
Abstract
Background
Mechanical thrombectomy (MT) is the gold standard treatment for large vessel occlusion (LVO). A vital factor that might influence MT outcomes is the use of intravenous thrombolysis (IVT). A few clinical trials in this domain thus far have not yielded consistent outcomes. We conducted this meta-analysis to synthesize collective evidence in this regard.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement guidelines were followed, and we performed a comprehensive literature search of four databases (PubMed, Scopus, Web of Science, Cochrane CENTRAL). For outcomes constituting continuous data, the mean difference (MD) and its standard deviation (SD) were pooled. For outcomes constituting dichotomous data, the frequency of events and the total number of patients were pooled as the risk ratio (RR).
Results
Seven clinical trials with a total of 2317 patients are included in this meta-analysis. Six trials are randomized, and one trial was nonrandomized. No significant differences were found between MT plus IVT and MT alone in successful recanalization (RR 1.04, 95% Confidence Interval (CI) [0.92 to 1.17], P = 0.53), 90-day functional independence (RR 1.03, 95% CI [0.90 to 1.19], P = 0.65), symptomatic intracranial hemorrhage (sICH) (RR 1.22, 95% CI [0.84 to 1.75], P = 0.30), or mortality (RR 0.94, 95% CI [0.76 to 1.18], P = 0.61).
Conclusion
The current evidence does not favor either MT plus IVT or MT alone for LVO except for the procedural time. More trials are needed in this regard, and certain factors should be considered when comparing the two approaches.
Introduction
Mechanical thrombectomy (MT) has become the gold standard for the management of acute ischemic stroke (AIS) caused by large vessel occlusion (LVO).1,2 However, there are many factors that are being studied, either in the clinical trial setting or via observational studies, to determine their impact on the procedural and clinical outcomes of MT in AIS-LVO patients. Amongst these factors, the use of intravenous thrombolysis (IVT) in combination with MT has been a very crucial question that many studies attempted to answer.3–11 Such studies assessed the outcomes of bridging IVT plus MT in terms of the procedural outcomes as well as clinical ones. Nonetheless, there was no solid agreement among the results of these studies.
The current guidelines by the American Stroke Association recommend that patients with AIS-LVO, who meet the eligibility criteria of both IVT and MT, can receive both treatment modalities. 12 The concept of using IVT with MT in eligible AIS-LVO patients stems from the potential of softening the thrombus which might ultimately facilitate the MT procedure and help achieve faster recanalization.13,14 However, there is a counterargument that such a lytic effect of IVT is somewhat limited when it comes to a large thrombus causing LVO. Moreover, partial fragmentation of the target thrombus by IVT might also facilitate distal migration of microemboli which could ultimately worsen the outcomes of the MT procedure.15,16 Furthermore, IVT might be associated with increased risk of hemorrhage. 17
With the availability of multiple clinical trials comparing bridging IVT plus MT to MT alone, and the results of these trials being mixed and sometimes contradictory, we conducted this systematic review and meta-analysis to provide comprehensive evidence regarding the benefits and safety of IVT in combination with MT from both clinical and procedural standpoints.
Methods
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement guidelines for this systematic review and meta-analysis. 18 The methods were done in strict accordance with the Cochrane Handbook of Systematic Reviews and Meta-analysis of Interventions (version 5.1.0). The study protocol was registered at PROSPERO database; ID CRD42022365950, https://www.crd.york.ac.uk/prospero/export_details_pdf.php.
Eligibility criteria
We included all studies satisfying the following criteria:
Population: Studies on patients with AIS. Intervention: Studies where the experimental group received IVT and MT. Comparator: Studies where the control group received MT alone. Outcome: We included studies reporting at least one of the following outcomes: mortality rate, successful recanalization, complete recanalization, favorable modified Rankin Scale (mRS) score at 90 days, National Institute of Health Stroke Scale (NIHSS) score at 24 h after the stroke event and/or at discharge from the hospital, onset-to-groin time, door-to-puncture time, and complications. Study design: Clinical trials comparing the outcomes of MT alone with IVT plus MT.
We excluded observational studies, articles that were not in English, and studies on either MT alone or MT combined with IVT without direct comparison between both arms.
Literature search
We performed a comprehensive literature search of four electronic databases (PubMed, Scopus, Web of Science, and Cochrane CENTRAL) from inception until 11 August 2022 using this search query (“Mechanical thrombectomy” OR “Endovascular thrombectomy”) AND (“Intravenous thrombolysis” OR “Alteplase”) AND (“Acute Ischemic Stroke” OR “AIS”). All duplicates were removed, and all references of the included studies were screened manually for any eligible studies.
Screening of the literature search results
Retrieved results from the literature search were screened in two steps. In the first step, the title and abstracts of all articles were screened for eligibility. Then, the full-text articles of eligible abstracts were retrieved and screened for eligibility.
Data extraction
Data were extracted to a uniform data extraction sheet. The extracted data included (1) characteristics of the included studies, (2) characteristics of the population of included studies, (3) risk of bias domains, and (4) outcome measures.
Outcome measures
In the present meta-analysis, we considered the following outcome measures: 1) mortality, 2) successful recanalization: defined as the proportion of patients with Thrombolysis in Cerebral Infarction (TICI) grades 2b-3, 3) complete recanalization: defined as the proportion of patients with TICI grade 3, 4) functional independence or favorable functional outcome: defined as achieving mRS score of 0–2 at 90 days, 5) NIHSS score change from baseline, 6) symptomatic intracranial hemorrhage (sICH), 7) any intracranial hemorrhage, 8) onset-to-groin time (in minutes): defined as the time from onset of stroke to groin puncture, 9) door-to-puncture time (in minutes): defined as the time from hospital arrival to groin puncture, and 10) puncture-to-recanalization time (in minutes): defined as the time from groin puncture to recanalization of the occluded vessel. Measures 1-4 and 6-7 are represented as the risk ratio (RR) between the two groups, while measures 5 and 8-10 are represented as the mean difference (MD) between the two study groups from baseline to endpoint.
