
Abstract
Background
Microsurgical clipping and endovascular coiling are viable treatment options for posterior communicating artery (PComA) aneurysms, but there are still major limitations to evidence-based decisions regarding standard-of-care treatment. In this study, we aimed at assessing potential selection biases that may influence our ability to extract conclusions about the comparative effectiveness or efficacy of the aneurysm treatment.
Objective
To study the patient/aneurysm characteristics as possible biases in the option for endovascular or neurosurgical treatment of PComA aneurysms.
Methods
A single-center, retrospective cohort study was performed, including all patients with treated PComA aneurysms with neurosurgical clipping or endovascular coiling between January 2010 and January 2021. Clinical and morphological data were collected from electronic records, and statistical analysis was performed.
Results
A total of 64 patients was eligible for inclusion; 24 (37.5%) patients were proposed for neurosurgical treatment, while 40 (62.5%) for endovascular treatment; 10 patients (25%) crossed over to the clipping group whereas none crossed over to the coiling side. Actual treatment analysis showed significantly higher diameters of mother vessel (t-test, p = 0.034) and aneurysm neck (Mann–Whitney, p = 0.029) in the clipping group and higher aspect and dome-to-neck ratios in the endovascular group (Mann–Whitney, p = 0.008). A significantly higher vasospasm frequency was found in the clipping group but only in the intention-to-treat analysis (Chi-square, p = 0.032).
Conclusion
Significant morphological differences between effective endovascular and surgical groups and differences in intention-to-treat analysis may limit the validity of a direct comparison between treatment options and suggest the presence of a possible selection bias.
Introduction
Cerebral aneurysms (CAs) are dilations that occur at vulnerable points along with the arterial circulation of the brain. Although there is an important variability among different populations, its estimated worldwide prevalence varies from 1% to 3%.1,2 CA are frequently diagnosed in asymptomatic patients, but their rupture remains a serious clinical event with high rates of morbidity and mortality. 3 Most CA are acquired lesions, and there are known risk factors for their formation, growth and rupture, namely advanced age, female gender, cigarette smoking, hypertension, dislipidemia and family history.1,4–6
The posterior communicating artery (PComA) constitutes one of the most common sites of CA formation, with an estimated relative frequency of up to 15% to 25% of all aneurysms.7,8
The advent and technological development of neurovascular surgery in the past years has made PComA aneurysms more and more suitable for endovascular treatment. Despite this, the need for a multidisciplinary decision by both experienced neurosurgeons and neuroendovascular experts remains critical, as age, comorbidities and morphological parameters are possible variables implied in the decision-making process. 9
Since the International Subarachnoid Aneurysm Trial in 2002, the comparison of endovascular treatments and microsurgical clipping has become paramount. 10 The emphasis has been put on the invasiveness of the treatment and on the importance of short- and long-term effectiveness, but several limitations have been pointed out regarding the design of the study and possible selection biases in the allocation to the intervention groups.
PComA aneurysms, in particular, have significant anatomical variability and coiled aneurysms appear to have a particularly high risk of recurrence.8,11 Multiple studies have tried to identify subgroups of patients suitable for endovascular or surgical treatment. Despite variable evidence, surgically clipped PComA aneurysms with an elongated fundus, true PComA aneurysms and aneurysms associated with a fetal PComA artery may have better occlusion rates and post-treatment patency of the PComA artery. 8 On the other hand, small aneurysm size, smaller dome-to-neck ratio and poor clinical grade at admission might benefit from endovascular coiling, especially in elderly patients.8,9
Major limitations to evidence-based decisions regarding the standard of treatment arise from the impossibility of randomizing patients and an inability to assess equipoise. We hypothesized that, in a real-world setting with multimodal treatment options available, there are differences among the two intervention groups resulting from selection biases that could potentially hamper the ability to extract conclusions about the effectiveness or efficacy of the actual treatment.
Methods
A single-center (tertiary University Hospital), retrospective cohort study was performed. All patients with diagnosis of ruptured or unruptured PComA aneurysm and proposed to neurosurgical (neurosurgical clipping) or endovascular treatment (single coiling) between January 2010 and January 2021 were included. Data regarding clinical and imaging variables were collected in January of 2021 in an anonymized fashion from electronic records. The study’s full protocol was reviewed and approved by the Ethics Committee and Institutional Board Review.
