
Abstract
Background
The occurrence of persistent intra-device filling (BOSS 1, using the Bicêtre Occlusion Scale Score (BOSS)) in aneurysms treated with a Woven Endobridge (WEB) device is infrequent based on angiographic follow-up. To date, three monocentric case series were published studying BOSS 1 cases. Through a multicenter retrospective study, we aimed to report the incidence, and risk factors of intra-WEB persistent filling.
Methods
We reached out to European academic centers that treat patients using WEB devices and requested de-identified data of patients treated with a WEB device and underwent angiographic follow-up, at least 3 months after embolization, to assess the BOSS 1 occlusion score. We compared baseline characteristics, treatment modalities, and aneurysm data of the included BOSS 1 patients with those of a control group consisting of non-BOSS 1 patients (n = 116) who had an available angiographic follow-up. Univariable and multivariable models were employed for analysis.
Results
Among the pooled sample of 591 aneurysms treated with WEB, the rate of persistent flow (BOSS 1) at angiographic follow-up was 5.2% (n = 31 out of 591), performed after an average of 8.7 ± 6.3 months. In the multivariable-adjusted analysis, dual antiplatelet therapy in the postoperative period (adjusted odds ratio [aOR] 4.3 [95% CI 1.3–14.2]), and WEB undersizing (aOR 10.8 [95% CI 2.9–40]) were independently associated with a BOSS 1 persistent flow result.
Conclusion
Persistent blood flow within the WEB device during angiographic follow-up (BOSS 1) is an uncommon occurrence. Our findings indicate that post-procedural dual antiplatelet therapy and undersizing of the WEB device are independently associated with the presence of BOSS 1 at follow-up.
Introduction
The Woven EndoBridge (WEB) device (Microvention, CA, USA) has been extensively studied for the treatment of intracranial aneurysms.1,2 It has been demonstrated as a safe alternative for wide-neck bifurcation aneurysms. 3
With the introduction of intrasaccular flow disrupters, the evaluation scales used for coiled aneurysms, such as the Raymond-Roy occlusion scale, needed revision due to their limited applicability to this new generation of devices.4–6 The WEB occlusion scale (WOS), adapted from the Raymond-Roy occlusion classification, emerged as the most commonly used grading scale following the implantation of the WEB device.6,7 Occasionally, during follow-up digital subtraction angiography (DSA), a persistent contrast opacification may be observed within the WEB device, which cannot be accurately assessed using the WOS scale. As a result, a revised occlusion scale score specifically for aneurysm treatment with the WEB device was introduced: the Bicètre Occlusion Scale Score (BOSS). This phenomenon, referred to as BOSS 1, can be considered a treatment failure. 6 Histologically, it may be attributed to an incomplete healing process, characterized by insufficient fibrosis of the intra-aneurysmal thrombus and partial endothelization at the aneurysmal neck.8,9
Three monocentric case series with BOSS 1 cases were published.10–12 Nguyen et al. 11 hypothesized that the administration of dual antiplatelet medication during the postoperative period could be associated with BOSS 1, leading to the absence of intra-device thrombosis and the persistence of blood flow within the WEB device. Similarly, Caroff et al. 12 reported a significant association between postoperative antiplatelet medication and the BOSS 1 phenomenon in a vaso computed tomography study. The optimal management of antiplatelet therapy (APT) before and after WEB implantation remains uncertain. Various practices have been described, but the assumption that the surface of the WEB device is not more thrombogenic than coils may justify the use of monotherapy for a few months. The duration of APT or the need for dual APT (DAPT) may be justified in cases of large aneurysm necks or when the device protrudes into the parent artery.13,14
In this multicenter retrospective study, our objective was to determine the incidence of intra-WEB persistent filling, identify factors associated with this phenomenon, and assess its evolution over time
Methods
Ethical statement
This study was a non-interventional retrospective analysis of de-identified data and therefore written informed consent was waived, however, patients or their relatives were informed that they could oppose the use of their de-identified health-related data for the purpose of research. A commitment to compliance was filed to the French National Information Science and Liberties Commission National for Healthcare Data before data centralization, with respect to the General Data Protection Regulation (CMR004, File number: 2226313).
Data collection
The Jeunes en Neuroradiologie Interventionnelle–Société Française de Neuroradiologie (JENI–SFNR) network, a collaborative research group led by trainees, 15 extended an invitation to academic centers that treat patients with WEB devices to contribute de-identified data for this study. 15 Each participating center received an electronic case report form and was requested to include all patients who underwent treatment with a WEB device and had a BOSS 1 occlusion score assessed through angiographic follow-up conducted at least 3 months after embolization. The data collection period ranged from 1 January 2013 to 31 December 2021.