Synthesis of results
For outcomes that constitute continuous data, MD between the two groups from the baseline to the endpoint along with the standard deviation (SD), were pooled in the DerSimonian-Laird random-effect model. In the case of studies reporting data in multiple time points, we considered the last endpoint for the primary analysis. For outcomes that constitute dichotomous data, the frequency of events and the total number of patients in each group were pooled as RR between the two groups in the DerSimonian-Laird random-effect model. All statistical analyses were done by Review Manager software Stata/MP version 17 for Microsoft Windows.
Heterogeneity assessment
Statistical heterogeneity among studies was evaluated by the Chi-square test (Cochrane Q test). Then, the chi-square statistic, Cochrane Q, was used to calculate the I-squared according to the equation: I2 =
Risk of bias across studies
Two authors independently assessed the quality of included clinical trials in strict accordance with the Cochrane handbook of systematic reviews of interventions. 19 Any discrepancies between the two assessors were resolved through discussion and including a third assessor.
Certainty assessment
We conducted a certainty assessment through sensitivity analysis (also called leave-one-out meta-analysis) to test the robustness of the available evidence. For every outcome in the meta-analysis, we ran sensitivity analysis in multiple scenarios, excluding one study in each scenario to make sure the overall effect size was not dependent on any single study.
Results
Literature search results and study selection
Our literature search process retrieved 2821 records. Following titles and abstract screening, 89 articles were eligible for full-text screening. From these 89 studies, seven studies were included in the meta-analysis. The references of the included studies were also manually searched, and no further articles were included. The flow chart of the study selection process is shown in the PRISMA flow diagram (Figure 1).
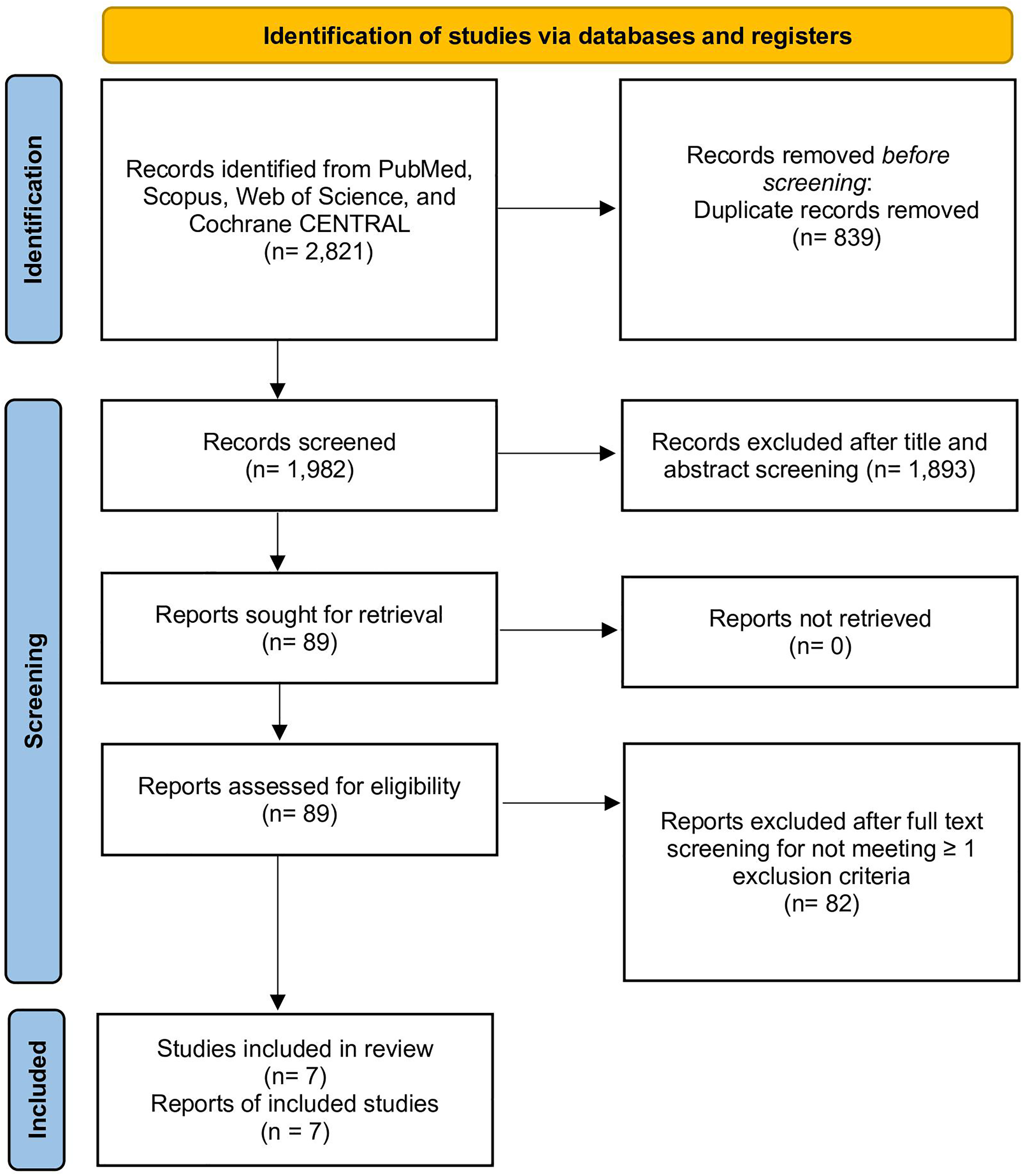
PRISMA flow diagram showing the process of study selection.
Study characteristics
The population of the studies was homogenous; all studies enrolled a cumulative of 2317 patients with AIS undergoing MT. All included studies were clinical trials. The characteristics of the included studies are summarized in Table 1, while summary and baseline characteristics of populations of these studies are shown in Table 2.
Summary of the included studies.