Demographic and clinical variables include gender, age at the time of intervention, smoking history (past or present history of tobacco abuse was considered), hypertension, dyslipidemia and diabetes mellitus diagnosed before the time of intervention. Familial predisposition to CAs was considered positive if there were reports of a first-degree family member being diagnosed and/or treated for multiple intracranial aneurysms.
Clinical presentation was described by the aneurysm status (ruptured or unruptured) and, in the case of rupture, clinical grading scales such as Hunt and Hess Scale and World Federation of Neurological Surgeons (WFNS) Scale. The extent of the subarachnoid hemorrhage (SAH) was classified according to the Modified Fisher Scale with non-contrast computed tomography (CT)-scans assessment.
Both analyses of intention-to-treat (first proposed treatment for the patient after multidisciplinary discussion) and effective treatment (actual treatment performed) were conducted.
Aneurysm size and morphology were recorded from pre-treatment digital subtraction angiography (DSA) or CT angiography (CTA) with multiplanar reconstructions. Size measurements, in millimeters, were made using the best projections profiling the aneurysm’s neck and dome, as well as the parent artery diameter on three-dimensional reconstructions. Aneurysm neck, height, maximum diameter, mother vessel diameter, and therefore size ratio, aspect ratio and dome-to-neck ratio were assessed and calculated.
Orientation of the aneurysm was determined according to three-plane orientation as described by Matsukawa et al. 12 Direction regarding the midline was defined as lateral, medial or neutral according to a line through the bifurcation of the internal carotid artery (ICA) and PComA parallel to the midline (“parallel line”) on the superior view of 