
Abstract
Background
Thoraco-lumbar spinal dural arteriovenous fistulae represent a rare subset of central nervous system vascular malformations. One of the unique features of spinal dural arteriovenous fistulae is their extremely low propensity to cause hemorrhage (either parenchymal or subarachnoid), with a distinct clinical presentation of myelopathy secondary to spinal venous congestion. The exact mechanism for this unique presentation is still unclear.
Methods
Following institutional review board approval, we retrospectively analyzed our prospectively maintained database of spinal dural arteriovenous fistulae and cranial (cr) DAVF cases presenting between 2008 and 2021. For all cases, angiograms were reviewed and arteriovenous transit times were calculated. Patient demographics, angiographic features, and clinical and radiological outcomes were assessed.
Results
In total, 66 patients presenting with confirmed thoracolumbar spinal dural arteriovenous fistulaes were identified and compared to patients presenting with cervical spinal dural arteriovenous fistulaes (n = 10), ruptured crDAVFs (n = 32) and unruptured crDAVFs (n = 20). Mean age in the target group was 66 ± 13 versus 57–62 in the other groups, p < 0.05 on one-way analysis of variance; with 80% males versus 50%–65% in other groups. Mean arteriovenous transit time in the thoracolumbar group measured 1.98 s ± 0.96 versus 0.25–0.5 s range in other groups (p < 0.0001 on one-way analysis of variance).
Conclusion
Prolonged arteriovenous transit times may represent a distinct feature of thoracolumbar spinal dural arteriovenous fistulaes. This may, amongst other factors, play a role in the observed lesser likelihood of hemorrhagic complications compared to other dural arteriovenous shunts.
Introduction
Spinal dural arteriovenous fistulas (sDAVFs) at the thoracolumbar level represent a rare but important cause of myelopathy, frequently leading to irreversible myelomalacia.1–3 The condition has a reported incidence of 1:500,000 with male predominance, peaking in the sixth to seventh decade of life. Etiology of the condition is predominantly idiopathic, with rare cases associated with trauma, infection and thrombosis. sDAVFs are usually supplied by a single dural branch arising from a radiculo-meningeal artery, with drainage into peri-medullary veins. The primary mechanism of myelopathy is thought to be secondary to venous congestion and subsequently decreased arterial perfusion. The main goal of treatment is to obliterate the arteriovenous (AV) shunt either through endovascular or open surgical means to prevent further deterioration.4,5
In contrast to cranial dural arteriovenous fistulas (crDAVFs) and sDAFVs at the cervical level, sDAVFs at the thoracolumbar level virtually never present with hemorrhage (i.e., a subarachnoid hemorrhage or hematomyelia), thus in patients with hemorrhage, alternative diagnoses (i.e., spinal AV malformation or spinal perimedullary AV fistula) are usually suggested.6–12 The reason for this discrepancy is unclear and various theories have been postulated.13,14 One hypothesis proposes a peculiar angioarchitecture of thoracolumbar sDAVFs, with a unique extra-medullary course of draining arterialized veins with a subdural course, typically leading to symptoms of venous congestion rather than a subarachnoid hemorrhage. 15 According to another hypothesis, thoracolumbar sDAVFs are assumed to be slow-flow shunting lesions and thus have a lesser propensity to rupture a vessel wall leading to a subarachnoid hemorrhage and/or hematomyelia,13–15 however this has to date not been quantified in a larger cohort.
In this study, we aimed to evaluate this in our series of thoracolumbar sDAVFs this hypothesis by quantifying AV transit times and compare them to similar AV transit times in cervical sDAVFs as well as in unruptured and ruptured crDAVFs.
Methods
Following institutional ethics review board approval, a retrospective analysis of our prospectively maintained DAVF database was conducted. We analyzed all cases of sDAVF (excluding epidural shunts) that presented to our service between 2008 and 2021 and compared them to a consecutive series of our most recent crDAVFs. We included all patients above 18 years of age, which had a confirmed digital subtraction angiographic (DSA) diagnosis of dural AV fistulae.
