
Abstract
Progressive stenosis and occlusion of the bilateral internal carotid artery terminals and circle of Willis are typical features of Moyamoya disease. However, aplastic or twig-like middle cerebral artery (Ap/T-MCA)—wherein the unilateral main trunk of the middle cerebral artery (MCA) is not depicted, and a plexiform arterial network is formed—is similar to the findings of Moyamoya disease. Here, we describe a 78-year-old man who presented with mild right paralysis and aphasia. Magnetic resonance angiography (MRA) at admission did not show the bilateral MCAs. The findings were similar to those of Moyamoya disease, and his symptoms worsened after hospitalization. Endovascular treatment was performed, and the left MCA was completely recanalized. Later, paroxysmal atrial fibrillation was detected, and we finally determined that left MCA occlusion had occurred due to embolism. The right MCA was completely occluded at its origin, indicating an Ap/T-MCA. Embolic occlusion of the unilateral MCA and contralateral Ap/T-MCA made this case resemble Moyamoya disease in the acute stage. Even when chronic occlusion is suspected on MRA in acute cerebral infarction, endovascular treatment should be considered. Additionally, a heterotypic R4810K polymorphism was later found in the RNF213 gene. To our knowledge, this is the second report of Ap/T-MCA with the RNF213 gene polymorphism; however, their association remains unclear and requires further analyses.
Introduction
Moyamoya disease is characterized by chronic steno-occlusive lesions involving the bilateral internal carotid artery (ICA) terminals and arterial circle of Willis with characteristic collateral vessel named as the “Moyamoya” vessels. 1 Aggressive treatments consisting of intravenous infusion of recombinant tissue plasminogen activator (rtPA) and neurointervention for ischemic strokes in patients with Moyamoya disease are not recommended because of the high risk of haemorrhagic complications and unsuccessful results.2–4 Recently, cases harbouring angiographic features, consisting of a steno-occlusive lesion on the unilateral middle cerebral artery (MCA) and plexiform arterial network instead of the main MCA trunk, have been reported and are designated as aplastic or twig-like MCA (Ap/T-MCA).5–7 The precise pathogenesis has yet to be elucidated; however, the R4810K polymorphism of the RNF213 gene—the strongest genetic susceptibility factor for Moyamoya disease in the East Asian population—was recently reported in one case of Ap/T-MCA, 8 suggesting a potential association between the RNF213 polymorphism and Ap/T-MCA.
Herein, we report a case of unilateral Ap/T-MCA with RNF213 polymorphism, exhibiting contralateral cardiogenic embolism and acute magnetic resonance imaging (MRA) findings mimicking Moyamoya disease, treated by mechanical thrombectomy.
Case report
The patient was a 78-year-old man with diabetes mellitus, who was treated with sitagliptin (50 mg). He had never smoked and had no family history of cerebrovascular disease. He presented with right mild hemiparalysis and mild aphasia at an unknown time of onset. On admission, his National Institutes of Health Stroke Scale (NIHSS) score was 6. His blood pressure was 159/76 mmHg, pulse rate was 59 beats per minute, and he had a sinus rhythm on 12-lead electrocardiogram. Computed tomography (CT) demonstrated a faint, low-density area in the left lenticular nucleus, and an Alberta Stroke Programme Early CT Score of 9. Magnetic resonance imaging (MRI) showed a high diffusion-weighted image signal in the left caudate nucleus and putamen, and a mildly high signal on fluid-attenuated inversion recovery (FLAIR) (Figure 1A, B). Intra-arterial signals were only observed on the left side of the FLAIR images (Figure 1B, C), while on MRA, the bilateral MCAs could not be visualized from the origin, suggesting Moyamoya disease at the first impression (Figure 1D).