To identify factors associated with the occurrence of BOSS 1, we compared patients with BOSS 1 to a control group consisting of patients who had available follow-up DSA images but were classified as BOSS 0, BOSS 0′, BOSS 2, or BOSS 3.
Angiographic analysis
Angiographic outcomes were evaluated by independent readers at each participating center using the BOSS six-point scale. 6 These readers were unaware of the patients’ clinical information to maintain objectivity. The presence of a BOSS 1 result was determined when contrast opacification was observed inside the WEB device during the angiogram conducted at least 3 months after embolization. Any modification in the shape of the WEB device, such as a reduction in the distance between the proximal and distal device markers on DSA, was considered an indication of device shape modification.16,17 The sizing of the WEB device was assessed by an independent reader who classified the treated aneurysms into two groups based on the rule of +1 mm/−1 mm. As per the existing literature, if the nominal transverse diameter of the selected device was not at least 0.5 mm larger than the average transverse diameter of the aneurysm measured on 3D DSA before implantation, it was deemed that the implanted device was undersized. 16
Statistical analysis
Continuous variables are reported as mean ± standard deviation, or median (interquartile range) as appropriate, and categorical variables as a number and percentage of the total.
To identify factors independently associated with the occurrence of BOSS 1 at follow-up we conducted univariable followed by backward stepwise multivariable logistic regression models. A variable was included in the multivariate model if it was associated with p < 0.1 in univariable analysis. All tests were two-sided and all probability values are provided uncorrected.
In post hoc analyses, and to consider the delay until recanalization as a potential confounder, we constructed a proportional hazards model, evaluating whether variables associated with a more frequent occurrence of BOSS I may be confounded by delay until angiographic follow-up. All analyses were done using JMP® Pro 14 (SAS Institute Inc., Cary, NC) software. Results were considered statistically significant if p values were <0.05.
This article was prepared according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 18
Results
BOSS 1 aneurysms incidence
During the study period, a total of 11 neurointerventional academic centers contributed data on 591 aneurysms that were treated with a WEB device and had at least one angiographic follow-up conducted after a minimum of 3 months. Among these treated aneurysms, 31 cases (5.2%) exhibited persistent blood flow within the WEB device, as observed during angiographic follow-up, which occurred between 3 and 24 months after treatment (with an average time of 8.7 ± 6.3 months). Among the cases with persistent flow inside the WEB device (BOSS 1), isolated persistent flow was observed in 28 out of 31 cases (90.3%), while in the remaining three cases (9.7%), persistent flow within the WEB device was associated with an aneurysm remnant (BOSS 1 + 3). Detailed examples of BOSS 1 cases are provided in Figure 1 and Supplemental Figures 3 and 4.