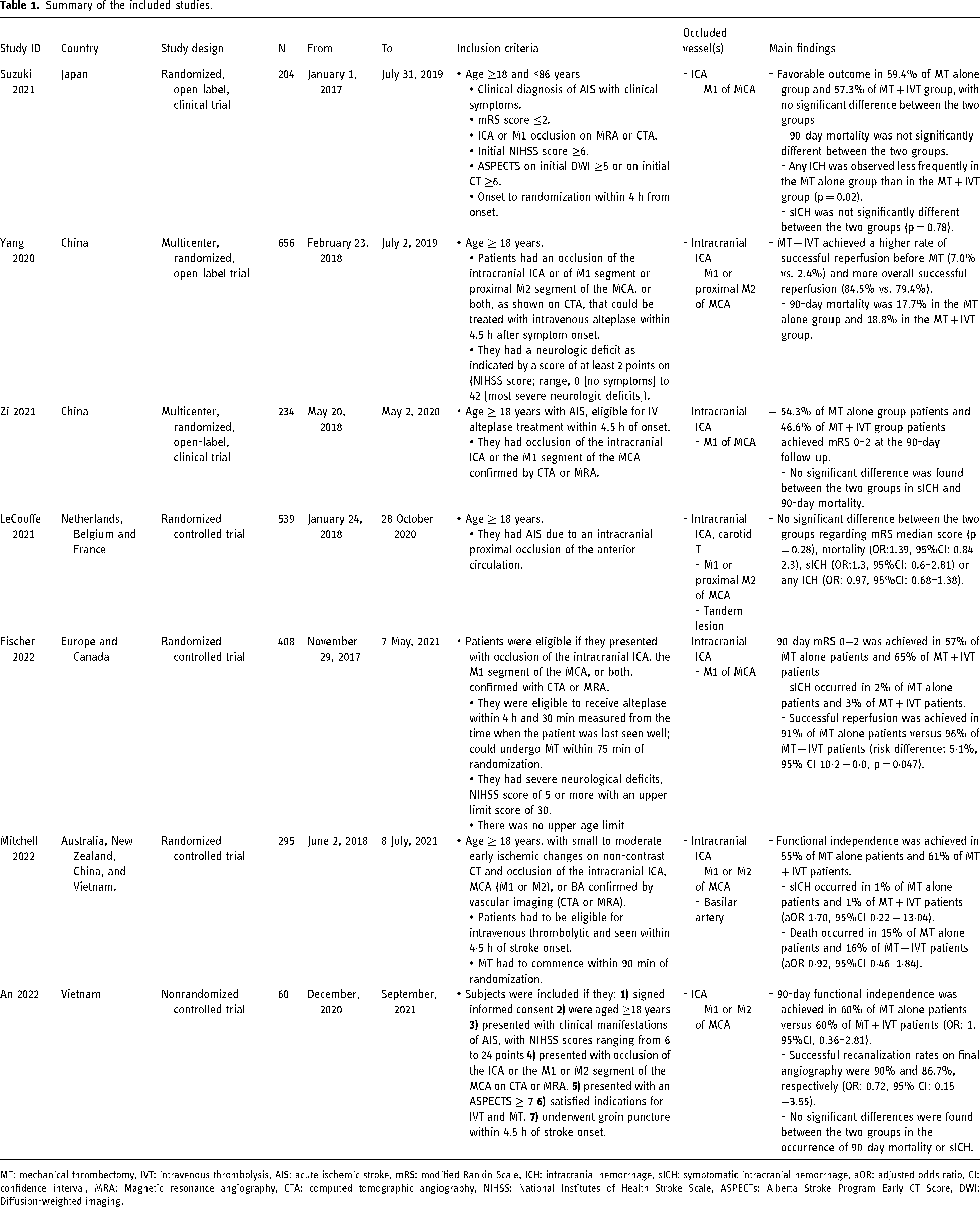
MT: mechanical thrombectomy, IVT: intravenous thrombolysis, AIS: acute ischemic stroke, mRS: modified Rankin Scale, ICH: intracranial hemorrhage, sICH: symptomatic intracranial hemorrhage, aOR: adjusted odds ratio, CI: confidence interval, MRA: Magnetic resonance angiography, CTA: computed tomographic angiography, NIHSS: National Institutes of Health Stroke Scale, ASPECTs: Alberta Stroke Program Early CT Score, DWI: Diffusion-weighted imaging.
Baseline characteristics of the included studies’ populations.
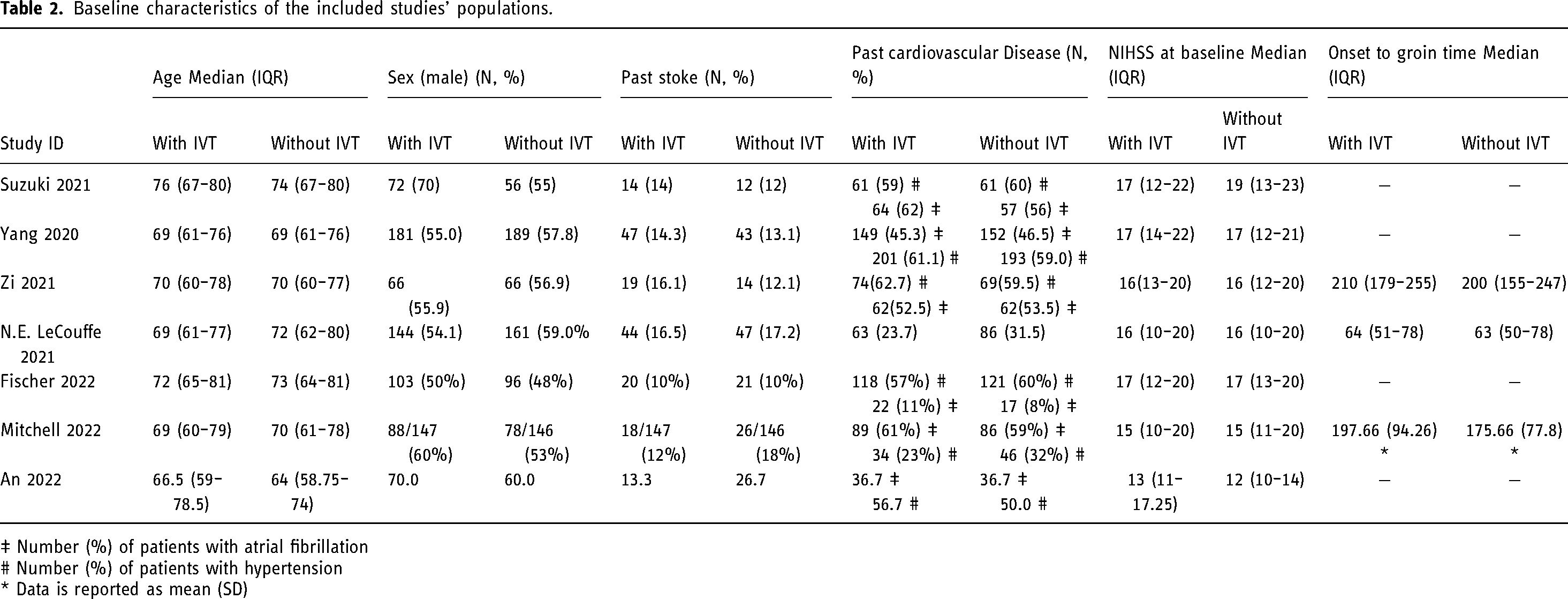
‡ Number (%) of patients with atrial fibrillation
# Number (%) of patients with hypertension
* Data is reported as mean (SD)
Risk of bias within studies
Two authors independently assessed the quality of included trials in strict accordance with the Risk of Bias Assessment tool-2 (ROB2) for randomized controlled trials19,20 and Risk of Bias in Non-randomized Studies - of Interventions tool (ROBINS-I) for non-randomized trials. 21 Any discrepancies between the two assessors were resolved through discussion and including a third assessor.
