
Abstract
Background
Digital subtraction angiography (DSA) is most commonly used in vessel disease examinations and treatments. We aimed to develop a novel deep learning-based method to deblur the large focal spot DSA images, so as to obtain a clearer and sharper cerebrovascular DSA image.
Methods
The proposed network cascaded several residual dense blocks (RDBs), which contain dense connected layers and local residual learning. Several loss functions for image restoration were investigated. Our training set consisted of 52 paired images of angiography with more than 350,000 cropped patches. The testing set included 10 body phantoms and 80 clinical images of different types of diseases for subjective evaluation. All test images were acquired using a large focal spot, and phantom images were simultaneously acquired using a micro focal spot as ground-truth. Peak-to-noise ratio (PSNR) and structural similarity (SSIM) were determined for quantitative analysis. The deblurring results were compared with the original data, and the image quality was subjectively evaluated and graded by two clinicians.
Results
For quantitative analysis of phantom images, the average PSNR/SSIM based on the deep-learning approach (35.34/0.9566) was better than that of large focal spot images (30.64/0.9163). For subjective evaluation of 80 clinical patient images, image quality in all types of cerebrovascular diseases was also improved based on a deep-learning approach (p < 0.001).
Conclusions
Deep learning-based focal spot deblur algorithm can efficiently improve DSA image quality for better visualization of blood vessels and lesions in the image.
Introduction
Digital subtraction angiography (DSA) is most commonly used in cerebrovascular disease examinations and treatments and is also the gold standard for diagnosing the disease. 1 The image quality of DSA can affect the diagnosis and treatment strategies of neurointerventionalists or neurosurgeons, so it is very important to ensure the clarity of DSA images. Meanwhile, more disease-related features should be found on DSA images.
One of the key factors affecting DSA image quality is the tube focal spot, which should be as small as possible to produce sharp images, in order to observe subtle vessels and fine structures. However, due to the tube power limit, in many cases, a large focal spot has to be used to achieve a sufficient dose by sacrificing the image sharpness. 2 We aimed to develop a novel deep learning-based method to deblur the large focal spot DSA images.
Methods
Overall architecture
