angiographic system. Whether we performed simple occlusion or stent-assisted occlusion depended on the characteristics of aneurysm. All operations were conducted strictly according to the manufacturer's instructions. Cosmos, helical and complex coils (all from MicroVention Co., US) were used for simple occlusion. Enterprise (Cordis Co., US), LVIS (MicroVention Co.) and Solitaire stents (Ev3 Co., US) were used for stent-assisted occlusion.
Patients with unruptured aneurysms who required stent-assisted coil embolization were medicated with dual antiplatelet therapy 3–5 days prior to stent deployment (aspirin 100 mg/d + clopidogrel 75 mg/d). For those with ruptured aneurysms, aspirin and clopidogrel (each 300 mg) were administered orally or per rectum 2 h before stent deployment. All patients were subsequently treated with aspirin 100 mg and clopidogrel 75 mg daily for 6 weeks, followed by aspirin only indefinitely. No antiplatelet drugs were taken before or after embolization for simple occlusions.
Angiographic follow-up
DSA was used to measure the degree of aneurysm embolization immediately postoperatively. Mean angiographic follow-up was 11.4 ± 3.9 months (median, 11 months; range 6–24 months). The results were assessed by at least two neurosurgeons. The immediate postoperative angiogram and follow-up images were studied to assess the degree of aneurysm occlusion using the Raymond–Roy Grade Scale (RRGS)11,12: Complete occlusion was considered Raymond grade I, residual neck was considered Raymond grade II and dome filling was defined as Raymond grade III.
Statistical analysis
All data were analyzed using SPSS Statistics version 20.0 (SPSS, Inc., Chicago, Illinois, USA). Data were presented as mean ± standard deviation (SD). Pearson chi-square test or Fisher's exact test were used to evaluate categorical variables and Student t-test or Mann-Whitney U test for continuous variables. As predetermined, variables with P-values <0.05 in the univariate analysis were included in the binary logistic regression analysis. P < 0.05 was considered statistically significant.
Results
Baseline characteristic of patients with PcomA
A total of 172 PcomA in 163 patients completed the follow-up. Patient characteristics are summarized in Table 1. The cohort consisted of 67 males and 105 females, with a median age of 53 years (range 21–87 years). The numbers of patients who had a medical history of hypertension, diabetes mellitus were 59 (34.3%) and 48 (27.9%), respectively. Fifty-seven (33.1%) were former or current smokers. There were no significant differences in gender, age, hypertension, smoking and diabetes between the groups (P > 0.05; Table 1).
Baseline characteristics of the patients with posterior communicating artery aneurysms.
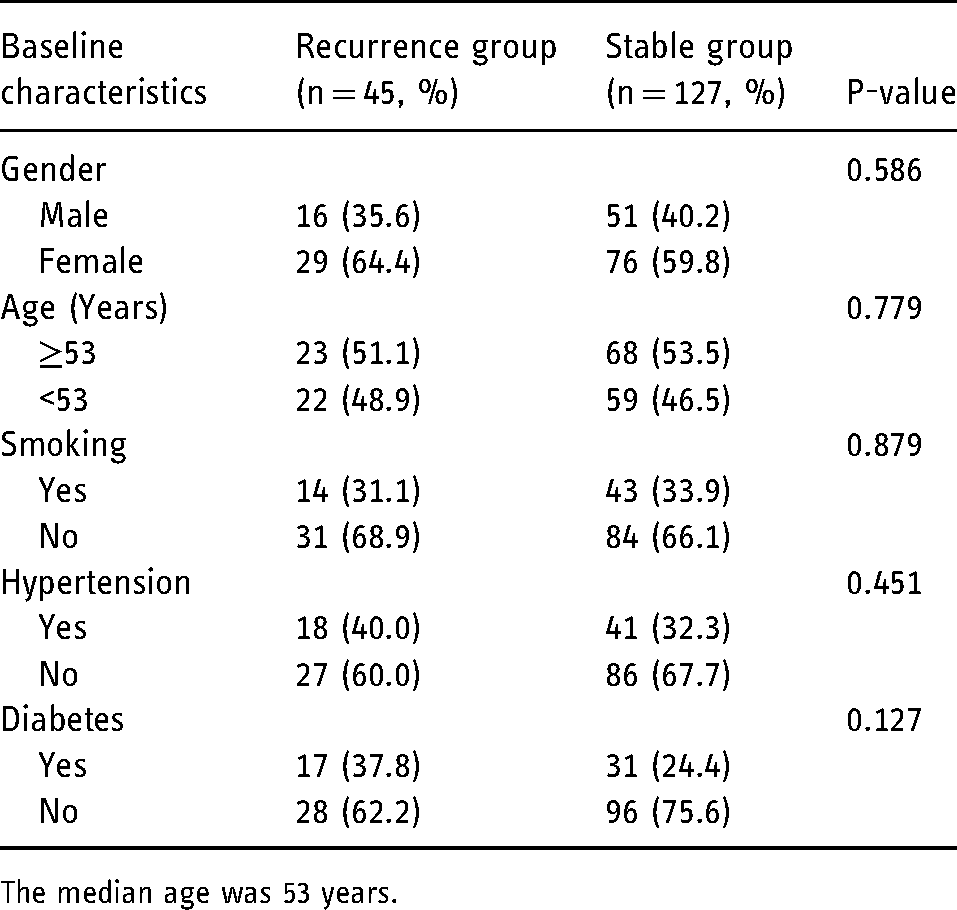
The median age was 53 years.
