
Abstract
Background
Perforator aneurysms of the basilar artery (PABA) are rare causes of subarachnoid haemorrhage (SAH) and challenging to diagnose. We present two cases of SAH caused by PABA diagnosed by cone beam computed tomography angiography (CBCTA) and a novel non-invasive method – 7T magnetic resonance imaging (7T MRI).
Methods
Two patients with SAH, diagnosed with PABA, were imaged on day 9 and 13 after onset, respectively, with CBCTA and 7T MR angiography (MRA) performed on the day after and at follow-up at 3 months.
Results
All four 7T MRI examinations in the two patients were technically successful with fully diagnostic images. No endovascular treatment was performed and control with 7T MRA at 3 months showed no remaining aneurysms.
Conclusion
PABA can be imaged with 7T MRI – a novel non-invasive method, allowing non-invasive follow-up to monitor this rare cause of SAH.
Keywords
Introduction
Perforator aneurysms of the basilar artery (PABA) are rare vascular intracranial pathologies that may cause subarachnoid haemorrhage (SAH). It was first described by Ghogawala et al., 1 and since then case reports, literature reviews2,3 and systematic review 4 have been published. Different treatment options for PABA have been suggested,5,6 and there is still a controversy concerning surgical, endovascular or conservative treatment since the natural history of PABA is largely unknown.
Recently, new methods for detailed vascular imaging of very small intracranial vessels have been developed and offer new possibilities for invasive and non-invasive vascular imaging. We present two cases of PABA imaged with the latest generation of invasive cone beam computed tomography angiography (CBCTA) as well as 7T magnetic resonance imaging (7T MRI).
Our initial experience from these cases suggests that non-invasive 7T MR angiography (7T MRA) may provide a non-invasive and non-ionizing alternative to images of these very small vascular abnormalities.
Methods
Digital subtraction angiography
Digital subtraction angiography (DSA) and CBCTA images were obtained during diagnostic neuroradiological examination using the Siemens Healthineers ARTIS icono biplane platform (Siemens Healthineers ARTIS icono, Siemens Healthineers, Erlangen, Germany), and images were reviewed and processed using the ARTIS software (ARTIS icono VE20 software), including 3D renderings.
Magnetic resonance imaging
MRI was performed using an actively shielded 7T MRI unit (Philips Achieva, Best, The Netherlands) with a dual channel transmit, 32 channel receive, head coil (Nova Medical, Wilmington, MA, USA). Dielectric pads were placed over the temporal lobes to increase the transmit efficiency in these areas (Multiwave Imaging, Marseille, France). No cardiac gating was used.
The imaging protocol included a whole-brain 3D T1 weighted fast gradient echo sequence, 1 mm3 resolution, used to position the MRA imaging volume over the location of the arteries. The 3D time-of-flight (TOF) MRA covered 42 mm axially with a spatial resolution of 0.25 × 0.25 × 0.35 mm3, scan time 4:57 min. After the first TOF MRA scan, a bolus of gadolinium contrast agent (Gadoteric acid 0.5 mmol/ml, Dotarem®, Gothia Medical, Sweden) was injected. After waiting for 5–10 min, the TOF MRA was repeated. If a PABA was present, it could be seen in both the pre- and post-contrast TOF MRA images but was better visualized in the post-contrast images.
Patients
Two patients identified by DSA following SAH during 2021 are constituting the patient material.
Patient 1
Patient 1 is a 67-year-old man with hypertension and a sudden thunderclap headache the day before (day 0). Computed tomography (CT) of the head showed SAH mainly located in the quadrigeminal cistern and posterior fossa. Computed tomography angiography (CTA) in the emergency phase (day 1) did not show any aneurysm, and a DSA was performed the same day, also with no aneurysm shown. 3D angiography was not performed on the first occasion, due to limited cooperability of the patient. The patient recovered slowly and on day 9, a new DSA including CBCTA was performed. A small PABA was found, incorporating the origin of a perforator artery. The day after (day 10) an MRI on 7T was performed, including 3D TOF MRA before and after intravenous contrast (i.v.) agent (16 ml, Dotarem®, Gothia Medical, Sweden), which clearly demonstrated the aneurysm. No endovascular treatment was performed. The patient recovered and was discharged to his home. Three months after discharge, a follow-up 7T MRA was performed, without any remaining aneurysm.
