
Abstract
Background
In US hospitals, the liquid embolic systems (LESs) n-butyl cyanoacrylate (n-BCA) and ethylene vinyl alcohol copolymer (EVOH) are used for brain arteriovenous malformation (bAVM) embolization to achieve presurgical devascularization. The aim of this study was to perform an economic analysis comparing four techniques for bAVM embolization based on LES, ancillary device, and angiography suite time costs.
Methods
An economic model was developed comparing the embolization costs for n-BCA, EVOH with the plug and push technique, EVOH with detachable-tip microcatheters, and EVOH with balloon microcatheters. Per procedure costs were calculated for bAVMs with one to four pedicles. Annual cohort analyses were performed to evaluate the potential impact for low and high-volume centers. Sensitivity analyses were performed to determine cost drivers.
Results
The analyses showed that the n-BCA technique was the least costly of the four techniques. Total per procedure costs for one to four embolized pedicles ranged from $5941 to $10,074 for the n-BCA technique, $8428 to $30,345 for the EVOH balloon microcatheter technique, $12,711 to $47,477 for the EVOH plug and push technique, and $13,900 to $52,233 for the EVOH detachable-tip microcatheter technique. Cohort analyses costs for 52 annual cases ranged from $308,953 to $523,838 with the n-BCA technique and from $722,816 to $2,716,096 with the EVOH detachable-tip microcatheter technique.
Conclusions
Procedure costs associated with n-BCA are lower than those with each of the three EVOH techniques examined. Future cost analyses should compare the costs of new LES products once available.
Introduction
Brain arteriovenous malformations (bAVMs) are uncommon vascular lesions characterized by direct arterial to venous shunting connected with histologically abnormal vessels or nidus (without intermediate capillaries). 1 Globally, asymptomatic bAVMs affect an estimated 50 per 100,000 people while symptomatic bAVMs affect 10 to 18 per 100,000 people.1,2 While unruptured bAVMs may present asymptomatically, the annual risk of hemorrhage is significant,1,3–5 and is associated with a significant risk of mortality and morbidity including permanent neurological deficits.6,7 Surgical removal of bAVMs to mitigate acute hemorrhage is often warranted, 7 despite the risk of hemorrhage. Brain AVM features such as deep location, eloquent location, or large size/volume may increase surgical morbidity related to blood loss. 1 Embolization of bAVMs can be performed to eliminate high-risk features (feeding artery aneurysms, intranidal aneurysm or venous varix/aneurysms) or for pre-operative devascularization (reduce intraoperative blood loss). 8 Two liquid embolic systems (LESs) commonly used to achieve presurgical bAVM devascularization are n-butyl cyanoacrylate (n-BCA; TRUFILL® Liquid Embolic System, Cerenovus, Irvine, CA) and ethylene vinyl alcohol copolymer (EVOH; Onyx™ Liquid Embolic System, Medtronicplc, Minneapolis, MN). 8
n-BCA and EVOH have unique properties and mechanisms of action. Briefly, n-BCA is an adhesive polymer that is diluted with ethiodized oil mixed with tantalum powder for use in bAVM embolization. Upon contact with body fluids and tissue, n-BCA polymerizes into a solid, radiopaque, thrombogenic material that prevents blood flow through the embolized bAVM pedicle.9,10 The n-BCA solution can be combined with different volumes of ethiodized oil to produce varying concentrations thereby tailoring the polymerization based on the clinical characteristics of the bAVM. 9 EVOH is a non-adhesive liquid that precipitates out of the dimethyl sulfoxide (DMSO) tantalum powder solution used to deliver it to the cannulated AVM pedicle.9,11 After precipitation, EVOH forms a minimally thrombogenic, radiopaque, spongy cast that prevents blood flow through the embolized bAVM pedicle. 9 In the US, EVOH is available in two concentrations with corresponding precipitation rates 9 and cannot be mixed or altered. Given these differences, deployment technique and required equipment are tailored to the bAVM and the LES.
A single RCT and several retrospective observational studies compare n-BCA and EVOH for the embolization of bAVMs and report nidal volume reduction, complete bAVM occlusion, procedure duration, fluoroscopic imaging duration, blood loss, and complication outcomes.9,12,13 Statistically significant differences were reported in procedure duration, fluoroscopic imaging duration, and complications related to catheter retention. Velat et al. reported procedure duration outcomes 12 that could be used to inform an economic analysis. In that retrospective observational study of 182 embolizations in 88 patients, the total procedure time required for n-BCA procedures (2.1 h) was significantly shorter than for EVOH procedures (2.6 h, p = 0.001). 12 In the same study, fluoroscopy time per procedure with n-BCA (37 min) was significantly shorter than with EVOH (57 min, p < 0.0001). 12 An RCT showed that catheter retention occurred in 9.3% (5/54) of patients with EVOH embolization and 1.6% (1/63) of patients with n-BCA embolization. 9 EVOH delivery may be complicated by reflux along the tip of the microcatheter that may lead to catheter retention or embolization of non-target vessels.14,15 Detachable-tip microcatheters may be used with EVOH bAVM embolization to mitigate risks related to catheter retention. 15 Balloon microcatheters can be used with EVOH bAVM embolization to reduce EVOH reflux around the microcatheter and expedite procedures because a plug does not need to be formed. 14 While n-BCA and EVOH have different mechanisms and procedural application, meaningful differences in bAVM presurgical devascularization efficacy have not been demonstrated.9,12,13
Despite the available clinical data, economic analyses have not been conducted comparing the procedure-related costs associated with n-BCA and EVOH bAVM embolization. Thus, the objective of this study was to develop an economic analysis to compare the procedural costs of n-BCA and EVOH bAVM embolization including LES and ancillary device costs (for microcatheters), as well as procedure time-related costs associated with different embolization techniques.