Our architecture was inspired by the residual dense network (RDN) that achieved favorable performance against state-of-the-art methods of single super-resolution. 3 We expanded the hierarchical feature extraction in the low resolution (LR) space of RDN to achieve a deblurring function. The proposed deblurring network is illustrated below (Figure 1). An attention module is added after the dense feature fusion of several residual dense blocks (RDBs). This development can enable the network to focus on learning informative features. The input of the deblurring neural network is low-resolution image, and the output is the deblurred image with the same dimension as the input image (Figure 1(a)).
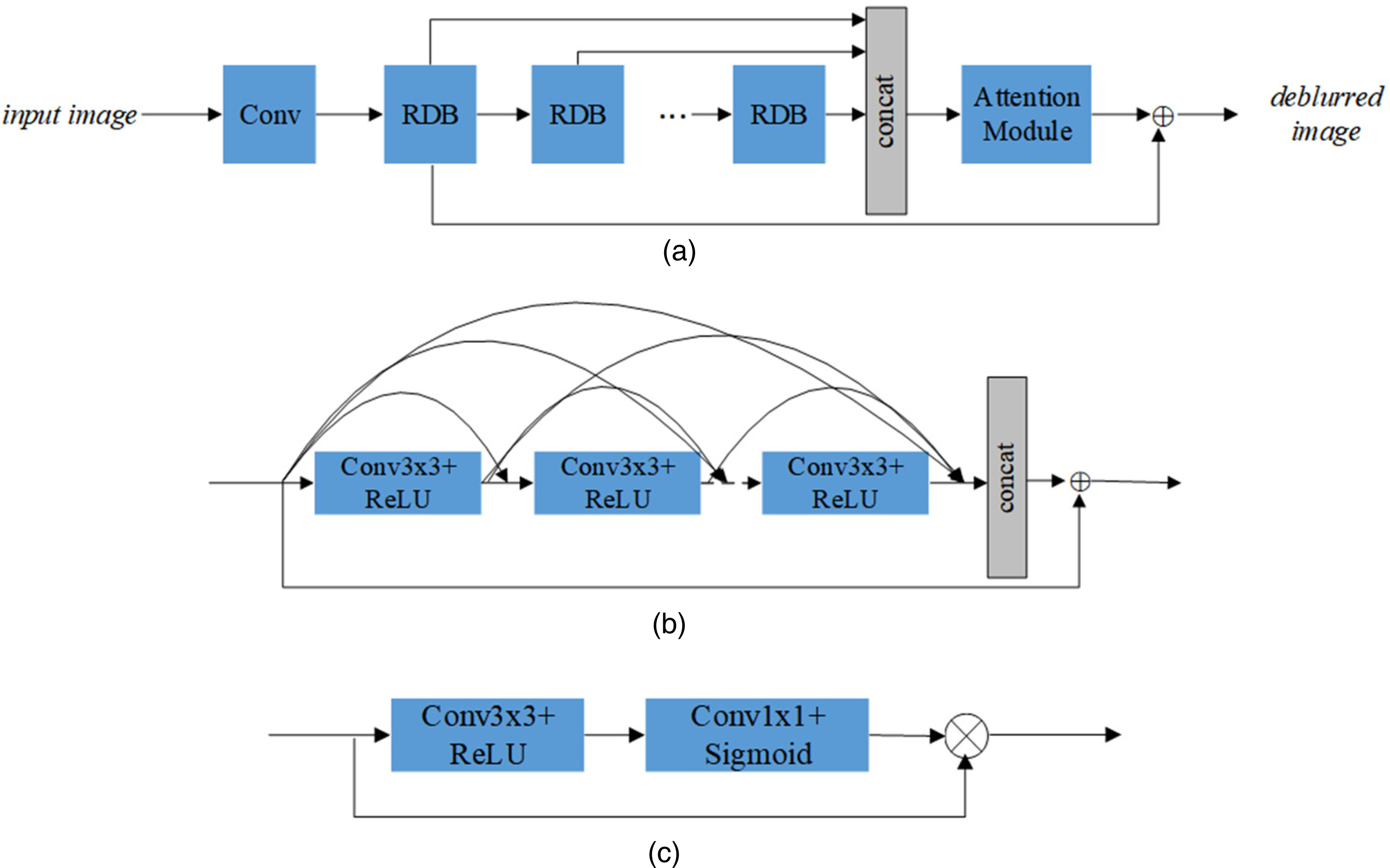
The architecture of deblurring network. (a) The overview design of the deblurring network, (b) structure of residual dense block (RDB) and (c) the structure of the attention module.
RDB structure
Herein, we exploited RDB connected in RDN. This structure contains dense connected layers and local residual learning, leading to a contiguous memory mechanism.
3
Before feeding into RDBs, one convolutional layer
Attention module
After the concatenation of dense features generated from RDBs, the channel attention module is exploited for more informative features extraction (Figure 1(c)). The first convolutional layer with kernel size 3 × 3 and rectified linear unit (ReLU) activation is utilized to reduce dimension, then the following layer whose kernel size is 1 × 1 is used to recover dimension with the same as input dimension so as to conduct the element-wise product. The output of the last layer with sigmoid activation represents the weight coefficients of each channel, which can be used for channel attention.
Multi-loss supervision
Several loss functions for image restoration have been investigated, such as

Training set
It is known that the size of the focal spot affects the amount of image blurring in all radiological imaging. 7 Therefore, we established more real-world datasets for angiography. It is impractical to collect the training images of the paired large–small focal spots in a clinic, so we established the dataset with the phantom simulation of the human body. Thus, paired blurred-distinct images on the same scene are captured by adjusting the focal spot of angiography in order to replace synthetic blurriness. In this case, the only distinction of scanned conditions for paired images is the size of the focal spot and the other settings stay the same.
We trained our deblurring model with 52 paired images of angiography, resulting in more than 350,000 cropped patches, whose size is 40 × 40 with stride 20. Furthermore, we used another 10 validation angiographic images in the training process. In our experiments, the mini-batch size was 128. We trained for 50 epochs. The network was optimized using the Adam algorithm with a learning rate of 10-4 for the first 30 epochs and 10-5 for the last 20 epochs. The network training and testing was implemented in Python with the Tensorflow library on an NVIDIA Titan Xp GPU.