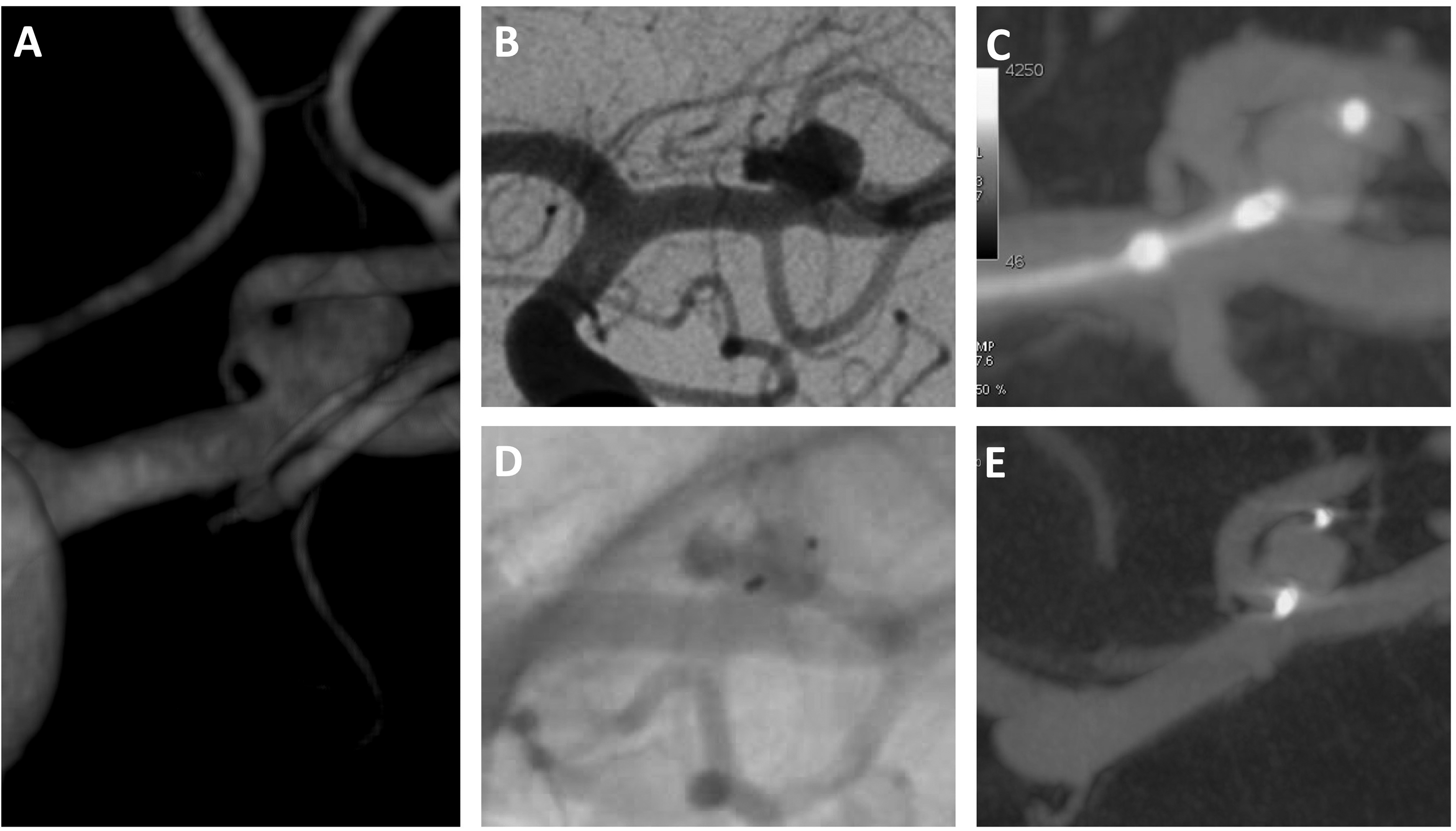
Unruptured left middle cerebral artery aneurysm treated with WEB 4.5 × 3 SL. The patient is under curative anticoagulation for a right femoral vein thrombosis. The angiographic follow-up at 6 months shows a completely circulating aneurysm (BOSS 1) despite a good positioning of the WEB. (A) Pre-operative 3D volume rendered angiography image; (B) pre-operative 2D view of DSA showing the aneurysm; (C) operative view with CB-CT angiography just before detachment showing a WEB device in place in the aneurysmal sac; (D) angiographic control at 6 months showing a completely circulating aneurysm despite good positioning of the WEB; (E) CB-CT follow-up at 6 months confirming a persistent blood flow inside the WEB device.
Evolution of BOSS 1 aneurysms
No instances of bleeding events were reported during the follow-up period. Out of the 31 patients with BOSS 1, 14 (45.2%) underwent a second angiographic follow-up, with an average time interval of 15.1 ± 11.1 months. Among these patients, six cases were ultimately assessed as having complete aneurysm occlusion at the last DSA follow-up (classified as BOSS 0 or BOSS 0′), indicating successful treatment. However, in the remaining eight patients, persistent flow inside the WEB device was observed. Among these cases, three patients experienced a decrease in the flow, four patients maintained a stable flow, and one patient exhibited a worsening of the phenomenon.
Comparison between BOSS 1 and control groups
Clinical and imaging data of the control group (non-BOSS 1 patients) were available from only one participating center, consisting of 116 patients.
In the univariable analysis (Table 1), the BOSS 1 group exhibited a shorter mean follow-up duration (15.1 ± 11 months vs. 23.0 ± 20.9 months, p = 0.004), larger aneurysm neck (4.8 ± 2 mm vs. 4.2 ± 1.6 mm, p = 0.04), and greater aneurysm width (5.7 ± 2.3 mm vs. 4.7 ± 1.7 mm, p = 0.02) compared to the non-BOSS 1 group. WEB undersizing (15 [48.4%] vs. 101 [87.1%], p < 0.001) and post-procedural APT (29 [93.5%] vs. 73 [62.9%], p < 0.001) were more prevalent in the BOSS 1 group, whereas WEB shape modification (WSM; 6 [19.4%] vs. 66 [56.9%], p < 0.001) was less frequently observed compared to the non-BOSS 1 group. No bleeding events were reported during the follow-up period after WEB implantation in the non-BOSS 1 group, and there was no significant difference in terms of retreatment rates between the two groups (7 [22.6%] vs. 16 [13.8%], p = 0.25).
