
Abstract
Skull base cerebrospinal fluid (CSF) leaks can be challenging to diagnose. We describe a first technical report on a fluoroscopy-guided multiphase flat panel computed tomography cisternography to diagnose a CSF leak in a complex postoperative anterior cranial fossa. The entry point, pathway of leakage, and exit point were visualized in detail. The feasibility and technical details are described. This technique could be an additional asset in the diagnostic work up of complex CSF leaks, not only of the anterior cranial fossa, but also complex CSF leaks of the middle cranial fossa.
Skull base cerebrospinal fluid (CSF) leaks can result from trauma, tumors, iatrogenic causes, or may be spontaneous. The accurate diagnosis of a CSF leak is necessary prior to intervention. The clinical diagnosis is confirmed by testing a sample of nasal or otological secretions and measuring β2-transferrin. Positive β2-transferrin proves a CSF leak, however, cross-sectional imaging is needed to localize the defect. 1 High-resolution computed tomography (CT) is the preferred initial study, whereas CT or magnetic resonance (MR) cisternography with contrast is indicated for patients with multiple skull base defects. 2 CSF leaks of the skull base can be challenging to diagnose, particularly in patients with multiple surgeries or an abnormal anatomy of the skull base. We describe a new technique of fluoroscopy-guided multiphase flat panel CT (FPCT) cisternography for the first time, to diagnose a CSF leak in a patient with a complex skull base. A FPCT cisternography diagnosed the entry point, trajectory, and exit point of the CSF leak through the anterior cranial fossa in a dynamic fashion.
An adult patient with fibrous dysplasia of the anterior skull base presented with right-sided rhinorrhea after a recent left-sided pterional craniotomy for decompression of the left optic nerve. The medical history included multiple surgeries of the anterior skull base and multiple prior CSF leaks resulting in meningitides. High-resolution CT proved insufficient to determine the precise location of the CSF leak, specifically, being unable to differentiate the significance and likelihood of CSF leakages from each area of osseous dehiscence and defects. Given the complex anatomy and medical history, we performed an FPCT cisternography.
The FPCT cisternography was performed with local anesthetic and intravenous sedation using a biplane neuroangiography system (Philips Allura Xper FD20/20, Eindhoven, The Netherlands). The patient was positioned prone and head down with bolsters under the patient's trunk, creating a 20° head-down tilt of the vertebral column, without using the table-tilt function. The head of the patient was positioned in minimal flexion supported by a small soft horseshoe cushion, to minimize pooling of contrast in the cervical thecal sac. A 22-guage spinal needle was inserted under fluoroscopic guidance with a direct posterior approach at the L1 to L2 level. The previously inserted lumbar drain for CSF diversion at L3 to L4 was clamped during the procedure. A 1.0 mL test injection of contrast (Omnipaque 300; GE Healtcare, Piscataway, NJ) ensured an intradural position of the needle tip. Following this, 5 mL of preservative-free normal saline was injected slowly for 3 min to further dilute and propel the test bolus in a cephalad direction in the spinal canal. The saline injection also potentially provided slight pressurization of the intradural compartment to encourage leaking. 3 For the CT cisternography, 10 mL contrast was injected, chased by 5 mL of saline to push the contrast through the tubing. Once reaching the clivus on lateral plane, three flat panel rotational CT cisternographies (20 s acquisition time; 20 s interval) were obtained in a subsequent fashion under three breath holds. After removal of the lumbar needle, the patient was slowly repositioned in supine position.
Multiplanar reconstructions of the three CT cisternographies demonstrated the CSF leak in a timely manner (Figure 1). The entry point of the leak was localized in the left anterior skull base medially of the decompressed optic canal, crossing the midline through multiple fibrous dysplasia and posterior ethmoidal air cells, taking a curvilinear route down in the right side of the skull base before exiting in the right nasal cavity (Figure 2). Furthermore, the cisternogram excluded CSF leakage from other areas of dehiscence identified on the preprocedural high-resolution CT.