Methods
Model comparisons and assumptions
An economic analysis of procedural costs of four bAVM embolization techniques: n-BCA with a Prowler microcatheter (Cerenovus), EVOH with “plug and push”, EVOH with a detachable-tip microcatheter, and EVOH with a balloon microcatheter. The costs in the analysis included the LESs, ancillary devices, and procedure time. Device costs as reported are average sales prices sourced by third party software PriceTrack derived from anonymized purchase orders from participating facilities. 16 A staged embolization approach is often used to partially occlude a bAVM nidus for presurgical devascularization, 12 thus, the analysis considered embolization on a per pedicle basis rather than comparing LESs in a volume to volume manner. This approach also standardized the analysis given that bAVMs that require presurgical embolization may be highly variable in size and volume (for example, a range of 0.08–290 cm3 was reported by Loh et al. 9 ). The total number of LES kits required to embolize one to four pedicles per patient with each technique was considered. For this analysis, the bAVMs treated were assumed to be similar. Each pedicle was embolized with the number of kits and microcatheters outlined in Table 1 as informed by the instructions for use for each agent. Each additional pedicle was embolized with the same number of LES kits and microcatheters as the number used for one pedicle. Additional details of embolic agent kit volumes used per technique are described below.
Total devices used per procedure based on the number of pedicles embolized and device costs.
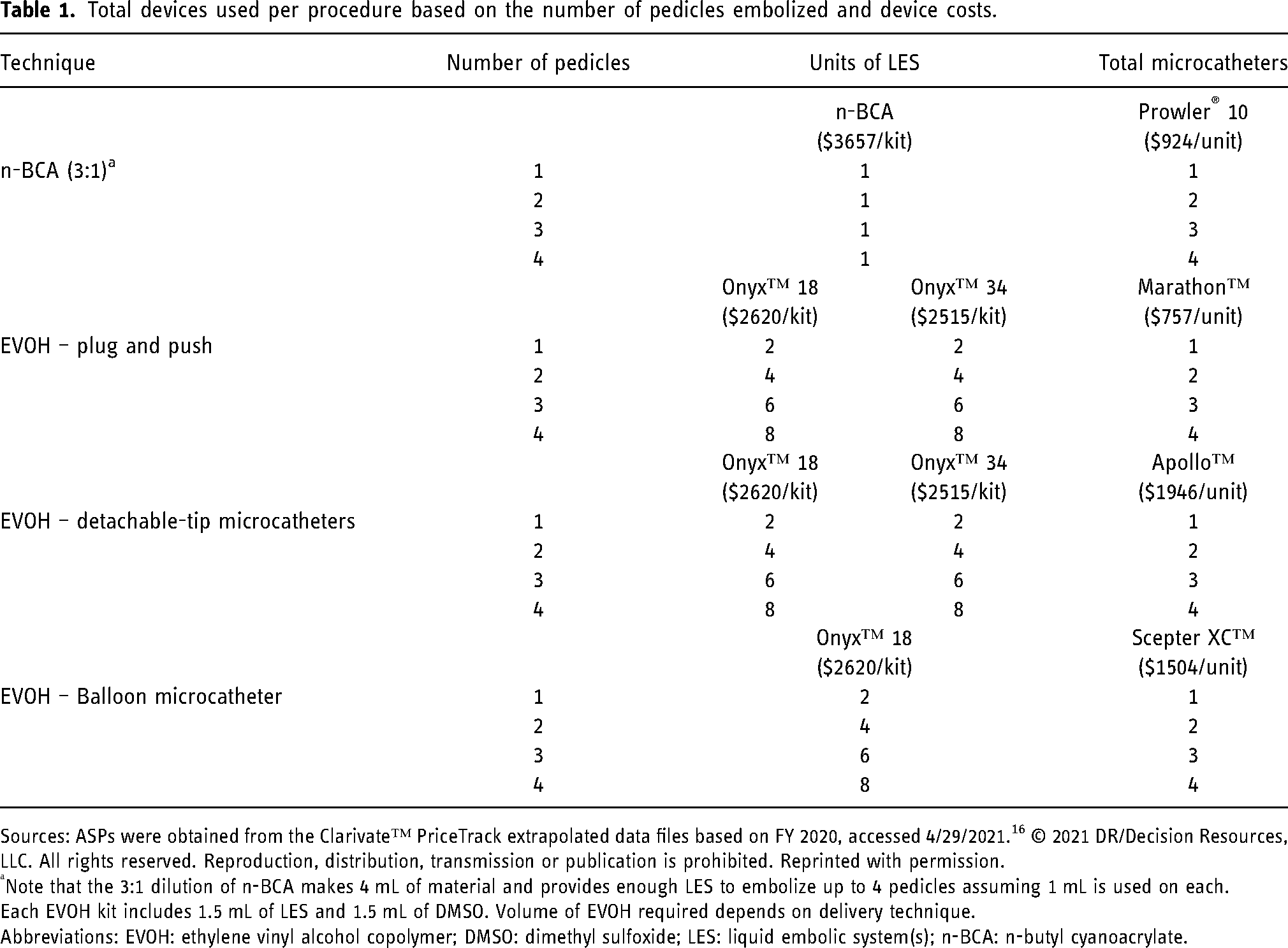
Sources: ASPs were obtained from the Clarivate™ PriceTrack extrapolated data files based on FY 2020, accessed 4/29/2021. 16 © 2021 DR/Decision Resources, LLC. All rights reserved. Reproduction, distribution, transmission or publication is prohibited. Reprinted with permission.
Note that the 3:1 dilution of n-BCA makes 4 mL of material and provides enough LES to embolize up to 4 pedicles assuming 1 mL is used on each.
Each EVOH kit includes 1.5 mL of LES and 1.5 mL of DMSO. Volume of EVOH required depends on delivery technique.
Abbreviations: EVOH: ethylene vinyl alcohol copolymer; DMSO: dimethyl sulfoxide; LES: liquid embolic system(s); n-BCA: n-butyl cyanoacrylate.
Embolization techniques
For each of the four techniques, device utilization per procedure with total devices used based on the number of pedicles embolized is outlined in Table 1.
n-BCA technique
