
Abstract
Objectives
This study evaluated the clinical impact of the Sim&Size® simulation software on the endovascular treatment with flow-diverter stents of patients with unruptured saccular intracranial aneurysms.
Methods
This monocentric retrospective study evaluated a cohort of patients treated with flow-divert stents between June 1, 2014, and December 31, 2019, for cerebral aneurysms. Patients belonged to two groups, patients treated with and without the Sim&Size® simulation software. Univariate, bivariate, and multivariate analyses were used to evaluate the clinical impact of simulation software.
Results
Out of the 73 interventions involving 68 patients analyzed by the study, 76.7% were simulated using the Sim&Size® simulation software, and 23.3% were not. Patients treated with the simulation software had shorter stent lengths (16.00 mm vs. 20.00 mm p-value = 0.001) and surgical time (100.00 min vs. 118.00 min p-value = 0.496). Also, fewer of them required more than one stent (3.6% vs. 17.6% p-value = 0.079). Three patients belonging to the non-stimulated group presented hemorrhagic complications.
Conclusions
Using the Sim&Size® simulation software for the endovascular treatment of intracranial aneurysms with pipeline flow-diverter stents reduces the stent length.
Keywords
Introduction
The prevalence of unruptured cerebral aneurysms varies between 0.5% and 7.0%, depending on the population. Treatments to prevent ruptured cerebral aneurysms include open surgery on selected cases or endovascular therapy. 1 Among these treatments, parent artery reconstruction with flow-diverter stents appears effective and safe.2,3
Cerebral arteries are tortuous and irregular vessels with different diameters in each segment, making the selection of an appropriate stent challenging. Physicians can select the stent size manually, using digital subtraction angiography. Alternatively, they can use virtual simulation programmes developed for this purpose. Among these programmes, the Sim&Size® software (Sim&Cure, Grabels, France) 4 bases on characteristics of the patient vessel and the device to simulate the behaviour of the pipeline stent (Medtronic).
Several centres have successfully used the Sim&Size® simulation software during the endovascular treatment with flow-diverter stents of patients with intracranial aneurysms. This software provides confidence to physicians while choosing the stent size as it simulates each patient's anatomy. 5 Using a simulation programme is expected to result in a more accurate stent size and fewer complications. This monocentric retrospective study evaluated the clinical impact of the Sim&Size® simulation software on the endovascular treatment with flow-diverter stents of patients with unruptured saccular intracranial aneurysms. Precisely, it determined the effect of the software on stent dimensions, surgical time, number of stents used, and whether using the simulation software associated with fewer complications.
Methodology
The study is a monocentric retrospective analytical evaluation of a cohort of patients treated with flow-divert stents for cerebral aneurysms. It was approved by the institution's medical ethics committee, but informed consent was waived due to the observational nature of this study which posed minimal risk to participants. The patients’ information came from the institution's database and comprised patients treated by the centre between June 1, 2014, and December 31, 2019. The Sim&Size® simulation software was used in all patients joining the centre after December 2017, the software acquisition date. Patients joining before the acquisition were not simulated. The study excluded patients with ruptured cerebral aneurysms and morphologies other than saccular.
The study evaluated the association between the use of the simulation software and its effect on the stent dimensions, surgical time, number of stents used, and complications. The data came from the medical records of patients treated with flow-diverter pipeline stents (Flex and Flex with SHIELD) for unruptured intracerebral aneurysms. This data included demographic information and comorbidities. The variables evaluated were aneurysm morphology, size and location, previous treatment of the aneurysm, the diameter and length of the stent, and the number of stents used. They also included surgical and follow-up times, intraoperative complications, aneurysms occlusion rates, and 30-days and 12-months post-procedure outcomes. Surgical time as the time between puncture and the end of anesthesia for the two groups of patients. The complications considered were thromboembolic, hemorrhagic, and vascular access complications, sudden stent shortening, and the need to adjust the stent position due to suboptimal stent size. The 3D angiography provided the size, location, and the number of aneurysms.
The centre relied on four neuro-interventionalists for the patient's treatment, and two participated in each procedure. The neuro-interventionalists had at least five years of experience in the endovascular treatment of intracranial aneurysms. Also, they had performed treatments with flow-diverter stents on at least ten occasions before the study evaluation period.
Stent deployment technique
All patients were started on ASA (100 mg per day) and clopidogrel (75 mg per day) 10 days prior to surgery. The antiplatelet activity was assessed 48 h before the procedure whit VerifyNow, considering an optimal value between 60 and 200. The Seldinger technique was used for the 3D digital subtraction angiography by puncturing the femoral artery under Doppler ultrasound guidance. The Destination catheter was raised, and unfractionated heparin was subministrated at a dosage of 50 IU per kilogram. Then, the activated clotting time was measured, and the intermediate catheter was placed in the petrous segment of the internal carotid artery (ICA). All cases used a pipeline flow-diverter stent implanted using the MarksmanTM microcatheter.