3D CTA/DSA image. Projection was further characterized with a perpendicular line through the bifurcation of the ICA and PComA perpendicular to the parallel line (“perpendicular line”) for anterior, posterior or neutral assessment. Finally, a line through the bifurcation of the ICA and PComA parallel to the anterior skull base (“horizontal line”) on sagittal images was drawn for superior, inferior or neutral projection. Such design results, in theory, in 27 different projections when decomposing for each different plane. Orientation is illustrated in Figures 1 and 2. Measurements and orientation were all determined by two different observers.
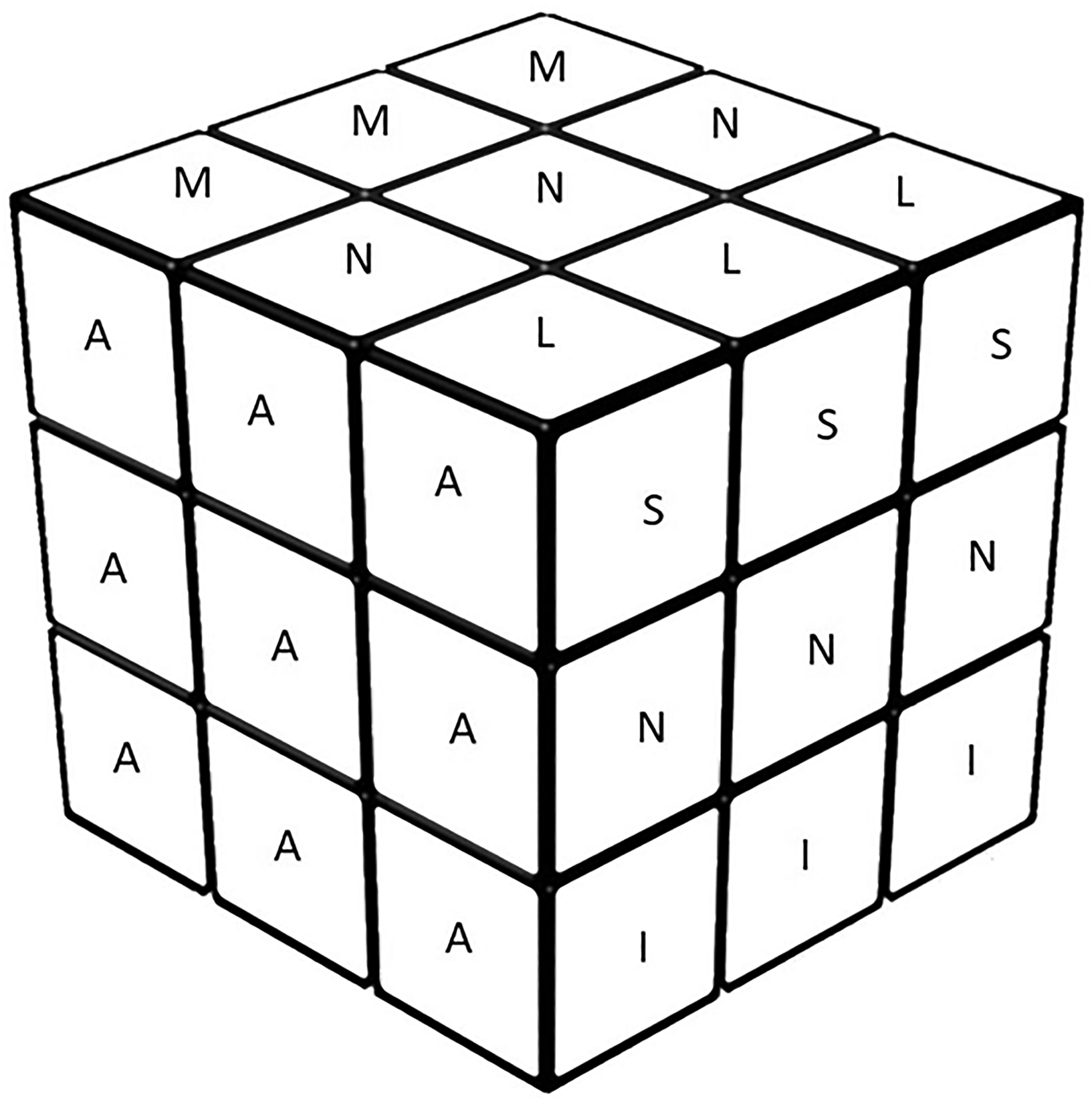
Example of the Rubik cube for an explanation for theoretical possible projections of posterior communicating artery (PComA) aneurysm dome when assessing for the three different planes. L – lateral; M – medial; A – anterior; S – superior; I – Inferior; and N – neutral.
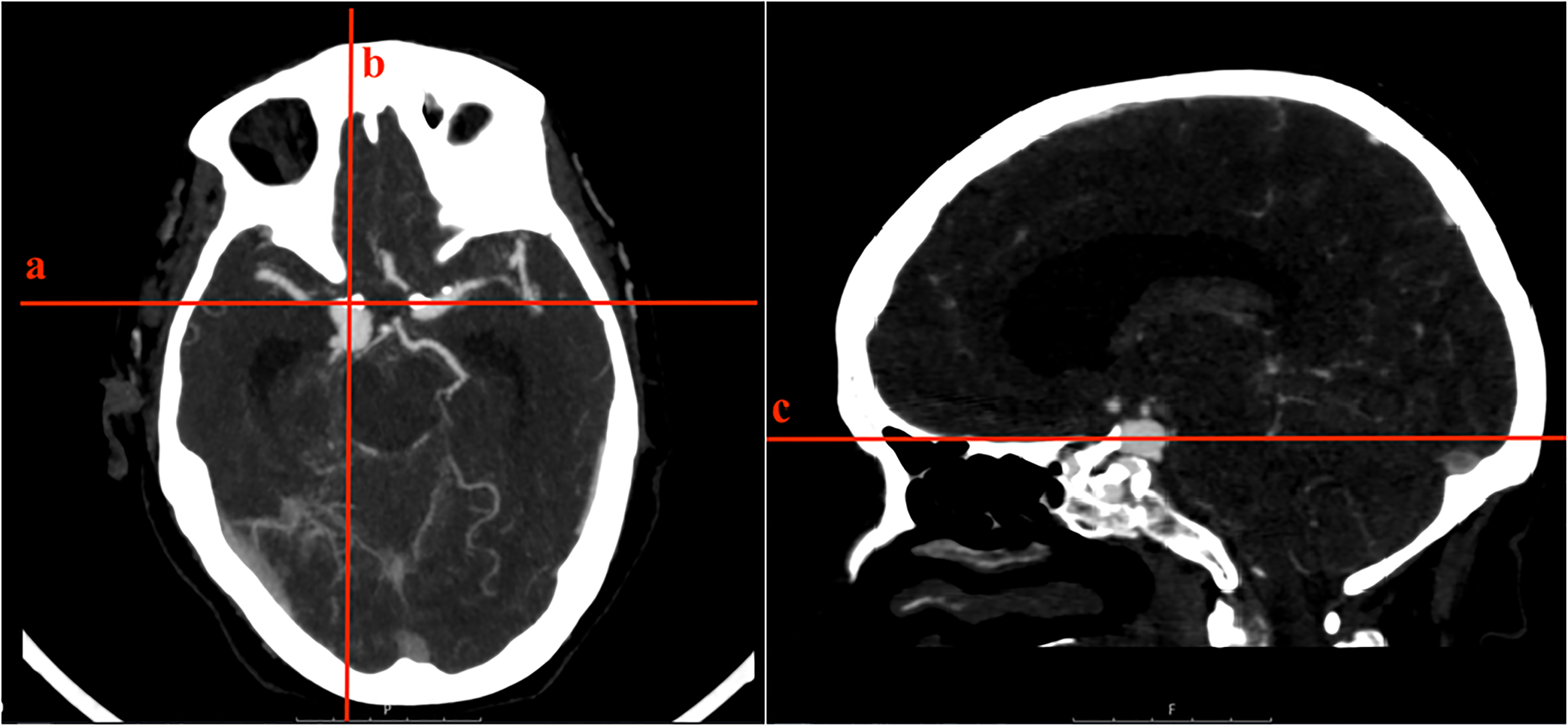
Orientation of the aneurysm according to three-plane orientation on a computed tomographic angiography (CTA) image. Orientation of the aneurysm regarding the midline was defined as neutral according to a line through the bifurcation of the internal carotid artery (ICA) and posterior communicating artery (PComA) parallel to the midline (line a); characterized as posterior according to a perpendicular line through the bifurcation of the ICA and PComA perpendicular to the parallel line (line b); orientation considered neutral according to a line through the bifurcation of the ICA and PComA parallel to the anterior skull base (line c) on the sagittal view.
