
Abstract
Background and Purpose
Two early basilar artery occlusion (BAO) randomized controlled trials (RCTs) did not establish the superiority of endovascular thrombectomy (EVT) over medical management. Yet many providers continued to recommend EVT. The goal of the present article is to compare physicians’ diagnostic and management strategies of BAO among middle-income and high-income countries (MICs and HICs, respectively).
Methods
We conducted an international survey from January to March 2022 regarding management strategies in acute BAO, to examine clinical and imaging parameters influencing clinician management of patients with BAO. We compared responses between physicians from HIC and MIC.
Results
Among the 1245 respondents from 73 countries, 799 (64.2%) were from HIC, with the remaining 393 (31.6%) from MIC. Most respondents perceived that EVT was superior to medical management for acute BAO, but more so in respondents from HIC (98.0% vs. 94.2%, p < 0.01). MIC respondents were more likely to believe further RCTs were warranted (91.6% vs. 74.0%, p < 0.01) and were more likely to find it acceptable to enroll any patient who met a trial’s criteria in the standard medical treatment arm (58.8% vs. 38.5%, p < 0.01).
Conclusions
In an area where clinical equipoise was called into question despite the lack of RCT evidence, we found that respondents from MIC were more likely to express willingness to enroll patients with BAO in an RCT than their HIC counterparts.
Keywords
Background
Despite a well-established evidence for endovascular therapy (EVT) in anterior circulation acute large vessel occlusion (LVO) stroke since 2015, 1 randomized clinical trial (RCT) evidence to support EVT for basilar artery occlusion (BAO) has, until the May 2022 presentation of the ATTENTION 2 and BAOCHE 3 trial results, been absent. Published RCTs of posterior circulation LVO (BEST 4 and BASICS 5 ) did not show a benefit of EVT over standard medical care. The results of these studies were limited by a slow recruitment and a moderate crossover rate in the BEST study.4,5 Due to the poor natural history of BAO, 6 and the high degree of clinical efficacy of EVT in anterior circulation proximal LVO, 1 many providers have continued to treat patients with acute BAO 7 with EVT while awaiting RCT evidence.8,9
We recently surveyed a diverse international cohort of physicians involved in acute stroke care regarding their practice in BAO and found significant variation in responses based on their demographics, roles, and experience. 7 Despite little improvements in recent decades, research highlights that patients from low and middle-income countries (LMICs) have less access to clinical research trials and high-cost technology.10–15 RCTs have the potential to improve resources and access to healthcare for patients in LMIC. 16 However care needs to be taken to safeguard against exploitation and “research tourism,” especially in areas where best practice treatment has been established. 17 In this follow-up analysis to the After the BEST of BASICS (ABBA) survey, we sought to determine areas of clinical uncertainty in acute BAO treatment; whether decisions and willingness to participate in RCTs, vary according to the country’s resources and if so, what learnings could be taken to influence future trial design.
Methods
Data is available from the corresponding author upon reasonable request.
The reader is referred to the primary report for detailed survey methodology.7,18 The survey was conducted between January 18 and March 31, 2022. The online questionnaire was distributed internationally among members of the Dutch Neurovascular Society, the British and Irish Association of Stroke Physicians, Stroke Clinical Trials Network in Ireland, International Stroke Trial Network of a co-author (UF), the Brazil Stroke Society, German Stroke Trial Network, the Italian Stroke Association, the Japan Stroke Society, the Japan Society for Neuroendovascular Therapy, the European Stroke Organization blog, the Madrid Association of Neurology, the Colombia Association of Neurology, the Norway Stroke Organization, Indonesian Neurointerventionalists, the Society of Vascular and Interventional Neurology (SVIN) Membership List, the Global SVIN COVID-19 stroke registry, and via invitation by co-authors to their colleagues. The survey was also distributed via the Whatsapp or Telegram group for two Neurointerventional groups, the WeChat Stroke Network in China, MT2020, and Women in Neurointervention. Participant emails were obtained to prevent duplicate response bias.
Ethics
Approval by the local research ethics board was obtained via the coordinating center's hospital. The study was classified as exempt as it did not qualify as human subjects research.