Stent manual sizing
Distal and proximal target landing zones were selected from a straight segment of the main vessel by the consensus of two operators during the manual stent sizing to ensure a good wall apposition. 2D-DSA parent artery measurements at the proximal target landing zone were used to determine implant diameter. Then, the operators predicted possible areas of stent elongation, particularly proximal to the aneurysm, and possible foreshortening. These predictions were based on the length of the aneurysm neck and the operators' experience. The stent length was estimated considering the parent vessel centreline measured between the distal and proximal target landing zones using the 3D-RA reconstruction of the Angio suite. All these measurements contributed to the choice of stent diameter and length.
Stent sizing with the simulation software
The commercially available, CE marked, and FDA approved Sim&Size® simulation software (version 1.2) was used to determine the stent size and simulate the stent behaviour according to the manufacturer's specification. This software reconstructs the 3D arterial geometry on a local computer using 3D-RA acquisition data and predicts the movement of endovascular devices such as pipeline stents. The accuracy of the reconstruction can be optimized by the operator when necessary. The software defines the microcatheter trajectory in the parent vessel and allows the operator to set the distal and proximal landing zones, targeting straight-vessel segments. Then, it determines the optimal flow-device dimensions and simulates its deployment within the chosen landing zones. In the interface, the software shows the degree of wall apposition, which appears as an interactive colour scale along the length of the stent. The effect of different landing zones and device dimensions on the device behaviour can be evaluated using the Sim&Size® simulation software. Also, the amount of ‘push’ applied during the deployment of the device can be estimated in real-time (Figure 1).
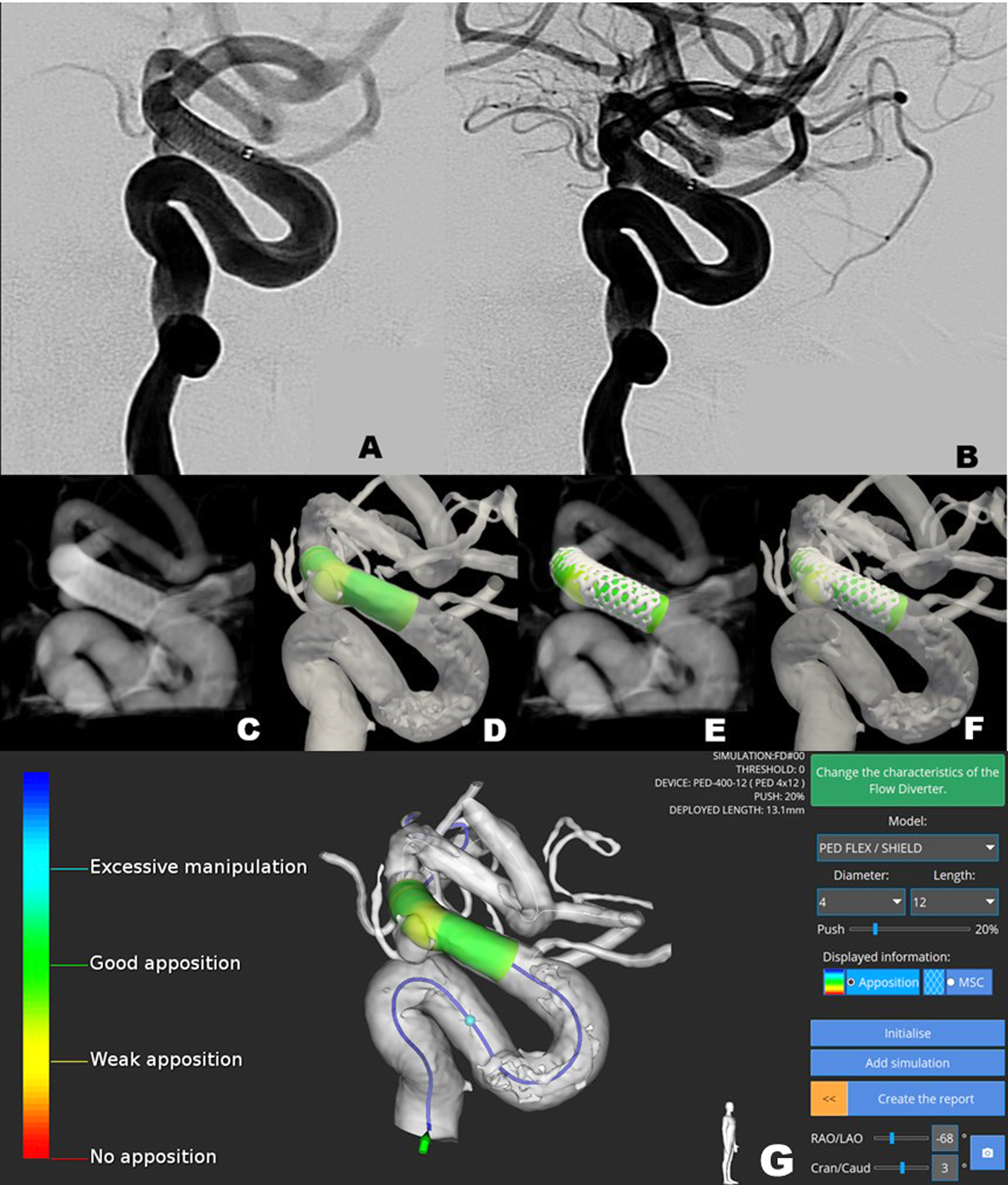
Representative images of a Sim&Size® simulation for a patient with an anterior chöroidal aneurysm. A: Projection of the aneurysm after pipeline flow-diverter stent deployment. B: Lateral projection of the aneurysm showing the stent proximal landing zone. C: Low contrast CT showing the stent wall apposition and proximal landing zone. D: Sim&Size® simulation indicating the proximal endings of the stent giving a good vessel wall apposition (Green). E and F: Simulated stent superposed on the Low Contrast CT showing a good correlation of the proximal landing zone. G. Sim&Size® simulation for a Pipeline Shield with a 4 mm diameter, 12 mm length, and 20% push. Here the pipeline shield does not cover the ophthalmic artery. The colour scale at the left shows the quality of the stent apposition with the parent vessel wall.
Statistical analysis