Quantitative validation by peak-to-noise ratio/structural similarity (PSNR/SSIM)
The performance of the proposed method is compared with that of the original data in terms of peak-to-noise ratio (PSNR) and structural similarity (SSIM). The PSNR is widely used for quantitative evaluation of image restoration quality, and SSIM is related to the perceptual quality. 8 Higher PSNR and SSIM represent the better performance of image quality. Since the calculation of PSNR and SSIM require distinct images scanned by small focal spot, it is difficult to get ground truth for clinical images. So we took the quantitative assessment on self-collected phantom images scanned by adjusting the focal spot. An anthropomorphic whole-body phantom, PH-2B CT (PBU-60) (Kyoto Kagaku, Kyoto, Japan), with and without a neoprene suit. The density of the simulated soft tissue of the phantom was 1.061 g/cm3, with a relative electron density of 0.975. The weight was 50 kg and the length was 165 cm. The phantom included relevant organs such as a lung cavity and a synthetic skeleton. 9 Ten angiographic images using this phantom were randomly selected from our DSA database, and we compared their PSNR(dB)/SSIM between the traditional large focal spots and our proposed deblurring technique.
Physician feedback
We evaluate our proposed method with three types of hemorrhagic cerebrospinal vascular disease that are common in a clinic, including aneurysm (AN), arteriovenous malformation (AVM), spinal arteriovenous malformation (SAVM) and cerebrovascular stenosis. DSA was performed in several angiographic systems, including AlluraXper of Philips Medical Systems, ARTIS of Siemens, TERRA of GE Medical Systems, and NeuAngio30C of Neusoft Medical Systems.
Between January 2021 and May 2021, we randomly selected 80 cases for deblur technique processing, including 20 ANs, 20 AVMs, 20 SAVMs and 20 cerebrovascular stenosis cases. Their images were deblurred by our proposed method. The study was approved by the ethics committee of our hospital. Informed consent was obtained from all individual participants included in the study.
Blind scoring on those images was performed by two physicians whose experiences in cerebrovascular diseases were more than 10 years. The scoring standard is based on the comparison between the original DSA image and its deblurred version processed by our method, and is presented as follows: Level 3 represents equivalent performance in comparison. Level 4 and Level 5 show that deblurred image has better performance than the original DSA image, and is especially helpful for treatment in Level 5. Level 2 and Level 1 indicate that the original DSA image has better performance and especially the deblurred image has a negative influence on treatment in Level 1.
Statistical analysis
Descriptive analysis was used in PSNR/SSIM validation part. In the physician scoring part, for each physician from every type of disease, the Mann–Whitney U-test was conducted on the score distribution. The middle score (level 3) for each type of disease was used as the null hypothesis. All statistical steps were performed with SPSS version 26.0 (IBM, NY, USA). A p-value < 0.05 was considered as statistically significant.
Results
Validation results
Table 1 shows the average PSNR and SSIM results on 10 randomly selected angiographic images of a phantom. We used the performance of data with a large focal spot as a reference, PSNR of the proposed method could have a gain of about 4.7 dB, and SSIM could outperform the reference by about 0.04, which shows the same trend with PSNR. The average PSNR/SSIM based on the deep-learning approach (35.34/0.9566) was better than that of large focal spot images (30.64/0.9163). Briefly, our proposed method could achieve better image quality.
Comparison of proposed deblurring neural network with reference on PSNR(dB)/SSIM.
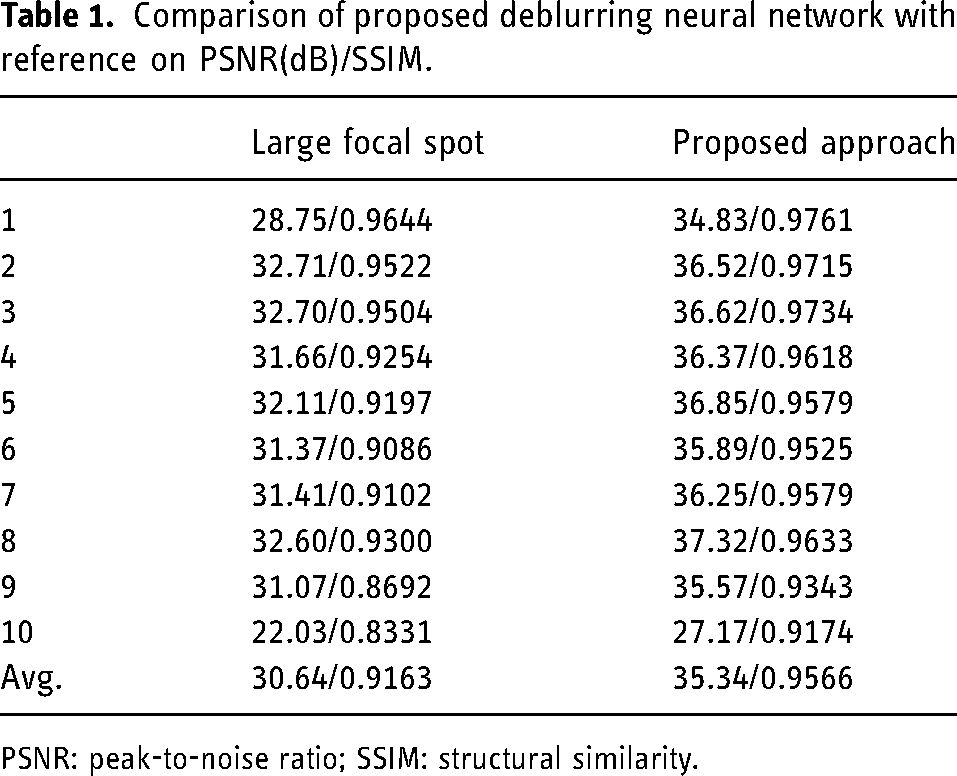
PSNR: peak-to-noise ratio; SSIM: structural similarity.