Physician respondents were grouped by their country of practice, as defined by the World Bank country classifications by income level, 2021 to 2022. 19 Countries were stratified into high-income countries (HICs), high-middle income countries, LMICs and low-income countries (LICs) based on gross national income per capita in US dollars. For the purpose of this analysis, high-middle and low-middle income respondents were grouped as middle-income countries (MICs) due to the lower sample size of high-middle and low-middle income respondents.
Statistical analysis
Statistical analysis was performed using SAS 9.4 software (SAS Institute, Cary, NC, USA). The results were summarized using descriptive statistics (i.e. frequencies and percentages). Differences between the groups (age, gender, experience, specialty, continent, and country income) were assessed by the chi-square test or Fisher's exact test (when appropriate). A p-value of <0.05 was considered statistically significant for all tests. Figure 1 was created with Tableau.
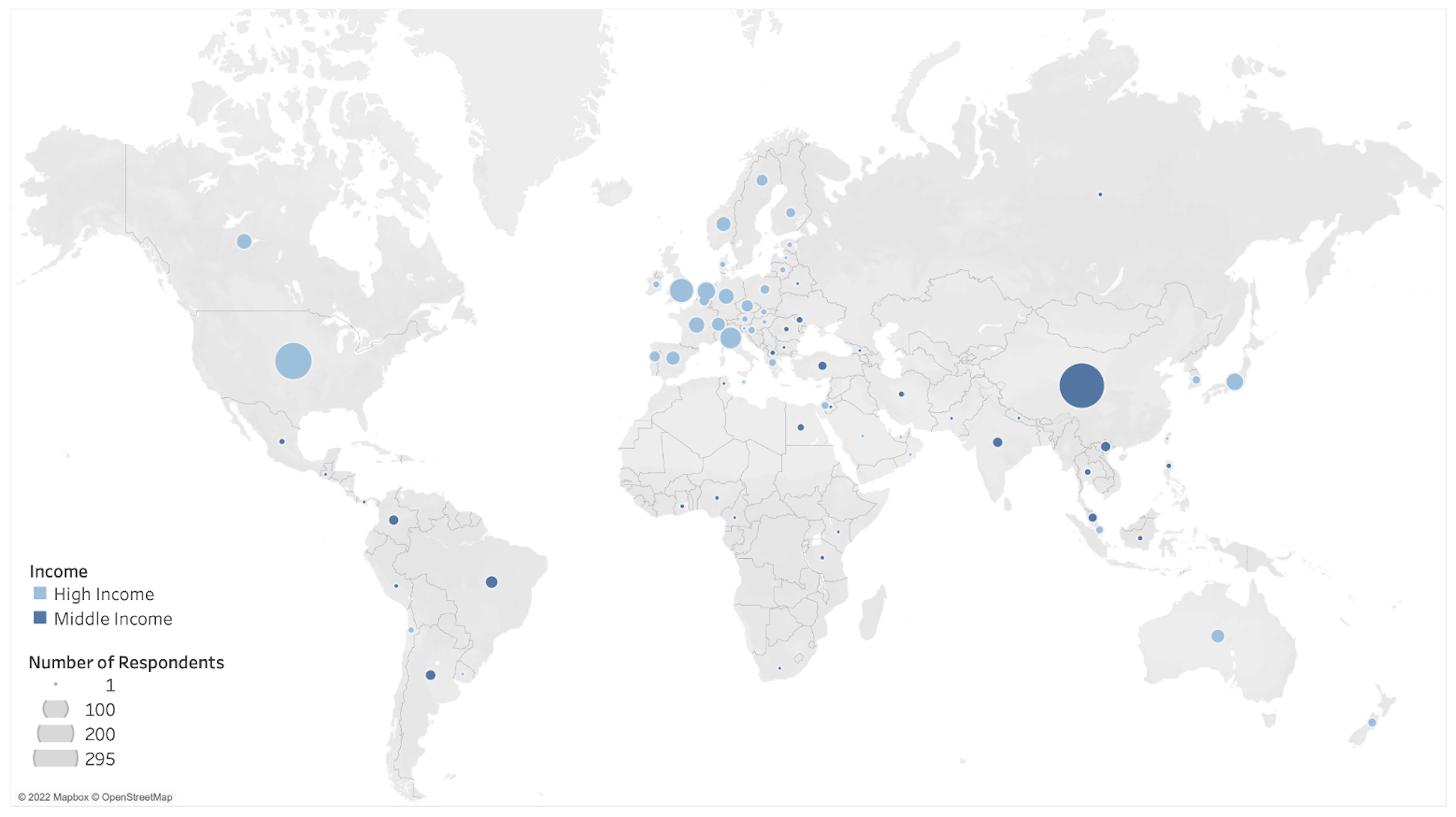
World map of respondents according to country income.