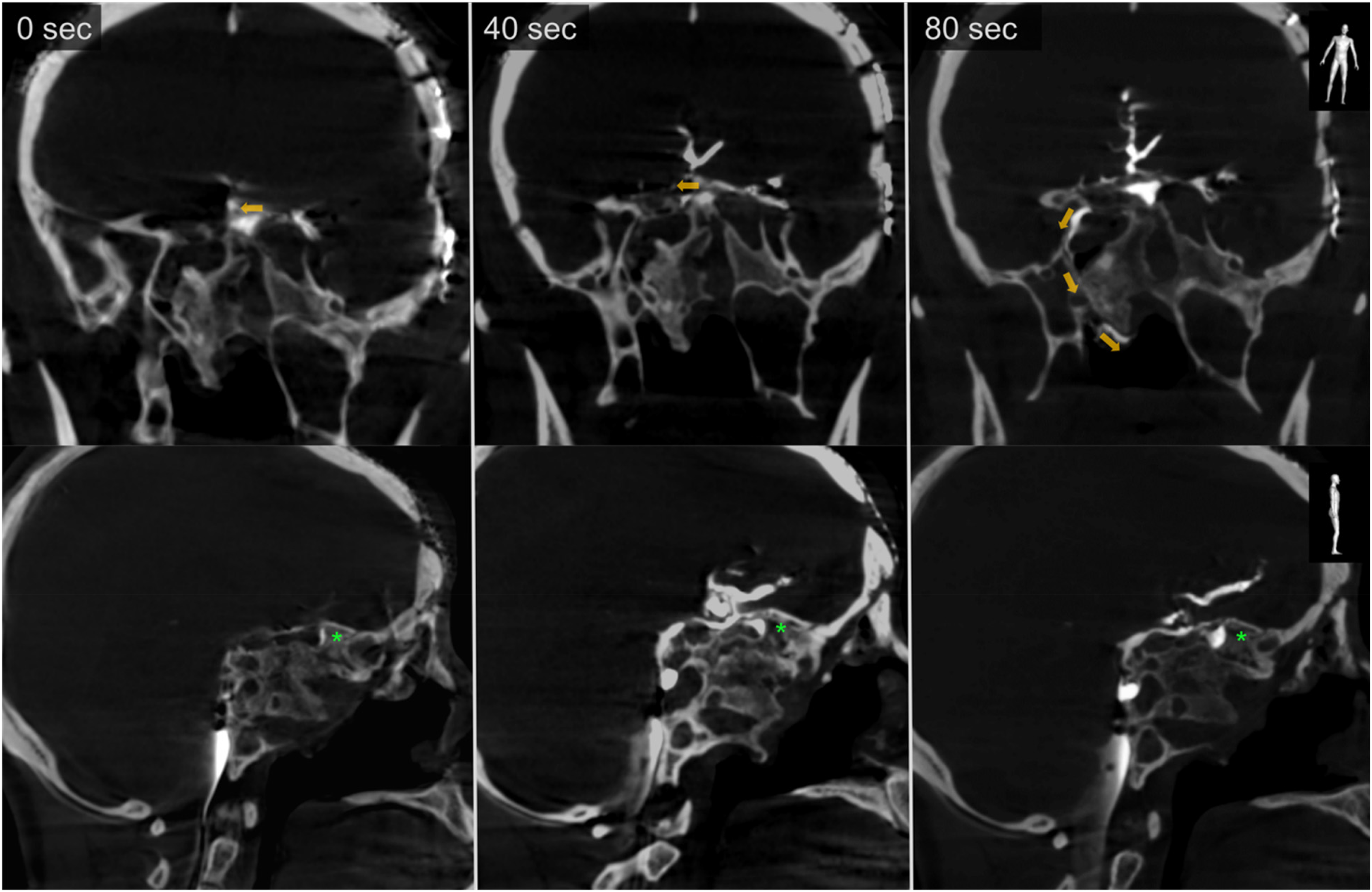
Coronal (upper) and sagittal (lower) 3.0 mm reconstructions of the flat panel CT cisternography performed at 0, 40, and 80 s, with arrows indicating the direction of the CSF flow. Coronal reconstructions demonstrate first filling of a left-sided skull base cell with contrast at 0 s with subsequent filling of a second contralateral right-sided cell at 40 s. At 80 s, a curvilinear trajectory of contrast leakage is visible in the right-side of the skull base into the nasal cavity. Sagittal reconstructions demonstrate gradual filling of the left-sided skull base cell, confirming it as initial path of entry (asterisk). Note the thin line of contrast posteriorly of the clivus due to the head-down tilt position. CSF: cerebrospinal fluid; CT: computed tomography.