Patient 2
A 54-year-old woman with a history of cigarette smoking, diabetes mellitus, hypertension, hypothyroidism, psoriatic arthritis and gastric bypass surgery presented with sudden onset of thunderclap headache and clinically Hunt and Hess 3. CT showed a peri mesencephalic SAH, hydrocephalus and CTA did not show any aneurysm. A DSA was performed (day 1), which did not identify any aneurysm. Also, in this case, 3D angiography was not performed on the first occasion, due to limited cooperability of the patient. The patient got a temporary ventricular drainage, and she recovered within one week, except lingering headache. On day 13, a second DSA was performed, including CBCTA, revealing a PABA, incorporating the origin of a perforator artery. The next day (day 14) a 7T MRI, 3D TOF MRA before and after i.v. contrast agent (20 ml Dotarem®, Gothia Medical, Sweden) showed the PABA. The patient recovered and was discharged to her own home. Three months after discharge, a second 7T MRA was performed, without any remaining aneurysm.
Discussion
Perforator aneurysm of the basilar artery (PABA) is a rare cause of SAH, with largely unknown incidence and prognosis. In the literature, there are examples of successful endovascular treatments7–9 as well as conservative management.10–12 Conservative management warrants repeated follow-up imaging to ensure that the aneurysm is obliterated 13 or grows over time – in the latter case, active endovascular treatment may be considered. Generally, a non-invasive imaging alternative is preferred for such repeat follow-ups to minimize the risk and nuisance of repeated invasive DSA examinations.
We present two patients with SAH caused by PABA. Both were not diagnosed at the first DSA within one day of onset, which is consistent with other reports.9,14 However, in both cases, CBCTA could not be performed due to the inability of the patient to comply. Instead, the PABAs were diagnosed on follow-up DSA including CBCTA with the latest generation biplane neuroradiological angiosystem, on day 9 and 13 after onset, respectively. If CBCTA had been performed in the acute phase, the PABAs perhaps would have been detected, owing to the high spatial resolution 15 and the possibility of multiplanar reconstructions that may aid in the visualization. However, Buell et al. 10 presented nine SAH patients with PABA of which seven were not seen on the initial angiogram, but instead diagnosed on a repeated DSA, similar to our patients.
In both cases, the first 7T MRI with gadolinium-enhanced TOF MRA was performed on the day after diagnosis was made by DSA, which minimizes the influence of any change of the PABA due to natural progress/regress of the disease. A follow-up 7T MRA was performed in both patients at three months, showing no residual aneurysm and none of the patients had a rebleed. Radojewski et al. 16 have shown the benefit of 7T MRI for improved visualization of small unruptured intracranial aneurysms (Figure 1).
