
Abstract
Purpose
Atherosclerotic cervical internal carotid artery disease is one of the major causes of ischemic stroke and transient ischemic attacks. The risk of stroke from mild to moderate stenoses (i.e. <50% stenosis) might be underestimated. There is increasing evidence that plaque morphological features reflect plaque instability that may harbor high risk for embolization. In this narrative review, we will review the literature on plaque features that predict vulnerability beyond the degree of stenosis, discuss the clinical association with stroke, and evaluate the evidence that these lesions serve as a source for embolic stroke of unknown source (ESUS).
Methods
We performed a literature search using PubMed, EMBASE, and Web of Science. The terms “embolic stroke of undetermined source” and “plaque morphology” were used either alone or in combination with “non-flow limiting stenosis,” “non-stenosing plaques,” “high-risk plaque features” or “internal carotid artery plaque.” Data on plaque morphology and ESUS were mainly taken from review articles, observational studies including retrospective cohort and cross-sectional studies, meta-analyses, and systematic reviews.
Conclusion
Nonstenosing carotid artery plaques with high-risk features carry a remarkable risk for stroke occurrence and randomized clinical trials are warranted for further evaluation of using carotid artery stenting or carotid endarterectomy to mitigate the risk of stroke.
Keywords
Introduction
Acute ischemic stroke (AIS) is one of the leading causes of disability and death worldwide. The secondary prevention of stroke varies based on the root cause of the initial event; thus, determining the cause of an individual AIS is critical for implementing effective care. 1 The well-described TOAST classification is used to classify stroke etiology and assigns stroke causes to one of five major categories: large artery atherosclerosis (LAA), cardioembolism, small vessel disease, stroke of other determined cause, or stroke of an undetermined cause. 2 According to this paradigm, the presence of large vessel disease is considered high risk for subsequent stroke only if >50% carotid artery stenosis is present.
Cryptogenic strokes represent around 30% of all AIS and are further classified as follows: stroke with no cause despite complete workup, stroke with multiple possible underlying causes, and stroke with incomplete workup.3,4 Embolic stroke of unknown source (ESUS) is a subcategory of the first cryptogenic stroke classification and is characterized as a non-lacunar ischemic stroke presumed to be of an embolic origin (i.e. superficial/cortical brain lesion) with no evidence of an obvious source of emboli. ESUS accounts for 9%–25% of all ischemic strokes.5–7 Cryptogenic strokes pose a remarkable treatment dilemma, as secondary prevention of stroke depends heavily on the identified cause, and these strokes have no apparent cause. For patients with ESUS, secondary stroke prevention strategies are primarily nonspecific, typically consisting of antithrombotic treatment with aspirin. 7