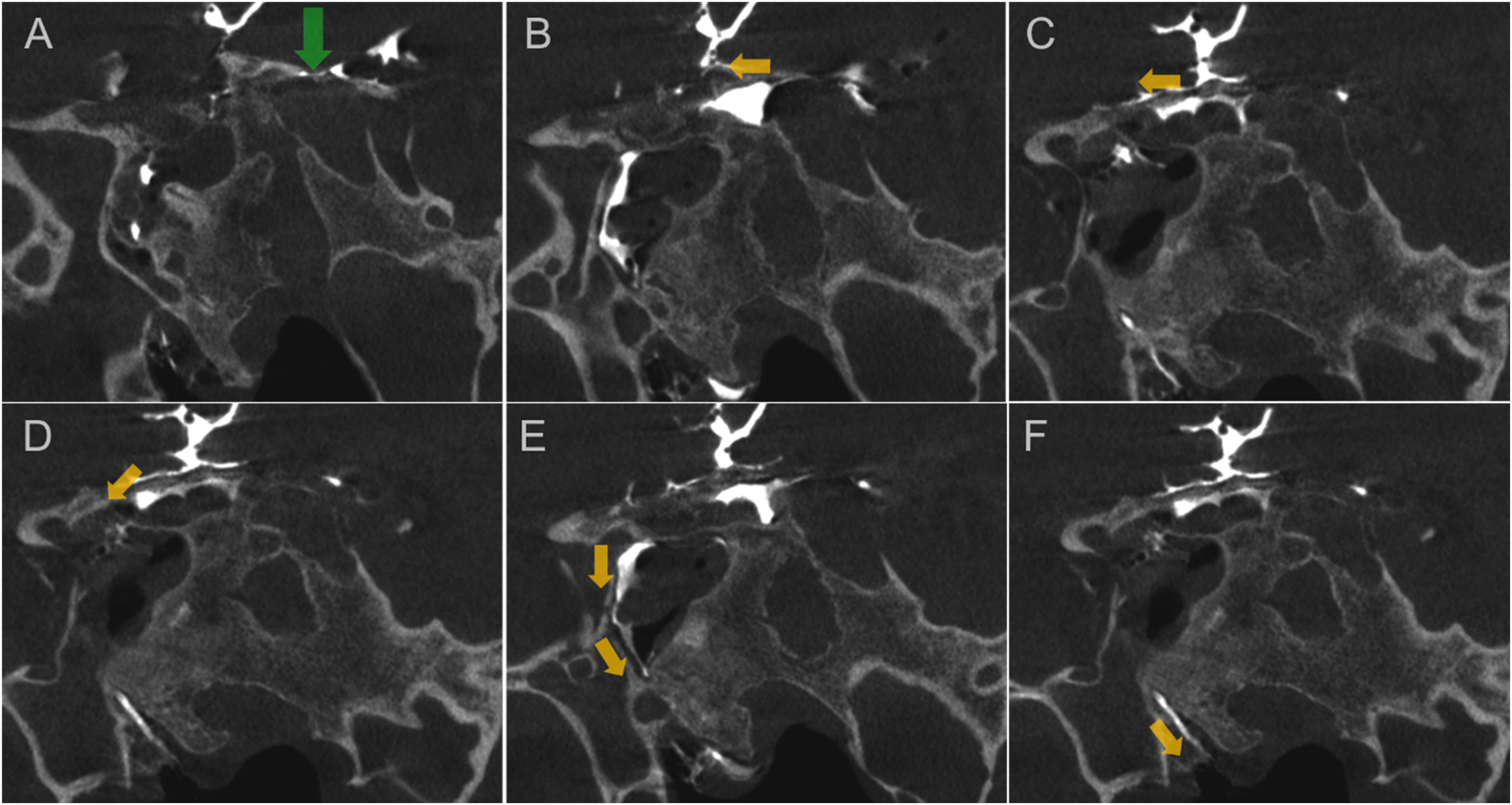
High resolution 0.16 mm coronal reconstructions at 80 s pinpoint the skull base defect (green arrow) with the trajectory of leakage through the fibrous dysplasia cells down to the right nasal cavity (arrows in A–F).
This is the first technical note on an FPCT cisternography to diagnose a CSF leak of the anterior cranial fossa. The feasibility and technical details are described. This technique could be an additional asset in the diagnostic work up of complex CSF leaks, not only of the anterior skull base, but also complex CSF leaks of the middle cranial fossa, with the patient positioned in a lateral decubitus position. Our neuroradiological, neurosurgical, and ENT (ear, nose, and throat) colleagues should be aware of this.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Eef J. Hendriks, Patrick J. Nicholson and Richard I. Farb thank the University Medical Imaging Toronto (UMIT) for their continuing support.
Informed consent
Informed consent was obtained from the patient.