
Abstract
Endovascular treatment (EVT) for large vessel, acute ischemic stroke in children remains a subject of debate, with evidence for its benefits derived from case series and individual case reports. At present, guidelines are cautious in recommending EVT for children under 5 years of age, mainly due to a lack of data and incomplete cerebral and femoral vessel development. However, based on the small number of cases reported in the literature, EVT appears to be safe and effective for pediatric use and arterial diameters can accommodate currently available devices. Available evidence shows that in patients with a normal arterial development, a 6-Fr femoral approach can be safely used by 2 years of age. We describe the case of a 2-year-old child who benefited from late-window EVT for a basilar occlusion. The procedure was safely performed using a 6-Fr femoral introducer, a 6-Fr guide catheter, and a 5-Fr aspiration catheter. We discuss also normal cerebral and femoral vessel development, providing descriptive tables of compatibility between femoral and cerebral arterial diameters by age groups and currently available endovascular devices.
Keywords
Introduction
Endovascular treatment (EVT) for acute ischemic stroke is currently one of the main pillars of reperfusion treatment in adult patients with large vessel occlusion.1,2 Notably, large vessel occlusion is also present in nearly one-quarter of pediatric stroke patients. 3 However, current pediatric guidelines do not provide strong recommendations for thrombectomy, mainly due to a lack of evidence, and they even state that EVT should probably be reserved for “larger children due to concerns about introducing catheters into small groin- and cerebral arteries.” 4 Nevertheless, despite the lack of high-quality evidence, some retrospective pediatric case series have shown encouraging clinical and radiological results of mechanical thrombectomy in the pediatric population. In a single-arm, retrospective study including 73 pediatric stroke patients treated with EVT, a favorable neurological outcome (modified Rankin Scale score of 0–2) was obtained in 87% of cases. 5 Similarly, a recent meta-analysis demonstrated favorable outcomes in 90.6% of 113 pediatric stroke patients treated with EVT. 6 While these high rates of a positive outcome vastly outperform results obtained in adult patients and are probably due to selection bias, a recent prospective cohort study identified a good functional outcome at three months in 50% of EVT-treated children compared to 27% in children who were offered conservative treatment. 3
The most significant two pediatric EVT series mentioned above reported less than 30 cases of thrombectomy in patients ≤6 years old, with even lower numbers in younger children.5,6 To complement the small number of cases of EVT described in children ≤6 years old, as well as the position of the American Heart Association/American Stroke Association guidelines regarding this topic, 4 we describe a case of a 2-year-old child with a basilar occlusion treated with EVT. Following a thorough review of the published literature reporting on the development of arterial diameters by age groups, we provide also detailed tables comparing the size evolution of femoral and cerebral vessels and the diameter of the most commonly used neuroendovascular materials.7–9
Case report
A 2-year-old, male child with normal development and no past medical history presented an episode of loss of balance and altered consciousness at 10h00, which was initially mistakenly interpreted as a seizure by the emergency medical team. He was weighing 15 kg and his height was 92 cm. He was hemodynamically stable, afebrile and was brought to a primary care center. The initial physical examination showed intermittent left-sided hypertonia, intermittent clonic movements, right-sided paresis, symmetric pupils with diminished right-sided photo-motor reflex and flexor plantar reflexes and the pediatric NIHSS was coted at 29 points. The initial non-contrast-enhanced computed tomography (CT) scan was interpreted as normal and the blood work-up was unremarkable. A suspicion of seizure was raised, and he was treated with clonazepam. Following a further episode of impaired consciousness, he was intubated, and brain magnetic resonance imaging (MRI) was performed. The MRI performed at 13h06 showed DWI-positive cerebellum and thalamic lesions, together with a basilar artery (BA) occlusion.