The most widely accepted predictor for AIS is the degree of carotid arterial stenosis, and rupture of the plaque itself is the main etiologic factor of embolic cerebrovascular events. 8 But several studies have indicated that measuring plaque stenosis alone underestimates the true plaque burden since certain physical plaque features are suggested to play a significant role in the plaque's contribution to stroke risk (i.e. high-risk plaques), even in non-stenotic internal carotid artery (ICA) plaques.9–11 It has been well reported that ipsilateral non-stenotic ICA plaques occur in approximately 40% of ESUS patients. 6 Despite the clear association between plaque composition and vulnerability to stroke development, current algorithms and guidelines still mainly use degree of stenosis and not plaque morphology as a decision-making criterion for secondary prevention strategies. 12 Also, the reporting of plaque features in radiological reports usually lacks a description of the plaque and tends to focus solely on the degree of carotid stenosis. 13 Therefore, our aim was to conduct a review of the literature to assess what is currently known about how non-stenosing carotid artery plaques contribute to the occurrence of stroke and TIA, and whether particular plaque features might be used as a tool for predicting patients’ risk of recurrent stroke and TIA events.
High-risk features indicating plaque vulnerability
Researchers have described the following high-risk features of plaques that may lead to stroke: presence of intraplaque hemorrhage (IPH), lipid-rich necrotic core, large plaque volume, significant plaque thickness, echolucency, thin/ruptured fibrous cap, plaque irregularity (0.3–0.9 mm fluctuation of plaque surface), plaque ulceration (depression of >1 mm in plaque surface), and plaque inflammation/hypermetabolism.4,14–23 Plaque vulnerability, in other words, is a plaque's susceptibility to rupture and is a proposed determinant of high risk for superimposed thrombosis. 24 From this concept, researchers have been investigating possible plaque features that would designate plaques as “vulnerable” in the hopes of aiding secondary prevention protocols to avert future cerebrovascular events.4,25–27
According to a meta-analysis conducted by Kamtchum-Tatuene et al. that analyzed 64 studies, high-risk plaque features were three times more prevalent in patients with symptomatic versus asymptomatic carotid stenosis (Odds Ratio [OR] = 3.4). 25 Another study showed that high-risk plaque signs were more common in symptomatic patients with mild-to-moderate carotid stenosis than in patients with asymptomatic stenosis—namely, thin or ruptured fibrous cap (100% vs. 36%,); IPH (86% vs. 33%); and the presence of a lipid-rich necrotic core (100% vs. 39%). 17
IPH, defined as high-intensity signals seen on fat-suppressed T1-weighted sequences by magnetic resonance imaging (MRI), has been identified as a potential trigger of plaque instability (Figure 1). 28 This phenomenon is based on histologic examinations that have shown free hemoglobin and erythrocytes within thin-walled microvessels, which may be prone to disruption. 29 Gupta et al. reported a significant association between IPH and cryptogenic strokes. 30 And three separate meta-analyses have also found that symptomatic patients with carotid IPH have an annual stroke risk of 15%–45%, despite optimization of medical therapy.21,31,32 This study illustrated the higher risk for recurrent stroke in patients with ESUS with an identifiable IPH (16.7% vs. 2.4% for patients without IPH). 33
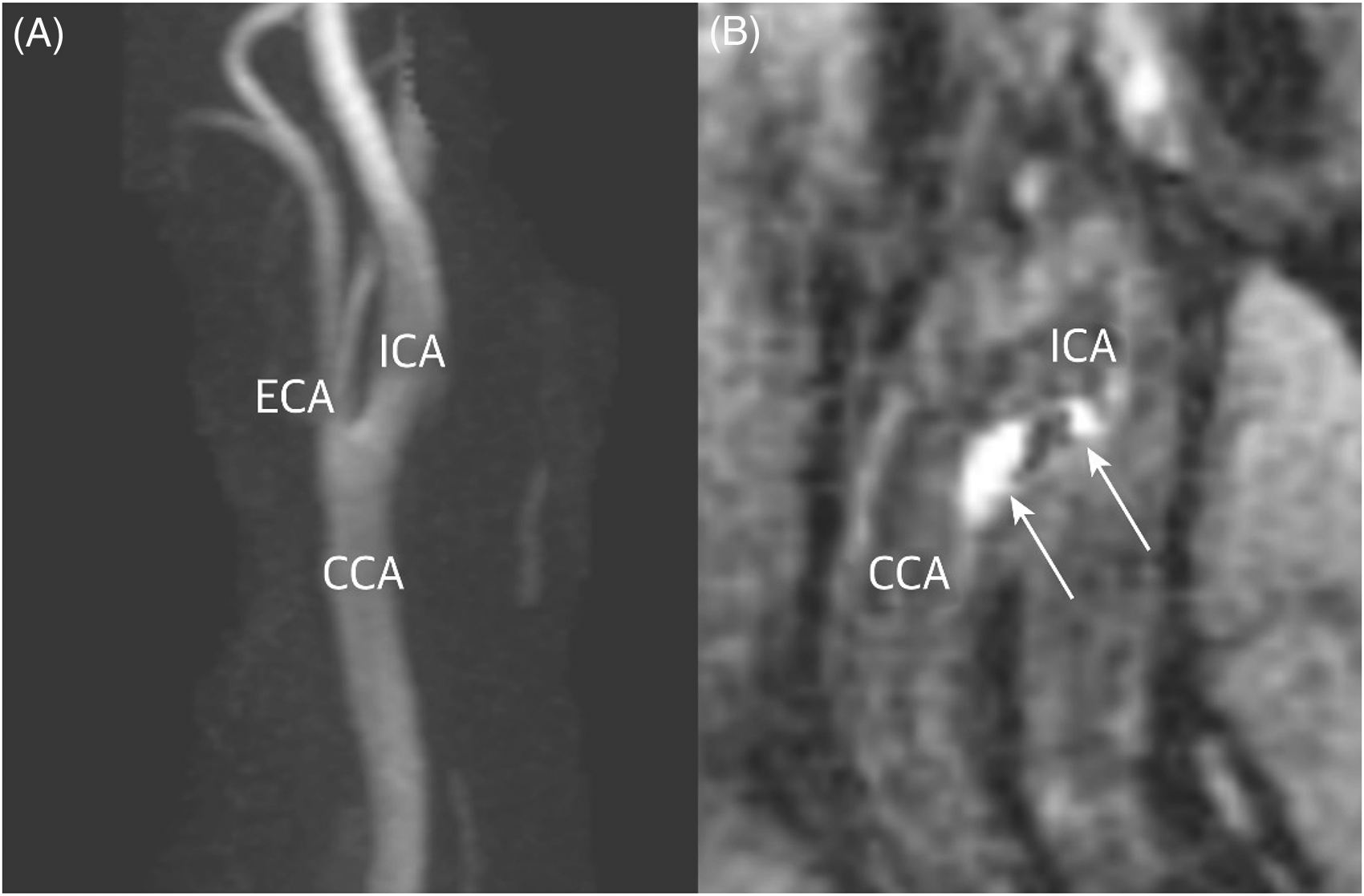
MRA with contrast showing a non-stenosing plaque (A). MPRAGE MRA shows hyperintensity on T1-signal on the left carotid artery suggestive of intraplaque hemorrhage (B). MPRAGE, magnetization-prepared rapid acquisition with gradient echo; CCA, common carotid artery; ECA, external carotid artery; ICA, internal carotid artery (From Larson et al. 33 with permission).