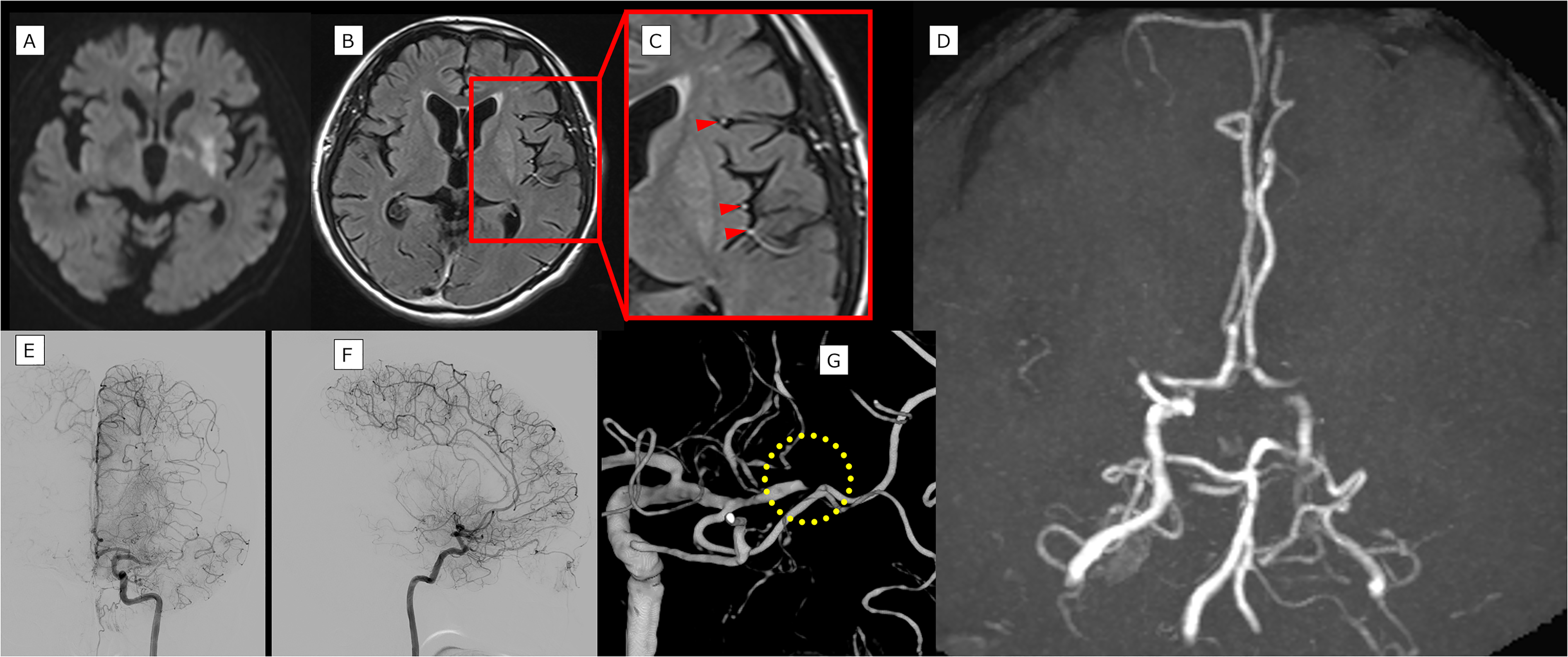
Detailed diagnostics (A) Diffusion-weighted image shows a high signal in the left putamen. (B, C) Fluid-attenuated inversion recovery at admission shows an intra-arterial signal on the left side. (D) Magnetic resonance angiography does not show bilateral middle cerebral arteries (MCAs), and the findings resemble those of moyamoya disease. (E, F) Cerebral angiography shows left M1 occlusion.(G) Three-dimensional (3D) digital subtraction angiography shows crab claw-like findings (dot circle).
Initially, we considered the occurrence of cerebral infarction due to a chronic obstruction, such as Moyamoya disease, concluding that rtPA or endovascular treatment was not indicated. We initiated treatment with oral aspirin (200 mg), clopidogrel (300 mg), intravenous argatroban, edaravone, and low-molecular-weight dextran; however, 6 h after admission, his right hemi paralysis and aphasia worsened, and his NIHSS score was 10. Therefore, urgent cerebral angiography was performed. Cerebral angiography indicated that the blood flow was occluded at the middle of M1 (Figure 1E, F), demonstrating a crab claw-like appearance suggestive of embolism (Figure 1G). The patient was considered to have an embolism and underwent subsequent mechanical thrombectomy.
