
Abstract
The Woven Endobridge (WEB; Microvention, Aliso Viejo, California, USA) is a relatively new device which has been shown to be safe and effective for the treatment of wide necked bifurcation aneurysms in multiple prospective Good Clinical Practice studies. However, the vast majority of aneurysms included in these studies have been unruptured. The aim of this review is to summarise the current evidence available on the treatment of ruptured aneurysms with the WEB.
Introduction and rationale
Endovascular coiling has become the treatment of choice for most ruptured aneurysms after the ISAT. 1 Wide neck bifurcation aneurysms (WNBAs), typically defined as having a neck dimension >4 mm or aspect ratio <2 are a therapeutic challenge.2,3 Stent assisted coiling (SAC) is routinely used to treat unruptured WNBAs. However, when used for ruptured aneurysms SAC has been associated with up to a 10-fold increase in adverse events – largely associated with the requirement for dual anti-platelet medication after stenting.4–6 Therefore a treatment option for ruptured WNBA aneurysms that does not require DAPT has the potential to overcome many of the issues associated with SAC.
Intrasaccular flow disruption is a relatively new endovascular technique that involves the placement of a device within the aneurysmal sac that modifies flow at the level of the aneurysm neck resulting in aneurysm occlusion. This is advantageous, as if appropriately sited it does not require the implantation of adjunctive devices or dual antiplatelet medications. The Woven EndoBridge (WEB; Microvention, Aliso Viejo, California, USA) is the best studied of these devices and has been shown to be effective and safe in a number of Good Clinical Practice Studies.7,8 This review will focus upon the available clinical experience documenting the use of the WEB to treat acutely ruptured aneurysms.
The Woven EndoBridge
The WEB was developed in 2010 primarily to treat wide neck bifurcation aneurysms without the requirement of adjunctive devices. It is a self-expanding structure of nitinol braids. Initially developed as a dual-layer structure (WEB-DL), advances in microbraid technology led to an iteration into single layer devices (WEB SL and WEB SLS). They are available in diameters of 3–11 mm and due to the requirement of oversizing this allows the stand-alone treatment of aneurysms ranging from 2–10 mm in diameter.
Search strategy and inclusion criteria
We performed a systematic review of the literature to identify articles that reported on the clinical experience of the WEB in ruptured aneurysms. We used the search terms ‘Woven Endobridge’ OR ‘WEB’ AND either of the terms ‘ruptured aneurysm’ OR ‘subarachnoid haemorrhage’. We searched PubMed and MEDLINE databases for articles published between January 2010 and October 2020. Figure 1 shows the flowchart for our search strategy. We included articles that included data for 10 or more ruptured aneurysms and reported on complications and clinical outcomes. For studies that reported on the treatment of ruptured and unruptured aneurysms we included articles that reported specific intergroup data allowing the extraction of data specifically for those ruptured aneurysms. In total 11 articles were included for further analysis and discussion: 6 studies9–14 reporting only on the treatment of ruptured aneurysms with the WEB were included and data on the treatment of ruptured aneurysms were included from 5 studies that reported on ruptured and unruptured aneurysms.15–19 Individual data can be viewed in Table 1.