Maximum soft plaque thickness and “rim sign” (thin adventitial calcifications) are usually identified through computed tomography angiography (CTA), and these signs in combination are likely to predict the presence of IPH that can be seen by magnetic resonance angiography (MRA).13,34,35 Additionally, identifying a rim sign, maximum soft plaque thickness (for each mm increase in thickness), and intraluminal thrombus was more predictive of stroke than measuring the degree of stenosis alone. A systematic review by Singh et al. showed that the risk of recurrent stroke/transient ischemic attack in patients who have non-stenosing carotid plaques was 2.6 per 100 patient-years, and this increased to 4.9 per 100 patient-years if IPH was identified. 36
Higher plaque thickness in non-stenosing ICA plaques is also shown to be associated with a higher risk for an ipsilateral AIS. Coutinho et al. reported that plaque thickness of ≥ 3 mm was significantly more commonly located ipsilateral to the side of the stroke (35%) than in contralateral carotid arteries (15%) (Figure 2). 37 Similar to Coutinho's results, they found that plaques thicker than 3 mm were significantly associated with a higher risk for an ipsilateral (29.2%) rather than contralateral (18.7%) AIS. In the same study, however, they did not find a significant association between plaque features (plaque irregularity, ulceration, density, plaque calcification) and occurrence of ipsilateral AIS, likely because the analysis may have been underpowered. Interestingly, Siegler et al. also showed similar findings in 2019, and they found that 35% of patients with ESUS had ≥ 3 mm of carotid artery plaque ipsilateral to the stroke versus 15% of patients with the problem in the contralateral artery. 38
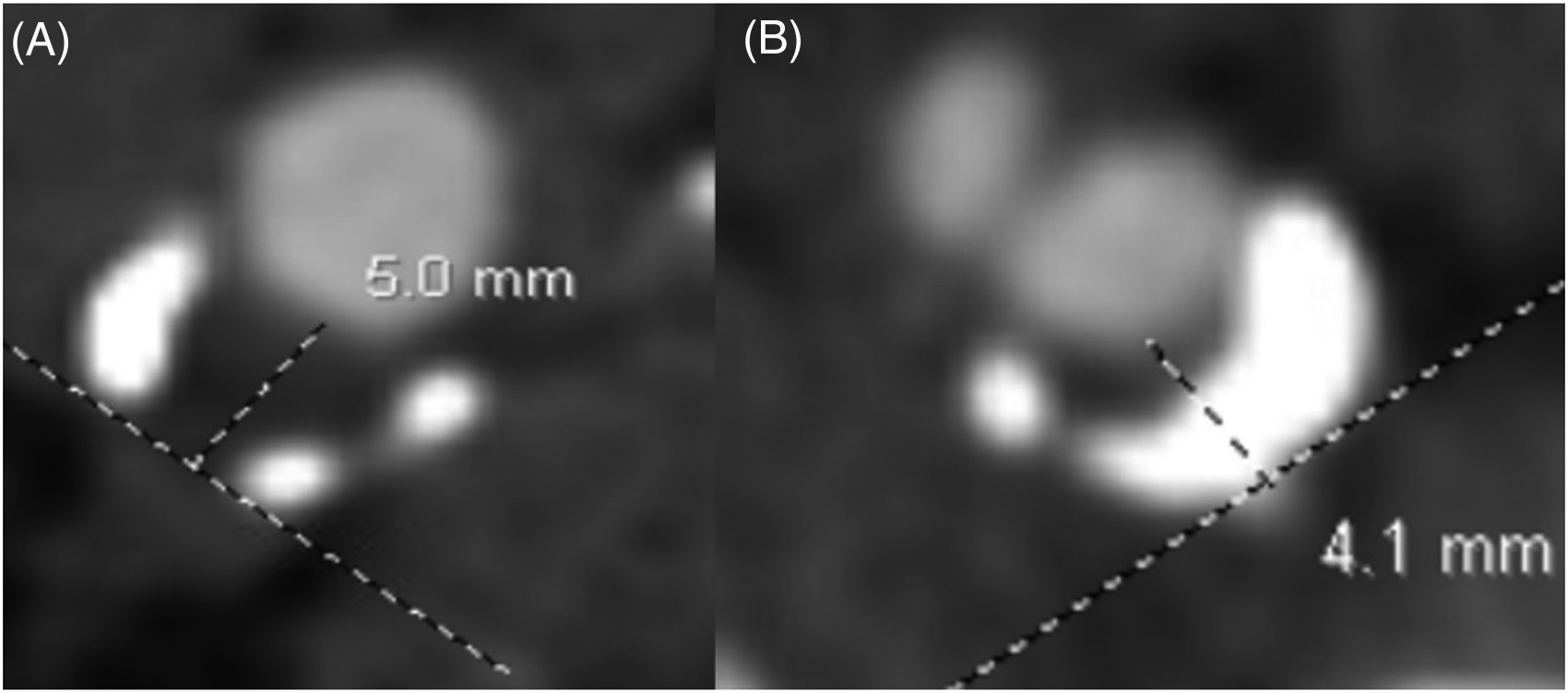
Right (A) and left (B) distal carotid arteries showing a soft plaque of 5 mm and a mixed plaque of 4.1 mm thickness, respectively.