A 3:1 mixture of ethiodized oil mixed with tantalum powder and n-BCA was assumed for the primary analysis. A TRUFILL® n-BCA kit (Cerenovus) contains a 10 mL vial of ethiodized oil, 1 g of tantalum powder, and 1 mL of n-BCA, which can be used to prepare 4 mL of the 3:1 dilution. 10 It was assumed that a maximum of 4 mL of LES mixture would be required if up to 1 mL were used to embolize each pedicle (see Table 1). After cannulating the target pedicle, up to 0.5 mL of n-BCA is injected to embolize it, then a branch run angiogram is performed to visualize the embolized pedicle (Figure 1(a) and (b)). Once sufficient pedicle embolization is confirmed, the Prowler 10 microcatheter is carefully withdrawn from the bAVM. The Prowler microcatheter was selected as the ancillary device because it is recommended for use with n-BCA by the IFU. 10
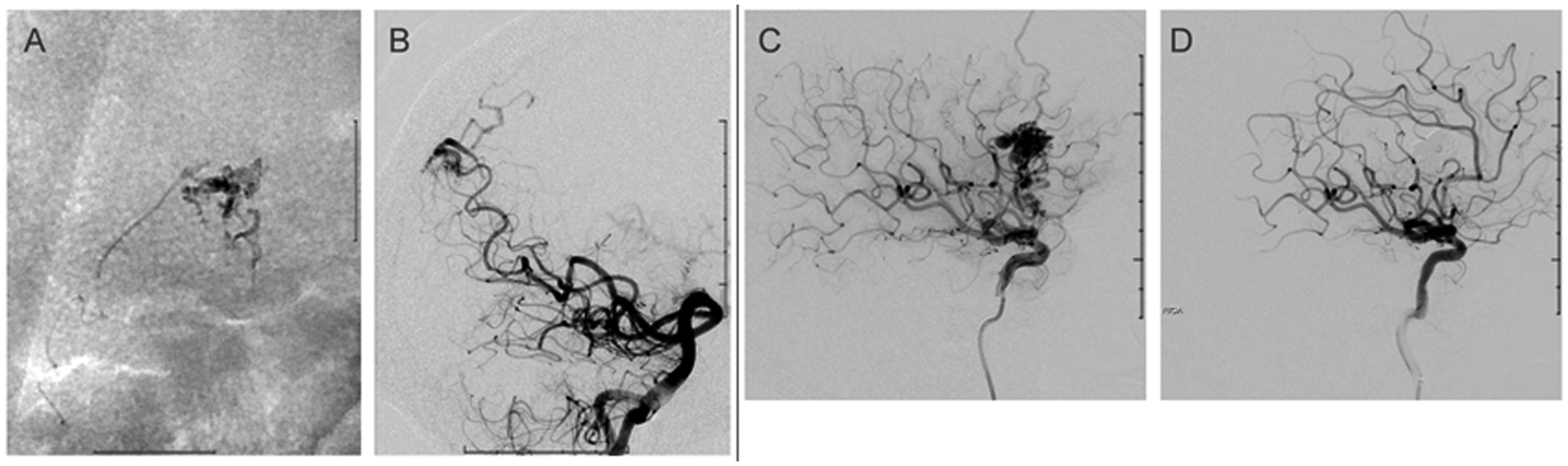
Example radiographs of the EVOH and n-BCA techniques. (a-b) n-BCA Technique: (a) Embolization was performed using n-BCA for the SCA AVM. (b) Post embolization complete obliteration cerebellar AVM (no residual shunting). (c-d) EVOH Plug and Push Technique: Embolization was performed using Onyx™ 34 as the plug and Onyx™ 18 for the push. (c) Right frontal AVM (2.0 × 1.7 × 1.5 cm); anterior MCA – superficial drainage frontal/temporal cortical veins in the superior sagittal sinus and right sphenoparietal sinus. (d) Post embolization complete obliteration AVM (no residual shunting). Abbreviations: AVM: arteriovenous malformations; MCA: middle cerebral artery; SCA: superior cerebral artery. Source: Dr. Sudhakar R. Satti, Neurointerventional Surgery, Christiana Care Health System.
EVOH plug and push technique
The plug and push technique with EVOH (Onyx™ 18 and Onyx™ 34, Medtronic plc) involves slowly injecting a plug of Onyx™ 34 embolic agent in front of the catheter tip and allowing it to reflux until it reaches the tip followed by injection of Onyx™ 18 for pedicle penetration (see Table 1).17,18 An Onyx™ EVOH kit contains 1.5 mL of either Onyx™ 18 (6% EVOH) or Onyx™ 34 (8% EVOH) and 1.5 mL of DMSO. 11 Two kits each of Onyx™ 18 and Onyx™ 34 were used for this technique. If EVOH refluxes to the catheter tip during the Onyx 18 “push”, embolization is paused allowing polymer precipitation, 17 then additional EVOH is injected in small volumes and, ideally, pushed into the target vessel (Figure 1(c) and (d)). 19 The microcatheter is removed by gently applying tension until the tip detaches from the cast. 17 Use of Marathon™ microcatheters (Medtronic plc) was assumed for the plug and push technique since it is a DMSO-compatible microcatheter indicated for neurovascular use. 11
EVOH detachable-tip microcatheter technique