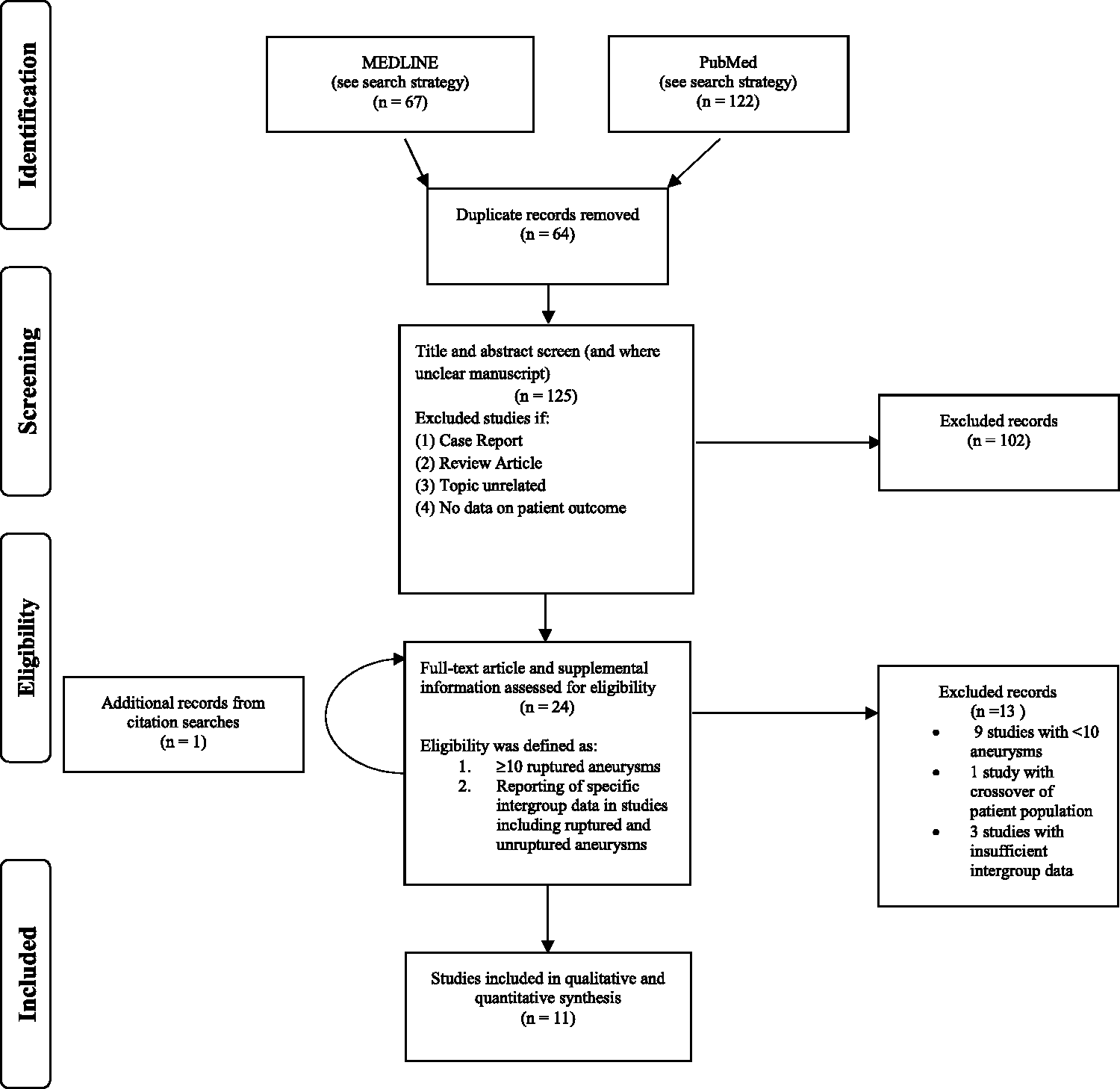
Flowchart for our search strategy.
Data from each of the studies included in the review.
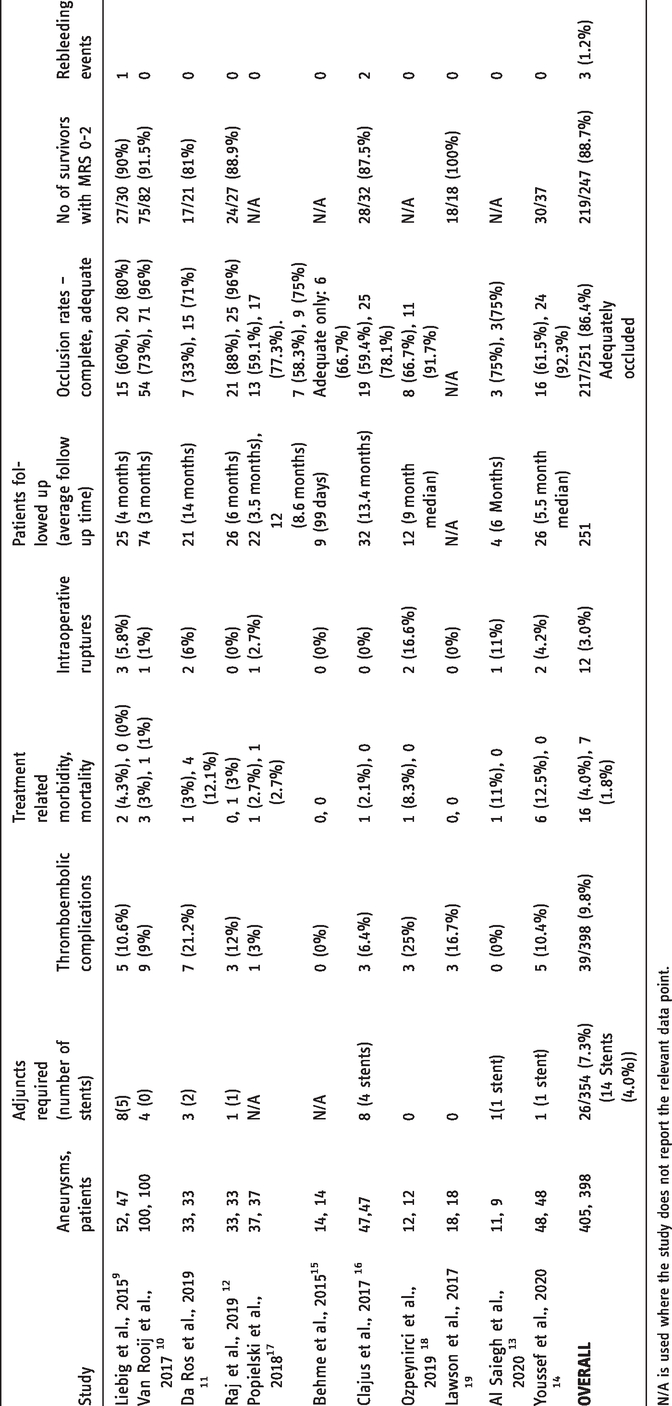
N/A is used where the study does not report the relevant data point.
Aneurysm characteristics
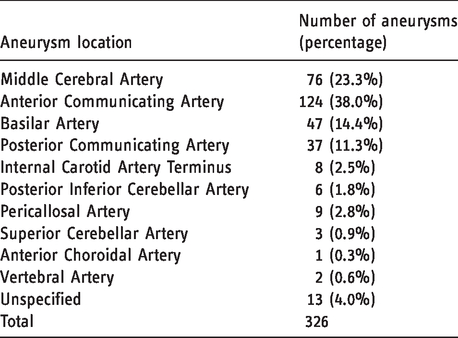
The number of patients treated in each study varied from 9–100 with 405 aneurysms treated in 398 patients. The proportion of aneurysms sited in the anterior circulation varies between 45–92%. The specific location of the aneurysm was reported in 8 of the studies9–14,17,18 and the number and proportion can be seen in Table 2. 3 studies included only aneurysms with a wide neck,11,12,17 whereas the remaining proportions were 94%, 9 92%, 18 90%, 13 81%, 16 and 66% 10 in those reporting. The proportion of patients presenting with a severe SAH (Hunt and Hess scale of 4 or 5) was 7–56% in those that reported this.9–13,15–17
Technical completion and adjunctive devices
The rate of technical success amongst the studies varied from 95.8–100%. The proportion of aneurysms requiring adjunctive techniques to achieve acceptable occlusion ranged from 0–15% between studies. 14 (4.0%) stents were required across 9 of the studies and protrusion of the WEB into the parent vessel was the most frequent indication for stenting.9–13,16 These data suggest that the WEB can be used effectively for ruptured wide necked aneurysms without the need for adjunctive devices in most cases.