Physician feedback results
For AN, 85% and 100% of the cases were scored in levels 4 and 5 by two physicians, respectively, indicating that the proposed method has obvious advantages over the original DSA image. For 50% of the cases, one physician considered that the proposed method was helpful for treatment in a clinic (Table 2).
Summary of responses from physician feedback and calculated p-value for various types of disease.
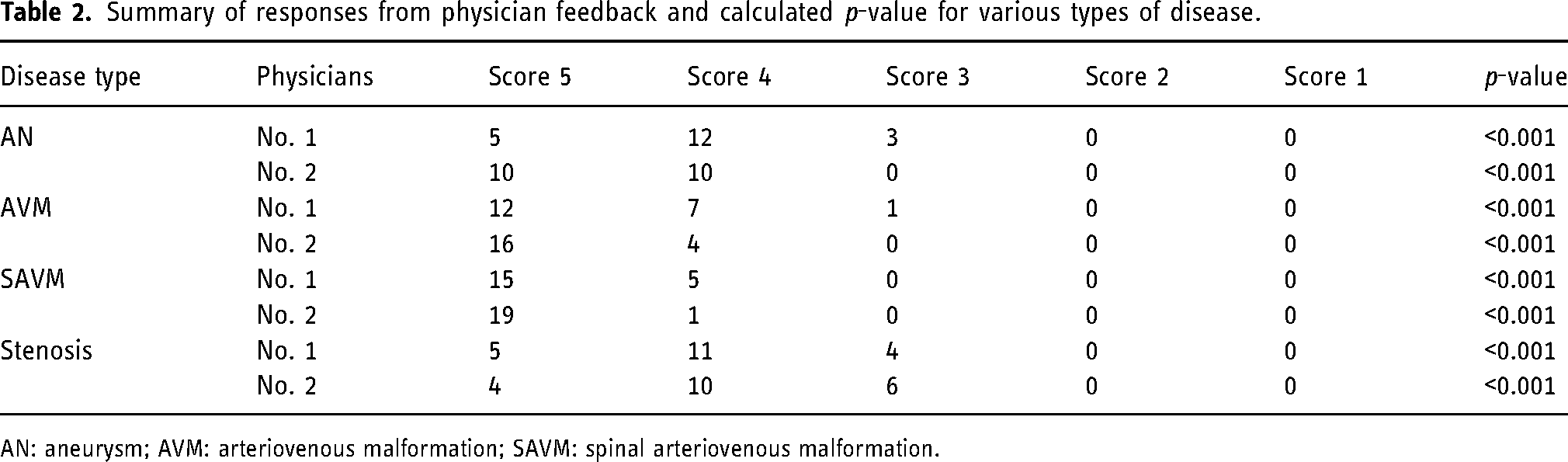
AN: aneurysm; AVM: arteriovenous malformation; SAVM: spinal arteriovenous malformation.
For almost 100% of the cases, two physicians concluded that the performance of deblurred images processed by our proposed method was significantly improved by scoring in levels 4 and 5 in terms of AVM and SAVM. Two physicians thought that our proposed method was helpful for treatment in more than 50% of the above cases (Table 2).