DSA was reviewed to quantify AV transit times according to frame per second acquisition rate. Transit time (measured in seconds) was calculated according to the time elapsed between the first appearance of a radicular artery following segmental artery contrast injection, and the first appearance of the arterialized medullary vein or cerebral sinus. An example of transit time calculation based on DSA acquisition is depicted in Figure 1, for spinal and cranial fistulae (1A and 1B accordingly). Given the almost uniform single radicular arterial supply on a single level in the case of sDAVF cases—point zero in spinal angiogram was set at the first appearance of the radicular artery, contrasted to first frame cervical artery injection in crDAVF cases. Additionally, since spinal angiograms in our institution are performed by means of manual injection versus contrast pump injection for crDAVFs the choice of radicular artery appearance as point zero was aimed to neutralize non-uniformity of manual injections. Since frame-per-second acquisition time was not uniform across the scored angiograms—final transit times were calculated according to frame-per-second acquisition rates.
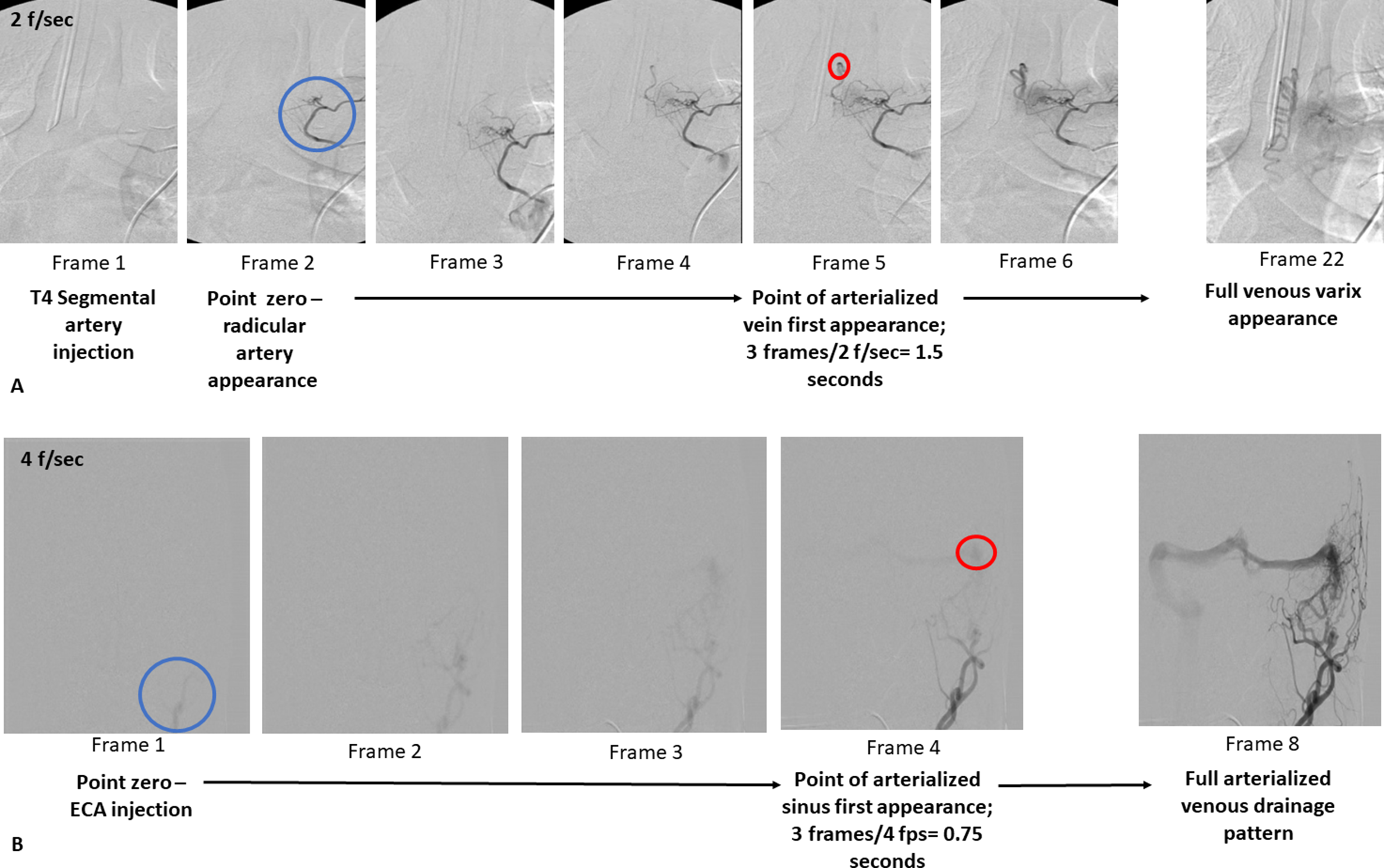
Graphic example for calculation of shunting time for spinal (A) versus cranial DAVF (B). Give the almost uniform single radicular arterial supply on a single level in case of spinal DAVF—point zero in case A is set at radicular artery appearance, as compared to ECA injection in case B. (f/sec—frames per second acquisition rate). DAVF: dural arteriovenous fistulae; ECA: external carotid artery.