Baseline characteristics in the BOSS 1 and control groups.
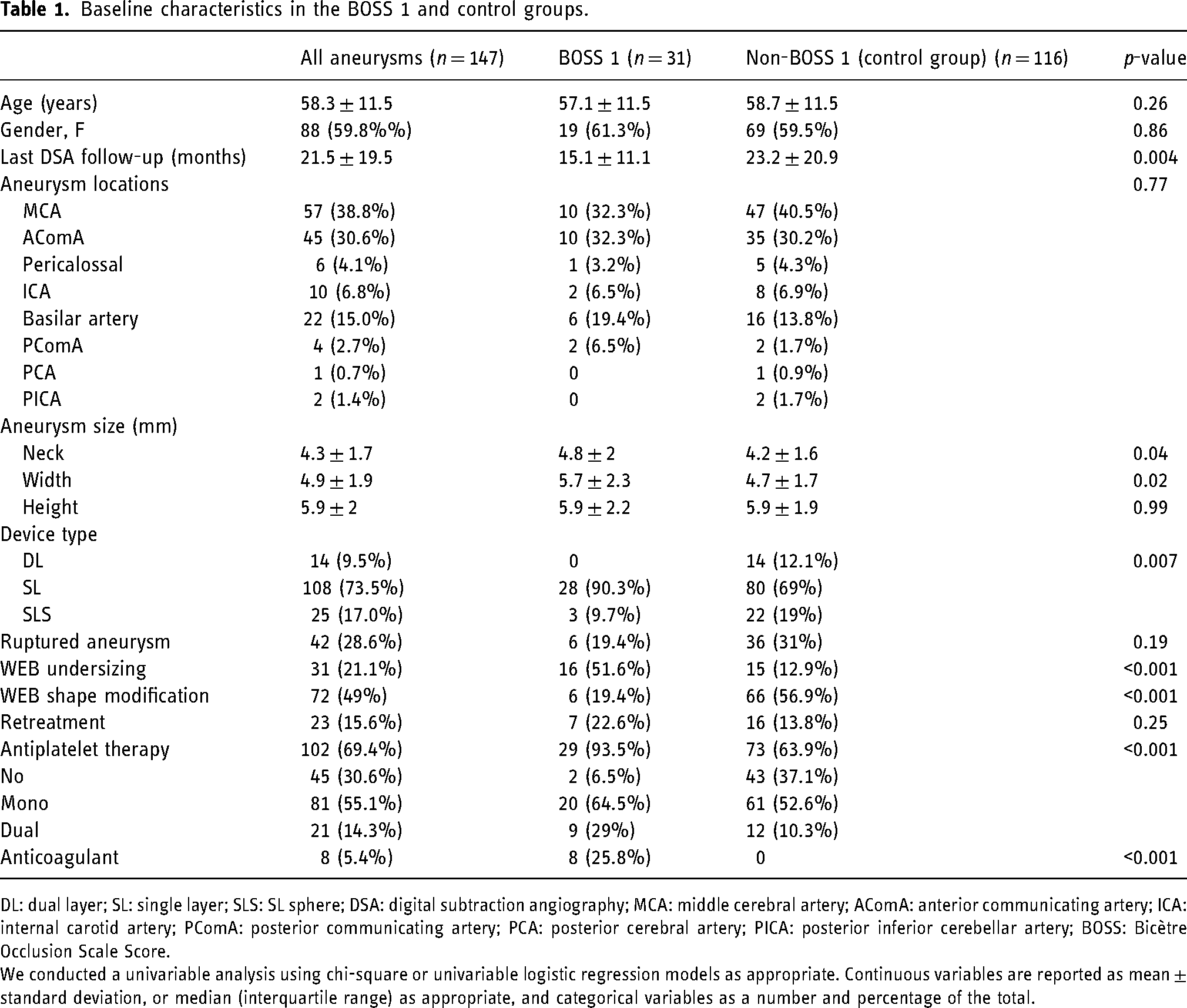
DL: dual layer; SL: single layer; SLS: SL sphere; DSA: digital subtraction angiography; MCA: middle cerebral artery; AComA: anterior communicating artery; ICA: internal carotid artery; PComA: posterior communicating artery; PCA: posterior cerebral artery; PICA: posterior inferior cerebellar artery; BOSS: Bicètre Occlusion Scale Score.