In ROB2 (five domains):
Six trials reported an appropriate method of random sequence generation either by a web-based system using permuted blocks, central telephone systems, or computer-generated random sequence. However, four of the six studies reported no information about the allocation concealment and were judged as having some concerns. The other two studies reported inability to achieve allocation concealment and judged as high risk. No significant baseline difference was detected in those six studies.
Six trials were open-label trials, and five of them reported an appropriate analysis method to estimate the effect of assignment to intervention (intention-to-treat or modified intention-to-treat principles). Only Suzuki 2021 study reported inappropriate analysis method (per-protocol analysis) to estimate the effect of assignment to intervention.
Two of those six studies reported nearly complete outcome data while four trials (LeCouffe 2021, Fischer 2022, Yang 2020, and Suzuki 202) reported incomplete or missing outcome data with justifications including participants withdrawal and loss of follow-up. There was evidence that the result was not biased by missing outcome data in the form of applying an appropriate analysis method that corrects for bias.
Six trials showed an appropriate outcome measurement. Moreover, blinding of the outcome assessors was observed in all the studies, where independent clinical event committees who were unaware of the group allocation were responsible for the adjudication of the primary outcomes.
In all those six studies, results were reported according to a pre-specified analysis plan and/or registered protocol. Further details and overall judgements are shown in the supplementary material.
In ROBINS-i
One trial was assessed by the ROBINS-I tool which is Ann 2022 study. The quality of this trial was high, and it was comparable to a well performed randomized trial according to ROBINS-I tool.
Successful and complete recanalization
The pooled analysis of the successful recanalization reported by seven studies (n = 2292 patients) did not favor either of the two groups (RR 1.04, 95% CI [0.92 to 1.17], P = 0.53, Figure 2 (A)). The pooled studies were homogenous (P = 1.00; I2 = 0%).
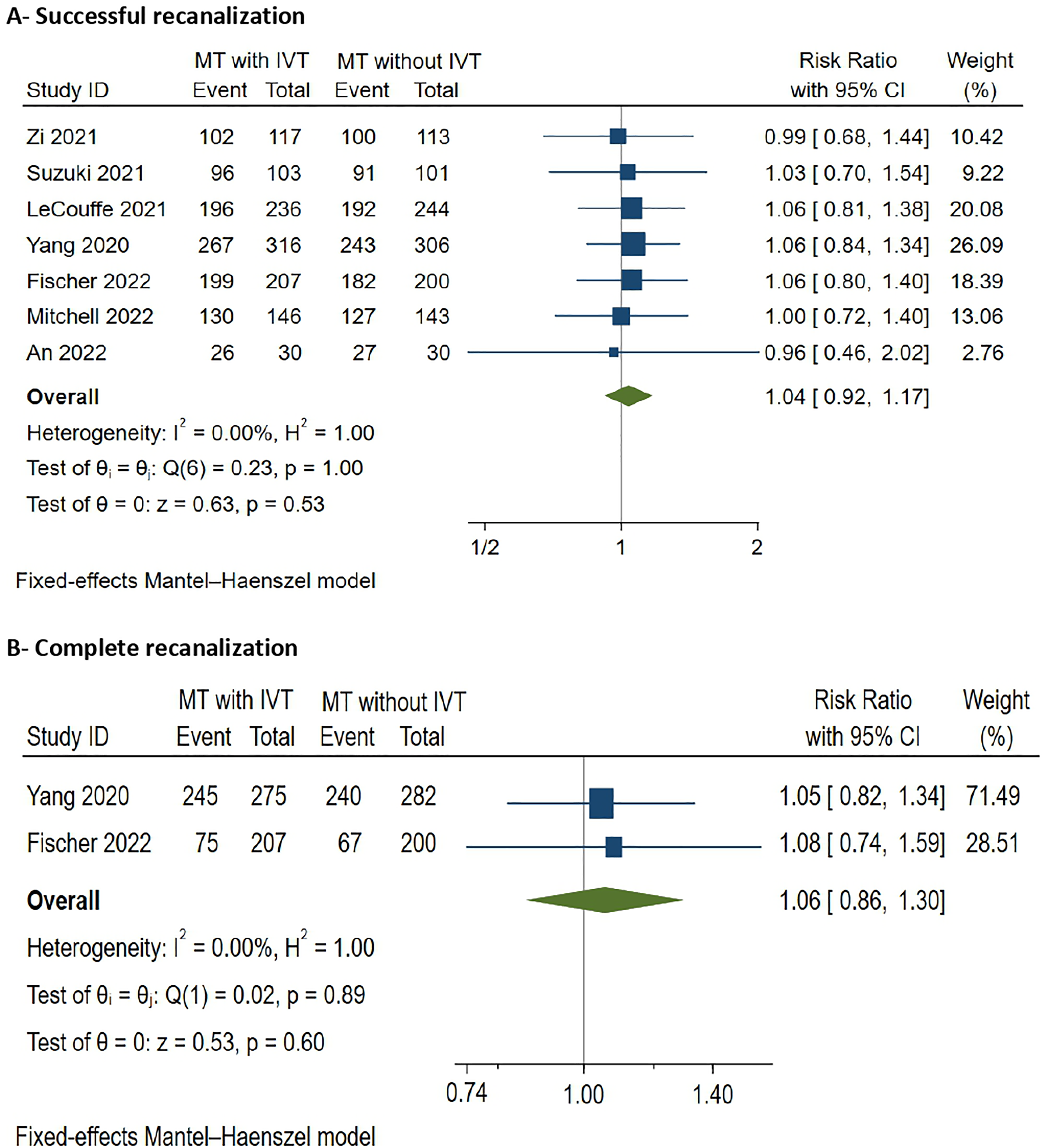
Recanalization outcomes.