EVOH with detachable-tip microcatheters (Apollo™, Medtronic plc) are used to avoid the risk of retaining the entire microcatheter and associated complications when the tip of the catheter will not easily detach from the EVOH cast embolizing the nidus. 15 It was assumed that two kits each of Onyx™ 34 and Onyx™ 18 were required per pedicle for this technique and that embolization was performed using the plug and push technique (see Table 1). Once EVOH has been injected using a detachable-tip microcatheter and embolization is complete, it is gently withdrawn until it either releases from the EVOH cast or until the tip detaches. 15
EVOH balloon microcatheter technique
EVOH with balloon microcatheters (Scepter XC™, MicroVention Inc., Aliso Viejo, CA) is performed to help prevent reflux of EVOH during the embolization procedure. It was assumed that two kits of Onyx™ 18 are required per pedicle for this technique (see Table 1). Once the target pedicle is cannulated, the balloon distal to the microcatheter tip is inflated to allow for embolization of the bAVM with EVOH and prevent excess reflux. 14 When embolization is complete the balloon is deflated and the microcatheter is gently withdrawn until it releases from the EVOH cast.14,18
Cost analyses
Cost analyses were performed for the four techniques with the device utilization per pedicle and per procedure outlined in Table 1. Device costs used in the analyses were annual 2020 United States Dollar (USD) average selling prices (ASPs) and are outlined in Table 1. Annual cohort analyses were performed to estimate the costs of treating twelve bAVM cases per year for low volume centers and fifty-two cases per year for high volume centers.
Procedure time analysis inputs
Model procedure time inputs were obtained from the Velat et al. study 12 where procedure duration per embolization (i.e. per pedicle) with n-BCA was 2.1 h versus 2.6 h with EVOH (p < 0.001). 12 Note that Velat 12 did not report details of the EVOH techniques used and procedure outcomes were not reported separately by technique. Additionally, Velat et al. reported that on average 1.7 pedicles were embolized per patient with n-BCA and 1.8 pedicles were embolized per patient with EVOH. 12 Thus, procedure duration inputs used for the 1 or 2 pedicle analyses were 2.1 h and 2.6 h for n-BCA and EVOH, respectively. For 3–4 pedicle procedures it was assumed that procedure time would be twice as long, 4.2 h and 5.2 h for n-BCA and EVOH, respectively. Although there are important differences in the methods of EVOH embolization examined here, procedure times for EVOH were assumed to be equal to the average reported by Velat and colleagues. 12 Variation in procedure duration was examined in the sensitivity analyses.