The comprehensive stroke center was alerted at 14h30, and the patient arrived 3 h later. Given the young age of the patient and the high chance of important disability associated with medical treatment alone in basilar occlusion in children, a decision was taken to undergo mechanical thrombectomy if a repeated MRI did not show irreversible pontine lesions. The repeated MRI (Figure 1A, B) showed stability of the ischemic lesions and occlusion so EVT was tempted. Symptom onset to groin puncture time was 8 h.
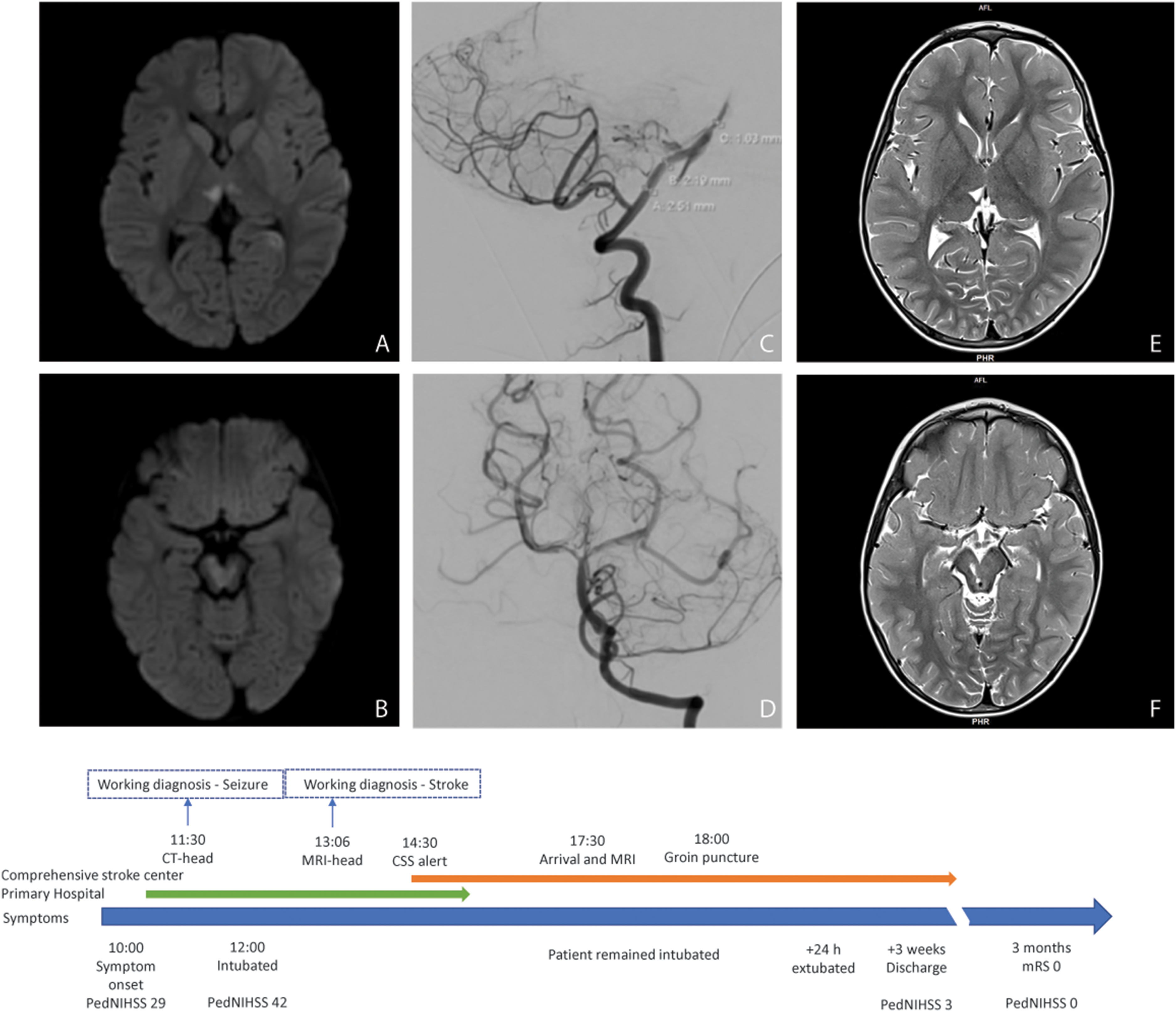
Patient timeline and initial diffusion weighted magnetic resonance imaging showing restricted diffusion at the level of the thalamus (A) and midbrain bilaterally (B). Digital subtraction angiography showing initial occlusion and vessel diameters (C) and final result (D). Follow-up FLAIR imaging at 6 - months showing residual sequelea at the level of the thalamus (E) and midbrain (F).