There were eight carotid artery stenosis cases (including one occlusion case), eight intracranial artery stenosis cases (including four occlusion cases) and four vertebral artery stenosis cases in the cerebrovascular stenosis group. Sixteen cases were determined to be level 4 or level 5 by one of the physicians, while the other physician thought 14 cases meet the definition of level 4 and level 5 (Table 2).
In terms of each type of disease, a p-value < 0.001 was calculated for each physician (Table 2).
Case illustration
We have selected an AVM and a SAVM case to show here, demonstrating that the deblur model optimized images are clearer and sharper, and optimally responded to vessel morphology. Meanwhile, it can also provide more information on the AVM vascular structure than conventional large-focus imaging in the ultra-early phase of the image (as illustrated in Figures 2 and 3).
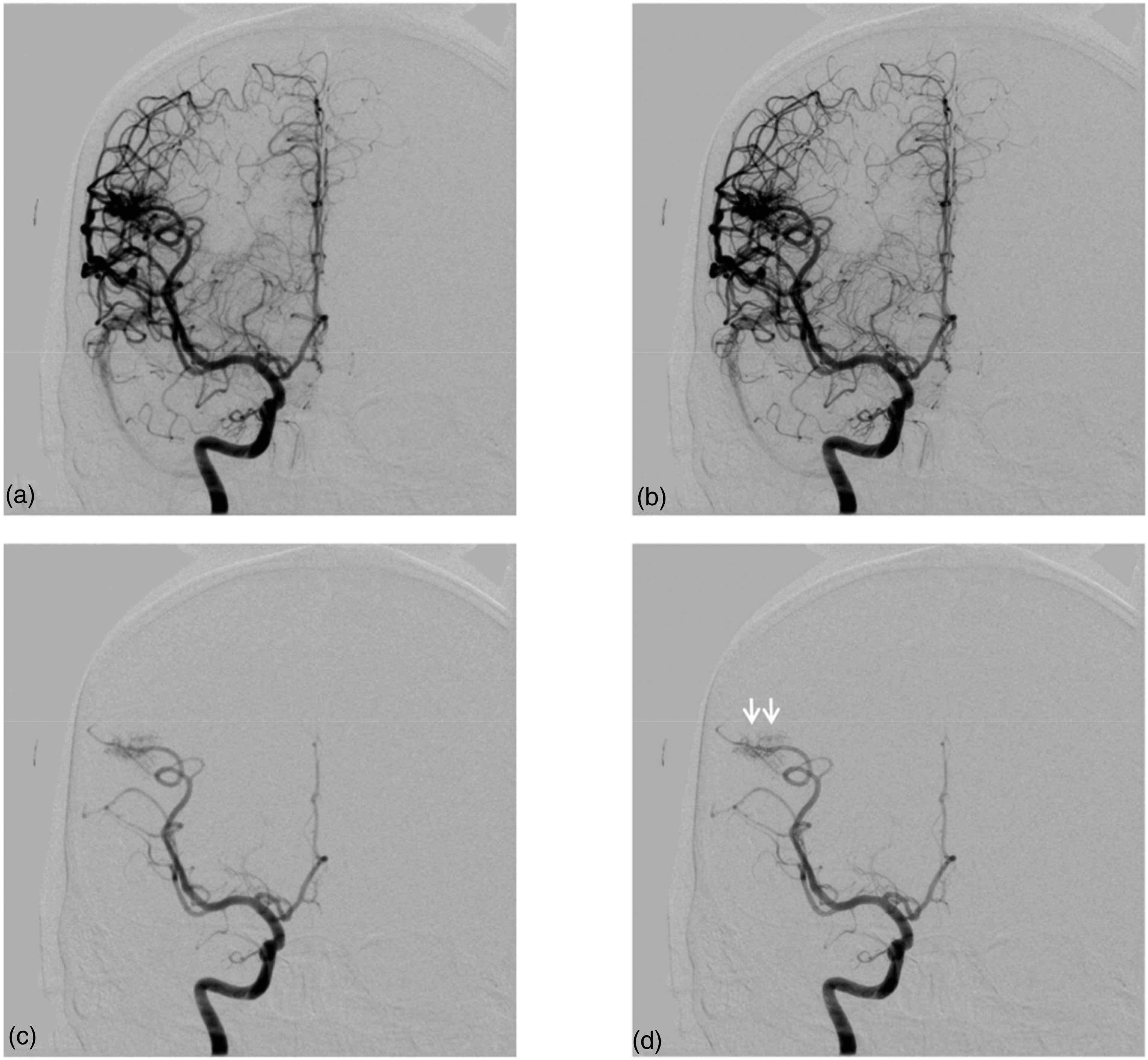
A case of a right frontal arteriovenous malformation (AVM): (a) shows cerebral angiographic imaging in the large focal spot situation, while (b) displays the image after deblur post-processing, in which the vessels appear sharper, the image has less background noise, and the overall vessels and nidus are clearer. (c) and (d) show arterial early stage, and the two tiny branches supplying the AVM are better defined by the deblur post-processed image (d, white arrows), which helps the physician to make a better pre-operative plan.