The demographic, clinical, and background characteristics of patients were analyzed using descriptive statistics. The categorical variables were reported as counts and percentages, and continuous variables as median and interquartile ranges (IQR). The student t-test was used to evaluate differences between the two groups of patients (i.e. with Sim&Size® simulation and without simulation) for the continuous variables following normal probability distribution. The Mann-Whitney test was used for non-parametric continuous variables and, for categorical variables, Fisher's exact test The normality of continuous variables was assessed using the Kolmogorov-Smirnov test
A multivariate analysis was used to assess the simultaneous predicting capacity of variables to differentiate between the two groups of patients (i.e. with Sim&Size® simulation and without simulation). Specifically, A binary logistic regression was modelled using the binomial family. The model included the variables showing differences between the two groups of patients with a confidence level of at least 92% (p-value < 0.080) in the bivariate analysis (i.e. aneurysm size, number of stents used, hemorrhagic complications, stent length, and occlusion occurrence). The model also included stent diameter and surgical time, as they were considered essential predictors. Model simplification was performed with a stepwise model selection by AIC using the R package MASS (version 7.3–13). 6
The effect of the aneurism localization-patient group interaction on stent diameter and diameter was evaluated using a two-way ANOVA and a generalized linear model with the Poisson family. This analysis only considered aneurisms localized in the ophthalmologic segment of the left ICA, the posterior communicating segment of the right ICA, the cavernous segment of the left ICA, and the left ICA as patients in both groups had aneurysms in these sites. All the analyses used a confidence level of 95% and the R package Stats (version 4.0.4) 7 unless otherwise stated, and the data was visualized using the R package Ggplot2 (version 3.3.3). 8
Results
In this study, the patient cohort comprised 75 patients with cerebral aneurysms treated with endovascular interventions using pipeline flow-diverter stents between June 1, 2014, and December 31, 2019. Our evaluations excluded seven of these patients, including three patients with fusiform aneurysms, two with dissections, one with a blister-like aneurysm, and one with a ruptured aneurysm.
The number of interventions performed was 73 for the 68 remaining patients. In the interventions, 64 dealt with single aneurysms, seven with two aneurysms that were embolized in the same procedure, and two with three aneurysms treated simultaneously using the same device. Only five patients required two interventions, while the rest required one. For patients receiving two interventions, four had separate aneurysms treated in each intervention as they were in separated cerebral hemispheres. The other patient had the same aneurysm treated twice.