The hourly cost of angiography suite time ($539) was obtained from Beheshti and Meek 20 and was inflated to $647.81 in 2021 USD. The angiography suite hourly costs included $75.27 for angiography suite direct fixed costs, $290.30 for direct labor costs, $21.24 for indirect overhead facility costs, $73 for indirect hospital overhead and administrative costs, and $79 for college of medicine overhead and administrative costs. 20 The labor costs included amounts for interventional radiology personnel: 1.5 technologists, 1.2 nurses, 0.7 administrative support, 1 faculty, 1 fellow, and 0.35 coordinators per hour. 20 Costs were inflated from 2014 to 2021 USD using the medical care component of the CPI index for all urban consumers. 21 Note that angiography suite costs do not include costs for length of stay and associated overhead or other consumables.
Sensitivity analyses
Sensitivity analyses varied cost categories by ±20% for all LESs, all microcatheters, or angiography suite costs (hours or cost/hour). Unit costs may have limited generalizability due to variable facility contracting, rebate, and bundling arrangements with manufacturers. We conducted a sensitivity analysis to address this limitation in product cost, and for the angiography suite costs from Beheshti and Meek. 20
Results
Per procedure and annual cohort analyses
Analyses were conducted for each of the four techniques (n-BCA using a Prowler microcatheter, EVOH with “plug and push”, EVOH with a detachable-tip microcatheter, and EVOH with a balloon microcatheter) considering embolization of one to four pedicles per bAVM per patient (Table 2 and Figure 2). Overall, costs for the n-BCA technique were lower than all three EVOH