Results
Demographic distribution
There were 1245 respondents from 73 countries, 799 (64.2%) from HIC, 393 (31.6%) were from high-middle income countries and 53 (4.3%) from LMICs. There were no respondents from LIC. Baseline characteristics of respondents are presented in Table 1.
Descriptive table of respondents.
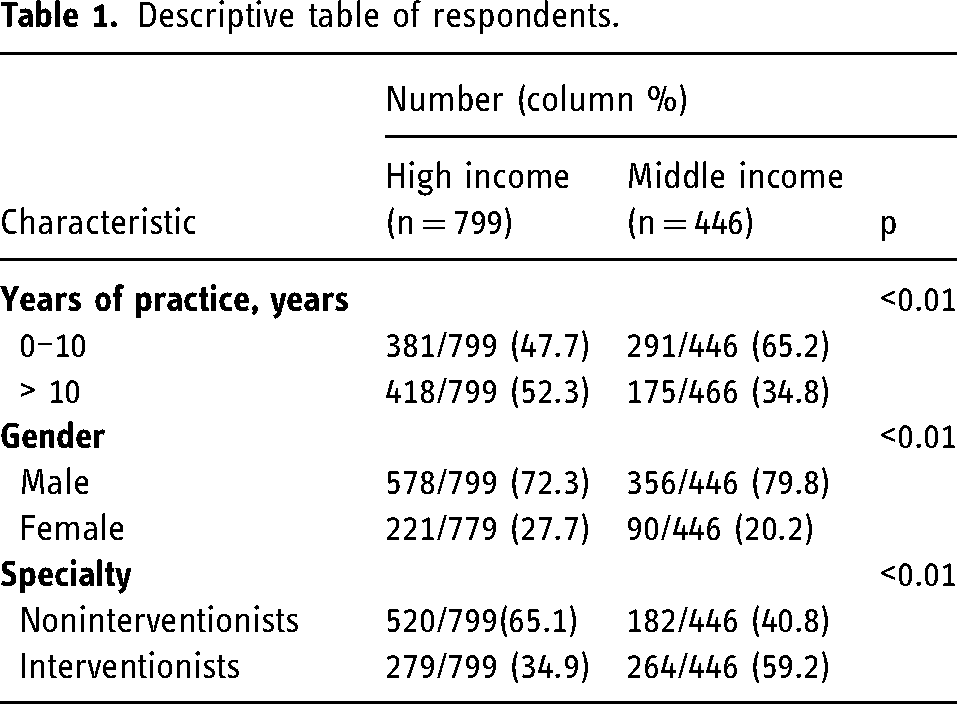
Compared to respondents from HIC, those from MIC were more likely to be interventionists (59.2% vs. 34.9%, p < 0.01), more likely to be male (79.8% vs. 72.3%, p < 0.01), and more likely to have <10 years of experience as a senior decision maker (65.2% vs. 47.7%, p < 0.01; Figure 1).
European respondents comprised 39.6% of all responses, followed by Asia, 33.3%, and North America, 18.8%. China, a high-middle income country, was the largest country in response, 23.7%, followed by the United States, a HIC, with 15.7%.
Decision to offer EVT in BAO in clinical practice
There was broad agreement that, in certain circumstances, EVT was superior to standard medical treatment (SMT) in patients with BAO; however, this perception was higher among those from HIC (98.0% vs. 94.2%, p < 0.01). Respondents from MIC were more likely to report that the results of the BEST and BASICS RCT had altered their management of BAO (37.9% vs. 25.6%, p < 0.01), and more likely to agree that further trials were warranted (91.6% vs. 74.0%, p < 0.01; Table 2).
Equipoise of basilar artery thrombectomy by income group.