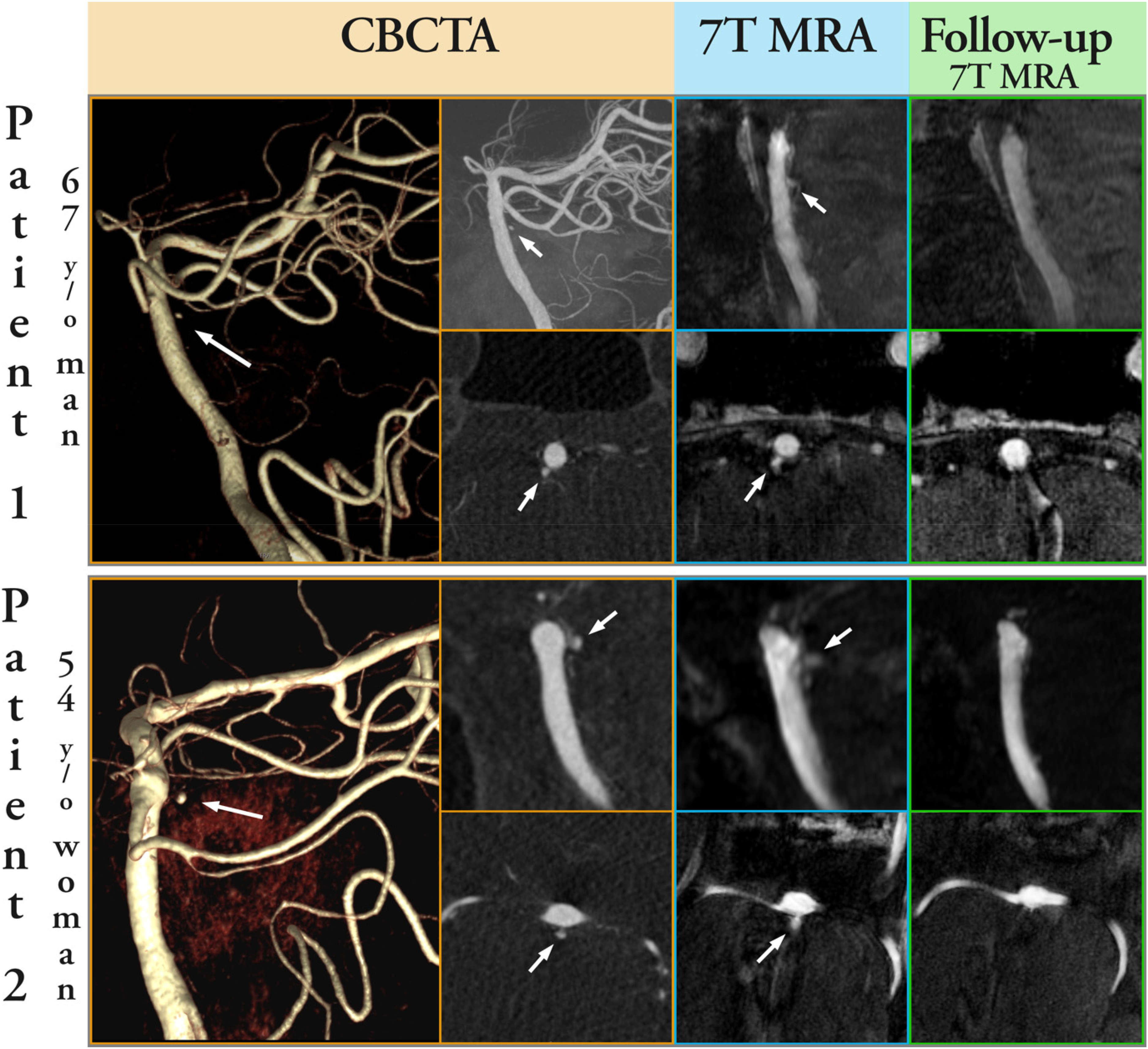
Images illustrating the PABAS in patient 1 (top row), aneurysm size one millimeter in diameter, and patient 2 (bottom row), aneurysm size 1.5 millimeter in diameter, including 3D rendering, sagittal and transaxial MIP images from cone beam computed tomography angiography (CBCTA) in the angiosuite at repeated digital subtraction angiography (DSA) (yellow frame), 7T magnetic resonance angiography (MRA) after Gd-contrast ToF the day after PABA had been confirmed by DSA (blue frames) and follow-up Gd-contrast ToF 7T MRA after 3 months showing no remaining aneurysm (green frames).
7T MRI has several benefits for neurovascular imaging in particular TOF MRA. 17 A higher field strength directly gives a higher signal-to-noise ratio, which allows for higher spatial resolution. In addition, several MRI image contrasts are enhanced at 7T fields as compared to 3T. Of relevance for TOF MRA is that the longitudinal relaxation times, T1, of tissues are prolonged with increased field strength. This gives a stronger inflow enhancement, and results in better suppression of signal from brain tissue and cerebrospinal fluid. 18 In combination with a higher spatial resolution, these effects allow for imaging of smaller arteries and aneurysms compared to at 3T. 19 It is also shown that phase-contrast MRA at 7T has the potential to be a useful tool in neurovascular diseases. 20 Due to the strong inflow enhancement, 3D Magnetization Prepared Gradient Echo sequences (MPRAGE or versions thereof) can also be used for MRA at 7T. 21 On the other hand, imaging of small veins as well as haemorrhages benefits greatly from the shorter T2* relaxation times and the greater susceptibility effects at higher field strengths. This gives a high image contrast in, for example, T2*-weighted imaging, susceptibility-weighted imaging and quantitative susceptibility mapping. However, the same effects also can cause areas of signal loss and geometrical distortions around air-tissue interfaces. The gradient echo sequences used for TOF MRA and all types of T2* based methods are less effected by the inhomogeneous RF-fields typical for 7T, but areas such as the temporal lobes and the cerebellum can suffer from signal loss. 18
Conclusion
Perforator aneurysms of the basilar artery are rare causes of SAH. They can be diagnosed with a non-invasive method such as MRI angiography, especially 7T, and the follow-up examination can be non-invasive.
Footnotes
Authors’ contribution
BR, JW and KMB contributed to the study conceptualization, study design, and data analysis. BR, BH and KMB contributed to data collection. BR wrote the first draft and all authors revised the manuscript. All authors have approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was regarded as quality surveillance and the need for ethical permission and informed consent was waived by the Swedish Ethical Review Authority.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.