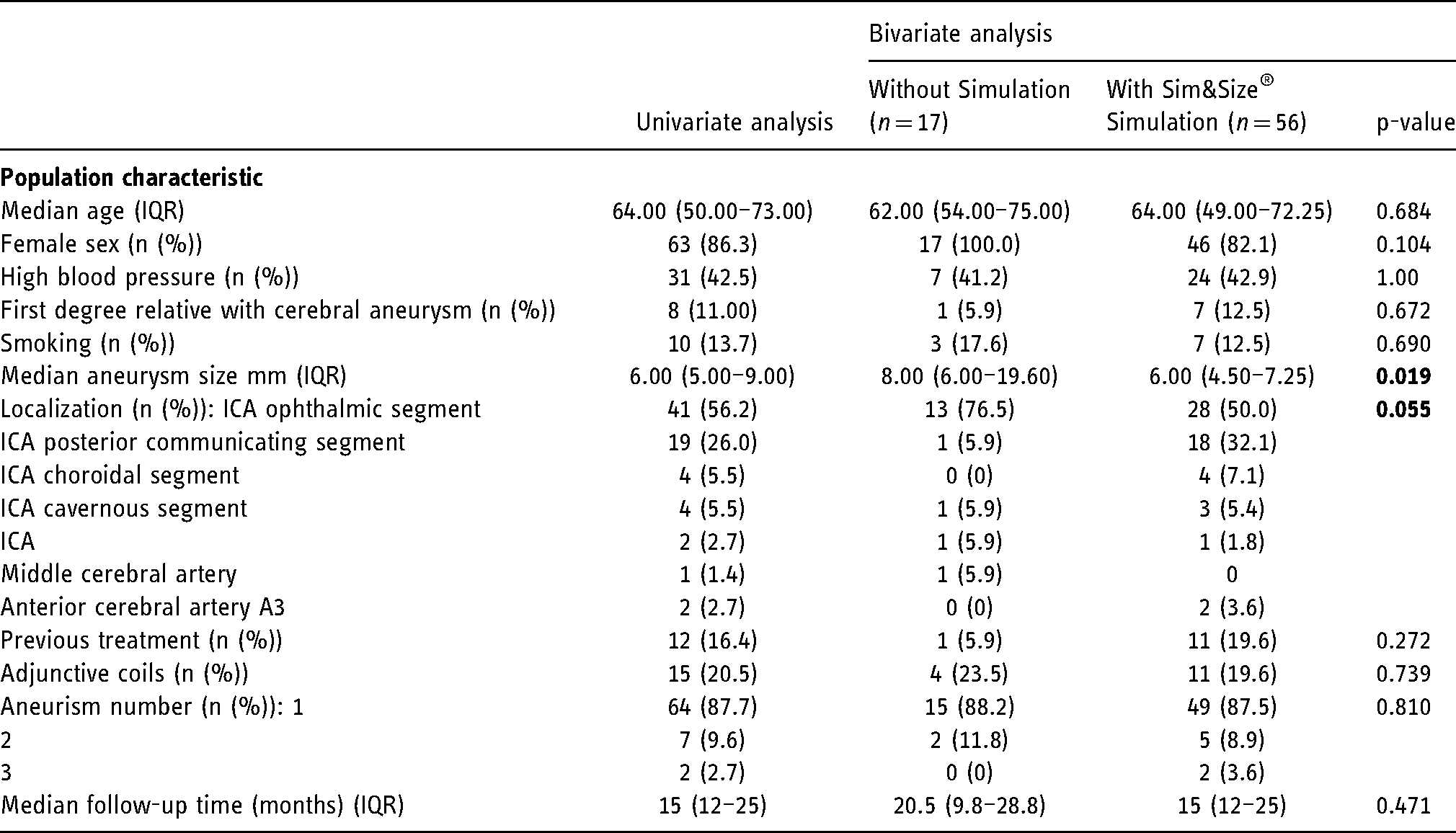
Most patients were women (86.3%), and the most prevalent comorbidities were high blood pressure (42.5%), followed by smoking (13.7%). The median age of patients was 64.00 IQR 50.00–73.00), and Table 1 summarizes the characteristics of the patients.
Demographic and clinical characteristics of the patients with cerebral aneurysms treated with endovascular interventions using pipeline flow-diverter stents.
Aneurysm characteristics
Most of the patients (56.2%) had multiple aneurysms, 34 of which belonged to the group with Sim&Size® simulation and seven to the group without simulation. Most of the aneurysms were at the ICA. Three were the exception and included two located in the anterior cerebral artery and one in the middle cerebral artery. The aneurysm greatest diameter had a median of 6.00 mm (IQR 5.00–9.00), with the lowest value of 2.00 mm and the largest of 40.00 mm.