The pooled analysis of the complete recanalization reported by two studies (n = 964 patients) did not favor either of the two groups (RR 1.06, 95% CI [0.86 to 1.30], P = 0.60, Figure 2(B)). The pooled studies were homogenous (P = 0.60; I2 = 0%).
Improvement in NIHSS score
The overall standardized mean difference (SMD) of improvement in the NIHSS score from baseline did not favor either group (SMD −0.01, 95% CI [−0.08 to 0.06]). Subgroup analysis, according to the time point at which the NIHSS score improvement was assessed, did not show any difference between the two groups either at 24 h reported by four studies (n = 1836) (SMD −0.001, 95% CI [−0.10 to 0.09]) or at discharge reported by four studies (n = 1712) (SMD −0.01, 95% CI [−0.13 to 0.11], Figure 3(A)). The pooled studies were homogenous (P = 0.35, I2 = 9.85%).
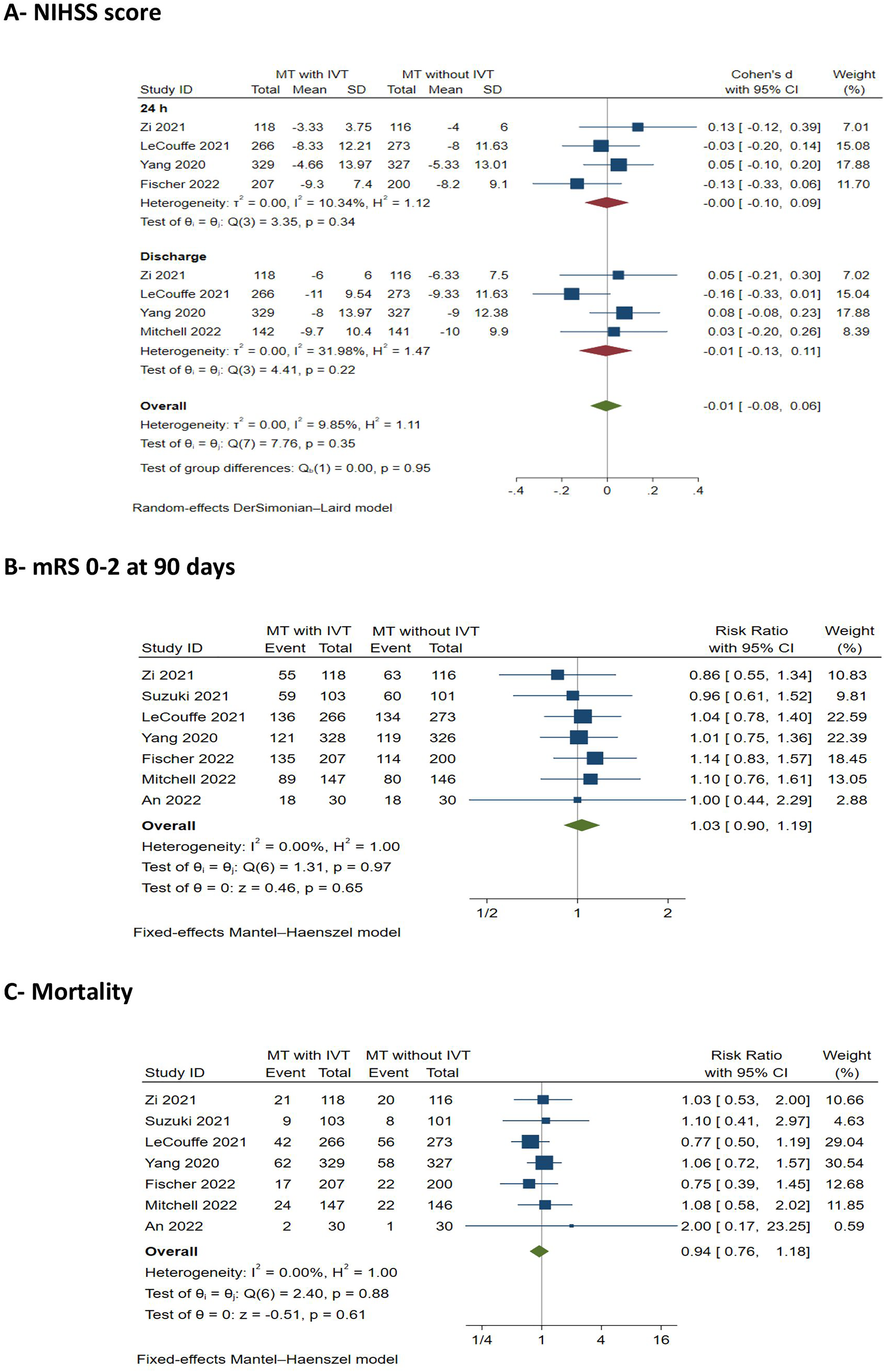
Clinical outcomes.
Favorable functional outcome (functional independence)
The pooled analysis of the favorable functional outcome according to the mRS score (ranging from 0 to 2) at 90 days was reported by seven studies (n = 2391 patients) did not favor either of the two groups (RR 1.03, 95% CI [0.90 to 1.19], P = 0.65, Figure 3 (B)). The pooled studies were homogenous (P = 0.97; I2 = 0%).
Mortality
The pooled analysis of the mortality reported by seven studies (n = 2393 patients) did not favor either of the two groups (RR 0.94, 95% CI [0.76 to 1.18], P = 0.61, Figure 3 (C)). The pooled studies were homogenous (P = 0.88; I2 = 0%).