The common femoral artery (CFA) was explored under echo and measured approximately 4 mm in diameter. A 6-Fr 7 cm radial introducer (Radiofocus, Terumo Europe N.V., Leuven, Belgium) was placed into the right CFA. Access to the left vertebral artery was gained using a 6-Fr 95 cm guide catheter (Chaperon MP2, Microvention, Tustin, CA, USA) (Figure 1C). Once cervical access was secured, a 5-Fr 125 cm distal access catheter (Sophia, Microvention, Tustin, CA, USA) was advanced on a 0.014’’ 200 cm guidewire (Synchro Standard, Stryker, Salt Lake City, UT, USA) and a 0.017’’ 150 cm microcatheter (Headway, Microvention, Tustin, CA, USA) just before the thrombus. After the first passage of manual aspiration, the BA was recanalized, but the right P1 segment was occluded by a thrombus. A second pass aspiration with a SOFIA 5-F was unsuccessful and a 3 × 20 mm pREset LITE stent retriever was combined with manual aspiration through the 5-F catheter, obtaining a complete recanalization (Figure 1D). Manual compression of the femoral puncture site was performed at the end of the procedure. The patient was transferred to the pediatric intensive care unit where he progressively recovered. At discharge, after 3 weeks, he presented a slight divergent strabismus of his right eye and a slight left-sided hemiparesis. At 3-month follow-up, the patient was fully recovered without neurological sequelae. After extensive stroke workup, which included transthoracic echocardiography with bubble contrast test, regular laboratory tests, and: antiphospholipid antibodies (lupus anticoagulant, anticardiolipin, and anti-β2-glycoprotein), protein C and S, activated protein C resistance, antithrombin III antibodies, homocysteine levels, antineutrophil cytoplasmic antibodies, anti-nuclear antibodies, complement proteins (C3, C4, CH50), immunoglobulins assay (IgG, IgA, IgM), varicella titer, genetic testing (COL4A1, COL4A2, COLGALT1, methylenetetrahydrofolate reductase, and CECR1/ADA2 genes), no stroke etiology was found. The final diagnosis was an ischemic stroke of undetermined cause. Follow-up imaging at six months showed minor sequela in the thalamus and pons (Figure 1E, 1F).
Discussion
Thrombectomy procedures in small children remain a subject of debate. 4 A recent review of 11 cases of thrombectomy in children <5 years of age showed that the procedure was feasible, without significant safety concerns, and with better recanalization in the posterior circulation compared to the anterior circulation (80% vs. 43%). 10 Although the median age in this series was 2.1 years, the youngest thrombectomy reported in the literature was a basilar occlusion successfully treated at 14 h after birth with two passes of a 3 mm stent retriever. 11 Unlike our case, children in this age group usually do not have normal development and frequently suffer from congenital cardiac problems.10,12
Due to diagnostic challenges, the timely identification of pediatric patients suitable for reperfusion therapies is challenging. Most high-volume centers expect to perform <3 childhood thrombectomies per year, with 64% performing thrombectomies after 6 h, despite setting up pediatric stroke protocols in their hospitals. 13 For example, 30% of patients included in the Save ChildS study underwent thrombectomy in the 6–24 h time window. 5 In this subgroup, cerebral vasospasm was the only encountered complication. In addition, there were no symptomatic intracerebral hemorrhages and outcomes were better than in the DAWN and DEFUSE-3 trials. 14 In our case, door-to-groin puncture time was achieved at least 8 h from symptom onset, and the patient had an excellent functional outcome, despite infarction already present in the mesencephalon and thalamus before thrombectomy (Figure 1A).