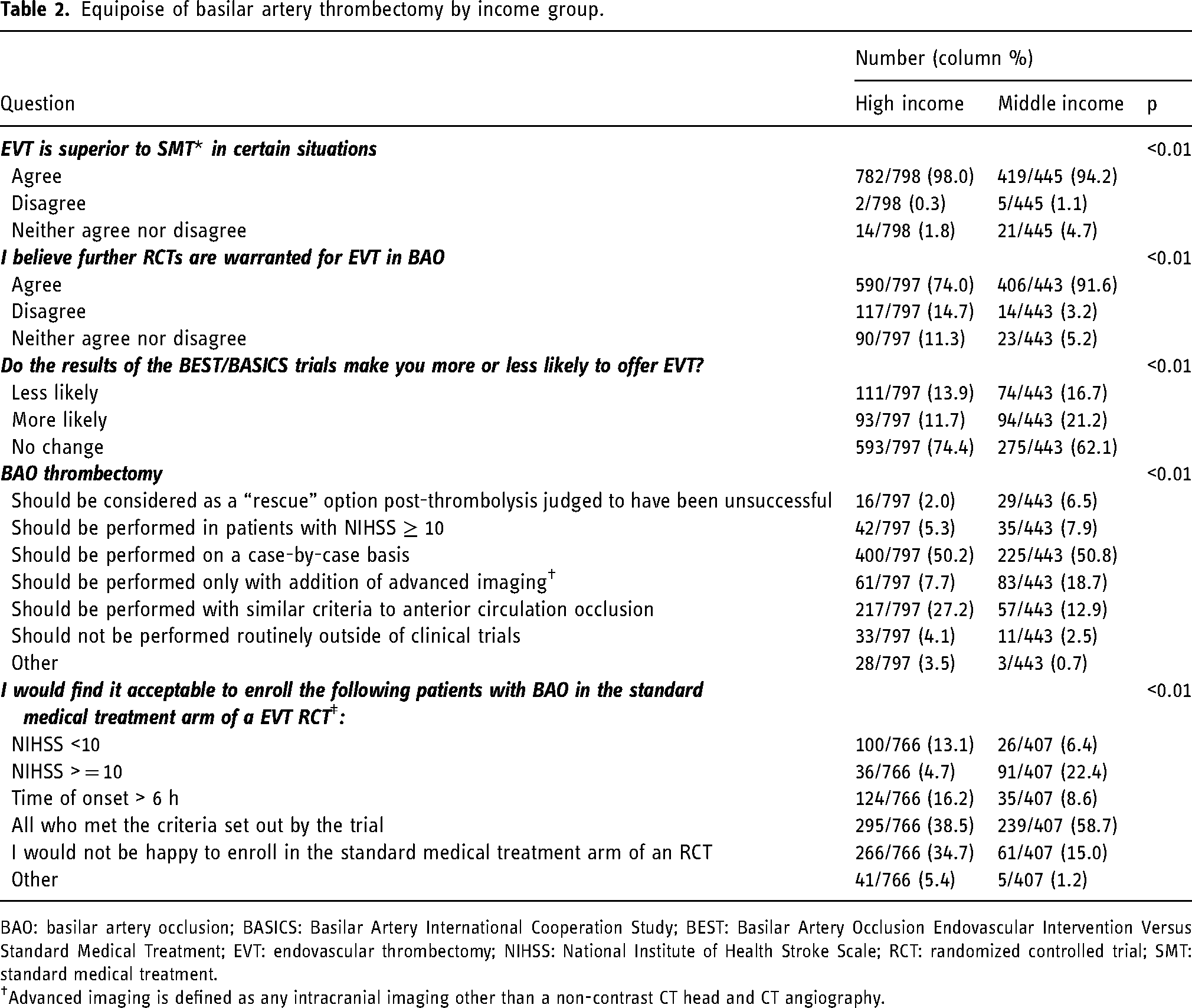
BAO: basilar artery occlusion; BASICS: Basilar Artery International Cooperation Study; BEST: Basilar Artery Occlusion Endovascular Intervention Versus Standard Medical Treatment; EVT: endovascular thrombectomy; NIHSS: National Institute of Health Stroke Scale; RCT: randomized controlled trial; SMT: standard medical treatment.
†Advanced imaging is defined as any intracranial imaging other than a non-contrast CT head and CT angiography.
Respondents from MIC were more likely to select that, if their center were to take part in a RCT for thrombectomy in BAO, they would find it acceptable to enroll all patients who met trial criteria in the SMT arm (58.7% vs. 38.5%, p < 0.01; Table 2).