We conducted a univariable analysis using chi-square or univariable logistic regression models as appropriate. Continuous variables are reported as mean ± standard deviation, or median (interquartile range) as appropriate, and categorical variables as a number and percentage of the total.
In the multivariable analysis (Table 2 and Figure 2), DAPT during the postoperative period (adjusted odds ratio [aOR] = 4.3, 95% CI: 1.3–14.2, p < 0.001) and WEB undersizing (adjusted OR = 10.8, 95% CI: 1.9–40, p < 0.001) were the only independent factors associated with a BOSS 1 result. There was no significant difference observed between monotherapy and no APT during the postoperative period (p = 0.99). Proportional hazards models revealed that both APT (B estimate: 6.9; p < 0.001) and undersizing (B estimate: 0.8) were independently associated with the occurrence of BOSS 1.
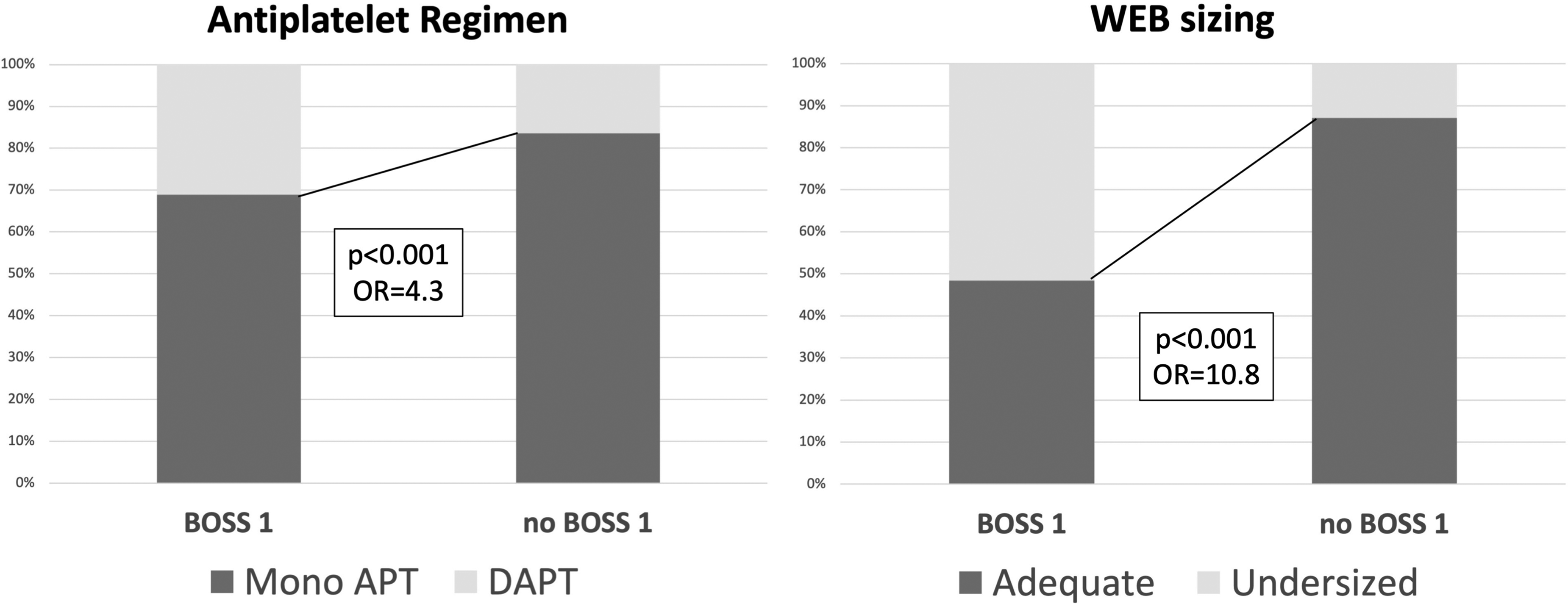
Association of dual antiplatelet therapy and WEB undersizing with BOSS 1 result.
Logistic regression analyses to determine independent predictors of BOSS 1.