Complications of the intervention were assessed as de novo ischemic lesion, vasospasm and hydrocephalus. An ischemic lesion resulting directly from the intervention was defined as a de novo ischemic lesion (that wasn't present at the time of SAH diagnosis) reported in two consecutive post-interventional CT scans. Vasospasm was positive if there were records of Doppler-ultrasound diagnosed vasospasm during hospital admission. Hydrocephalus was defined as the accumulation of cerebrospinal fluid and increased intracranial pressure that merited neurosurgical intervention.
Statistical analysis was performed using IBM SPSS Statistics® 25. Kolmogorov–Smirnov test for continuous variables was performed for normality assessment. Chi-square or Fisher’s exact test was used for categorical variables association. Independent sample t-test or Mann–Whitney test was performed for continuous variables according to the group (depending on the presence of normality). Whenever clinically relevant, a variable's stratification was performed, namely on clinical presentation grading scales. We considered a level of statistical significance of 0.05.
Results
Sixty-four patients (47 women and 17 men) were treated for PComA aneurysms in our center between January 2010 and January 2021 and included in this study. The mean age was 58.5 ± 13.6 years (range 34–93).
Regarding the aneurysm status, 47 (73.4%) aneurysms were ruptured and 17 (26.6%) were unruptured aneurysms selected for elective treatment; 24 (37.5%) patients were primarily proposed for neurosurgical treatment and 40 (62.5%) for endovascular treatment; 54 patients received the same treatment they were firstly proposed for, but 10 patients crossed over from the endovascular to the neurosurgical intervention, whereas none crossed over from the neurosurgical to the endovascular treatment. Patient characteristics, aneurysm morphology and aneurysm dome orientation are shown in Tables 1, 2 and 3, respectively.
Clinical characteristics, clinical presentation and complications.