A balloon-guiding catheter, 8Fr Optimo (Tokai Medical Products, Kasugai, Aichi, Japan), was advanced to the ICA. We attempted to retrieve the thrombus by combining the techniques of the Solitaire 4 × 40 mm stent retriever (Medtronic, Irvine, CA, USA) and ACE68 reperfusion device (Penumbra, Inc., Alameda, CA, USA) (Figure 2A). Although a small part of the thrombus was removed, the thrombolysis in cerebral infarction (TICI) score remained 0 (Figure 2B, C). Arteriosclerotic obstruction was also suspected, and percutaneous transluminal angioplasty was performed with a balloon catheter (Unryu; 2 × 10 mm; Kaneka Medix, Osaka, Japan); still, the occlusion remained. (Figure 2D, E). When a combined technique using the ACE68 and Trevo 4 × 30 mm stent retriever (Stryker, Kalamazoo, MI, USA) was attempted, a slight improvement in blood flow was observed up to the distal part of M1; however, M2 remained occluded (Figure 2F, G, H). A Marksman microcatheter (Medtronic, Irvine, CA, USA) was advanced into M2 and local intra-arterial injection of urokinase (360,000 units) was administered. Partial recanalization was obtained, and the final TICI score was 2a (Figure 2I, J). Subsequent CT showed mild intra-infarct and minimal subarachnoid haemorrhage, which gradually improved. After continuous rehabilitation, the modified Rankin Scale score at 3 months was 2.
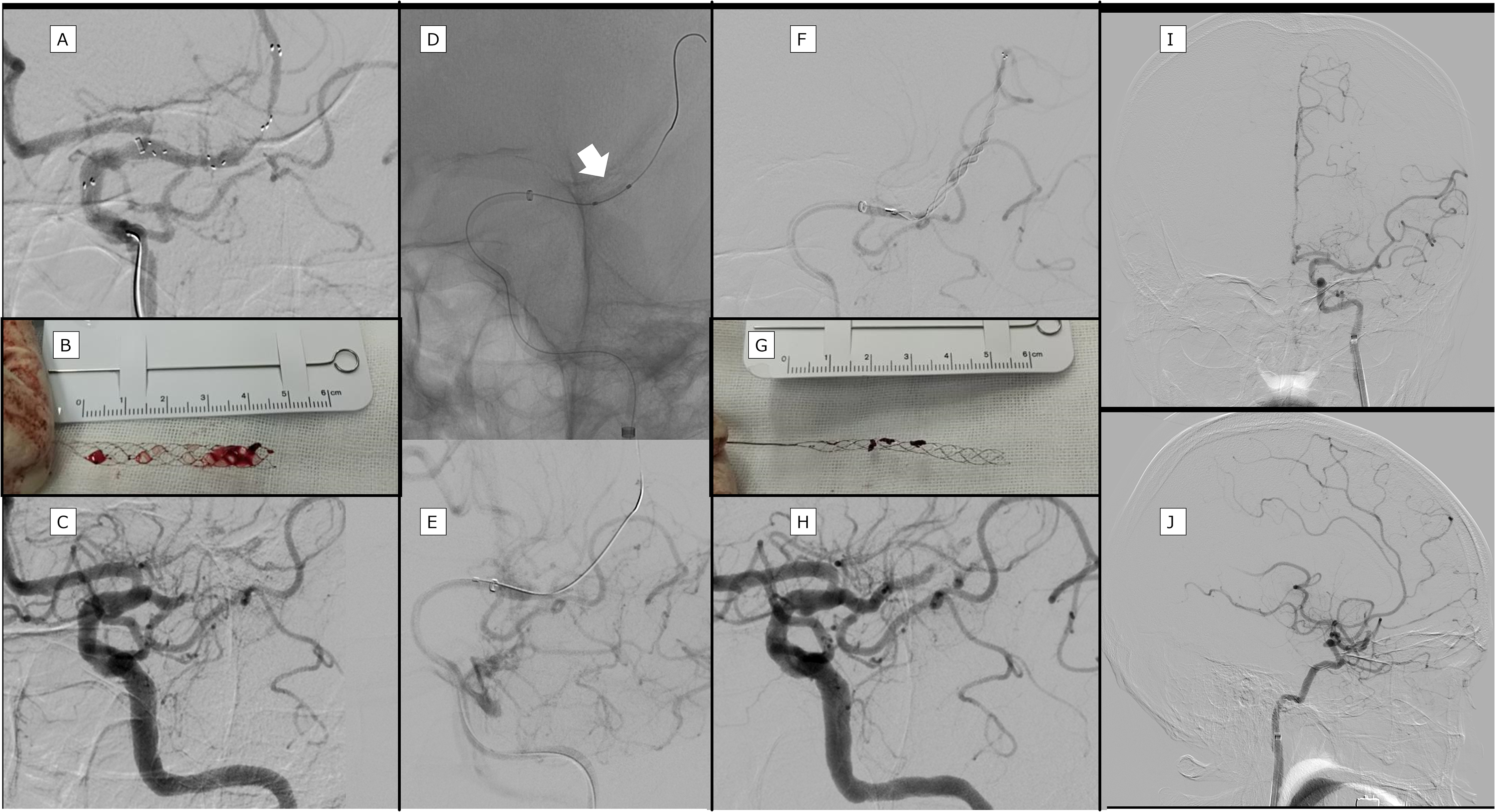
Mechanical thrombectomy