Characteristics of PcomA between recurrence and stable groups
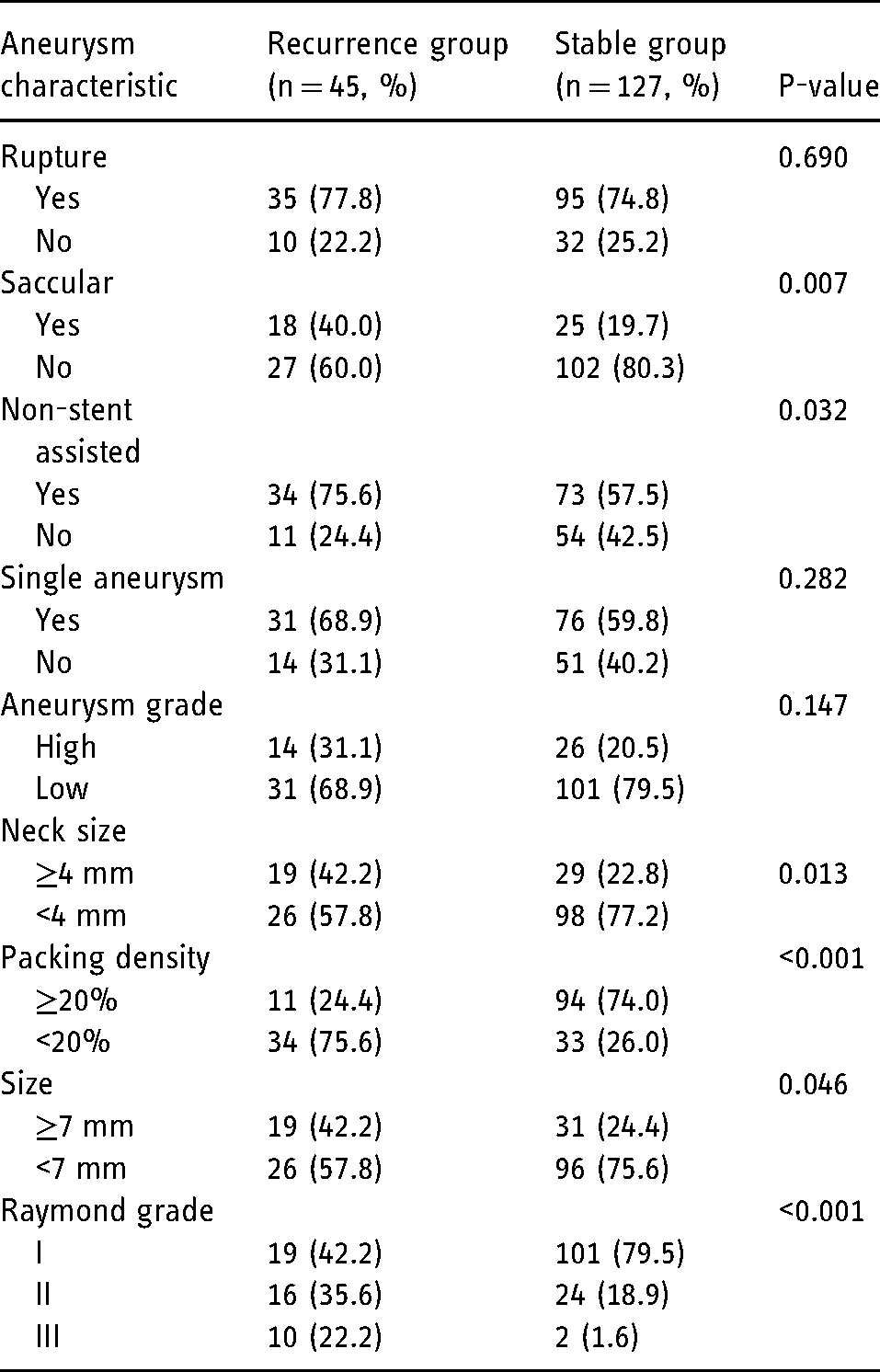
After univariate analysis between two groups, we found that aneurysm size (P = 0.046), neck size (P = 0.013), Raymond grade occlusion classification (P < 0.001), saccular aneurysm (P = 0.007), packing density (P < 0.001) and non-stent assisted coil embolization (P = 0.032) were significantly associated with recurrence. These confounders were corrected for using logistical regression analysis (Table 2).