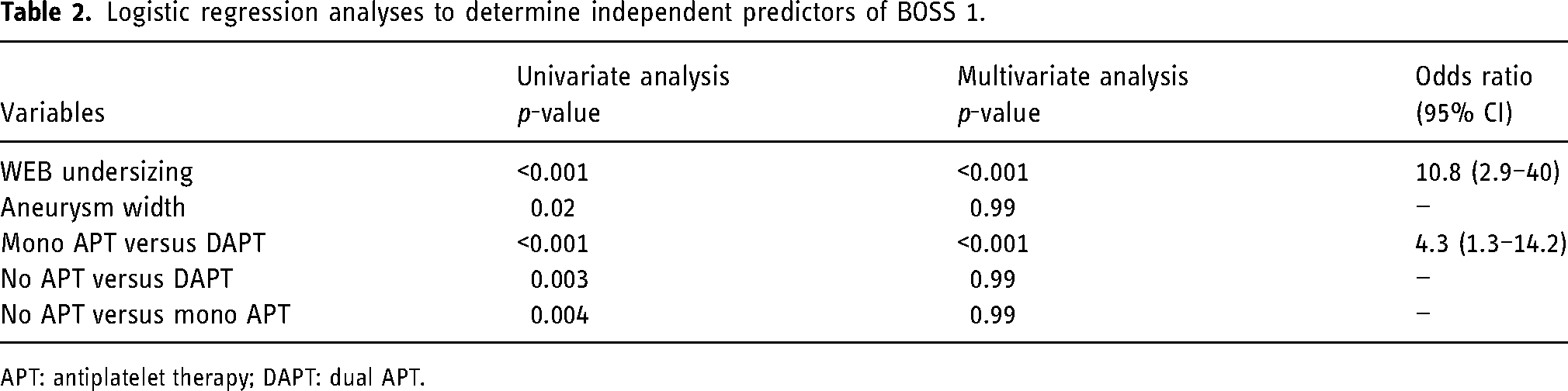
APT: antiplatelet therapy; DAPT: dual APT.
Discussion
In this large multicenter study consisting of 591 aneurysms, we found that BOSS 1 persistent flow following WEB treatment was relatively rare, appearing in 5.2% of cases. This result aligns with previous studies which have reported frequencies ranging from 6.3% to 16.4%.10–12,19 In our sample, we showed that the post-procedure use of dual antiplatelet medication and the undersizing of WEB were independently linked to a BOSS 1 outcome, irrespective of the duration until subsequent follow-up.
In the present dataset, we found that APT during the postoperative phase was administered in 93.5% of cases that resulted in BOSS 1, compared to 63.9% in the group that did not result in BOSS 1 (p < 0.001). This finding is consistent with a recent study that indicated a significant association between the delivery of APT beyond one week post-procedure and BOSS 1 aneurysms. 12 Additionally, Nawka et al. 10 and Nguyen et al. 11 documented the use of APT for a minimum of 6 weeks in all their BOSS 1 patients. Interestingly, when compared to single antiplatelet treatment, dual antiplatelet treatment in the postoperative period was robustly associated with a BOSS 1 result in our multivariable analysis (adjusted OR 4.3, p < 0.001). This finding echoes the reports of Nguyen et al., 11 who observed that most BOSS 1 patients (7 out of 8 patients) received DAPT postoperatively for at least 1 month. Further data indicate a potential influence of DAPT on aneurysms treated with hydrocoils. An animal study suggested less organized aneurysmal tissue in the case of DAPT use. 20 Moreover, a clinical study reported that DAPT delayed aneurysmal occlusion after flow diverter stent treatment with a higher chance of aneurysm retreatment in the case of prolongated DAPT. 21 Antiplatelet management for WEB-treated aneurysms remains unclear. There is no data regarding the optimal APT before or after WEB implantation. However, 8 in 10 physicians report using any antiplatelet before WEB implantation in a recent survey. 22
Following the deployment of the WEB device, particularly in elective cases, the mechanisms of flow diversion that slow down blood flow within the aneurysm and promote the formation of a blood clot in the aneurysmal sac may introduce a theoretical risk of embolism. This rationale justifies the use of low-dose aspirin for a few months at the beginning of aneurysmal thrombosis. 13 The duration of APT or the need for DAPT may be warranted in cases of large aneurysm necks or when the device protrudes into the parent artery. Within our cohort of BOSS 1 patients, nine individuals were receiving DAPT (Table 1). However, it is noteworthy that most of them required DAPT for conditions such as intracranial stenosis or protrusion of the WEB device, rather than solely for the WEB implantation itself. For instance, one patient had recently undergone cardiac stenting prior to our treatment, while another patient had been treated for a second aneurysm using a flow diverter stent during the same procedure. In these two cases, DAPT was administered for valid reasons unrelated to the WEB treatment. It is possible that patients who were already on DAPT before the procedure may not be ideal candidates for the use of the WEB device.