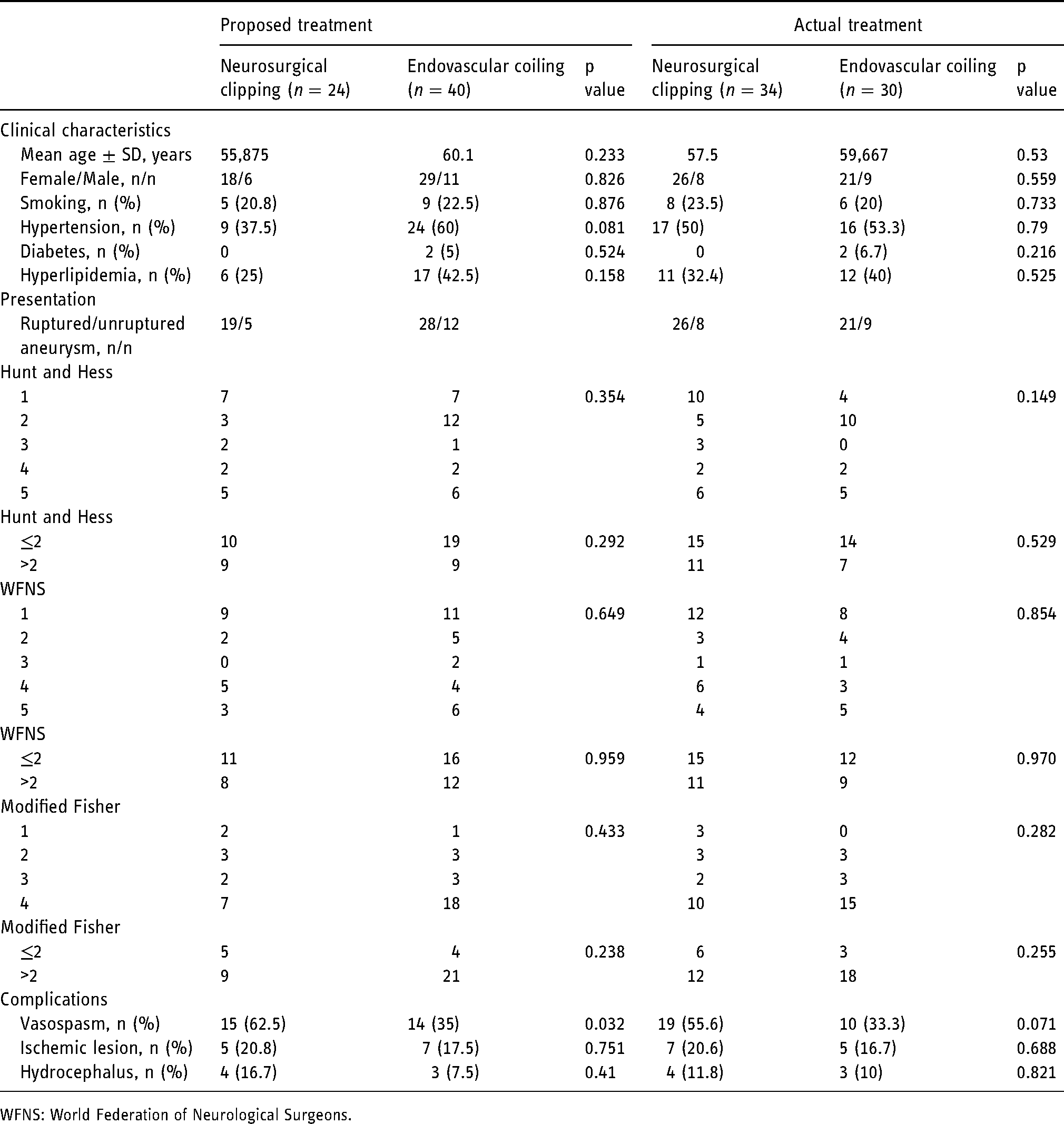
WFNS: World Federation of Neurological Surgeons.
Aneurysm-related morphologic measurements.