Complications
Symptomatic intracranial hemorrhage
The pooled analysis of the sICH reported by seven studies (n = 2385 patients) did not favour either of the two groups (RR 1.22, 95% CI [0.84 to 1.75], P = 0.30, Figure 4 (A)). The pooled studies were homogenous (P = 0.93; I2 = 0%).
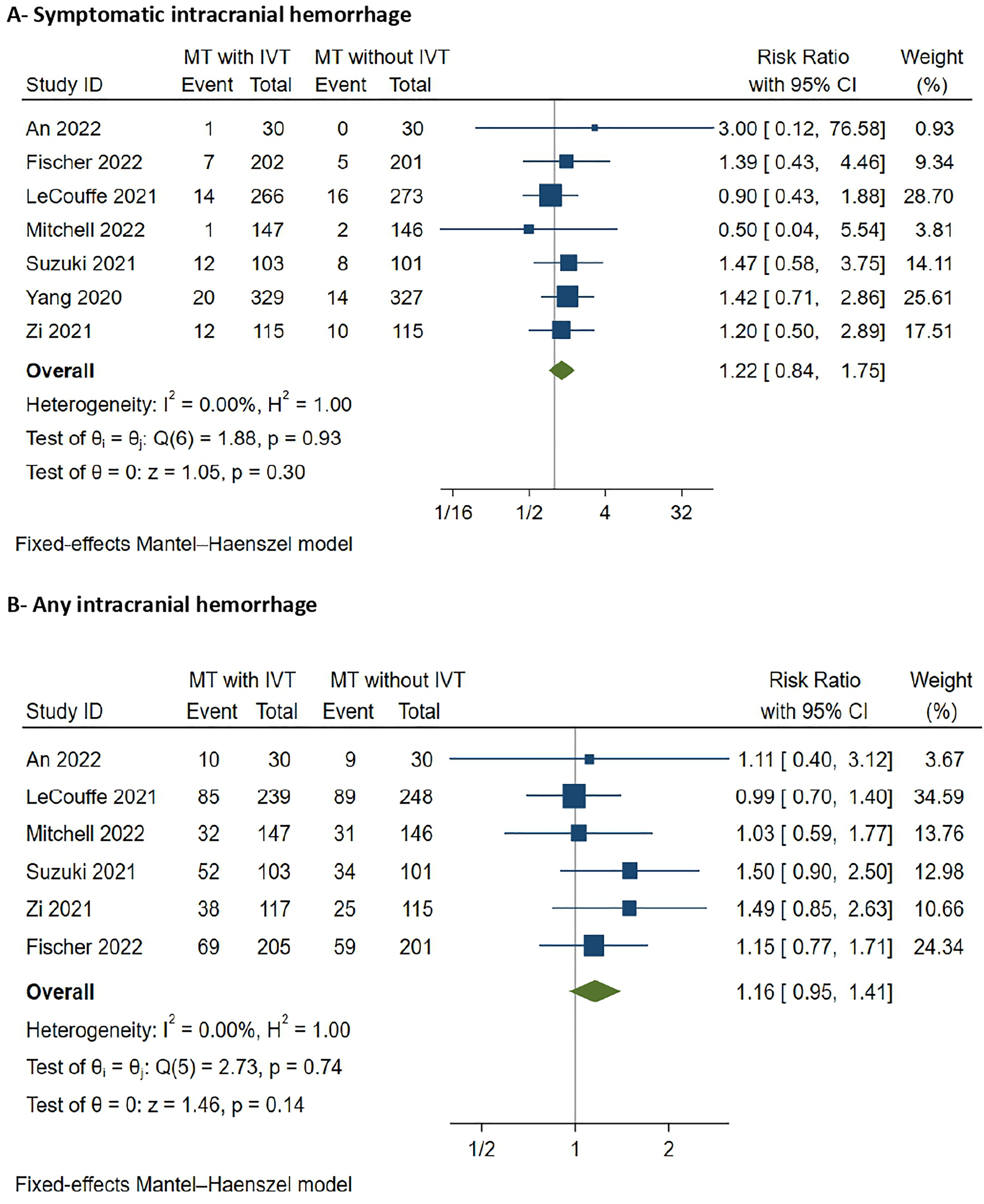
Hemorrhagic outcomes.
Any intracranial hemorrhage
The pooled analysis of the any intracranial haemorrhage reported by six studies (n = 1682 patients) did not favour either of the two groups (RR 1.16, 95% CI [0.95 to 1.41], P = 0.14, Figure 4 (B)). The pooled studies were homogenous (P = 0.74; I2 = 0%).
Time metrics
Onset-to-groin time
The overall MD of the onset-to-groin time reported by five studies (n = 1882 patients) favored MT alone over the bridging group (MD 1.12 min, 95% CI [0.02 to 0.22], P = 0.0.1, Figure 5 (A)). The pooled studies were homogenous (P = 0.34; I2 = 0%).