Patients’ demographics and clinical presentation, angiographic findings, treatment modality, and clinical outcomes were reviewed and presented as well.
For quantitative analysis, transit times were averaged and presented along 4 distinct anatomical DAVF groups; thoracolumbar sDAVFs, cervical sDAVFs, ruptured crDAVFs and unruptured crDAVFs. Spinal magnetic resonance imaging (MRI) review for quantification was also performed for spinal cord myelopathic involvement and its correlation to transit times.
All the statistical analysis was performed using GraphPad Prism software © (San Diego California), multivariate, t-test and one-way ANOVA tests were utilized. P value for statistical significance was set at < 0.05.
Results
We evaluated a total of 66 consecutive patients with thoracolumbar sDAVFs, 10 patients with cervical sDAVFs, 32 patients with ruptured crDAVFs, and 20 patients who presented with unruptured crDAVFs. Patients with thoracolumbar fistulae significantly differed in terms of mean age and male gender overrepresentation (66 ± 13 vs. 57–62 in the other groups, p < 0.05 on one-way ANOVA; with 80% males vs. 50%–65% in other groups). Thoracolumbar fistulae had significantly longer AV transit times compared to the other groups (1.98 s ± 0.96 s versus 0.25–0.5 s in other groups). Transit times did not differ between crDAVFs and cervical sDAVF patients or amongst the ruptured and unruptured crDAVFs, regardless of clinical presentation, and were uniformly short (Figure 2), specifically below 1.5 s in the ruptured crDAVF group (Figure 2).
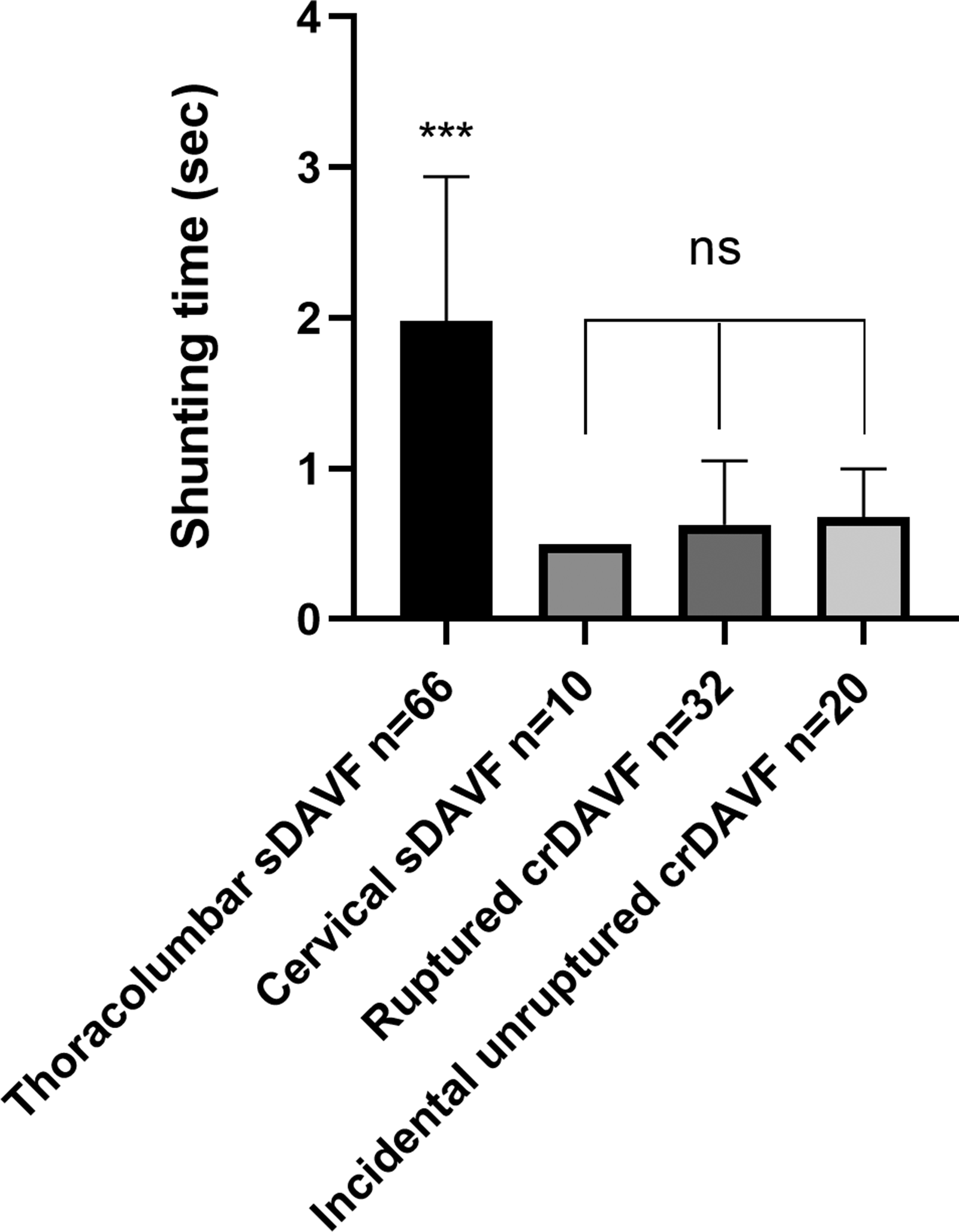
Shunting times analysis of the cohort. Thoracolumbar fistulae exhibit significantly slower shunts compared to other anatomical locations. crDAVF: cranial dural arteriovenous fistula; sDAVF: spinal dural arteriovenous fistula; ns: non significant. *p < 0.05; ***p < 0.001).
Correlation analysis between transit times and the extent of radiographic spinal cord edema or enhancement (quantified by the number of affected levels on spinal MRI) did not reveal a significant correlation.
On a clinical level, all the patients (n = 6) with the shorter thoracolumbar fistulae AV transit times (<1–1.5 s) presented with progressive sensory-motor and/or sphincteric myelopathy accompanied by radiographic myelopathic changes. Whereas clinical presentation of patients with longer transit times varied between mild sensory symptoms to severe myelopathy.
Figure 3 presents selected imaging of representative sDAVF patients according to fistula location and shunting times.
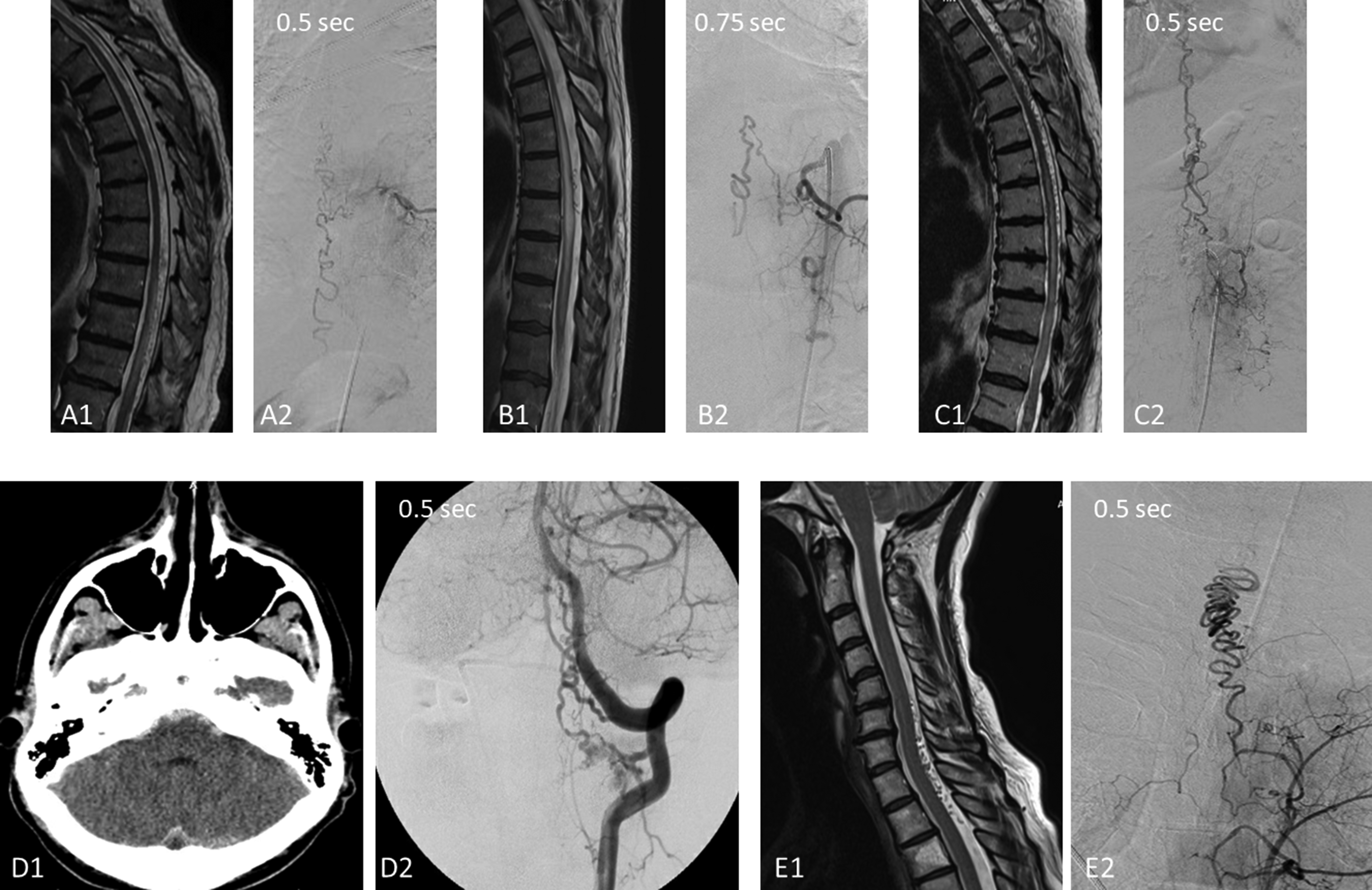