techniques for all analyses when comparing costs per procedure (one to four pedicles), and for the low or high-volume annual cohorts. Total per procedure costs for one to four embolized pedicles ranged from $5941 to $10,074 for the n-BCA technique, $8428 to $30,345 for the EVOH balloon microcatheter technique, $12,711 to $47,477 for the EVOH plug and push technique, and $13,900 to $52,233 for the EVOH detachable-tip microcatheter technique. Embolizing AVMs with multiple pedicles was associated with increased cost for the LES in all EVOH techniques given that additional kits were required for each pedicle. In contrast, costs for LES were static for the n-BCA technique since a single n-BCA kit provided adequate volume for multiple pedicles. Per procedure costs for the three EVOH techniques ranged from 1.42 to 5.18 times greater than the cost of the n-BCA technique (when comparing procedures with the same number of pedicles embolized), indicating that substantial cost savings may be associated with using n-BCA for bAVM embolization rather than EVOH when considering cost of devices and angiography suite time.
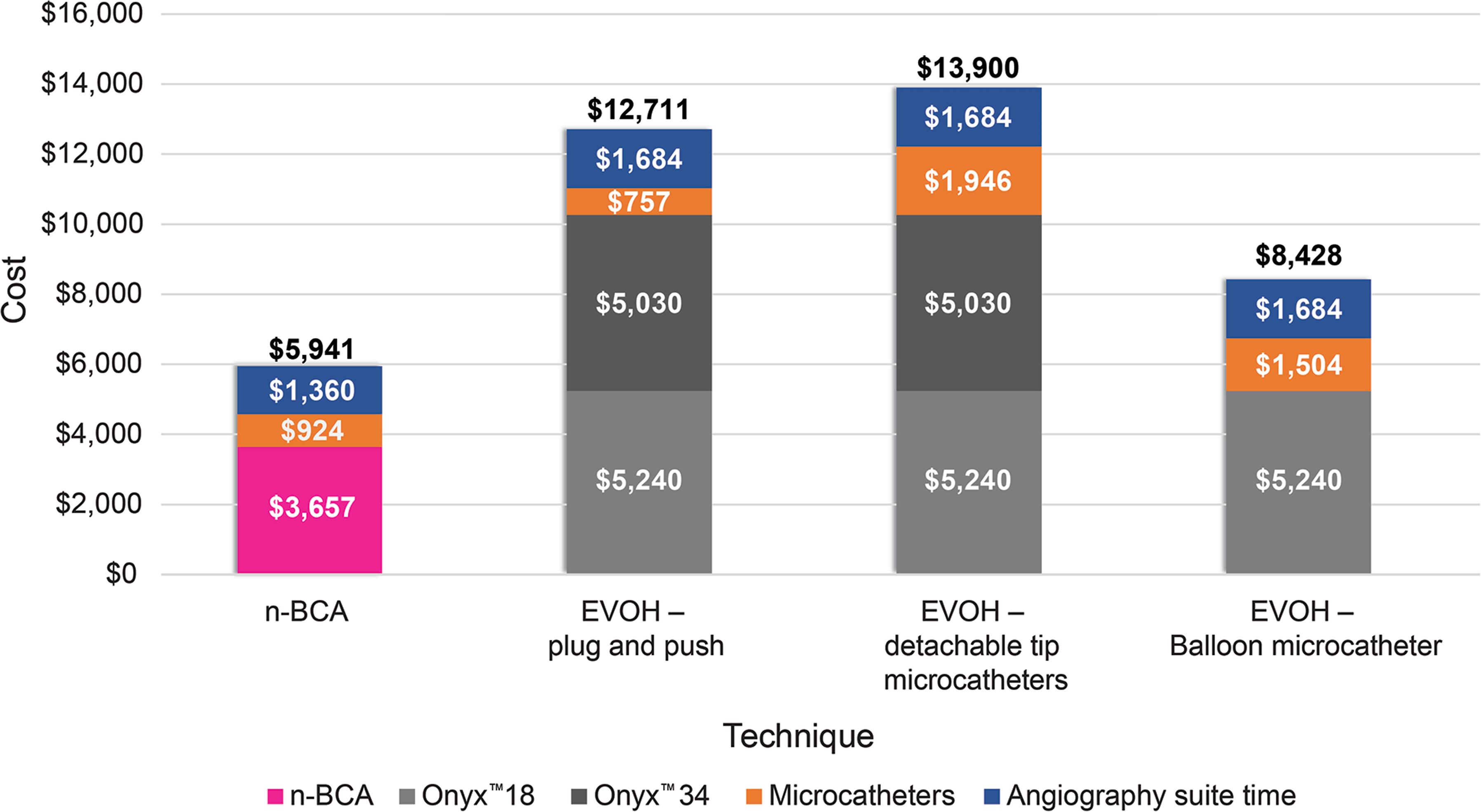
Cost per procedure for the four embolization techniques. Per procedure costs for LES, microcatheters, and angiography suite time for each of the four treatments analyzed for the embolization of bAVMs with one pedicle. Abbreviations: EVOH: ethylene vinyl alcohol copolymer; LES: liquid embolic system n-BCA: n-butyl cyanoacrylate.
Cost analysis results by technique and number of pedicles embolized.
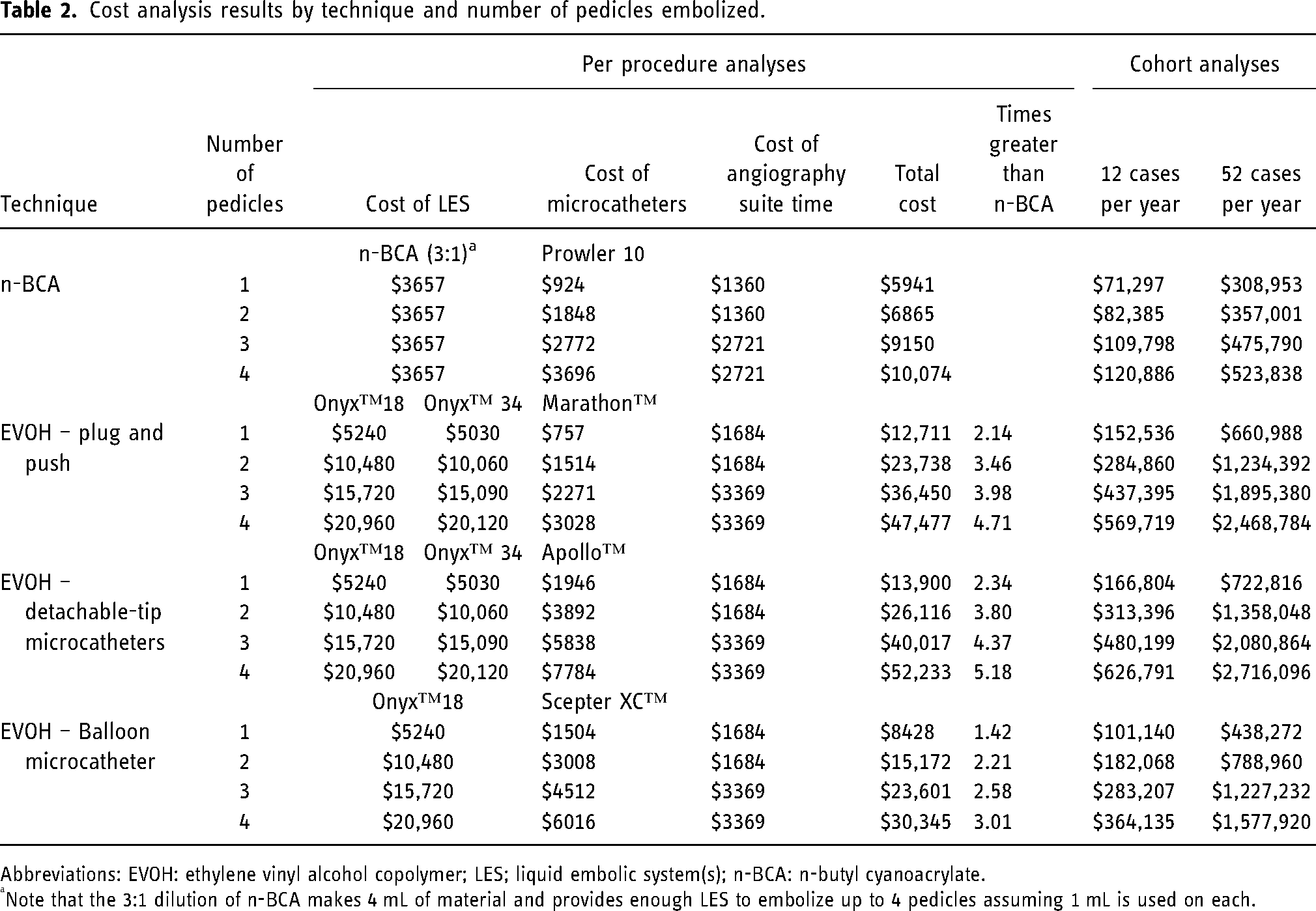
Abbreviations: EVOH: ethylene vinyl alcohol copolymer; LES; liquid embolic system(s); n-BCA: n-butyl cyanoacrylate.