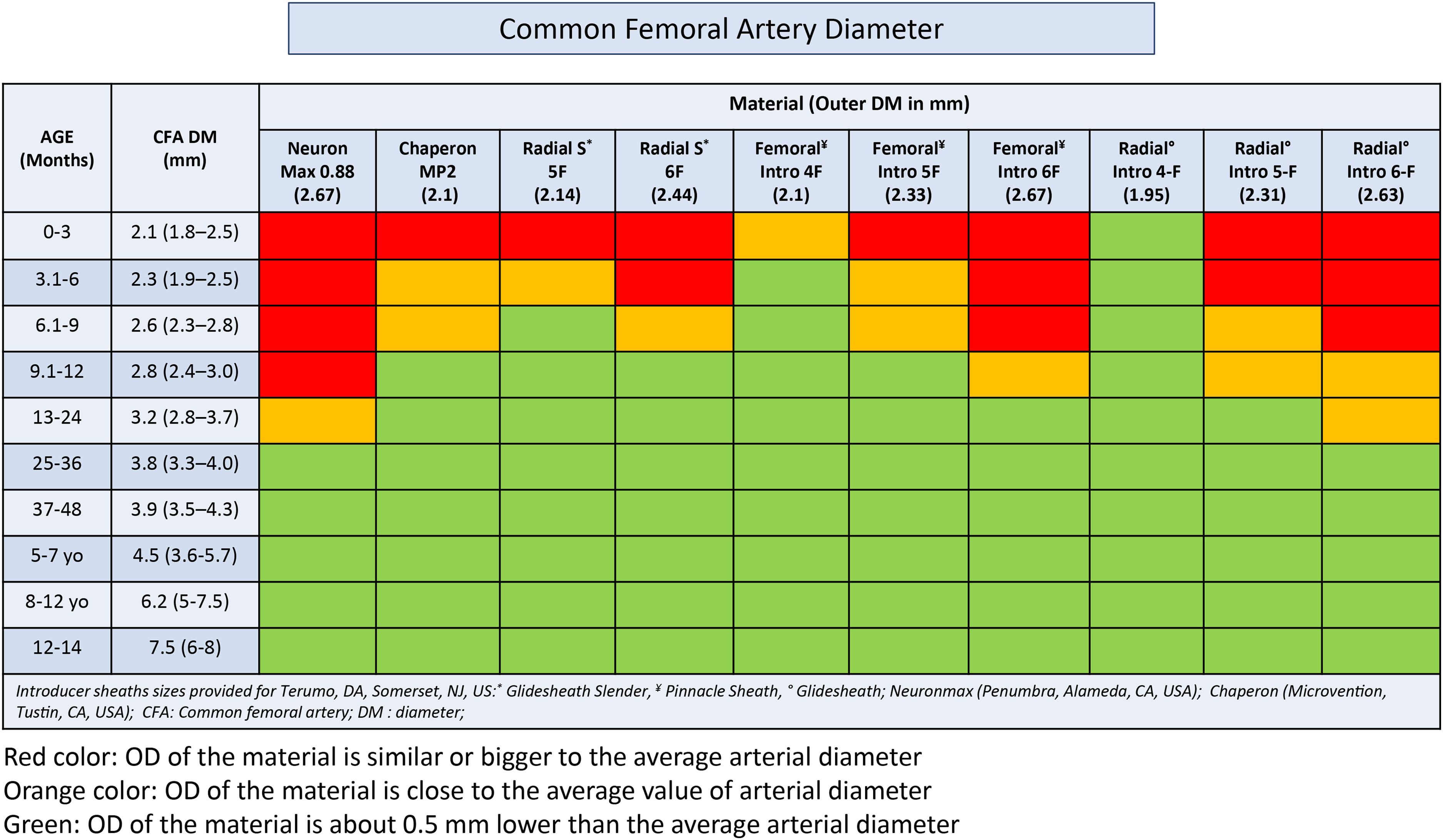
The main challenge of endovascular procedures in children is the size of the femoral and brain and neck arteries. Nomograms of femoral and cerebral artery diameters help to plan emergency endovascular procedures in children. Palpation techniques cannot assess the level of bifurcation of common femoral arteries in children and puncturing below the bifurcation point raises the risk of inadvertent complications. For this reason, echo-guided puncture should strongly be considered in this population. 15 The risk of femoral artery complications increases with punctures in arteries less than 3 mm. Based on currently available normograms, this diameter is attained in most patients by 1 year of age. 16 Moreover, femoral artery diameters are strongly correlated with height, and children over 110 cm usually have a median diameter greater than 3 mm. 8 Based on currently available data, we have produced a chart to show the compatibility between different catheters and introducers and common femoral artery diameters based on age.7,8,17 Figure 2 shows that at 5 years of age, the mean CFA diameter is very close to the adult diameter. 