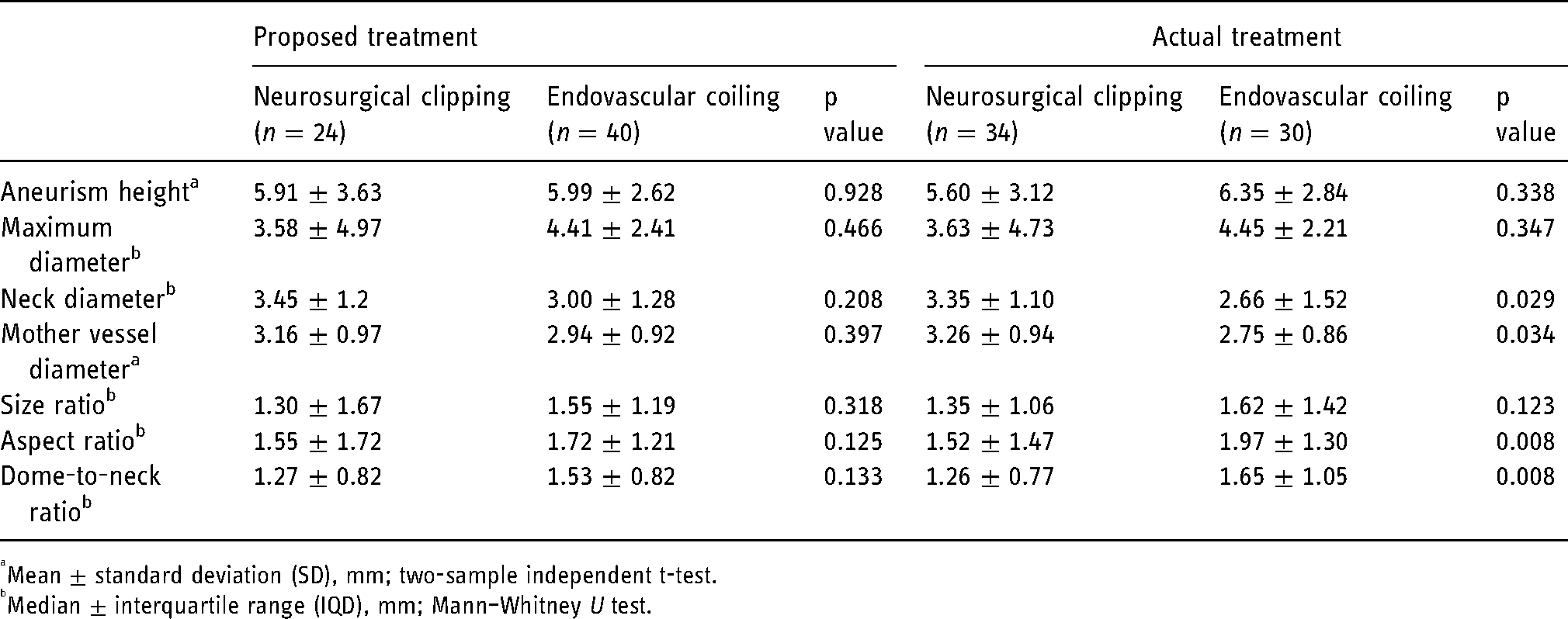
Mean ± standard deviation (SD), mm; two-sample independent t-test.
Median ± interquartile range (IQD), mm; Mann–Whitney U test.
Aneurysm dome orientation.
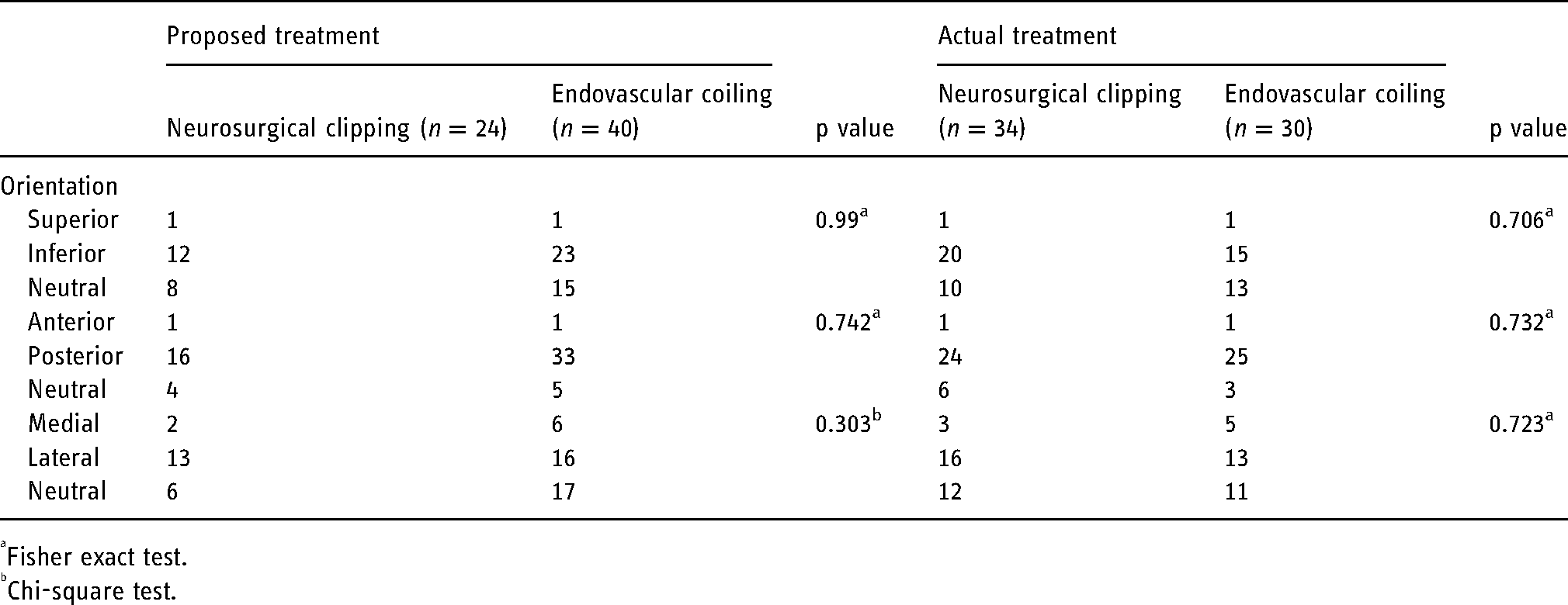
Fisher exact test.
Chi-square test.
Effective treatment analysis
Assessing the data on an actual treatment basis, there are no significant differences between treatment groups regarding age at the time of the intervention, sex nor clinical characteristics (smoking, hypertension, diabetes and hyperlipidemia). Clinical presentation grading scales (Hunt and Hess, WFNS and Modified Fisher scales) also showed no differences between groups. Hospital mortality was 7.8% and resulted from the death of five patients: three patients died in the neurosurgical treatment group and two patients died in the endovascular intervention, all of which were in the context of a ruptured aneurysm and after the intervention. There were no differences between the intervention groups in terms of the rate of complications.
Regarding morphological parameters, diameters of the mother vessel and the aneurysm neck were both significantly higher in the neurosurgical group (p = 0.034 and p = 0.029, respectively). Patients submitted to endovascular treatment showed a higher aspect ratio and dome-to-neck ratio (p = 0.008 in both).
Aneurysm orientation regarding the three axes and as shown in Figure 1 did not show any difference among groups, even when stratifying for each axis.
Intention-to-treat analysis
Regarding the proposed treatment, in an intent-to-treat analysis, there were also no significant differences between groups regarding age at the time of the intervention, sex, clinical characteristics (smoking, hypertension, diabetes and hyperlipidemia) nor presentation grading scales. However, when assessing complications, the presence of vasospasm during hospital admission was significantly higher in patients who were initially proposed for neurosurgical intervention (p =0.032). There was no difference among groups regarding ischemic lesions or late hydrocephalus. Morphological parameters did not show any significant difference comparing both intention-to-treat groups, including aneurysm orientation.