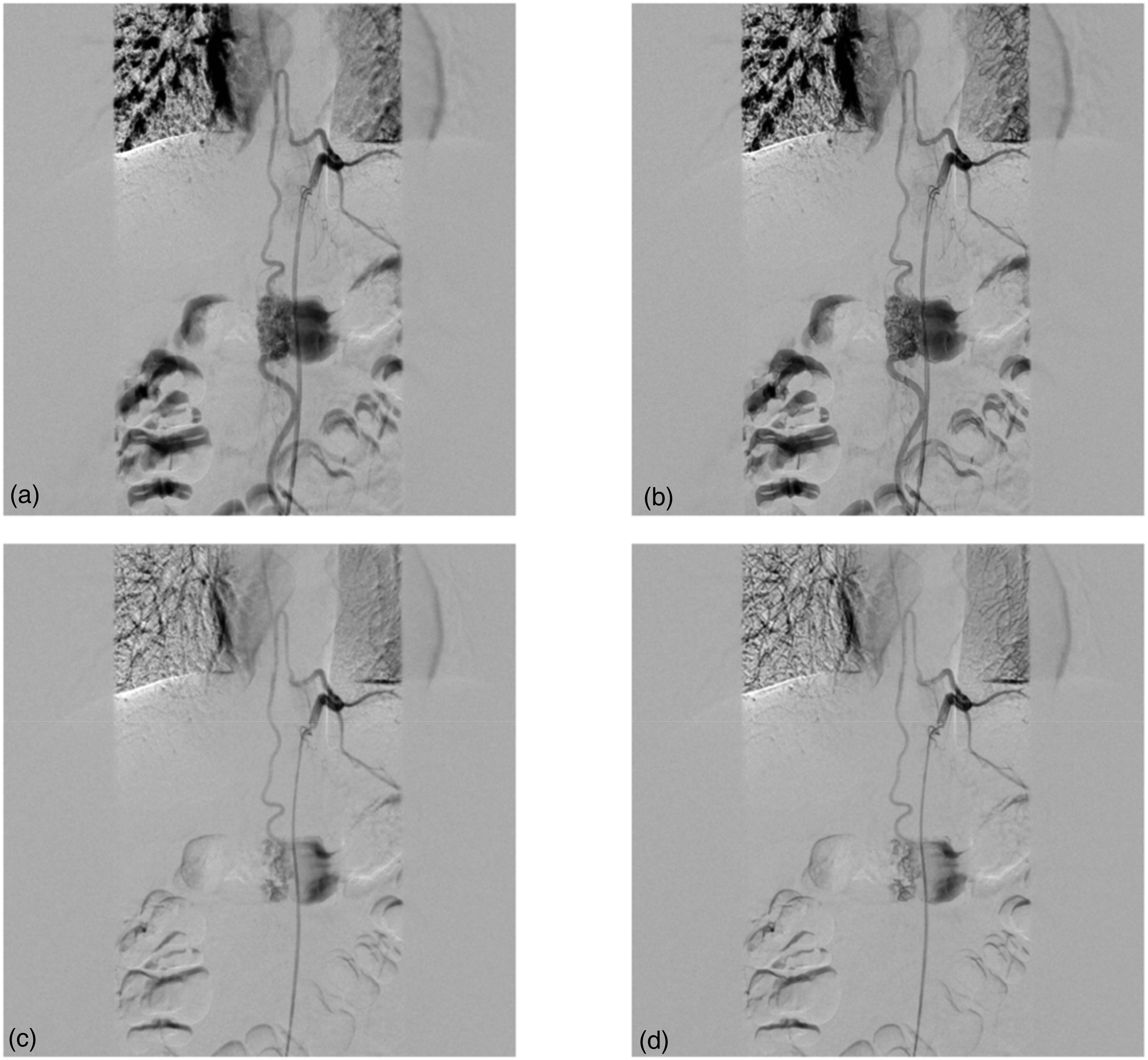
A case of spinal arteriovenous malformation (SAVM) fed by the anterior spinal artery: (a) shows normal spinal angiographic imaging in the large focal spot situation, while (b) shows the image after deblur post-processing, which has sharper and clearer vessels. (c) and (d) show arterial earlier stage, and compared to the large focal image in (c), deblurred image shows a clearer anatomy of sulcal-commissural arteries as well as SAVM (d).