Notably, among the six cases that ultimately achieved complete aneurysm occlusion during the second angiographic follow-up, four of them were receiving DAPT, and one was under anticoagulation treatment during the postoperative period. All patients had discontinued their antiplatelet or anticoagulant treatment prior to the last angiographic follow-up, which demonstrated aneurysm occlusion. These findings provide further support for our hypothesis of an association between BOSS 1 results and the use of DAPT or anticoagulant agents. In our study, WEB undersizing was strongly linked to the occurrence of BOSS 1 during follow-up (aOR 10.8, p < 0.001), which contradicts the findings of Nawka et al. 10 Adequate device sizing plays a crucial role in aneurysm treatment, particularly with the WEB device, as undersized WEB devices may result in insufficient coverage of the aneurysm neck and reduce the likelihood of aneurysm occlusion during angiographic follow-up. 3 Initially, physicians tended to select a WEB device that matched the mean transverse diameter and height of the aneurysmal sac. 16 However, with growing experience, the device is now typically oversized, with a transverse diameter approximately 1 mm larger than the aneurysm's diameter. 13 Despite increased expertise, selecting the appropriate device can still present challenges, and virtual simulations may assist physicians in optimizing device selection. 23
No instances of bleeding events were reported during the follow-up period after WEB implantation in our cohort. In cases where the contrast opacification is in contact with the aneurysm wall or associated with an aneurysm remnant (BOSS 1 + 3), BOSS 1 may warrant retreatment to prevent the risk of bleeding. In our cohort, the three cases with the BOSS 1 + 3 phenomenon underwent retreatment, with one case involving the coiling of a lateral daughter cyst and two cases treated with a flow diverter stent. When the contrast opacification is limited inside the WEB device at the neck of the aneurysm or in cases of neck remnant (BOSS 2), the risk of aneurysm rupture is presumed to be low. Similarly, Caroff et al. 12 reported a favorable evolution of the BOSS 1 phenomenon over time without any bleeding events.
Within our series, WSM was observed in 19.4% of cases with BOSS 1, compared to 56.9% in the control group (p < 0.001). This finding aligns with the observations of Caroff et al., 12 who reported lower rates of WSM in comparison to BOSS 0, 0′, 2, and 3. These findings suggest that WSM may be associated with aneurysm occlusion and intrasaccular healing.17,24,25 Nguyen et al. 11 also reported similar observations, indicating the absence of WSM in cases of persistent flow inside the WEB, supporting the hypothesis that in the absence of intra-WEB thrombosis, no web shape modification is observed.
A previous study identified the fifth generation of the WEB device (WEB17) and aneurysm aspect ratio (height/neck) as predictive factors for the evolution of BOSS 1. However, in our study, neither device type nor aneurysm measurements were independently associated with the BOSS 1 phenomenon during angiographic follow-up.
This study possesses several limitations. Firstly, the retrospective nature of the analysis may have introduced selection and recall biases that are difficult to control. Secondly, the sample size, particularly within the BOSS 1 group, was small, but this can be attributed to the rarity of persistent intra-WEB filling. Thirdly, while there were differences in baseline characteristics and average DSA follow-up between the two groups, we adjusted for these differences and employed a proportional hazards model to account for the variation in time until recanalization. However, residual confounding factors may have influenced our results. Lastly, data from non-BOSS 1 patients were only available from one center with a relatively small sample size, potentially introducing a selection bias. Nevertheless, to the best of our knowledge, this is the largest study to report factors associated with the BOSS 1 phenomenon compared to non-BOSS 1 patients.
Conclusion
In conclusion, persistent blood flow within the WEB device during angiographic follow-up (BOSS 1) is a rare occurrence. Post-procedural DAPT and undersizing of the WEB device were independently associated with the BOSS 1 result during follow-up.