Not only plaque thickness, but also plaque length was investigated; Jumah et al. reported significant association between Plaques with >1 cm length and ulcerated plaques on CTA with ipsilateral ESUS (Figure 3). 26
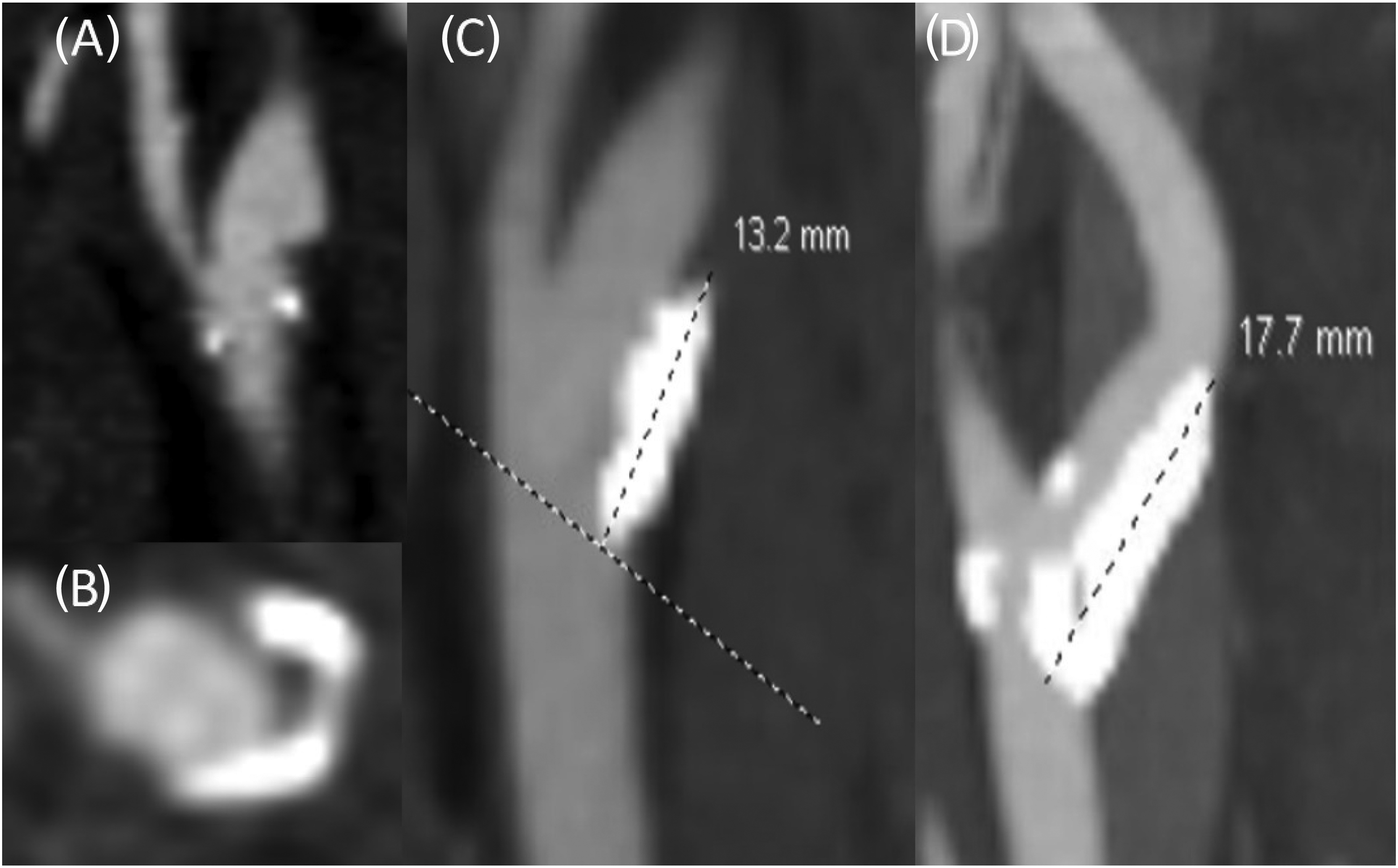
Left-sided internal carotid artery showing an ulcerated plaque on sagittal (A) and axial (B) sections. (C) and (D) show left-sided carotid arteries harboring calcified plaques of >1 cm in length.
A retrospective cohort study discussed a novel paradigm for predicting which patients were at highest risk for developing a new stroke due to carotid artery disease. 39 Their model included patients 75 years of age or above, with a maximal carotid wall thickness of >4 mm, and the prescribed antihypertensive medication regimen was included in the model. The model's receiver operating characteristic curve (ROC) analysis showed an area under the curve of 0.706 for prediction of new stroke, identifying 10 out of 14 patients who had a new carotid stroke. A lower cutoff value for plaque thickness (≥ 1.5 mm) was also found to be more often seen ipsilaterally rather than contralaterally to the side of the stroke (59% vs. 42%). 40
Plaque size has also been highlighted in the literature to be associated with an increased risk for AIS. The ACSRS study analyzed plaque areas that were causing 12%–99% stenosis as assessed by ultrasonography in patients with carotid disease and found that higher plaque areas (>0.8 cm2) were associated with an increased risk for ipsilateral stroke. 41 A study by Elhfnawy et al. evaluated internal carotid artery plaques with 20%–40% stenosis in both symptomatic and asymptomatic patients. Interestingly, plaques with a cross-sectional area ≥0.36 cm2 had 71% sensitivity and 76% specificity for predicting symptomatic ipsilateral ICA-stenosis. 27
Some studies showed that vulnerable and complex plaques had higher fluorodeoxyglucose uptake as seen on PET scans in which this metabolic activity is thought to be due to increased inflammatory cell content (e.g. activated macrophages) within the location of complicated plaques, which leads to the high risk for embolism (Figure 4).15,42 Watase et al. used MRI to study plaque features, the plaque location relative to stroke laterality, and the presence of high-risk plaque features in the carotid artery ipsilateral to a recent ischemic stroke of the anterior circulation. 39 They categorized patients' internal carotid arteries into four groups based on the presence of significant stenosis (50% vs. <50%) and/or the presence of a high-risk plaques. The group that had high-risk plaques, but no significant stenosis had greater wall thickness and eccentricity indices than those who had significant stenosis but no high-risk plaques, suggesting a high risk for rupture and embolism despite a lack of significant stenosis.