Note that the 3:1 dilution of n-BCA makes 4 mL of material and provides enough LES to embolize up to 4 pedicles assuming 1 mL is used on each.
Cohort analyses showed that the estimated annual costs of treating twelve bAVM cases per year ranged from $71,297 to $120,886 with the n-BCA technique (1 to 4 pedicles each) and costs ranged from $166,804 to $626,791 with the EVOH detachable-tip microcatheter technique (one to four pedicles each). Costs for treating fifty-two cases per year ranged from $308,953 to $523,838 with n-BCA (one to four pedicles each) and from $722,816 to $2,716,096 with EVOH detachable-tip microcatheters (one to four pedicles each; see Table 2). For both per procedure and annual cohort analyses, additional costs for EVOH procedures compared to n-BCA were driven by higher total costs for all the LES kits and use of additional and/or specialized microcatheters required to embolize bAVMs. This was because more LES kits were required per pedicle with EVOH techniques compared to the n-BCA technique. Angiography suite costs were also higher with EVOH techniques because they required additional time to perform embolization procedures compared to n-BCA, although were not a major driver of cost differences.
Sensitivity analysis results
Sensitivity analyses were performed to examine the effects of varying categories of input costs by ±20% and using alternate assumptions for the duration of procedure time with the different EVOH techniques (Table S1). Varying the angiography suite costs (hours or cost/hour) by ±20% had the smallest impact on per procedure results, followed by varying the microcatheter costs by ±20%, while varying the LES costs by ±20% had the largest impact on the results. The category cost sensitivity analyses were consistent with the primary analysis and the ranking of techniques from least to most expensive was the same for each analysis performed compared to the primary analysis.
Discussion
The results from the economic analysis show that embolization with the 3:1 mixture of n-BCA was consistently the most cost efficient across all analyses of the four embolization techniques examined. The total annual procedure costs for the low-volume cohort (12 cases per year) ranged from $71,297 to $120,886 with n-BCA and $166,804 to $626,791 with EVOH detachable-tip microcatheters for one to four pedicles, with potential cost savings with n-BCA ranging from $95,507 to $505,906 annually. The total annual procedure costs for the high-volume cohort analyses (52 cases per year) ranged from $308,953 to $523,838 with n-BCA and $722,816 to $2,716,096 with EVOH plug and push for one to four pedicles, with potential cost savings with n-BCA ranging from $413,863 to $2,192,258 annually. The order of techniques from least to most expensive was n-BCA, followed by EVOH with balloon microcatheters, then EVOH using plug and push, and EVOH with detachable-tip microcatheters. The sensitivity analysis results were consistent with the primary analysis as the ranking of the techniques from least to most expensive was consistent, and the cost of LES was a key driver. These results, which leverage the hospital resource use reported by previous clinical studies,9,12,13 highlight the cost implications when considering which embolization technique to use for bAVM devascularization.
In addition to the differences in procedure time that were reported by Velat et al. (2.1 h vs. 2.6 h, p < 0.0001), n-BCA procedures required significantly shorter fluoroscopy time compared to EVOH procedures (37 vs. 57 min, p < 0.0001). 12 Extended procedure duration is associated with significantly more (14%, p < 0.001) complications for every additional 30 min of procedure time. 22 Fluoroscopy time should be minimized if possible to avoid the complications associated with radiation exposure including erythema, cataracts, hair loss and alopecia, as well as skin burns. 23 Radiation exposure has relevance for patients given direct radiation of the brain tissue, especially for young patients in active brain development, as well as for clinicians given repeated exposures. The cost analyses presented here demonstrate substantial costs associated with longer procedure time, however, the cost of complications or hospital stay were outside the scope of the analysis. Future clinical studies should examine resource use related to complications and length of stay for n-BCA and EVOH to inform such analyses.