Characteristics of posterior communicating artery aneurysms.
Logistic regression analysis of aneurysm recurrence post-embolization
Stent-assisted coil embolization, packing density and Raymond grade were independent variables. Aneurysm recurrence post-embolization was the dependent variable. Significant variables in the univariate analysis were entered in binary logistic regression analysis. After logistic regression analysis, there were significant associations with non-stent-assisted coil embolization, as well as packing density and Raymond grades II and III (all P < 0.05; Table 3).
Logistic regression model assessing risk of recanalization in posterior communicating artery aneurysms.
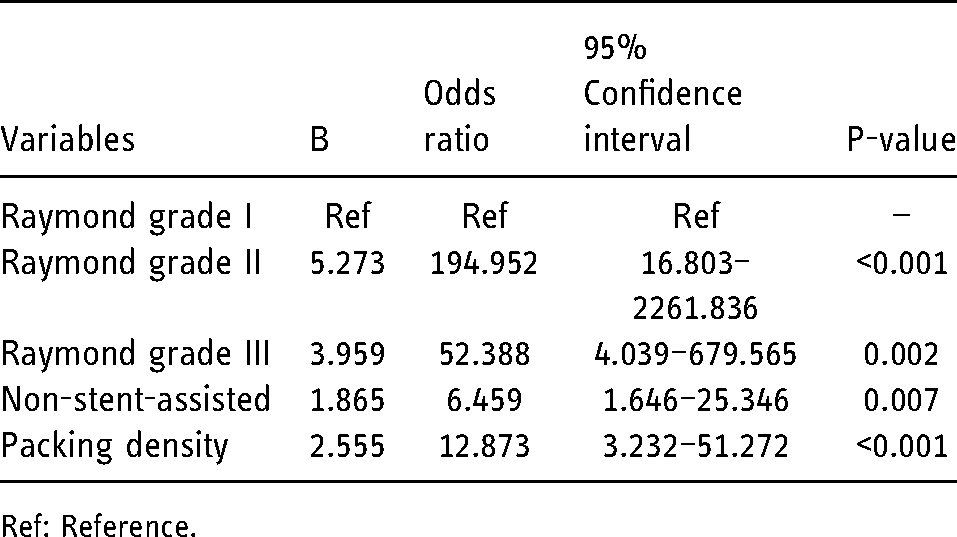
Ref: Reference.
Discussion
With improved perioperative outcomes and trends toward minimally invasive surgery, endovascular treatment for intracranial aneurysm have become increasingly popular.13,14 Despite this surge in popularity and studies showing good results, increasing numbers of surgeons have questioned the long-term efficacy of endovascular treatment for aneurysms. The purpose of our study was to determine the potential risk factors for recurrence of PcomA.
Aneurysm size influences the incidence of recurrence of aneurysms post-embolization. Some studies11,15 showed that aneurysm size >10 mm was an important factor for recurrence, and the incidence of recanalization post-occlusion would increase 0.12% for every 1% increase in diameter. Park et al. 16 reported that aneurysm size ≥8 mm was an independent risk factor for recurrence after endovascular treatment. A similar study 6 of 400 paraclinoid aneurysms managed with endovascular treatment reported that aneurysms ≥7 mm had a higher incidence of rupture and recurrence. In a study of 870 saccular aneurysms, 17 aneurysms ≤7 mm were more susceptible to late recanalization (more than 6 months). By contrast, early recanalization (within 6 months) correlated with size >7 mm, while aneurysms ranging from 4 to 7 mm were more prone to delayed recanalization. Murayama et al. 18 reported a 5.1% overall recanalization rate for small aneurysms (4–10 mm), which was much lower than the 35.3% rate for larger aneurysms. In the present study, we showed that aneurysm size correlated with recurrence after occlusion (P < 0.001), a similar result. Nevertheless, size was not an independent risk factor for recanalization. Furthermore, we found that saccular aneurysms had a recurrence rate of 40.0%, higher than rates reported in other studies. The reason for higher rate may be that, in irregular aneurysms, it was difficult to achieve complete embolization, and therefore it was difficult to generate thrombosis in the aneurysmal sac.