Intervention and device
Fifty-six of the 73 interventions (76.7%) were simulated using the Sim&Size® software, while the remaining 17 (23.3%) used no simulation. The first intervention of patients requiring two interventions involved no simulation, while the second used the Sim&Size® simulation. The second intervention resulted in successful occlusion in all the cases (Table 2).
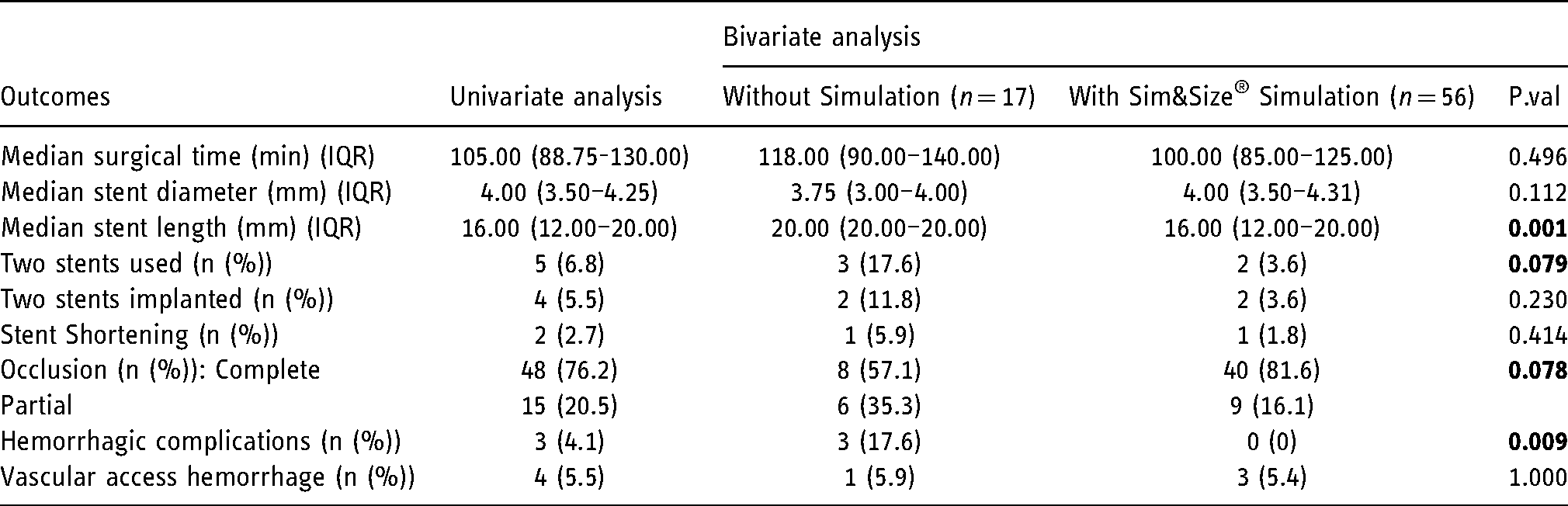
Surgical time had a median of 105.00 min (IQR 88.75–130.00), with the shortest procedure lasting 55.00 min and the longest 205.00 min. One of the patients belonging to the group with Sim&Size® simulation had no record of surgical time available. The median stent length was 16.00 mm (IQR 12.00–20.00), with the shortest stent being 12.00 mm long and the longest 35.00 mm. The median stent diameter was 4.00 mm (IQR 3.50–4.31), with the minor diameter being 2.50 mm and the widest 5.00 mm.
Patients belonging to the group with Sim&Size® simulation had shorter stent lengths than those in the non-simulated group (16.00 mm vs. 20.00 mm p-value = 0.001), and a lower proportion of them required more than one stent (3.6% vs. 17.6% p-value = 0.079). The surgical times also tended to be shorter in these patients (100.00 min vs. 118.00 min), but this result was not statistically supported (p-value = 0.496) (Table 2).
Only one stent implantation failed due to technical failure of the device. This failure occurred in one patient belonging to the group without stimulation. Four patients needed two stents to cover the neck of the aneurysm, one of them belonging to the group with Sim&Size® simulation. Two patients suffered from stent shortening, one of which was simulated during the preoperative phase, while the other was not.
Follow-up and aneurysm occlusion
A total of 63 (86.3%) of the 73 interventions had imaging follow-up. Fifty-three of them used 2D-DSA and 10 MRI. Forty-eight (65.8%) of the interventions had complete occlusion and 15 (20.5%) incomplete occlusions, with a median clinical follow-up of 15.00 months (IQR 12.0– 25.0). 71.4% of the interventions in patients belonging to the group with Sim&Size® simulation resulted in complete occlusion and had a median follow-up of 15.00 months. Only 47.1% of the interventions resulted in complete occlusion in patients without simulation, and the median follow-up was 20.50 months (Table 2).