Comparisons between n-BCA and EVOH for presurgical bAVM devascularization in the literature have focused on intermediate efficacy outcomes such as percentage of patients with complete nidal occlusion24–27 or bAVM volume reduction.9,12,13 These outcomes are not the primary goal of bAVM presurgical devascularization, but have been used as endpoints to compare the technical differences between n-BCA and Onyx. 9 Since the degree of occlusion has not been shown to correlate with the ease of bAVM surgical removal or the likelihood of bAVMs to exhibit an intraoperative hemorrhage, the comparative value of these intermediate endpoints is limited. Ideally studies would examine the rates of hemorrhage during surgical removal of the bAVMs to provide evidence for which LES is more efficacious at preventing hemorrhage, however, studies reporting such comparisons were not identified by a literature review.
In the absence of comparative effectiveness data, it is important to consider the complications associated with the different LESs. Although catheter retention rates were higher with EVOH than n-BCA (9.3% vs. 1.6%) in an RCT comparing the two LESs, a statistical comparison was not reported. 9 Thus, future studies powered to detect differences in complications should examine catheter retention risks. The detachable tip microcatheter and balloon microcatheter techniques were included in this analysis because they may help to reduce retention of the entire catheter and EVOH reflux leading to embolization of non-target vessels. An observational study of 23 patients with bAVMs embolized with EVOH using the detachable-tip microcatheter technique showed no instances of catheter retention. 14 Additionally, an observational study of various neurointerventional procedures (including 13 bAVM embolizations) in 37 patients using balloon microcatheters documented no cases of catheter retention or entrapment or associated thromboembolic complications. 15 To synthesize, microcatheters designed to reduce catheter retention and prevent EVOH reflux may help avoid these complications, but they are associated with additional costs compared with ancillary devices used with techniques such as n-BCA. In selecting an LES technique, total procedure costs should be considered rather than LES unit costs alone due to the uniqueness of the procedure and dependency on ancillary devices.
Strengths and limitations
The key strengths of this analysis are that inputs were from published sources including comparative clinical studies and that resource use and technical considerations were validated by neurointerventionalists experienced with both n-BCA and EVOH techniques. Another strength was that analyses were performed to calculate the costs for one to four pedicles to ensure applicability to most clinical bAVM presentations. Finally, sensitivity analyses were performed to address input cost and parameter uncertainty to support the main analyses presented.
Several simplifying assumptions had to be made to facilitate the cost analysis. We assumed that all techniques examined would be equally suitable to embolize a hypothetical bAVM pedicle. In clinical practice, bAVM characteristics such as flow rate and volume of the nidus may make one technique preferable. However, fixed conditions were assumed in these analyses to enable more direct cost comparison. Since procedure duration was not available for all EVOH techniques and procedure time for EVOH from Velat et al. did not specify the technique for EVOH embolization, we assumed equal procedure time for all EVOH techniques. To address this limitation, sensitivity analyses were performed examining varied procedure duration for the different EVOH techniques. Additionally, it was assumed that only one type of LES would be used per AVM, but it is possible to use n-BCA and EVOH in a complementary manner, which could be examined in future analyses. Another limitation was the impact of performing staged embolization procedures. Larger bAVMs may require treatment in multiple sessions, however, there were no published data specifying the percentage of patients who required staging by LES type, so this variable was not included. While we are not able to provide an analysis at the patient level, the reader can leverage Table 2 to estimate the costs associated with multiple sessions in addition to treating multiple pedicles.
Conclusion
This analysis evaluates the cost consequences of the two leading LES products and estimates that procedure costs associated with n-BCA are lower than each of the three EVOH techniques examined. Comparative clinical data and retrospective database analysis on bAVM embolization are limited by the low prevalence of bAVM. In the future, new LES options are expected to enter the market and additional cost comparison analyses should be performed to evaluate all available options.
Footnotes
Author contributions
All authors contributed to developing the study concept. EK obtained the funding and supervised the study. GW and HC performed the analyses. GW and HC drafted the article and SS, EK, and AK revised it critically for important intellectual content. All authors approved the version to be published and take public responsibility for the content.
Conflict of interest
SS is a paid consultant for Balt, CERENOVUS, Q Apel, Stryker, Terumo, Cordis, and Penumbra. EK and AK are employees of CERENOVUS which provided the funding for this study. GW and HC are employees of EVERSANA which was contracted by CERENOVUS to perform the analyses and prepare the manuscript.
Ethical approval
Since this study did not enroll any subjects it was exempted from ethics approval.
Funding
Funding for this study was provided by CERENOVUS, a Johnson & Johnson Medical Devices company.