Imaging selection
Respondents were asked their opinion of using a posterior circulation (pc)-ASPECTS threshold for patient selection to BAO EVT, and respondents from MIC were more likely to favor using a pc-ASPECTS threshold in selecting patients for EVT in BAO (40.2% vs. 29.5%, p < 0.01).
In cases where clinicians felt advanced imaging, defined as any intracranial imaging other than a noncontrast computed tomography (CT) head and CT angiography (CTA) was required to aid in patient selection, respondents from MIC were more likely to select CT-based imaging techniques (CT perfusion or multiphase CT) than their HIC counterparts (39.7% vs. 15.2%, p < 0.01). The most commonly selected advanced imaging technique in HIC was magnetic resonance imaging (MRI) with diffusion-weighted imaging 59.3% vs. 34.2% in MIC (p < 0.01; Table 3).
Clinical and imaging parameters aiding selection by income group.
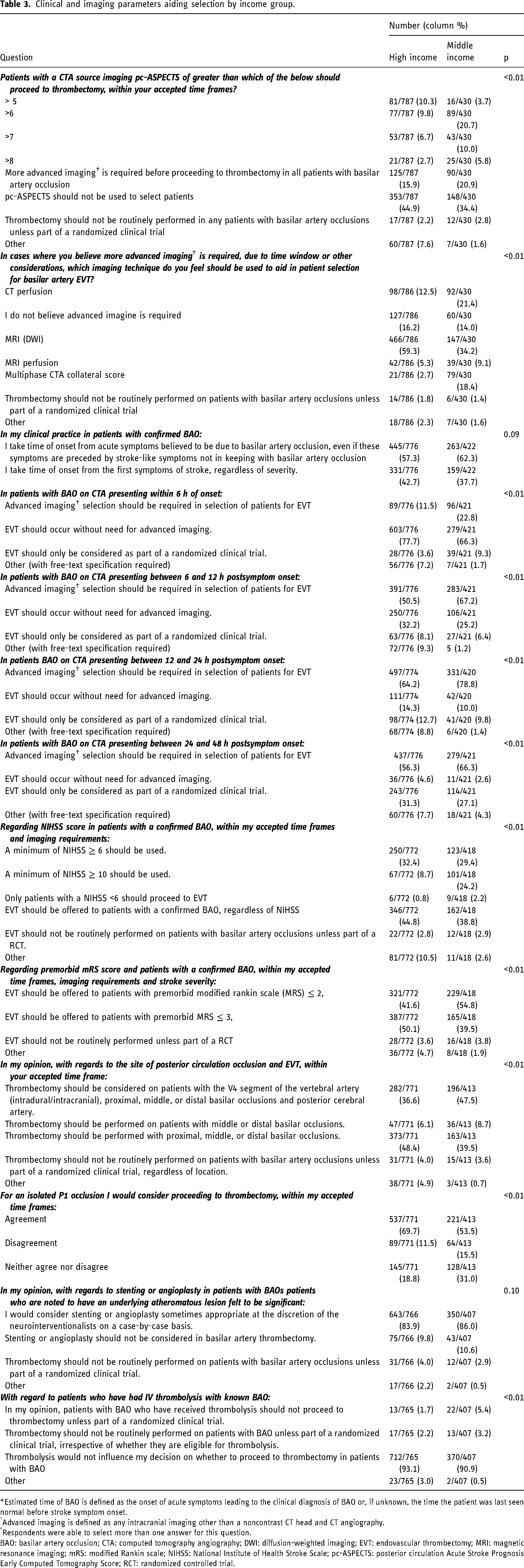
*Estimated time of BAO is defined as the onset of acute symptoms leading to the clinical diagnosis of BAO or, if unknown, the time the patient was last seen normal before stroke symptom onset.
Advanced imaging is defined as any intracranial imaging other than a noncontrast CT head and CT angiography.
Respondents were able to select more than one answer for this question.
BAO: basilar artery occlusion; CTA: computed tomography angiography; DWI: diffusion-weighted imaging; EVT: endovascular thrombectomy; MRI: magnetic resonance imaging; mRS: modified Rankin scale; NIHSS: National Institute of Health Stroke Scale; pc-ASPECTS: posterior circulation Acute Stroke Prognosis Early Computed Tomography Score; RCT: randomized controlled trial.