Outcomes of patients with cerebral aneurysms treated with endovascular interventions using pipeline flow-diverter stents.
Complications
In this study, complications included three intracranial hemorrhagic complications, all of them in patients in the non-simulated group. One of these complications occurred during surgery and was secondary to an aneurysm rupture. The rupture happened during coiling while using coils and FD. The other two occurred after the surgical procedure, one in the immediate postoperative period and the other in the following 30 days. In both cases, intraparenchymal hemorrhage occurred without the involvement of the previously treated aneurysm, and the Fisher grade for these hemorrhages was Fisher III for one patient and Fisher IV for the other. The initial PRU was 128 for the patient having the intraparenchymal hemorrhage 30 days following the procedure. However, this value might be misleading as the clopidogrel responses can change over time, and the PRU at the moment of the hemorrhage was not included in the patient records.
Hemorrhagic complications related to femoral vascular access occurred in four patients, three belonging to the simulated group and one to the non-simulated group. No neurological sequelae secondary to complications were observed during the 30-day evaluation.
Four patients in the simulated group (6.3%) presented stent-related complications before the 12-month follow-up. One of these patients suffered a stroke occlusion of the right anterior choroidal artery six weeks after stent placement. This patient also had a non-optimal apposition of the stent at the origin of the anterior choroidal artery and a VerifyNow of 181 PRU, which is close to the upper limit of the test Regarding the other patients with stent-related complications, one patient suffered from left-monocular hemianopsia, and another from visual acuity decreases. The last patient experienced a 70.0% in-stent stenosis at 12-months follow-up. The mortality percentage for the study was 0% at the 12-month follow-up.
The multivariate analysis corroborated the bivariate analysis to some extent. It showed that patients presenting shorter stents (log odds = −0.21, Std. Error = 0.74, p = 0.003) but with increased diameter (log odds = 2.19, Std. Error = 0.07, p = 0.003) were more likely to come from the group with Sim&Size® simulation. Aneurysm size, number of stents used, hemorrhagic complications, occlusion occurrence, and surgical time gave no information about whether the patient underwent the simulation (p-value > 0.050).
The aneurism site impacted the stent diameter but only at a 93.4% confidence level (p-value = 0.066). Stents used to treat aneurism located in the posterior communicating segment of the right ICA had smaller diameters (p-value = 0.068, Figure 2A). However, these smaller diameters were independent of the patient group (i.e. patients with Sim&Size simulation and without simulation). For the stent length, the aneurism site had an impact (Figure 2B). Although, in this case, it depended on the patient group (p-value = 0.010) as most patients in the group with Sim&Size® simulation had shorter stents except for those with an aneurism located in the left ICA.
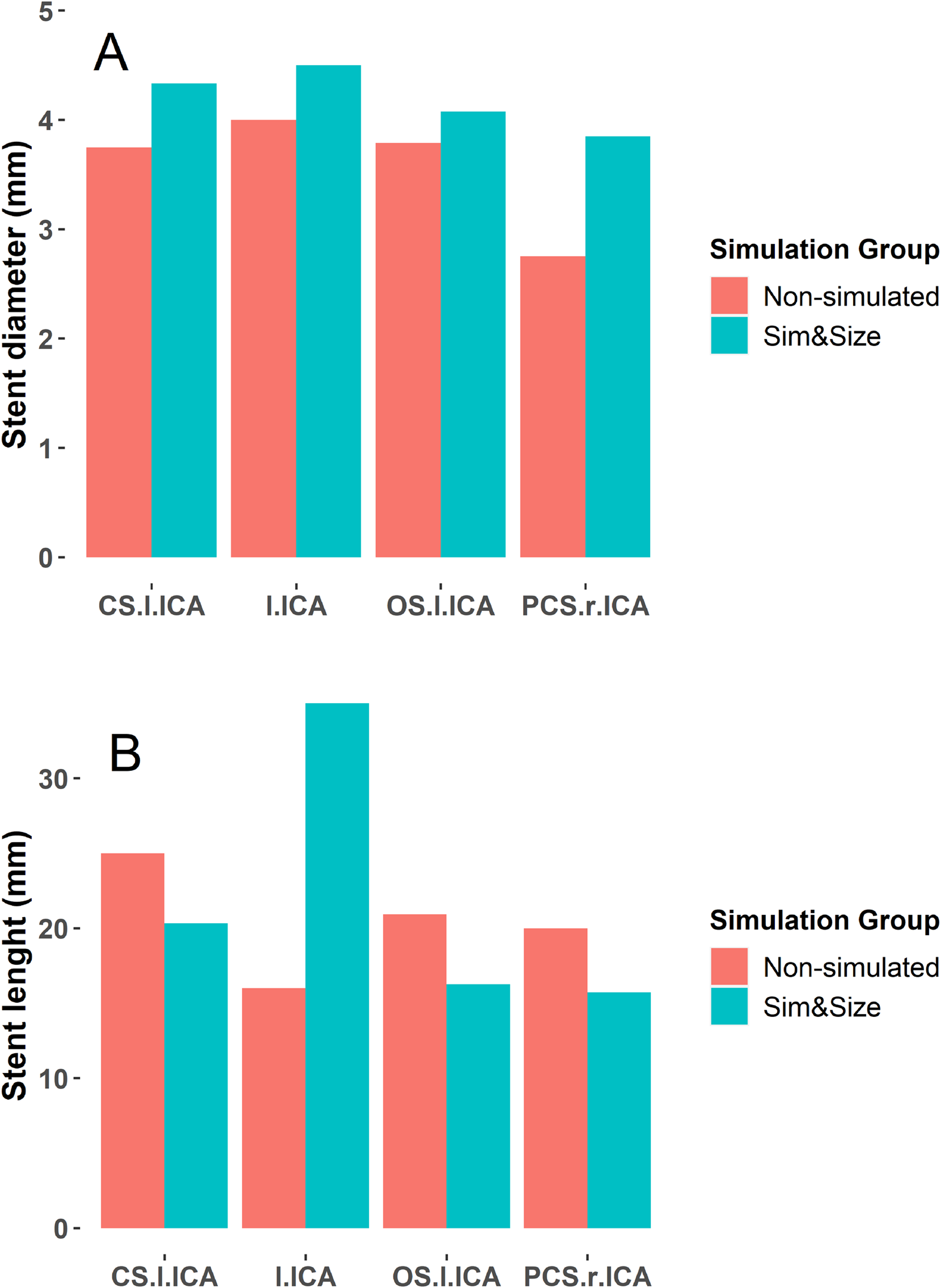