Supplemental Material
sj-docx-1-ine-10.1177_15910199231185805 - Supplemental material for Persistent flow inside the Woven EndoBridge at angiographic follow-up: A multicenter study
Supplemental material, sj-docx-1-ine-10.1177_15910199231185805 for Persistent flow inside the Woven EndoBridge at angiographic follow-up: A multicenter study by Kevin Janot, Guillaume Charbonnier, Gaultier Marnat, Peter Sporns, Julien Burel, Chrysanthi Papagiannaki, Geraud Forestier, Jean-Francois Hak, Thibault Agripnidis, Frederico Bolognini, Pablo Ariel Lebedinsky, Heloise Ifergan, Richard Bibi, Denis Herbreteau, Nourou Dine Adeniran Bankole, Alessandra Biondi, Xavier Barreau, Alexis Guédon, Eimad Shotar, Frederic Clarençon, Basile Kerleroux, Grégoire Boulouis, Fouzi Bala and Aymeric Rouchaud in Interventional Neuroradiology
Supplemental Material
sj-docx-2-ine-10.1177_15910199231185805 - Supplemental material for Persistent flow inside the Woven EndoBridge at angiographic follow-up: A multicenter study
Supplemental material, sj-docx-2-ine-10.1177_15910199231185805 for Persistent flow inside the Woven EndoBridge at angiographic follow-up: A multicenter study by Kevin Janot, Guillaume Charbonnier, Gaultier Marnat, Peter Sporns, Julien Burel, Chrysanthi Papagiannaki, Geraud Forestier, Jean-Francois Hak, Thibault Agripnidis, Frederico Bolognini, Pablo Ariel Lebedinsky, Heloise Ifergan, Richard Bibi, Denis Herbreteau, Nourou Dine Adeniran Bankole, Alessandra Biondi, Xavier Barreau, Alexis Guédon, Eimad Shotar, Frederic Clarençon, Basile Kerleroux, Grégoire Boulouis, Fouzi Bala and Aymeric Rouchaud in Interventional Neuroradiology
Supplemental Material
sj-docx-3-ine-10.1177_15910199231185805 - Supplemental material for Persistent flow inside the Woven EndoBridge at angiographic follow-up: A multicenter study
Supplemental material, sj-docx-3-ine-10.1177_15910199231185805 for Persistent flow inside the Woven EndoBridge at angiographic follow-up: A multicenter study by Kevin Janot, Guillaume Charbonnier, Gaultier Marnat, Peter Sporns, Julien Burel, Chrysanthi Papagiannaki, Geraud Forestier, Jean-Francois Hak, Thibault Agripnidis, Frederico Bolognini, Pablo Ariel Lebedinsky, Heloise Ifergan, Richard Bibi, Denis Herbreteau, Nourou Dine Adeniran Bankole, Alessandra Biondi, Xavier Barreau, Alexis Guédon, Eimad Shotar, Frederic Clarençon, Basile Kerleroux, Grégoire Boulouis, Fouzi Bala and Aymeric Rouchaud in Interventional Neuroradiology
Footnotes
Authors’ contribution
Kevin Janot: Conceptualization, acquisition of data, and writing—original draft preparation. Guillaume Charbonnier: Acquisition of data, reviewing, and editing. Gaultier Marnat: Acquisition of data, reviewing, and editing. Peter Sporns: Acquisition of data, reviewing, and editing. Julien Burel: Acquisition of data, reviewing, and editing; Chrysanthi Papagiannaki: Reviewing and editing. Geraud Forestier: Acquisition of data, reviewing, and editing. Jean-Francois Hak: Acquisition of data, reviewing, and editing. Thibault Agripnidis: Reviewing and editing. Frederico Bolognini: Acquisition of data, reviewing, and editing. Pablo Ariel Lebedinsky: Reviewing and editing; Heloise Ifergan: Reviewing and editing. Richard Bibi: Reviewing and editing. Denis Herbreteau: Reviewing and editing. Alessandra Biondi: Reviewing and editing. Xavier Barreau: Reviewing and editing. Alexis Guédon: Acquisition of data, reviewing, and editing. Eimad Shotar: Acquisition of data, reviewing, and editing. Frederic Clarençon: Reviewing and editing. Basile Kerleroux: Reviewing and editing. Grégoire Boulouis: Writing—reviewing and editing. Fouzi Bala: Writing, reviewing, and editing; Aymeric Rouchaud: Writing—reviewing and editing. Nourou Dine Adeniran Bankole: acquisition of data, reviewing and editing.
Data sharing
Data are available upon reasonable request.
Declaration of conflicting interests
Alessandra Biondi reports consulting for Balt, Cerus Endovascular, Medtronic, Microvention, and Stryker Neurovascular; Frederic Clarençon reports consulting for Microvention, Medtronic, Balt, and Stryker Neurovascular; Chrysanthi Papagiannaki reports consulting for Microvention, Stryker Neurovascular, and Balt; Aymeric Rouchaud reports consulting for Balt and Microvention. The other authors have no competing interests to report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.