Discussion
Neurosurgeons as well as neurointerventionalists regularly perform DSA to identify cerebrovascular lesions or as a reference image prior to or during the interventional or cranial treatment procedures. Almost all DSA machines can provide various field of views (FOVs) to facilitate use in different scenarios. For the same FOV, the image of the small focal spot is clearer than that of the large focal spot, but due to the dose limitation, the small focal spot cannot be applied to the image of a small FOV, leading to a poor image quality. However, small FOV is usually used for the precise imaging of vascular lesions or simultaneous imaging during interventional treatment, which determines the importance of small FOV image clarity and sharpness. The model constructed according to our neural network can successfully deblur the small FOV and large focal spot images synchronously, resulting in a clearer image, which has potential value for clinical application.
Several recent studies have focused on improving the clarity and sharpness of DSA images, but they all had different focuses from our study. Amelung et al. 10 proposed a metal artifact reduction algorithm applied to flat detector CT-angiography, which could improve image evaluation. However, their aim was to reduce the extent of metal artifacts in the follow-up images. Lang et al. developed a DSA sequence algorithm named artificial intelligence (AI)-based 3D angiography that allows better reconstruction of three-dimensional DSA but does not help in improving the clarity of intraoperative real-time DSA. 11 Setlur Nagesh et al. 12 evaluated a new system called high-resolution 76 µm high-definition (Hi-Def) mode, which improves the clarity of the pipeline embolization device in postoperative angiography but also differed from our study's focus. A computer-based method called the spatiotemporal denoising method was proposed by Hariharan et al., 13 whose aim was closest to the purpose of our research. However, the aim of Hariharan's study was to obtain satisfactory DSA images with a lower dose of contrast agent, and the algorithm is very different from the neural network algorithm. Our algorithms focus on clarifying and sharpening the large focal spot images, thus allowing the physicians to obtain more details from the angiography while observing more clearly at the time of treatment. Our aims and algorithms are innovative.
Our results also suggested that this algorithm may be of greater use in a proportion of patients with both cerebral AVM and SAVM. The treatment of AVM requires a more detailed view of the AVM architecture and their feeding branches, and clearer images will allow the neurointerventionalists to conveniently observe these details. In the cerebrovascular group, vascular occlusion images rarely benefit from deblur, but this technology can make vascular stenosis clearer and easier to measure. Furthermore, although our deblur algorithm does not focus on the treatment of the other group of AVM patients and the majority of the aneurysm and cerebrovascular stenosis patients, it can make the images clearer, which is still useful for physicians and their patients.
In addition, our DSA data were extracted from four different angiographic systems. This demonstrated that deblur technology can be well applied in the post-processing procedure of all kinds of angiographic systems. However, there is no denying that images obtained from the different angiographic systems, or even the same system but different machine models, may have differences in clarity inevitably. According to our result, we tend to believe that our technology can improve the clarity of DSA images in various angiographic systems, but whether the images processed by this technology are helpful for treatment depends more on the doctor's own judgment and the type of disease.
A prominent limitation was that we did not include a reduction in the amount of radiation in our study compared to other studies.12,13 However, we believe that clearer images will definitely reduce the number of repeated imaging due to image quality issues, and thus reduce the dose of radiation exposure to physicians.
Conclusion
We have developed the deblur technology based on a neural network model that allows for clearer and sharper DSA images, which has been proven in this study. This technology has excellent potential applications in the treatment of cerebrospinal vascular disease in the future.
Footnotes
Ethics approval
This study was approved by our institutional ethics committee (Xuanwu hospital, N0.2017024 and No.2017082).
Informed consent
Obtained.
Data availability statement
Data are available upon reasonable request. Because of the sensitive nature of the data, it is available upon request to the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Key Research and Development Program (grant number: 2016YFC1300800), Beijing Scientific and Technologic Project (grant number: Z201100005520021).