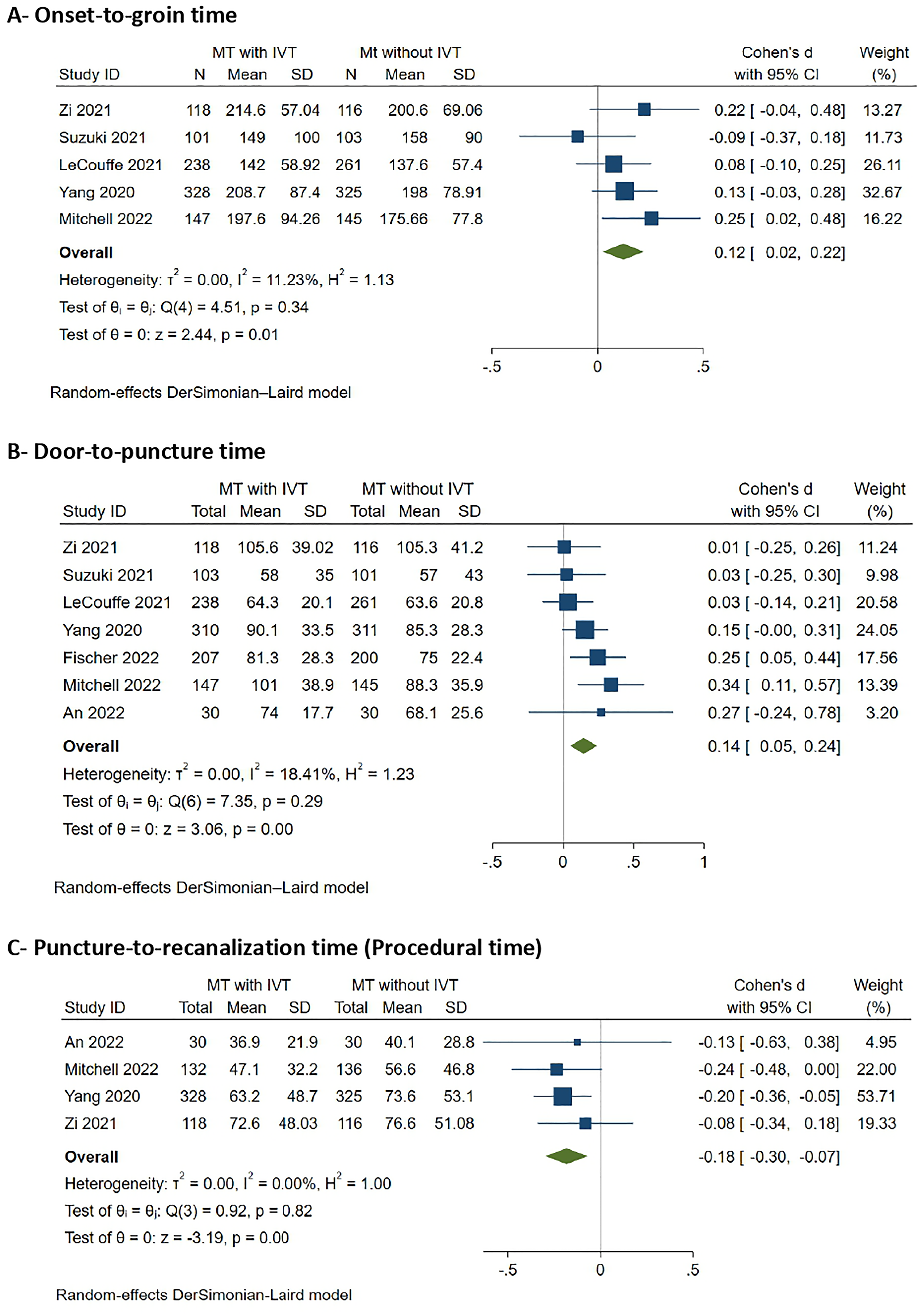
Time metrics.
Door-to-puncture time
The overall MD of the door-to-puncture time reported by seven studies (n = 2317 patients) favored MT alone over the bridging group (MD 0.14 min, 95% CI [0.05 to 0.24], P < 0.001). The pooled studies were homogenous (P = 0.85; I2 = 0% Figure 5 (B)). The pooled studies were homogenous (P = 0.29; I2 = 0%).
Puncture-to-recanalization time (procedural time)
The overall MD of the procedural time reported by three studies (n = 981 patients) was shorter in the bridging group compared with MT alone (MD −0.18 min, 95% CI [10.30 to −0.07], P < 0.001 Figure 5 (C)). The pooled studies were homogenous (P = 0.92; I2 = 0%).
Discussion
Our meta-analysis, which included 7 clinical trials, reveals that there were no significant differences between MT plus IVT and MT alone in terms of achieving successful or complete recanalization, achieving functional independence as represented by the 90-day mRS score, mortality, improvement of the NIHSS score either at 24 h or at discharge, and complications including sICH, or any intracranial hemorrhage. Regarding the time metrics, onset-to-groin and door-to-puncture times were significantly longer in the MT plus IVT group than in the MT alone group. However, puncture-to-recanalization time was significantly shorter in the MT plus IVT group than in the MT alone group.
As previously mentioned, there is debate regarding the use of IVT in combination with MT versus MT alone in eligible AIS-LVO patients. On one hand, IVT is suggested to facilitate the MT procedure by dissolving the thrombus and making it more susceptible to extraction by MT. 3 In a study by Shehabeldin and colleagues, 22 IVT was found to be associated with fewer number of passes required to achieve successful or complete recanalization, which might be reflected as reduced procedural time. A longer procedural time was found to be associated with lower chances of achieving functional independence, and higher rates of complications such as sICH. 23 On the other hand, the counter debate against the use of IVT plus MT relies theoretically on the increased risk of hemorrhage. 17 Additionally, while it is suggested that IVT might dissolve the obstructing thrombus and ultimately facilitate the MT procedure, 14 this dissolution of the thrombus might paradoxically complicate the MT procedure by increasing the chances of distal microembolism.15,16
While our meta-analysis did not show significant differences between the two approaches either in terms of clinical outcomes or in terms of safety profile and complications, it highlights a few factors which might influence the impact of IVT on MT. For instance, it is important to understand whether the MT technique can alter the impact of IVT on the outcomes of the MT procedure. In this regard, a post-hoc analysis from the COMPASS trial compared the outcomes of each of the two MT techniques (stent retriever (SR) technique and aspiration technique) when used alone versus when combined with IVT. The only significant difference was found between aspiration MT plus IVT and aspiration MT alone as the latter was associated with a higher rate of successful reperfusion, 100% versus 87.9% (p = 0.03). No significant differences were noticed in the rest of the procedural, angiographic, and clinical outcomes. 24 On the contrary, a post-hoc analysis from MR CLEAN-NO IV trial showed that among patients who underwent aspiration MT, MT alone was associated with worse functional outcome when compared to aspiration MT plus IVT (adjusted common odds ratio (OR), 0.44 [95% CI, 0.21–0.90]), with no other statistically significant differences in clinical or procedural outcomes. 25
Another factor to consider when evaluating the benefits and safety of combined MT and IVT approach is the presence or absence of tandem occlusion in patients undergoing MT. With tandem occlusion, carotid artery stenting (CAS) is known to be beneficial with an acceptable safety profile, 26 with early antiplatelet therapy in the perioperative period being standard. 27 Theoretically, there might be an increased risk of ICH in those patients if they received IVT based on the results of the study by Zinkstok and colleagues 28 showing increased risk of sICH in patients receiving aspirin within 90 min after the start of IVT, yet MT was not done in patients included in this trial. In this regard, a few cohort studies investigated the benefits and safety of IVT in patients with tandem occlusions undergoing MT. The results of these studies indicated significant benefits of IVT in terms of favorable clinical outcome and/or mortality, without increased risk of sICH.29–32 Amongst the trials we included in this meta-analysis, only the trial conducted by An and colleagues 6 looked at the safety of IVT in patients requiring acute stenting with no significant difference between IVT and no IVT in those patients.