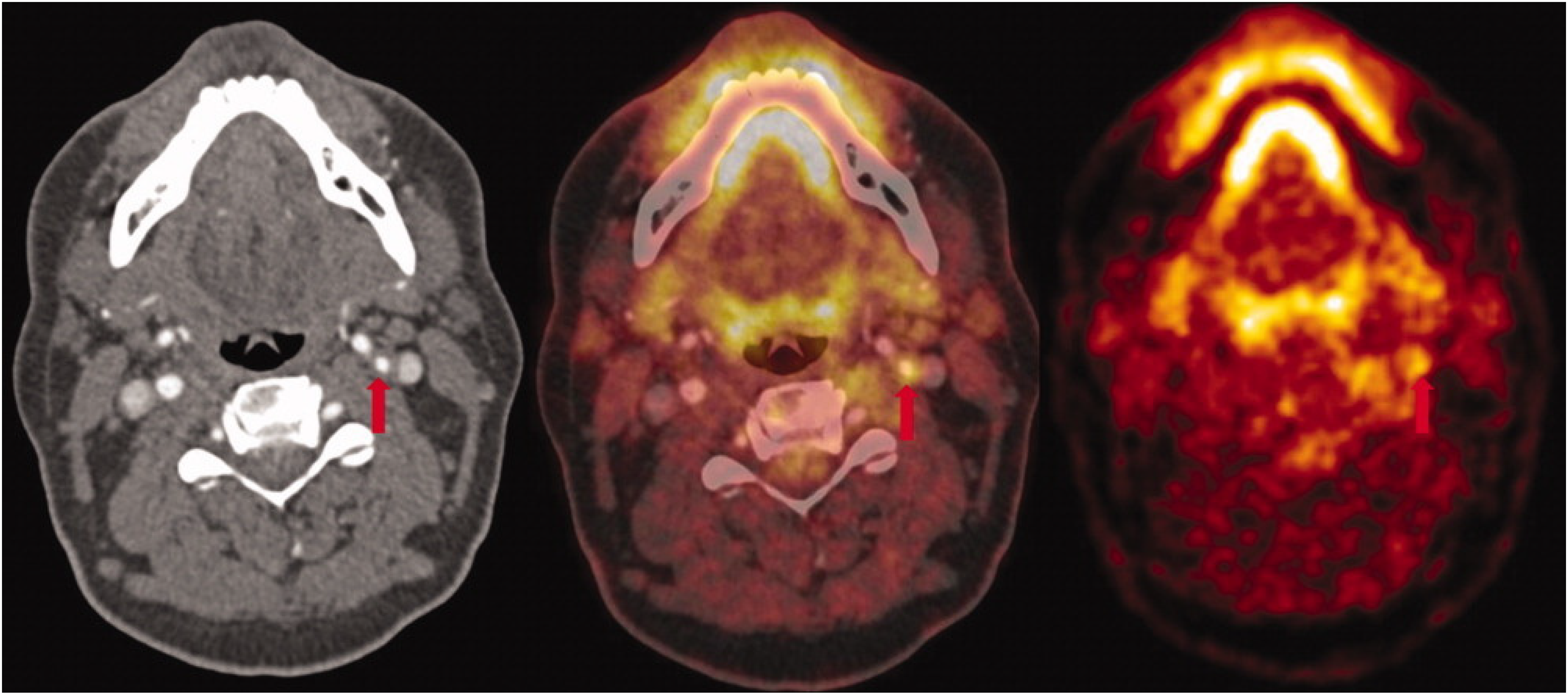
Carotid PET/CT (from left to right, axial CTA, fused PET/CT and PET image) showing inflamed left carotid artery plaque in a patient who had a stroke in the same vascular territory. (From Marnane et al. 42 with permission).
Current evidence on the relationship between ESUS and non-stenosing carotid artery plaques
Laterality of carotid plaques and stroke
Multiple studies have observed a higher prevalence of high-risk plaques being ipsilateral to the stroke side, substantiating the idea of a direct relationship waiting to be confirmed.26,43,44
The CAPIAS trial was an observational study that analyzed patients older than 49 years of age who were diagnosed with AIS with unilateral or bilateral carotid artery plaques causing <70% stenosis. 45 Patients with complicated disease more frequently had ipsilateral infarcts; specifically, patients with 50%–69% stenosis had a higher prevalence of complicated plaques, which most commonly featured IPH.
A meta-analysis that assessed 323 patients with ESUS showed that mild carotid stenosis with unstable or high-risk plaque features (i.e. ruptured fibrous cap) was significantly more commonly located ipsilateral to the stroke side in patients with ESUS (32.5%) versus being contralaterally located (4.6%). 46 This was similarly shown by Kamel et al., who studied 579 patients enrolled in the Cornell Acute Stroke Academic Registry (CAESAR). 47 This study, which used MRI with contrast enhancement, showed that the prevalence of complicated atherosclerotic plaques ipsilateral to the infarct were more than twice as prevalent as those that were found contralaterally; 31% and 12%, respectively. Similar to the CAPIAS trial, the most frequent characteristic of an ipsilateral complicated plaque in the CAESAR study was IPH. 45
Knight-Greenfield et al. evaluated plaque features by CTA in patients with AIS who did not have hemodynamic stenosis. They found that patients with ESUS had a higher total plaque thickness ipsilateral to the stroke side. 48
Inflammation plays an interesting role in the stability of carotid plaques as shown in previous studies. 49 A very recent study by Hu et al., analyzed the prevalence of pericarotid fat density, measured by Hounsfield units on CTAs. The authors showed that it significantly increased ipsilateral to ESUS when compared with strokes on the contralateral side. This was suggestive for the presence of inflammation that extends beyond the vessel lumen, putting patients at a higher risk for plaque rupture. 50 On the contrary, Li et al. argued against occult atherosclerotic disease as a cause of cryptogenic stroke. This study, however, lacked detailed imaging of high-risk plaque features and instead used ultrasonographic assessments of luminal stenosis. 51 Evidently, multiple questions and ambiguities still exist, suggesting that more research is needed to establish causation between non-stenosing carotid plaques and ESUS and to quantify the risk for ESUS and rates of recurrence.