Representative imaging, digital subtraction spinal angiograms and MRI T2 sequences. Thoracolumbar sDAVFs with short shunting times (A–C) present with unquestionable myelopathy and venous varices. Cervical sDAVFs (D–E) can present with either subarachnoid hemorrhage (D) or fast shunting accompanied by a venous varix (E). sDAVF: spinal dural arteriovenous fistulae; MRI: magnetic resonance imaging.
Discussion
Spinal thoracolumbar AV dural AV fistulae have unique clinical features: While crDAFVs and cervical sDAVFs can present with intracranial hemorrhage,16,17 thoracolumbar sDAVFs typically do not. The exact reason for this is a matter of debate. In the few case reports of thoracolumbar sDAVF presenting with hemorrhage, a varix-like draining vein has been demonstrated, presumably secondary to an accelerated AV transit time.6,9–11 Cervical sDAVFs are more commonly present with hemorrhages and up to now their drainage towards the intracranial pial veins had been mentioned as the cause for higher incidences of hemorrhage.18–20
The aim of the current study was to quantify shunting times of thoracolumbar sDAVFs and compare them to cervical as well as unruptured and ruptured crDAVFs. To our knowledge, this is the first systematic angiographic analysis of DAVF AV transit flow. We show a statistically significant difference in transit times between thoracolumbar versus other dural arteriovenous fistulae.