The growing use of tenecteplase as the first-line thrombolytic agents in many stroke centers, brings to question whether tenecteplase behaves differently when used as a bridging thrombolytic agent with MT. EXTEND-IA TNK trial compared tenecteplase plus MT with alteplase plus MT. The primary outcome was defined as reperfusion of >50% of the involved ischemic territory or absence of a retrievable thrombus at the time of the initial angiographic assessment, and the secondary outcomes were the 90-mRS score and sICH. The results favored tenecteplase plus MT approach in terms of the primary outcome (incidence difference: 12 percentage points; 95% CI, 2 to 21; incidence ratio, 2.2; 95% CI, 1.1 to 4.4; p = 0.002 for noninferiority; p = 0.03 for superiority), and the 90-day mRS score (median mRS score 2 versus 3; OR, 1.7; 95% CI, 1.0 to 2.8; p = 0.04). On the other hand, there was no difference between the two approaches in terms of sICH. 33 EXTEND-IA TNK Part 2 trial compared two different doses of tenecteplase (0.40 mg/kg versus 0.25 mg/kg) in combination with MT, and the results did not favor either of the two doses in terms of reperfusion of >50% of the involved ischemic territory prior to MT, the level of disability according to the 90-day mRS score, substantial neurological improvement at 3 days, sICH within 36 h, and all-cause mortality. 34 Note that when it comes to tenecteplase as a bridging thrombolytic agent, there is no data available in the clinical trial setting regarding the comparison between tenecteplase plus MT versus MT alone.
Lastly, we should note that most of the trials that investigated IVT plus MT versus MT alone included patients with LVO within the anterior circulation,5–7,9–11 and only the trial by Mitchell and colleagues 8 included patients with LVO within either the anterior or the posterior circulation. Within the anterior circulation itself, according to a pre-specified subgroup analysis of the data from the DIRECT-MT trial, the occlusion site did not have any impact on the comparison between MT plus IVT and MT alone in terms of successful recanalization, functional outcome, and sICH. 35 Regarding AIS within the posterior circulation, a recent meta-analysis has found that bridging IVT in patients with basilar artery occlusion (BAO) was associated with a lower 90-day mortality rate without increasing the risk of sICH or subarachnoid hemorrhage. This study reported no difference in the functional outcome between IVT plus MT and MT alone except in patients with large artery atherosclerosis who achieved better functional outcomes with bridging IVT. 36 With the encouraging results of the ATTENTION and the BAOCHE trials in terms of the benefits of MT in patients with BAO,37,38 future trials comparing MT plus IVT versus MT alone might need to include patients with BAO. Also, studies comparing the outcome of the MT plus IVT approach between anterior circulation LVO versus BAO might help drawing a conclusion whether the impact of IVT varies according to the LVO location in the anterior or posterior circulation.
All things considered, the question of whether IVT combined with MT is superior to MT alone cannot be answered only with studies comparing the procedural, angiographic, and clinical outcomes between the two approaches. Future clinical trials need to include multivariate analyses to investigate the impact of the LVO location and MT technique on the outcome of combined MT and IVT. Moreover, further clinical trials are needed to compare alteplase with tenecteplase in combination with MT, and to compare tenecteplase plus MT with MT alone.
Strengths and limitations
There are a few previously published meta-analyses that compared MT plus IVT and MT alone.39–41 To our knowledge, this is the largest and most updated meta-analysis of clinical trials comparing MT plus IVT to MT alone in patients with AIS-LVO. We have compared the two approaches in as many aspects as possible given the data available in the included trials. However, we were unable to perform subgroup analyses based on the MT technique, acute stenting in patients with tandem occlusions, type of the thrombolytic agent used, or the location of the LVO.
Conclusion
Our meta-analysis compared MT plus IVT versus MT alone and did not favor either of the two approaches with regard to clinical and procedural outcomes. Regarding the time metrics, puncture-to-recanalization time was found to be shorter with the MT plus IVT approach, while onset-to-groin and door-to-puncture times were significantly longer in this group. We highlight certain factors that need further research to understand their potential influence on the combined IVT and MT approach as compared to MT alone. These factors include the technique used for MT, the type of the thrombolytic agent, the need for acute carotid stenting, and the location of the LVO.
Supplemental Material
sj-docx-1-ine-10.1177_15910199221140276 - Supplemental material for Intravenous thrombolysis plus mechanical thrombectomy versus mechanical thrombectomy alone for acute ischemic stroke: A systematic review and updated meta-analysis of clinical trials
Supplemental material, sj-docx-1-ine-10.1177_15910199221140276 for Intravenous thrombolysis plus mechanical thrombectomy versus mechanical thrombectomy alone for acute ischemic stroke: A systematic review and updated meta-analysis of clinical trials by Mohamed Elfil, Hazem S Ghaith, Hanaa Elsayed, Mohammad Aladawi, Ahmed Elmashad, Neisha Patel, Chaitanya Medicherla, Mohammad El-Ghanem, Krishna Amuluru and Fawaz Al-Mufti in Interventional Neuroradiology
Supplemental Material
sj-docx-2-ine-10.1177_15910199221140276 - Supplemental material for Intravenous thrombolysis plus mechanical thrombectomy versus mechanical thrombectomy alone for acute ischemic stroke: A systematic review and updated meta-analysis of clinical trials
Supplemental material, sj-docx-2-ine-10.1177_15910199221140276 for Intravenous thrombolysis plus mechanical thrombectomy versus mechanical thrombectomy alone for acute ischemic stroke: A systematic review and updated meta-analysis of clinical trials by Mohamed Elfil, Hazem S Ghaith, Hanaa Elsayed, Mohammad Aladawi, Ahmed Elmashad, Neisha Patel, Chaitanya Medicherla, Mohammad El-Ghanem, Krishna Amuluru and Fawaz Al-Mufti in Interventional Neuroradiology
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.