Paroxysmal atrial fibrillation was detected later, and cerebral angiography performed after a month revealed that the left M1 was completely recanalized without stenosis (Figure 3A); we finally diagnosed a cardiogenic embolism in the left MCA, rather than Moyamoya disease. In the right MCA, cerebral angiography showed occlusion at the origin of M1, with an abnormal arterial network around it (Figure 3B, C, D). The circulation characteristics for Moyamoya disease, including stenosis of the terminal part of ICA and findings from the external carotid artery (ECA) were lacking. T2-weighted three-dimensional (3D) fast-spin echo (FSE) MRI showed apparent right M1 hypoplasia when compared with the left side (Figure 3E, F - arrowhead; reference lines are indicated in a coronal section; Figure 3G). Based on the above, an Ap/T-MCA was diagnosed on the right side, and we concluded that the acute phase MRA resembled Moyamoya disease due to the combination of the Ap/T-MCA and cardiogenic embolism on the contralateral side (Figure 3H). Later, the R4810K polymorphism in the RNF213 gene was tested, and a heterotypic polymorphism was found.
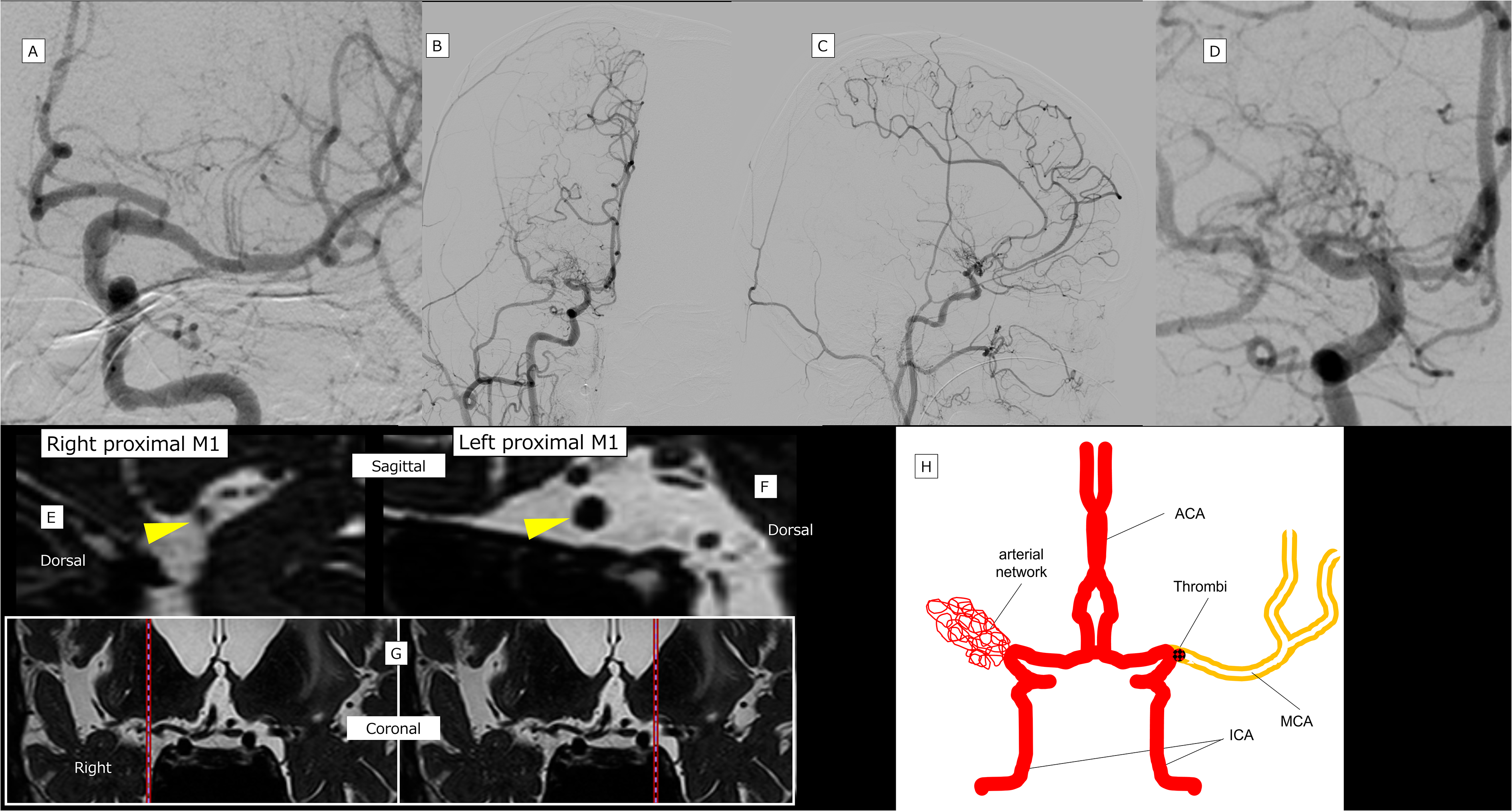
Follow up study and schema cerebral angiography performed after 1 month demonstrates that the left MCA had completely reopened without any stenosis (A). The right MCA was completely occluded at its origin; reticular vessels are observed around it (common carotid angiography, B: Frontal; C: Lateral; D: Enlarged frontal).
Discussion
In the present case, the MCA on the right side was chronically occluded, while acute MCA embolization on the left side resembled Moyamoya disease on the MRA at admission. We hesitated to perform catheterization in the acute phase, since the MRA findings were suggestive of Moyamoya disease; however, after the patient's symptoms worsened, we performed cerebral angiography, which revealed an embolus that was subsequently treated via neurointervention.
Due to the high risk of bleeding in patients with Moyamoya disease, rtPA was once contraindicated in Japan, 2 and is now administered with caution. 3 Moyamoya disease is also associated with the perforation of abnormal vessels in conjunction with neurointervention, and percutaneous revascularization is often unsuccessful. 4 Because of the extremely high risks, endovascular treatment for Moyamoya disease is generally not recommended. However, we should not necessarily hesitate to perform cerebral angiography, since it is possible that what appears to be a Moyamoya disease can be an embolism of the ipsilateral MCA and pre-existing chronic steno-occlusive MCA of the contralateral side, as was observed in the present case. In our case, a high intra-arterial signal was observed on FLAIR on the left side alone. This signal reflects the slowing of blood flow velocity, as well as large vessel occlusion or stenosis. 9 Therefore, it has been suggested that patients with intra-arterial signals may be suitable for rtPA and endovascular therapy candidates. 9 In addition, the presence of cortical symptoms, such as mild aphasia, indicates that more aggressive examination and treatment should have been performed at admission. Although there is little value in diagnosing Ap/T-MCA in the acute phase, the presence of this disease should be considered, as it is possible to miss the timing of revascularization.