Stent-assisted coil embolization for intracranial aneurysms is another putative factor for aneurysm recanalization. Stents are increasingly used in this setting while aneurysms with wide necks require greater coil packing and flow diversion. Recurrence rates registered after simple coil embolization were significantly higher than those encountered after stent-assisted coil embolization.19–21 Piotin et al. 22 reported that the incidence of recanalization after embolization with stent-assisted coils (14.9%) were notably lower than those after simple coil embolizations (33.5%). A similar study 23 of 114 small PcomA (3–10 mm) reported that the rate of recanalization in the stent group (4.4%) was significantly lower than that of the non-stent assisted group (30.2%). These results suggested that the use of stents may alter the hemodynamics in the aneurysm, improving the packing density and promoting the proliferation of intravascular membrane.24,25 The present study demonstrated that non-stent-assisted coil embolization was an independent risk factor for recanalization (P < 0.01), consistent with results of previous studies.
Packing density is another important factor for recurrence post-embolization. Raymond et al. 26 reported that incomplete occlusion during treatment of aneurysms with coils was a risk factor for aneurysm recanalization. Linzey et al. 27 studied 122 stent-assisted coil aneurysms and concluded that aneurysms with <20% packing density were more likely to have clinically significant recurrences than those with >20% packing density, and the required reoperation rates were 19% and 5.1%, respectively. Lawson et al. 28 reported that packing density was a predictor of complete occlusion in aneurysms treated with stent-assisted coil embolization. A study of 49 circumferential unruptured aneurysms 4 also found that packing density was the main predictor of complete occlusion and aneurysm recurrence. In the present study, packing density not only was a risk factor for recurrence; Raymond grades II and III were also independent risk factors for recurrence (all P < 0.01).
Smoking is a debate factor for the recurrence of aneurysms post coil embolization. Shimizu et al. 29 analyzed more than 400 paraclinoid aneurysms and concluded that smoking status was not an parameter of the recurrence of aneurysms post embolization. Similar in present study, the relationship between smoking status and aneurysm recurrence is not obvious. However, there are other researchers oppose views on the relationship between smoking history and aneurysm recurrence. Ortiz et al. 30 retrospectively more than 100 smokers and demonstrated that the rate of recurrence and recanalization of cerebral aneurysms treated with coil-embolization higher than those nonsmokers. Futchko et al. 31 stratified their patient cohort into 3 groups with respect to smoking status—current smokers, former smokers, and nonsmokers. Their study found that a history of smoking (either current or former) was significantly and independently related to an increased risk of aneurysm recurrence after endovascular treatment. Similar research 32 about three groups smoking status showed that former smokers, like current smokers, have odds of aneurysm recurrence similar to nonsmokers. The accounts for different studies finding may be the difference in the adjunctive devices used. Different therapy ways like balloon-assisted coiling or stent-assisted coiling may reach discrepancy in outcomes. In addition, short follow-up time and not enough patients may draw different outcomes. In a word, the role of smoking plays in the recurrence of aneurysms post embolization need larger populations, longer follow-up time and similar therapy way to demonstrate.
There are several limitations in our study. First, the study was designed as a retrospective review based on a single-center experience with a small sample size. Further studies with larger populations and more centers are needed to confirm our results. Second, the angiographic follow-up time was short (11.4 months). Longer angiographic follow-up times may alter the rate of progression of occlusion. Finally, we found that rupture was not a risk factor for recurrence. Nevertheless, Zuo et al. 33 and Raper et al. 34 demonstrated that ruptured aneurysms were strongly predictive of aneurysm recurrence. The discrepancy may be the result of the small sample size in our study. Further research with larger numbers of patients will are necessary to address this issue.
Conclusions
Non-stent-assisted coil embolization, packing density and Raymond grades II and III are risk factors for recurrence after endovascular treatment of PcomA. This suggests that neurosurgeons may need to adjust treatment of aneurysms, depending on the Raymond grade. More detailed investigations regarding lowering the rate of recanalization of PcomA are needed.
Footnotes
Authors’ contribution
DG contributed the conception, design, data analysis. XG collected the data and drafted the manuscript. BS and ZB did the conception, design, and final approval of the version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the Scientific Research Project of Anhui Provincial Health Commission (no. AHWJ2021b114) and the Key Programs of Wannan Medical College (no. WK2020ZF07).