Timing
Respondents from both groups were more likely to select time of deterioration consistent with BAO (MIC 62.3% vs. HIC 57.3%, p = 0.09), as opposed to time of first symptom as the time of onset in patient selection for EVT in BAO (Table 3).
In the early time window of < 6 h from estimated symptom onset of BAO, most respondents from both MIC and HIC agreed that EVT selection could forego advanced imaging (66.3% vs. 77.7%, p < 0.01). Across all other later time windows surveyed (between 6 and 12 h, between 12 and 24 h and between 24 and 48 h), respondents in MIC were more likely to choose advanced imaging to aid patient selection (MIC 67.2% vs. HIC 50.5%, MIC 78.8% vs. HIC 64.2%, MIC 66.3% vs. HIC 56.3%, respectively, all p < 0.01; Table 3).
Severity
Respondents from MIC were more likely to specify a National Institute of Health Stroke Scale (NIHSS) threshold to stratify patients with BAO stroke for selection to EVT (55.7% vs 41.8%, p < 0.01) whereas HIC respondents were willing to offer EVT to patients with confirmed BAO regardless of NIHSS (44.8% vs 38.8%, p < 0.01).
Respondents from MIC were less likely to offer a thrombectomy to patients with a pre-stroke modified Rankin Scale (pmRS) of ≤ 3 compared to HIC respondents (39.5% vs. 50.1%, p < 0.01), whereas with a pmRS of
Clot location
In cases of occlusions of the first segment of the posterior cerebral artery respondents from MIC were less likely to indicate that they would favor proceeding to thrombectomy (53.5% vs 69.7%, p < 0.01; Table 3). However, they were more likely to consider patients with a V4 segment of the vertebral artery occlusion for EVT (47.5% vs 36.6%, p < 0.01; Table 3).
Procedure-related references
With regard to stenting or angioplasty, the majority of respondents from MIC (86.0%) and HIC (83.9%) advocated its use on a case-by-case basis (p = 0.21; Table 3). Respondents from MIC (90.9%) and HIC (93.1%) did not feel that whether a patient had received thrombolysis would alter their decision on whether to proceed with EVT (p = 0.17; Table 3).
Discussion
This international survey conducted after the BEST and BASICS trial results, but before the publication of the results of the ATTENTION and BAOCHE,2,3 shows significant differences between physicians in HIC and MIC, both in their responses to areas of potential equipoise, as well as in the clinical and imaging parameters used to aid in patient selection.
In recent years many LMICs have increased their proportion of gross domestic product spending on science, technology, and innovation as a way of increasing external investment. 13 The globalization of clinical trials has improved, but overall participation of LMIC in research remains comparatively low. 10 In an area of clinical uncertainty, at the time of the survey, respondents from MIC were significantly more likely to agree that further RCTs were warranted for EVT in cases of BAO and significantly more likely than their HIC counterparts to enroll all patients who met the criteria specified by a trial in a BAO RCT. This was observed despite 94.4% of respondents reporting that they believed EVT was superior to SMT in certain situations, even though EVT in cases of BAO was lacking RCT evidence to support this position at the time. 20
The results of this international survey open the possibilities of increasing involvement of MIC in areas where the high resources, expense, and administrative hurdles in larger systems often experienced in HIC can create barriers to conduct research studies. This is in addition to the many other potential benefits of undertaking research trials in LMICs. This may include decreased operational costs, increased research capacity, availability of treatment naïve patients for recruitment, opportunity for participants to access otherwise unavailable treatments12,21 and a decrease in migration of LMIC researchers to HICs, the so-called “brain drain.” 14
Further expenditure and increased contribution from HICs to official development assistance may be required to drive research growth in LMIC. 16 The symbiotic nature of a research relationship between HIC and LMIC means it is vital that research funding flowing from HIC to LMIC is not cut when pressures on budgets arise. 14 This study highlights the potential benefit to all countries when MIC are included in research studies.