Arterial stiffness index in ESUS
Blood pressure variability has been shown to be associated with an increased incidence of cerebrovascular events, as greater variability means greater mechanical stress applied on arterial walls. 52 This was thought to be due to the pressure leading to higher risk for carotid arterial stiffness and arterial remodeling, thus resulting in rupture of atherosclerotic plaques.
Arterial compliance is the linear regression slope of diastolic blood pressure on systolic blood pressure calculated through plotting blood pressure measurements monitored continuously. Its complement (1 minus the Slope) indicates arterial stiffness index (ASI) which is a measure of arterial stiffness and plaque burden. 53 With that said, arterial stiffness is a concept thought to be associated with higher atherosclerotic disease burden, and higher arterial stiffness index (ASI) values have been observed in patients who have had ischemic and hemorrhagic strokes, which would suggest a prognostic value of ASI for predicting ESUS.54,55 A study by Acampa et al. showed that patients with ESUS and non-stenosing carotid plaques had high ASI values (>0.7), indicating that these patients had a similar cardiovascular complication risk as patients with stroke due to atherosclerosis. 53
Ultrasonography and ESUS
Ultrasonography is a safe diagnostic tool that has almost no contraindications, which makes it a useful approach for determining stroke risk in patients with carotid disease. Transcranial doppler is a validated tool used to detect microembolic signals by using a probe that is placed next to the ipsilateral middle cerebral artery. 56 It is mainly used for the detection of embolism in patients with carotid stenosis, and severe degrees of stenosis are significantly associated with higher microembolic signal detection. 57 Reportedly, researchers have shown that ESUS was detected more often by microembolic signals (50%) than by LAA (40%), cardioembolism (33%), TIA (17%), and small vessel disease (14%). 58 This supports the nature of embolic phenomena in patients with ESUS, irrespective of the origin of the embolus.
Nonetheless, echolucency via ultrasonography can reveal high lipid content, macrophage density, and hemorrhage, which reflect a higher tendency for the plaque to rupture (Figure 5).59–61 Plaque burden was also assessed by measuring plaque length, thickness, volume, and echolucency, all quantified through carotid ultrasonography. This suggested that a greater carotid plaque burden is potentially associated with a higher risk for embolization. 62 A meta-analysis that was conducted by Brinjikji et al. reported that high-risk plaque features (including plaque neovascularity, echolucency, ulceration, and intraplaque motion) seen by ultrasonography were associated with a higher risk for an ischemic process. 63
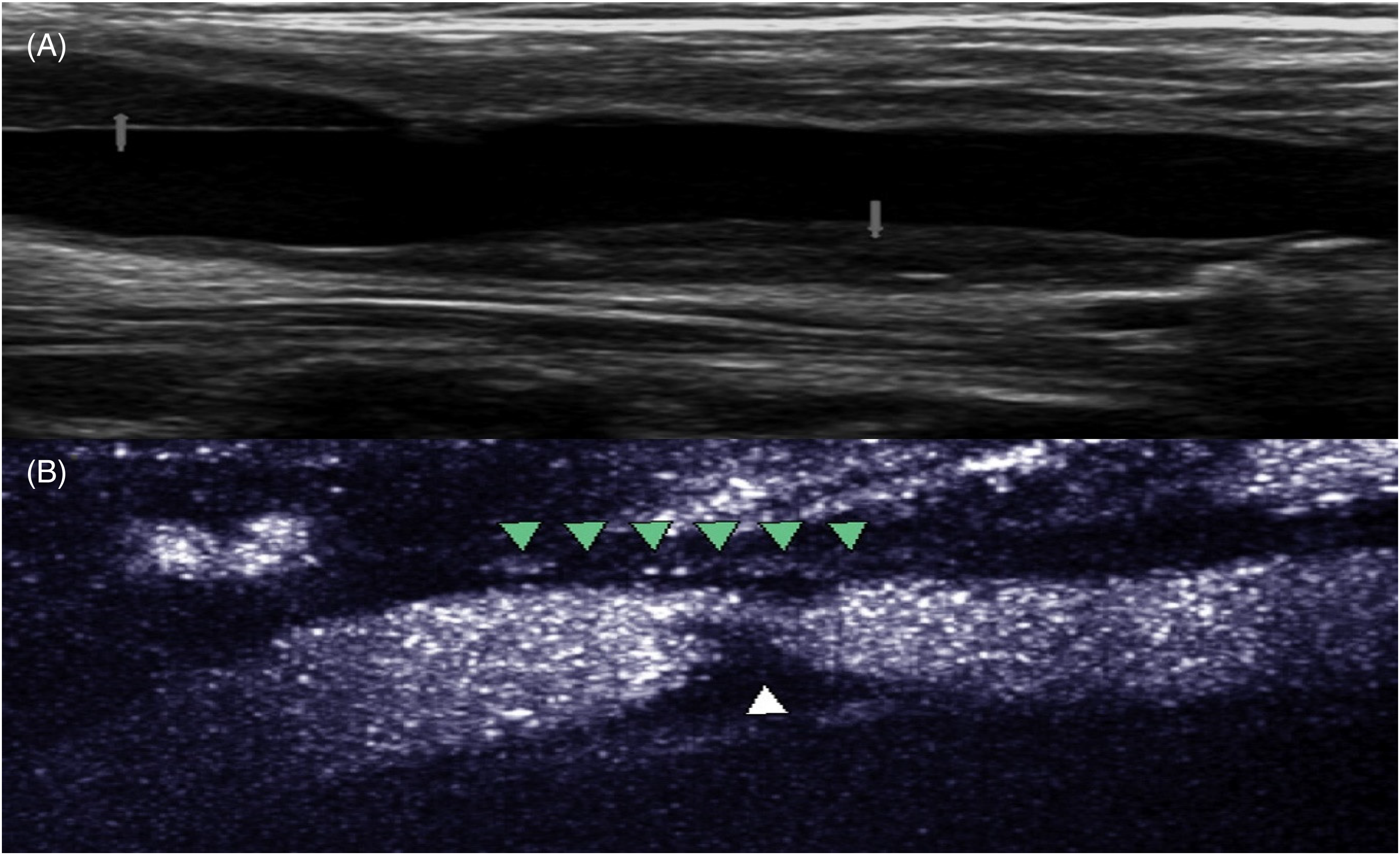
Carotid US showing echolucent plaques (arrows in A). Contrast enhanced carotid US showing intraplaque neovascularization (B). Microbubbles seen within atheromatous plaque (Green arrowheads). White arrow indicates a region of the plaque not perfused by microbubble contrast (A; from Skagen et al. 60 with permission), (B; From Shalhoub et al. 61 ; with permission).