Procedural complication
A particular concern in the treatment of aneurysmal SAH with the WEB is the potential for thromboembolic events (TE). Indeed a systematic review on the WEB, primarily including data on unruptured aneurysms, found that 70% of complications related to the WEB were thromboembolic in nature. 20 The risk for patients with aneurysmal SAH is increased due to the pro-thrombotic state induced by SAH, 21 the thrombogenicity of the WEB device at the parent artery-aneurysm neck interface and the absence of anti-platelet medication pre-treatment in many ruptured patients. To stabilise the microcatheter during deployment of the WEB a distal access catheter is required, and movements of this catheter could contribute to TE. 10 Device protrusion has been noted to cause TE and this is often the result of device oversizing.9,11,22 It should be noted that ruptured aneurysms often have irregular anatomy with the presence of a daughter sac and when sizing the WEB this extra sac should not be incorporated into sizing calculations. The rate TE reported in the studies ranged from 0–25% for the 10 studies, with 39 TE’s for 398 patients (9.8%). Most of the TE were managed without clinical consequence – typically with IV or IA IIb/IIIa receptor antagonists. Only 11 (28%) of the 39 patients who suffered TE were reported to develop any morbidity as a consequence. One group 11 found a particularly high rate of TE (21%) although procedures in this study were performed without heparin, this may have contributed to that result. Only one study had a higher rate of 25%, however the sample size of 12 likely affected this. 18 The CLARITY series of endovascular treatment of ruptured aneurysms with coiling reported a rate of TE of 13.3%. 23 When further analysis was performed to assess for the subset of wide necked aneurysms (neck > 4mm) this rate rose to 20.8%. 24 More recently, the ARETA study reported a rate of TE of 10.4% in a population of 753 ruptured aneurysms treated with coiling. 25 Therefore the evidence suggests that the treatment of intracranial ruptured aneurysms with the WEB has a rate of TE that is generally in line with alternative coiling strategies.
Intraoperative aneurysm rupture by the WEB device or the tip of the microcatheter has been observed in most studies.9–11,13,14,17,18 The rate of rupture in the studies ranged from 0–16.6%. Tortuous anatomy within two anterior communicating artery (Acom) aneurysms is suggested to have led to unintended catheter tip motion at the time of WEB deployment, this resulting in intraoperative rupture. 11 The anatomy associated with Acom and Pcom aneurysms is more angulated and requires more manipulation of catheter systems than the approach to MCA bifurcation or basilar tip aneurysms, and the authors suggest this factor is related to the risk of intraoperative rupture. 7 of the 12 ruptures occurring in all studies were for Acom or Pcom aneurysms and 5 of these events were due to unintended movement of the microcatheter tip before WEB deployment.9,17,18 The stiffness of the larger inner diameter VIA microcatheters may contribute to the risk of rupture, with these catheters being subjectively more rigid than typical coiling microcatheters. 11 A series of 46 aneurysms treated with the newer VIA-17 system, including 25 ruptured aneurysms, found no procedural ruptures and the group noted the ease with which this system navigated complicated anatomy. 26 The VIA-17 system is currently only available for aneurysms up to 7 mm in diameter – however this size range does cover the majority of ruptured saccular aneurysms. Importantly during intra-operative aneurysm rupture deployment of the WEB can achieve rapid haemostasis within one minute.10,11 This haemostatic property of the WEB adds to its’ safety profile and due to the rapidity of hemostasis following deployment, limits the clinical consequence of procedural perforation. This is important as the current dimensions of microcatheters used do not always permit adjunctive balloon use. 11 The CLARITY series reports a rate of intraoperative rupture of 3.7% for coiling of ruptured aneurysms 23 which is similar to that seen in our review of the WEB (3.0%).
Morbidity and mortality
Death from sequelae of the SAH ranged from 6.3–21% between the studies apart from 2 smaller studies which recorded no mortality.18,19 There were 7 incidences of procedural related death across the studies. Massive TE events arising from the WEB at the parent artery-aneurysm interface was the cause in 2 cases,10,17 clear device protrusion the cause in 3, 11 1 case of intraoperative rupture, 11 and one suspected case of hydrophilic polymeric embolization. 12 Da Ros et al., 11 noted significant issues with accurately sizing the device, and subsequently this led to a device protrusion rate of 15% and 3 deaths. The use of in-room cone-beam CT prior to WEB detachment has been shown to detect this complication before the device has been permanently deployed. 27 In fact, Da Ros et al., note that since having this technology available at their centre device sizing has become more accurate. 11 One group noted 2 deaths from SAH, both in patients who suffered a procedural complication (aneurysm perforation and induced vasospasm). 9
Treatment related morbidity and mortality ranged between 0–15% between the studies. Combining the data from the studies, treatment related morbidity was 4.0% (16/398) and mortality was 1.8% (7/398). These safety data are also in line with the data from the CLARITY study which reported treatment related morbidity of 3.7% and mortality of 1.5%. 23
Follow up occlusion
Between the studies the rate of complete occlusion at follow up ranged from of 33–88% and adequate occlusion (defined as those completely occluded and those with a small neck remnant) from 71–96%. None of the studies had a routine follow up schedule and only one study reviewed occlusion twice (median of 3.5 and 8.6 months). 17 The average interval to follow up varied between 3–14 months in the remaining studies. In all, 251 patients were followed up across the available studies with 217 (86.4%) showing adequate occlusion. The reliability of these findings are limited because of the varied follow up schedules, the large proportion of patients lost or unable to follow up and the use of differing imaging modalities for follow up (CTA,MRA and DSA). The largest reported rate of adequate occlusion (96% at 3 months) was also reported in the largest study (100 patients). 10 This may be reflective of the aneurysm characteristics of the study population: 44 aneurysms were small with a diameter of <4mm and 44% of the aneurysms did not meet criteria for a wide neck (>4mm or dome to neck ratio <1.5). Smaller aneurysms with a smaller orifice in this cohort may have contributed to the favourable findings at early follow up. Current data suggests that the WEB is capable of stable occlusion in ruptured aneurysms however, prospective long-term studies are needed to assess the adequacy and durability of occlusion.