Discussion
This study highlights the presence of different characteristics among groups of patients submitted to neurosurgical or endovascular treatment of PComA aneurysms: despite similar clinical risk factors, age and rate of complications, there is a striking difference in the morphologic characteristics between endovascular and surgical groups, as well as a significant variability between intention-to-treat and effective treatment groups. This brings the question: why is any given patient proposed for one treatment and not the other?
Our results showed that almost two-thirds of the patients (62.5%) were first proposed for an endovascular approach, which is in line with the knowledge of a growing trend of surgical clipping being gradually replaced by endovascular coiling.13,14 The current guidelines for the management of aneurysmatic SAH by the American Heart Association (AHA) recommend that the endovascular approach should be the first-line option for aneurysms technically amenable for both modes of treatment. 9
The decision for which intervention to be proposed should be a multidisciplinary decision that takes into consideration the patient and aneurysm characteristics. In our institution, a treatment was proposed in all cases based on a revised endovascular treatment adequacy/safety profile after 3D angiography between the vascular neurosurgeon and intervention neuroradiologist. Despite AHA recommendations that, among others, endovascular coiling may receive increased consideration in the elderly patients and in those presenting with poor WFNS grade SAH, 9 we did not find any differences in any of these variables when comparing the two proposed treatment groups in our population.