Clot composition and stroke etiology
The development of stent retrievers and advancements in endovascular reperfusion via mechanical thrombectomy in clinical practice have resulted in the possibility of analyzing retrieved blood clots. Understanding thrombus characteristics to determine the causes of a stroke has the potential to improve the treatment of stroke, and this has gained significant attention in the recent literature.64,65
Fitzgerald et al. showed that higher platelet count in the thrombus was indicative of LAA as a cause of stroke, which supports treatment algorithms for cryptogenic strokes that include using antiplatelet agents.
Carotid endarterectomy for non-stenotic carotid plaques
Indeed, current guidelines do not support using CAS or CEA for addressing non-stenosing carotid plaques. However, as mentioned earlier, a growing body of evidence suggests that not all symptomatic plaques result in clinically significant stenosis. In a study by Tonetti et al., the number of patients with carotid stenosis ≥50% was overestimated based on non-invasive carotid imaging results, and the use of digital subtraction angiography showed that many of these patients actually had an insignificant (<50%) stenosis. 66 Also, most patients were found to have ulcerations and higher plaque thickness, correlating with a higher risk of stroke risk despite the mild stenosis.
A systematic review performed by Larson et al. analyzed 6 studies on the treatment of non-stenosing carotid plaques. Prior to the CEA, 55.8% of the patients had a recurrent ipsilateral ischemic event despite optimal medical therapy; after CEA, none of the 138 patients who had an available follow-up (mean 36.1 months) had a recurrent ipsilateral ischemic event. 67 This opens the consideration for CEA as a beneficial treatment for patients with non-stenosing carotid plaques and supports the hypothesis that CEA might be a plausible intervention as a secondary stroke prevention strategy in patients with symptomatic mild carotid stenosis harboring high-risk features. In a study by Coutinho et al., the authors have also suggested that patients who have had multiple strokes stemming from problems in the same territory of a high-risk non-stenosing plaque and who were not treated successfully with optimal current treatments may benefit from investigation into alternative causes and treatment with CEA. 37
Discussion
Studies using data from retrospective and prospective registries have revealed a remarkably higher risk of ESUS within the context of ipsilateral non-stenotic ICA plaques, suggesting a possible association between these two clinical phenomena.30,68 As detailed in this review, multiple adequately powered studies looking at the possible characteristics and features that cause a high risk of ESUS, such as stroke location compared to plaque location, plaque morphology, arterial stiffness, and others, have been done, and they cumulatively suggest an association between the presence of non-stenosing ICA plaques and ESUS. However, few of these studies have been replicated to reinforce the aforementioned relationship. This association has been shown not only in studies used CTA and MRA for identifying non-stenosing ICA plaques, but also in studies that looked at PET scan results, which have revealed that the metabolic activity within the plaque's milieu may be correlated with its vulnerability. 15 Nonetheless, with the development of sophisticated imaging techniques, we are now able to better characterize ICA plaques and identify the commonly seen features that reflect a high-risk for embolism (Table 1).
High-Risk Carotid Plaque Features.