Rebleeding and retreatment
Rebleeding from an aneurysm treated with the WEB was only reported in 3 cases.9,16 Given that within the 11 studies 247 patients were followed up, the re-rupture rate would be 1.2%. This figure is smaller than that reported in studies using other techniques. A series of ruptured wide neck aneurysms treated with stent assisted coiling reported a rebleeding rate of 4.5% 28 and ISAT found a re-bleeding rate of 1.8% at 1 year of follow up in those treated with coils and surgical clipping. 1 The number of aneurysms requiring retreatment ranged from 6.8–16%. Survivors at follow up (>3 months from SAH) had a good neurological outcome (mRS ≤ 2) in 81–100% of cases.9–12,14,16,19 The Clinical Assessment of WEB Device in ruptured aneurysms (CLARYS) study is the first prospective trial for ruptured aneurysms treated with WEB. A total of 58 patients were recruited and the 1 month follow up showed the WEB successfully prevented any recurrent haemorrhage with longer term (12 month) follow-up pending. 29
Overall the existing literature suggests a very low chance of repeat haemorrhage with successful WEB implantation.
Conclusion
In conclusion, the available data indicate that the treatment of ruptured aneurysms with the WEB device is feasible, safe and effective in comparison to other endovascular techniques. Most importantly in the management of subarachnoid haemorrhage the WEB is effective at preventing repeat haemorrhage from the target aneurysm. The existing studies, with the exception of CLARYS, are retrospective and operator adjudicated. None of the existing studies used a concurrent active control group to allow direct comparison to other contemporary endovascular treatments.
The advantages of the WEB mean it is a useful technology for the treatment of selected ruptured aneurysms. Further prospective studies will be critical in confirming the peri-procedural and long-term safety and effectiveness.
Footnotes
Author contributions
WC – manuscript preparation, review, editing.
PB –review, editing, guarantor.
CC – review, editing.
HLDM – review, editing.
KW – review, editing.
DF – review, editing.
AA – review, editing.
HH – review, editing.
LP – review, editing.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article:
P. Bhogal—consultant for phenox.
C. Cognard—consultant for Stryker, Medtronic, Cerenovus and Microvention.
H. L. D. Makalanda—Consultant: Microvention, Penumbra, Balt, Cerenovous, Stryker, Neuroventures.
K. Wong—none declared.
D. Fiorella—Consultant: Medtronic, Microvention, Penumbra, Balt, Cerenovous, Stryker, Research Support: Siemens, Microvention, Penumbra, Cerenovous, Stockholder: Marblehead, Neurogami, Vascular Simulations, Board Member: Vascular Simulations.
A. Arthur—consultant for Balt, Johnson and Johnson, Leica, Medtronic, Microvention, Penumbra, Scientia, Siemens, Stryker. Shareholder in Bendit, Cerebrotech, Endostream, Magneto, Marblehead, Neurogami, Serenity, Synchron, Triad Medical, Vascular Simulations.
H. Henkes—co-founder and shareholder for phenox GmbH and femtos GmbH.
L. Pierot—consultant for Balt, Cerus Endovascular, MicroVention, Phenox, Vesalio, Penumbra.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.