Dimensions of the pipeline flow-diverter stents used in the endovascular treatment of the patients with cerebral aneurysms according to the aneurism localization. Show are the mean stent diameter (A) and length (B) of the patients treated with and without the Sim&Size® simulation. CS.l.ICA denotes cavernous segment of the left internal carotid artery (ICA), l.ICA left ICA, OS.l.ICA ophthalmologic segment of the left ICA and PCS.r.ICA posterior communicating segment of the right ICA.
Discussion
Endovascular treatment of intracranial aneurysms with flow-diverter stents is a safe and effective treatment. 9 However, selecting the stent dimensions is challenging due to patient anatomy and the stent conformation. The Sim&Size® simulation software helps the neuroradiologist in this selection. 4 Nevertheless, only a few studies have evaluated the intraoperative and clinical impact of this simulation software. More patients belonged to the group that underwent Sim&Size® simulation in our cohort. This increased number is consequent with the technique's continuous evolution and the physicians' confidence in the simulation software. Also, it is in line with our centre's continuous improvement, which is a benchmark to our region. All the above acknowledged, it is crucial to consider that the experience gained by our team in this technique might have influenced our results to some extent.
Surgical time
Patients treated using the Sim&Size® simulation software tended to have shorter surgical interventions (median surgical time 100 min (IQR 85–125) versus 118 min (IQR 90 −140)). Despite the lack of statistical support (p-value = 0.496), we consider that this reduction in surgical time is crucial as it may represent a lower risk for patients. Other studies have shown that more prolonged neurointerventions result in higher complications rates. 10 In a similar study, Piergallini et al. 11 evaluated the effect of using the Sim&Size® simulation software for treating patients with cerebral unruptured aneurysms using flow-diverter pipeline stents. The authors also found shorter surgical times for patients treated using the simulation (46 min vs. 52 min p-value = 0.002). The differences between Piergallini et al. surgical times and ours come from the criteria used by the study to define this time. The surgical time in our study was the period between the femoral puncture and the femoral sheath removal, including catheterization. In comparison, Piergallini et al. measured surgical time from the catheter positioning in the internal carotid or vertebral artery to the end of the procedure.
Reducing surgical time in the operating room is critical for several reasons. Shorter times lead to more procedures per angiosuite and lower patient exposure to radiation. 12 However, our evaluations did not include the radiation dosage or fluoroscopy time of patients, and further studies are required to determine whether using the Sim&Size® simulation decreases the patients' radiation exposure. Also, they associate with lower rates of ischemic events in interventions treating intracranial aneurysms. 10 The Sim&Size® simulation software likely improves interventions by reducing the surgical time, leading to fewer complications and lower radiation doses.