We did not find any statistically significant differences regarding aneurysm orientation regarding treatment allocation, performed treatment or complications. Evidence is sparse and controversial regarding projection. Despite recent data suggest a higher risk for rupture in laterally projected aneurysms, 12 ruptured aneurysms with medial projection 15 and posterior projection 16 were also associated with poorer outcomes.
Despite the larger number of PComA aneurysms first proposed for an endovascular treatment, cross-over to the clipping side occurred in 25% of these patients; reasons ranged from difficult/bad intravascular accesses, inability for coil stabilization and wide-neck/bad aspect ratio for simple coiling. Consequently, more than half of all PComA aneurysms treated in this hospital ended up being treated with surgery, which is significant even considering the time frame of this study. There are clear-cut characteristics of aneurysm morphology in the effective treatment groups: effective treatment analysis showed that aneurysms with larger necks were more likely to be effectively treated with a neurosurgical approach, which correlates with the knowledge that a large aneurysm and a wider neck are thought to be associated with lower rates of complete aneurysm occlusion with coiling.11,17 This finding is reinforced by the fact that, in an intention-to-treat analysis, there are no differences between groups. This highlights the fact that, although there is no “cherry-picking” for each of the treatment groups, there is a significant different morphological basis to each group that should be recognized first-hand to avoid simple intervention outcome comparisons such as rate of occlusion, functional status or even mortality.
Moreover, it is also interesting to notice that, in patients with an intention-to-treat surgical clipping allocation, there was a higher prevalence of vasospasm, which did not occur in an effective treatment comparison. Such findings suggest that this does not relate to the technique itself but, in fact, to an intrinsic selection bias between these groups. This could be another important factor to keep in mind when analyzing and comparing the results and complications of these two modalities of treatment. This way, the fact that there aren't consistently recognized factors in the literature for allocation to treatment groups, both for PComA and other aneurysm locations, may result in an important bias where the patients selected for a neurosurgical approach are those deemed too difficult not only to the endovascular approach but to any approach. Despite these differences, it must be reinforced that we only addressed comparison with single-coiling treated aneurysms on the endovascular treatment side. Technique development over the years and the advent of new and safer devices such as flow-diverter devices are changing the trend for more complex aneurysms (fusiform, dissecting, bifurcating and with fetal circulation involvement) offering better solutions for a higher probability of occlusion and less morbidity. 18
Although this is the experience of a multidisciplinary team over the course of more than 10 years in a tertiary hospital, there are some limitations to our study. First and foremost, this is a single-center study with a small study population and, therefore, with limited external validity, seeing as the management of aneurysms in this specific hospital is related to the resources available and experience of its professionals, among other variables. Another limitation is that we had to rely only on retrospective data collection from electronic medical records, meaning some data was missing. The difficulty to come by quality data constituted a particularly important limitation in aneurysm-related measurements, since not all images or projections had a scale we could use to take as a reference and we sometimes had to use a projection of the aneurysm that wasn’t the best for these measures. Another limitation relies on the intrinsic lack of inter-rater reliability on the grading scales used to quantify SAH presentation.19,20
Despite this study’s limitations, we were able to summarize some of the characteristics of patients and PComA aneurysms selected for each treatment mode in this hospital. So far, however, there aren’t any detailed reports studying PComA aneurysm morphology and treatment results in literature, 11 and there is very little data that stratifies morbidity and mortality based on aneurysm location. 8
Conclusion
Significant morphological differences between effective endovascular and surgical groups, as well as differences in intention-to-treat analysis, may limit the validity of a direct comparison between treatments and suggesting the presence of possible selection bias. It is therefore of the utmost importance to invest in larger studies on this matter and to have more short- and long-term prospective analyses of these patients’ outcomes to help assessing the proper patient population and aneurysmal characteristics best suited for each treatment.
Footnotes
IRB approval/Research Ethics Committee
Full-protocol approval.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.