Based on the present data we suggest that a short arteriovenous transit may be a unique feature of cranial and cervical sDAFVs. Exact timing cutoff is difficult to determine since a larger cohort of fistulae would be required
The exact anatomical mechanism for the arteriovenous shunting differences is not clear. A fundamental anatomical difference between spinal versus cranial venous systems is the structure of the dural sinuses. Brain dural venous sinuses are comprised of the dura mater with a monolayered epithelium, while spinal intradural veins have a typical three-layered venous morphology. 21 Moreover, cranial dural venous sinuses are at least partly engulfed by bony skull structures, and typically represent larger diameter venous routes. At least in the standing position, the intracranial venous pressure is likely lower compared to the venous pressure of the spinal veins, thus leading to a larger arteriovenous pressure gradient and subsequently fast shunting. Also, morphological differences such as different resistance and elasticity properties of cerebral versus spinal venous systems may contribute to different arteriovenous shunting times. Brain dural venous sinuses are low resistance, low elasticity large straight vessels, whereas spinal veins are long, elastic, and present with higher resistance networks of small vessels. Hence, in terms of flow dynamics, highly pressurized arterial blood can maintain its high flow velocity in its transition in the dural sinus, with the expense of subsequent pressure drop, while in the transition to a spinal vein, the high downstream resistance brings about a rise in venous pressure and thus a decrease in flow velocity. In cases of cervical sDAVFs, the decreased static venous pressure and the distal drainage into the cerebral sub-arachnoid space—creates a similar high-flow outlet thus creating an early high flow with high resistance and thus a higher risk for bleeding. 18 To support this, in our series a case of high thoracic DAVF presenting with fast cervical venous drainage was accompanied by a fast shunting transit. This concept is depicted in Figure 4. According to this hypothesis, at the time of diagnosis a slow flow shunt is present in sDAVFs. The rare instances of high flow may be related to venous dilatation and thus a lower outflow resistance which may present in long-standing fistulae with gradual venous dilatation, varix formation, and hemodynamic shift toward low pressure-high flow shunts. Based on these findings, we suggest that shunting transit time may be considered as an additional risk factor for dural AV shunts and added to the current treatment decision-making paradigm. 22
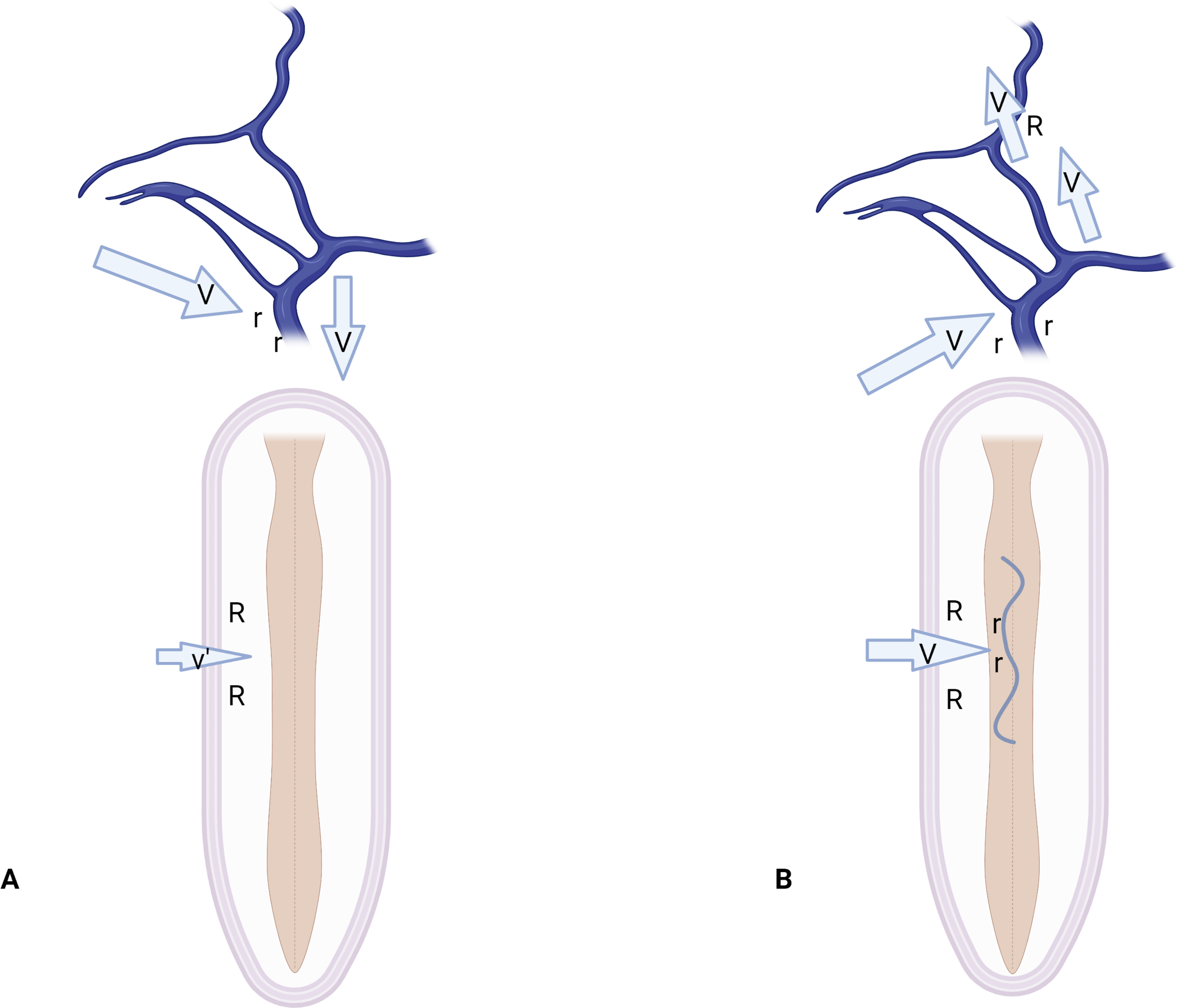