18 In general, until the age of 6 months, the average CFA diameter is approximately 2.3 mm and a 4-Fr radial introducer should be preferred. At 1 year of age, an average CFA may safely accommodate a 6-Fr introducer.
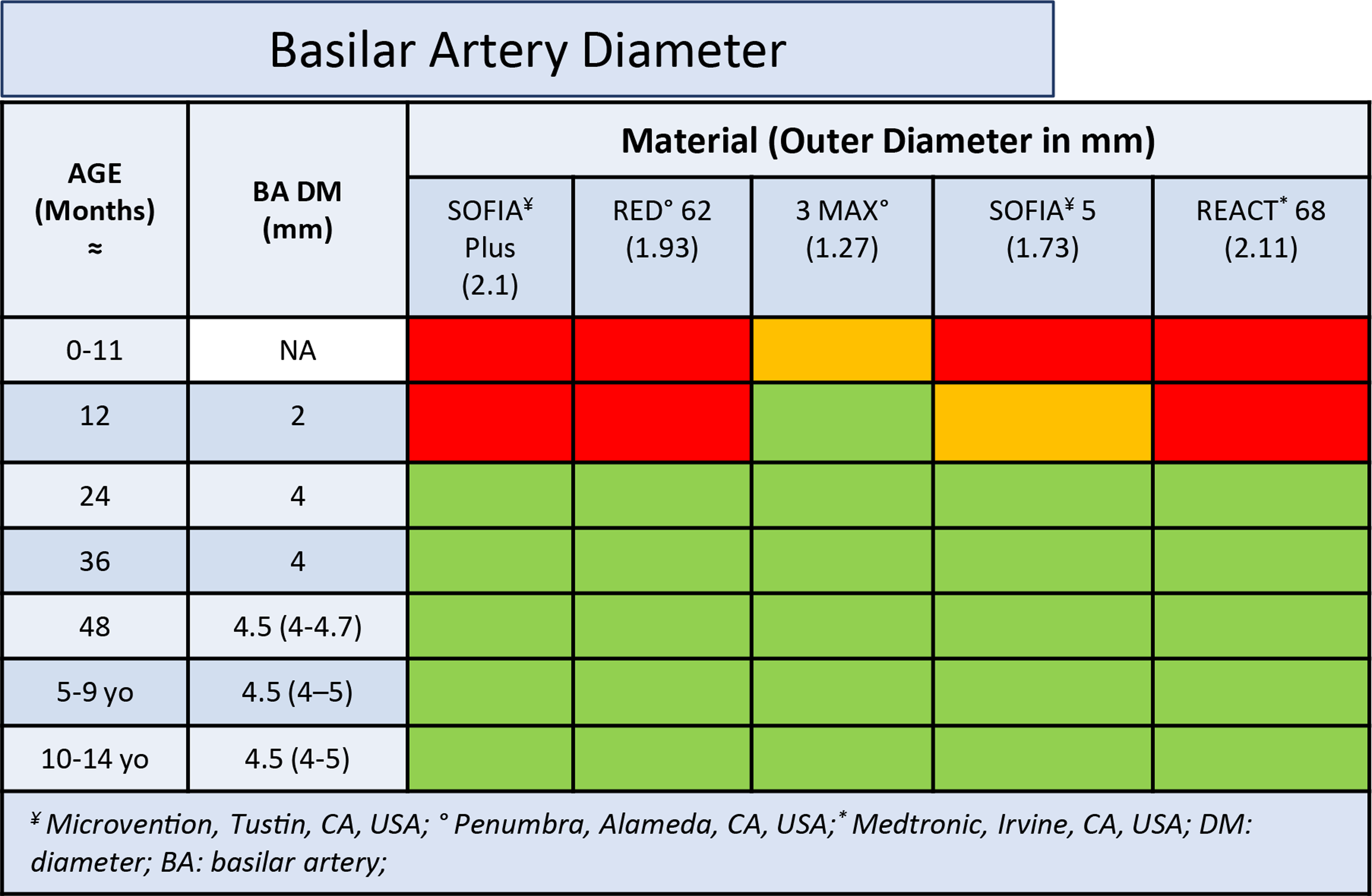
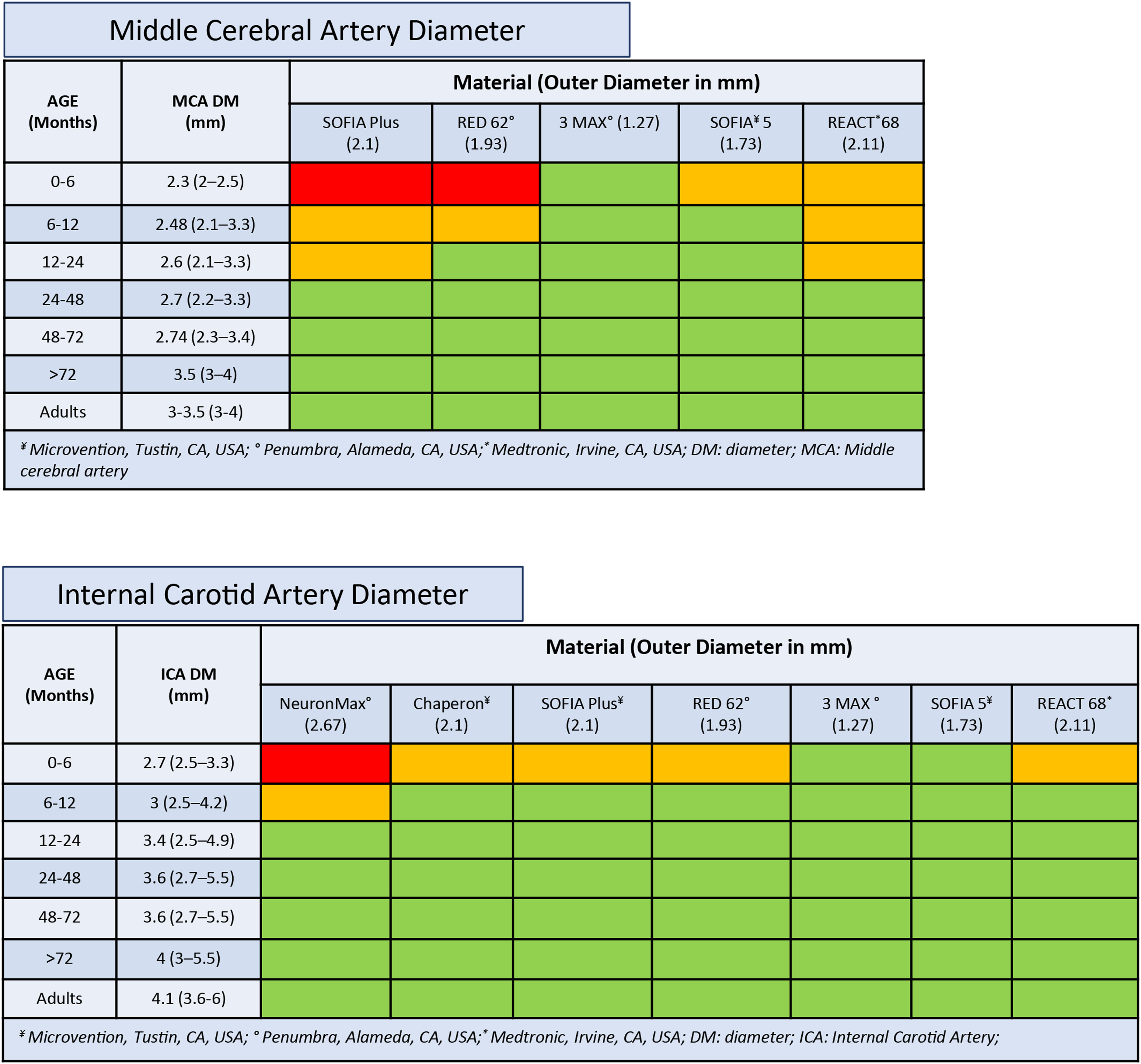
As for femoral artery diameters, a detailed knowledge of expected cerebral artery diameter sizes is crucial to safely perform thrombectomies in children and a personalized measurement of artery size can be done on available pre-procedure, diagnostic imaging (time-of-flight MRI or CT angiography). However, knowledge of the evolution of the cerebral arterial diameter by age may help in the decision-making process in order to assess the feasibility and safety of the endovascular procedure based on patient age. In contrast to the iliac artery, which reaches 60% of the average adult diameter by 2 years of age, all segments of the internal carotid artery (ICA) circulation