Reasons for the increased willingness to enroll in RCTs in MIC is likely multifactorial but our survey points to access to resources as an important component. Respondents from MIC were significantly more likely to choose CT-based imaging rather than MRI to guide their clinical decision making in BAO than respondents from HIC.22,23 This selection paradigm is further reinforced by the recent positive BAO trials, ATTENTION and BAOCHE, performed in China, which allowed enrollment based on standard and widely available CT imaging.2,3 These findings highlight the importance of research infrastructure and broadening of thrombectomy trial eligibility considerations to improve enrollment of patients from MIC, to improve the generalizability of thrombectomy trial data results not only to patients in HIC or MIC but also to those from LIC. 24 Respondents from MIC were also more likely to favor a stricter mRS cut-off score of <3 than their HIC counterparts in patient selection. MIC respondents were also more likely to use scoring systems, both NIHSS and pc-ASPECTS, to aid patient selection for enrollment. This result may reflect that physicians from MIC, based on available resources, select patients more likely to have better clinical outcomes at the functional and societal level. In patients presenting with isolated P1 occlusions, respondents from MIC were less likely to proceed to thrombectomy compared to those from HIC, underscoring uncertainty in benefit of EVT in patients with medium vessel occlusion of the posterior circulation.25–27
Our study highlights the potential to improve the quality and recruitment of patients to RCTs by increasing participation from MIC. The fact that we had no respondents from LIC is either a reflection of the challenges we faced in recruiting such participants to participate in BAO surveys or a reflection of their limited resources to care for patients with BAO. As we suspect the latter, this disparity highlights the need to improve access to EVT for patients in LIC and MIC, 28 in light of the evolution of anterior LVO and now BAO trial data.
Limitations
This survey captured the opinions of a large and diverse number of physicians involved in stroke care; however as with all surveys, the results should be interpreted with caution. While this survey reflects the reported beliefs of practicing physicians across the globe, these beliefs do not reflect the correct course of action in clinical practice.
As the survey was distributed via national and international organizations involved in stroke care, it may be limited by sampling bias reflective of the participation of physicians involved in such organizations and those who are fluent in English or Chinese.
The survey was conducted before the preliminary results of the ATTENTION and BAOCHE BAO trials were presented at the European Stroke Organization Congress in May 2022. Although the result of these trials would likely have influenced respondents’ answers, in this prespecified analysis looking at differences between MIC and HIC respondents with respect to treatment preference, our study highlights the difference of approach to areas of clinical equipoise between these two country-income strata.
Conclusions
While most physicians globally were in agreement that, in certain circumstances, EVT is superior to SMT at the time of the survey, respondents from MIC were more likely to perceive that further trials were warranted and more likely to express willingness to enroll eligible patients in a BAO RCT than their HIC counterparts.
This difference in approach to an area where clinical equipoise has been called into question without supporting RCT evidence highlights the potential for greater contribution from a wider range of MICs to new research trials.
Footnotes
Abbreviations
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Alemseged reported research grants from Medical Research Future Fund, Australian Heart Foundation, Sylvia & Charles Viertel Charitable Foundation. Dr Fischer reported research grants from Medtronic; consultant for Medtronic, Stryker, CSL Behring; advisory board for Alexion/Portola. Dr Kaesmacher reported grants from the Swiss Academy of Medical Sciences/Bangerter Foundation, Swiss Stroke Society, Clinical Trials Unit Bern, and the Swiss National Science Foundation. Dr Nagel reported consultancy for Brainomix, speaker bureaus with Boehringer Ingelheim and Pfizer. Dr Nguyen reported research support from Medtronic and SVIN. Dr Puetz reported fees as lecturer for Daiichi Sankyo. Dr Sacco reported research grants from Novartis and Uriach; fees for advisor or speaker from Abbott, Allergan-Abbvie, AstraZeneca, Lilly, Lundbeck, Novartis, Novo Nordisk, Pfizer, Teva. Dr Siegler reported consulting from Ceribell and speakers’ bureau with AstraZeneca. Dr Thomalla reported fees as a consultant from Acandis, Alexion, Amarin, Bayer, Bristol Myers Squibb/Pfizer, Boehringer Ingelheim, Portola, and Stryker. Dr Yamagami reported research grants from Bristol-Myers Squibb, lecturer’s fees from Bayer, Daiichi-Sankyo, Stryker, Bristol-Myers Squib; advisory boards for Daiichi-Sankyo. Dr Banerjee reported consultancy for RapidAI. Dr Marto reports consulting fees from Amicus Therapeutics and Boehringer Ingelheim; speaker fees from Boehringer Ingelheim. Dr Kaiser reported grants from the Joachim Herz Foundation and the Else Kröner Fresenius Center for Digital Health.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.