Proposed mechanism of venous shunting in spinal and cranial DAVFs. In crDAVFs (A, B). In typical sDAVFs (A) high inflow resistance (R) leads to prolonged shunting and slow flow (v'), and in cases of further reflux into cortical veins in crDAVFs (B) low resistance (r) leads to fast inflow into a high resistant cortical veins (R) and subsequent breakthrough bleeding. In selected thoracolumbar sDAVFs or cervical sDAVs(B) low inflow resistance of the venous varix (r) leads to shorted shunting times and high flow (V). Prepared with assistance of BioRender ©. sDAVF: spinal dural arteriovenous fistulae; crDAVF: cranial dural arteriovenous fistulae.
Another plausible hypothesis is one of a shunted blood flow direction, well illustrated in cases of cervical sDAVFs. According to previously published observations,23–26 a direction of the venous reflux in the case of cranio-cervical junction dural AV fistulae was an important angiographic marker of fistulae pathophysiology. In cases of cerebral reflux, flow into low-resistance venous cerebral space results in fast transit, varix formation, and subsequent rupture. Whereas in instances of thoracic spinal reflux, given a lower number of venous outlets with higher resistance to flow, a slow transit is created with long-standing generation of venous congestion leading to myelopathy.
A major limitation of our study is a non-uniform image acquisition, non-uniform contrast injection and lack of angiographic and clinical data to allow standardization of analysis leading to a rather simplistic evaluation resulting in only approximation of venous shunting transit velocity. These factors are addressed in Table 1 and should be of use for future prospective study design. Nevertheless, the simplicity of the proposed method allows a rapid and readily available analysis of DAVF without requiring sophisticated imaging modules or software. In addition, the significant difference between the two groups can not be explained solely by differences in frame rate or contrast injection techniques.
Potential variables affecting transit time and velocity calculations, consideration of which should be implemented in future prospective and controlled studies.
Another limitation of our study is its retrospective nature and a lack of a robust anatomical surrogate marker that would be able to add structural value to the suggested hemodynamic hypothesis. Additionally, the connection between prominent venous arterialization and severe clinical course in sDAVF had been already pointed out. 27 However, this is the first comprehensive and systematic angiographic analysis of a large cohort of sDAVFs that sheds additional light on this intriguing pathology mechanism.
Conclusions
Thoracolumbar sDAVFs present with significantly longer arterio-venous transit times, while shorter transit time may be associated with a worse clinical course. Hence, we propose an additional hemodynamic feature of sDAVFs, that has the potential to explain the unique clinical and radiological behavior of sDAVF, future anatomical studies are warranted to further strengthen this finding.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.