already reach 81–99% of the adult diameter by 2 years, with the middle cerebral artery size attaining 87% of the adult size in the first 6 months of life. 9 Moreover, cerebral vessel diameter changes minimally after 5 years of age. Similar to the anterior circulation, the BA reaches the average adult diameter by 2 years of age. It is expected to measure around 2 mm at 1 year of age, thereby capable of accommodating smaller intracranial aspiration catheters and stent retrievers. 19 In Figure 3 provides BA and Figure 4 provides MCA, ICA diameters by age and their compatibility with currently used catheters. In general, up to 1 year, the ICA may accommodate all guiding catheters <2.2 mm outer diameter. At 2 years of age, the average diameter of the ICA is >3 mm and a larger catheter, such as the NeuronMax (Penumbra Inc, Alameda, CA, USA), can be safely used. The MCA and BA can be safely catheterized with a 5-Fr distal catheter until 1 year of age, while at 2 years, 6-Fr catheters are allowed.
Data on artery size and device compatibility are limited to a few published series and our work provides additional information for the choice of the endovascular material. However, given the apparent safety and significant functional gains expected from EVT in childhood stroke, thrombectomy should not be contraindicated, considering that most of the available neurocatheters are compatibles with the arterial diameter in the pediatric population.
In conclusion, our experience brings additional insights about the compatibility of endovascular catheters to access arterial vessels in pediatric patients presenting with a stroke associated with large vessel occlusion. Knowledge of age-related arterial diameters is crucial to select the most appropriate material in pediatric stroke cases.
Footnotes
Authors’ contributions
All authors made substantial contributions to the conception, design of the study, acquisition or analysis, and interpretation of the data.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This work did not require ethical approval. Written informed consent was obtained from the parents of the patient presented herein.