In 1982, Fukawa et al. first described cases of MCA occlusion with a Moyamoya-like vascular network, where clinical features were not identical to those of Moyamoya disease. 5 For similar diseases, Liu et al. 6 (in 2005) and Seo et al. 7 (in 2012) used the names twig-like MCA and Ap/T-MCA, respectively. To date, common angiographical features of Ap/T-MCA are described as follows: 1) a steno-occlusive lesion can be seen on the unilateral MCA, 2) plexiform arterial network exists instead of the main MCA trunk, 3) perforators arise from the plexiform arterial network, and 4) cortical branches beyond the occluded MCA trunk have an anterograde flow with a normal configuration.10–12 It is considered that MCA hypoplasia occurs because of the twig-like network remnants that exist at the time of MCA development. Reported characteristics of an Ap/T-MCA are stenosis or occlusive lesions confined to the unilateral M1. However, there are cases of the so-called unilateral Moyamoya disease (quasi-Moyamoya disease), wherein the lesion is confined to one side, and the other side is almost normal. The unilateral involvement can also occur in the early stage of Moyamoya disease, although the involvement of bilateral ICAs is the hallmark of this disease. It is difficult to differentiate the two diseases; however, the following characteristics should be helpful: Ap/T-MCA is further characterized by normal vasculature beyond M2 and in other arteries, no collateral blood flow from the ECA, and no progression of the lesion.10–12 Ap/T-MCA is a very rare condition, accounting for 0.11–1.17% of serial cerebral angiography cases, and is associated with bleeding events in more than half of these cases, with aneurysms often occurring in abnormal vessels.6–8,13,14
The present case had the angiographical features of an Ap/T-MCA. T2-weighted 3D-FSE evaluation of the vessel's outer diameter suggested the presence of a thin outer diameter and traces of cord-like structures in the right M1. A previous report similarly showed a cord-like structure in M1 on the MRI in a case of Ap/T-MCA, 14 suggesting dysplasia in the background of the Ap/T-MCA.
The R4810K polymorphism of the RNF213 gene, located at the 17q25.3, has been reported to be the strongest genetic susceptibility factor for Moyamoya disease in the East Asian population. Matsuda et al. have shown that RNF213 polymorphisms are not only associated with Moyamoya disease, but also with intracranial arterial steno-occlusive vasculopathy. 15 They advocate that the wide variety of vascular phenotypes in association with RNF213 mutations can be understood as a spectrum of RNF213-related intracranial vascular disease. 15 Interestingly, RNF213 polymorphisms are noted in patients with Ap/T-MCA. The Ap/T-MCA and RNF213 polymorphism association was first reported by Fukuyama et al. 8 in 2020; to the best of our knowledge, our case is the second report of Ap/T-MCA with the RNF213 gene polymorphism. In patients with RNF213 polymorphisms, intracranial arterial stenosis may also progress to other sites. The association between RNF213 polymorphisms and Ap/T MCA is unclear.
The pathogenesis of Ap/T-MCAs is still not fully understood. While it is often thought that the proximal M1 defect does not form at all during development, the accuracy has not been warranted. 11 Embryologically, the ICA and MCA should form first, otherwise the affected cerebral hemisphere will not develop normally. 11 In fact, deformed and discoloured M1 trunks have been observed in intraoperative findings, 8 and similar to the present case, a cord-like M1 trunk has been identified on MRI in a previous report. 14 This suggests that the changes are not completely aplastic in the foetal period, but secondary to stenosis and occlusion of the proximal MCA. 11 The pathogenesis of Ap/T-MCAs has been considered to be different from that of Moyamoya disease, however; further genetic analysis may reveal a common aetiology between Ap/T-MCA as RNF213 gene polymorphism-related spectrum diseases.
Conclusion
We encountered a case of acute embolic occlusion on the left side with chronic M1 occlusion due to an Ap/T-MCA on the right side, where the MRA findings resembled those of Moyamoya disease on the first impression. In the absence of previous information and when chronic occlusion is suspected on MRA in cases of acute cerebral infarction, examination and treatment should be aggressively performed. Understanding the association between the RNF213 gene polymorphism and Ap/T-MCA will further require analyses of similar cases.
Footnotes
Acknowledgements
We thank Dr Ihara and Dr Yoshimoto of the National Cerebral and Cardiovascular Center for the RNF213 analysis.
Author contribution
H.I. analysed the data and drafted the manuscript. M.O. and Y.N. reviewed the draft critically. M.M. and N.M. presented the direction to the conclusion, and reviewed the manuscript.
Data availability
The data included in this study are available from the corresponding author M.O. upon reasonable request
Patient consent
Informed consent was obtained from the patient's wife for publication of this case report and accompanying images.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.