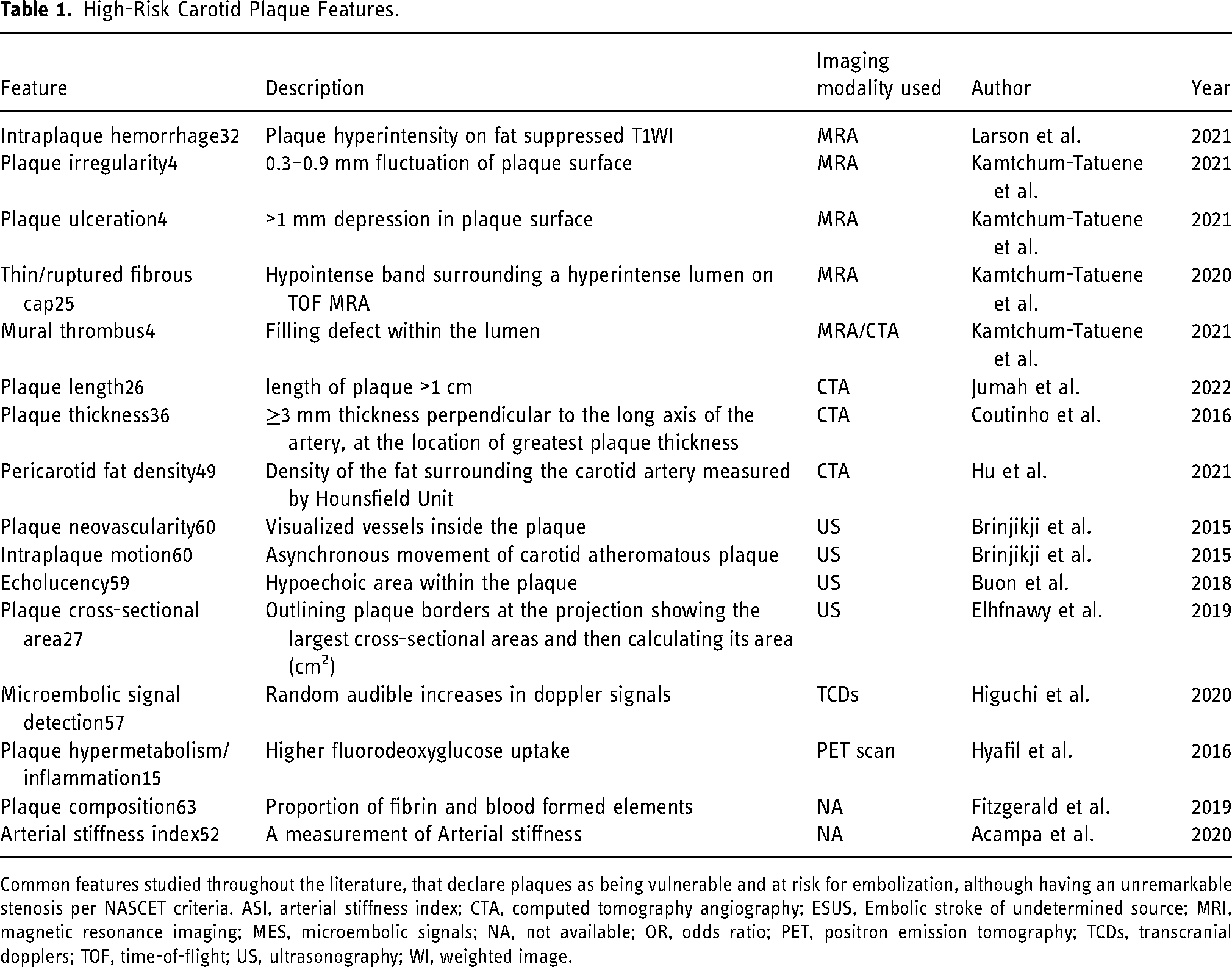
Common features studied throughout the literature, that declare plaques as being vulnerable and at risk for embolization, although having an unremarkable stenosis per NASCET criteria. ASI, arterial stiffness index; CTA, computed tomography angiography; ESUS, Embolic stroke of undetermined source; MRI, magnetic resonance imaging; MES, microembolic signals; NA, not available; OR, odds ratio; PET, positron emission tomography; TCDs, transcranial dopplers; TOF, time-of-flight; US, ultrasonography; WI, weighted image.
Some studies have focused on plaque features other than the degree of stenosis. In defining LAA, the Chinese Ischemic Stroke Subclassification (CISS) system incorporates plaque vulnerability into the classification scheme, which offers details on stroke pathophysiology. 69 The Subtype of Ischemic Stroke Classification System (SPARKLE) focuses on plaque burden for defining LAA, and the authors suggest a total plaque area of ≥1.19 cm2 as a definition for LAA. 70 This helped the authors identify more cases of LAA than when the degree of stenosis alone was used (33% vs. 21%, respectively). The validation of these classification systems was studied by Zhang et al., showing a substantial agreement among the 3 main stroke classification schemes: TOAST, CISS, and SPARKLE. In the same analysis, the CISS system showed excellent inter-rater reliability (k = 0.857). 71 The association between ESUS and non-stenotic ICA plaques is plausible, and from the reviewers’ perspective, a routine description of asymptomatic carotid artery plaques in radiology reports is warranted to be used as a future reference in clinical trials to help answer whether interventions for such plaques by either CEA or CAS for the prevention of future strokes is justifiable. Finally, caution must be taken while interpreting the association between high-risk plaque features and ESUS, as there are no clinical trials to suggest absolute benefit from intervention. Predictive models and scoring systems incorporating multiple plaque features for the assessment of recurrence risk of stroke and TIA events are of utmost importance in guiding treatment in the future.
Conclusion
Despite the evidence that high-risk plaque features can predict a recurrent stroke, adoption of this principle and its integration into the medical guidelines have not yet been established. This reflects a lack of clinical trials that have utilized detailed plaque characterization for assessing risk of stroke. Thus, randomized controlled trials are warranted to evaluate the utility of using CEA and CAS versus optimized medical care for treating high-risk, non-stenosing ICA plaques, as this may clarify future stroke risk stratification and may guide development of improved treatment strategies.
Footnotes
Abbreviations and Acronyms
Acknowledgements
The authors thank Karla D Passalacqua, PhD, at Henry Ford Hospital for editorial services.
Availability of data and material
All data is available from the corresponding author upon reasonable request
Code availability
Not applicable.
Disclosures
Authors have no relationships to disclose.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
No institutional approval required for review articles.
Informed consent
Consent is not applicable for review articles.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.