Device size
During the simulation, the Sim&Size® simulated software predicts the proximal landing zone base on the patient's artery anatomy and the stent dimensions provided by the physician. Here, the software tries to set a landing zone in a straight segment of the parent artery. A proximal landing zone that is straight facilitates the apposition between the stent and artery surface. A good apposition improves the endothelialization process and decreases leaks. 13 The physician can modulate the stent dimensions until a desire proximal landing zone is achieved. In this manner, the Sim&Size® simulation software helps the physician determine the proper stent dimensions, which respond to the characteristics specific to the patient's vessel.
We found that using the Sim&Size® simulation software resulted in shorter stents (16 mm (IQR 12–20) v.s 20 mm (IQR 20–20) p-value = 0.001). These findings go in line with those reported in other studies, even though these other studies found stent length reductions that were less pronounced.11,14 Using shorter stents is beneficial as it decreases the chances of covering arterial branches originating from the parent artery. It also reduces the amount of metal inside the parent artery, which results in good appositions with the vessel wall. A proper apposition promotes endothelization and lowers intimal hyperplasia.
Stent diameter is also critical for stent design and is another parameter that can be established using the Sim&Size® simulation software, besides stent length. We found that using the Sim&Size® simulation software led to a tendency of greater stent diameters (4 mm (IQR 3.5–4.3) v.s 3.8 mm (IQR 3.0–4.0). However, the differences in stent diameters for patients coming from the two groups (with and without Sim&Size® simulation) lacked statistical support (p-value = 0.112). This lack of statistical support aligns with the findings of other studies.11,14
While Piergallini et al. 11 found decreased stent diameters in simulated patients (3.8 mm vs. 4.0 mm) and Ospel et al. 14 increased stent diameters (3.94 mm vs. 3.89 mm), none of these differences were statistically supported. Despite the lack of evidence for the effect of using the Sim&Size® simulation software on the stent diameter, we consider that the tendency towards greater diameters is interesting as they might result from the neurointervenionists trying to achieve a proper stent apposition into the vessel wall. The Sim&Size® simulation software shows a colour map illustrating stent contact with the vessel walls. A better wall apposition is linked to a larger diameter of the device as it assures no gaps between the stent and the vessel wall and reduces possible treatment failures.
Personalized medicine aims to achieve better outcomes for patients. Interventional Neuroradiology clinical practices have been using virtual simulation software such as the Sim&Size® simulation software during the treatment of patients with intracranial aneurysms. This software is improving the design process of flow-diverter stents. It helps physicians to find proper stents' dimensions, which reduces stent mispositioning and associated complications. An adequate apposition to the parent artery lowers the risk of device migration, late stent rupture, stroke, and acute thrombus formation.15–17 Additionally, using a stent with the proper dimension reduces the probability of stent shortening, lowers the need for a second device to cover the aneurysm neck completely, and helps cover branches emerging from the parent artery, such as the ophthalmic and anterior choroidal arteries.
Complications
Intracranial hemorrhagic, vascular access hemorrhagic and ischemic complications were 13.7%. Although, the rate of ischemic complications (4.1%) was less than those reported in the literature. 18 Four complications (5.5%) occurred in the puncture site of patients belonging to the group with Sim&Size® simulation. Nevertheless, the simulation did not induce these complications. None of them were associated with the stent placement, as they were related to antiplatelet therapy and coiling placement. Three intracranial hemorrhagic complications also occurred in our patient cohort, but all occurred in patients from the group without simulation. No mortality occurred after 30 days of the procedure.
Limitations
This study is limited as it is a retrospective, monocentric and non-randomized evaluation with a small sample size and lacked statistical power to support the differences found on some of the evaluated variables. Also, the number of patients without simulation was smaller than that of patients with Sim&Size® simulation. These differences resulted from our centre having a low neurointerventional activity before the Sim&Size® simulation software acquisition. The aneurysm sizes are smaller for patients in the group with Sim&Size® simulation, and they are found in less tortuous arteries segments than in the non-simulated group. These differences between aneurysms might have affected our result interpretations, especially for stent vessel apposition.
Conclusions
The use of Sim&Size® simulation software for the endovascular treatment of patients with intracranial aneurysms using pipeline flow-diverter stents reduces the stent length. It may also impact the number of devices needed per treatment and decrease the surgical time.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Ethical approval
This study was approved by the institution's medical ethics committee at FOSCAL clinic, the approval number was 02214/2020.