
Abstract
Introduction
Carotid Web (CaW) is an increasingly recognized etiology of ischemic stroke, and has been shown to be amenable to endovascular stenting. The technical complexity of stenting for CaW may be lower than for carotid atherosclerotic disease (CAD). We aimed to assess procedural characteristics of stenting for CaW as compared to CAD.
Methods
We retrospectively analyzed a cohort of consecutive patients at a single comprehensive stroke center from 2014 to 2021, who had undergone elective endovascular stent placement for symptomatic CAD or CaW.
Results
In total, 118 patients underwent elective stent placement following ischemic stroke/transient ischemic attack; 88 patients had CAD and 30 patients had CaW. CAD patients were older (63.2 vs 51.2 years, p < 0.001), less likely to be female (28.4% vs 73.3%, p < 0.001), and more likely to have pre-existing vascular risk factors. Procedure time (73.0 vs 57.5 min, p = 0.007), radiation exposure (1482 vs 1125 milliGray, p = 0.03), filter time (24 vs 14 min, p = 0.04), and use of pre-stent (68.2% vs 0%, p < 0.001) and post-stent (34.1% vs 3.3%, p < 0.001) balloon angioplasty were higher in CAD cases. There was no significant difference between groups in the rate of periprocedural complications such as hypotension, use of vasopressors, or bradycardia. Recurrent stroke/TIA was reported in five CAD patients and 0 CaW patients by the end of the follow-up period (8.3% vs 0%, p = 0.12). In-stent restenosis was detected in seven CAD patients and 0 CaW patients (10.1% vs 0%, p = 0.09) at a median follow-up of 4 vs 16 months (p = 0.01), respectively. Periprocedural intracranial hemorrhage was not observed in either group.
Conclusion
Stenting for CaW was found to be technically simpler than CAD and not to confer increased risk of baroreceptor dysregulation. Intimal hyperplasia was uncommon in CaW cases.
Introduction
Carotid Web (CaW) is a shelf-like luminal protrusion of intimal hyperplasia arising at the carotid bulb. 1 It has been overlooked as a potential etiology for stroke, and it remains a commonly misdiagnosed and underreported entity. 2 The consensus guidelines for secondary prevention of ischemic stroke included a section on CaW for the first time in 2021, suggesting that more data was needed to determine optimal management for symptomatic CaW. 3
Stenting for symptomatic CaW could constitute a viable option for the management of symptomatic CaW, theoretically reducing the high risk of stroke recurrence through endoluminal reconstruction.4,5 The technical complexity of the procedure for CaW was anecdotally suggested to be lower than for stenting of carotid atherosclerotic disease (CAD), although comparative studies are not available. 6 We aim to assess the procedural characteristics and periprocedural complications in stenting for symptomatic CaW as compared to CAD.
Methods
This study was approved by the local Institutional Review Board (approval ID IRB00091421).
Inclusion criteria
Consecutive patients that underwent extracranial carotid artery stenting for symptomatic CAD or symptomatic CaW at a single comprehensive stroke center, from October 2014 to November 2021, were identified through the review of the local neurointerventional procedural case log. All patients were diagnosed with extracranial carotid disease via CT angiography, which confirmed the presence of CAD with moderate (50%–69%) or severe (70%–99%) stenosis per NASCET criteria [North American Symptomatic Carotid Endarterectomy Trial] or a CaW. 7 For management of symptomatic atherosclerosis, the institutional protocol involves a multidisciplinary evaluation of all patients with ≥50% CAD stenosis, during which an individualized decision for medical management, endarterectomy, or stenting is made. For symptomatic CaW, all patients were treated with endovascular stenting at our institution within the study period.
CaW were determined to be symptomatic following an appropriate stroke or TIA workup per American Heart Association/American Stroke Association guidelines at the time of presentation. Symptomatic CaW patients were found to have either TIA or stroke of undetermined etiology (as defined by TOAST criteria-Trial of Org 10172), with the area of acute cerebral infarct in the vascular territory of the CaW-affected internal carotid artery. 8 Patients received dual antiplatelet therapy prior to stenting, including aspirin and either clopidogrel or ticagrelor. Platelet response levels were confirmed with VerifyNow assays within 24 h of puncture (Regional Medical Laboratory; Tulsa, OK, USA) for all clopidogrel-based cases. Only elective procedures were included; patients who received other concomitant intervention (e.g., thrombectomy or cerebral aneurysm treatment) on the same day as CaW/CAD stenting were excluded.
Stenting procedure
Either a 6 French long sheath, an 8–9 French balloon guide catheter or a MOMA (Medtronic; Minneapolis, MN, USA) were used either via femoral or radial arteries as per operator preference. Patients were heparinized to achieve an activated clotting time of 250–300 s. The intention was to utilize proximal protection with either a balloon guide catheter or the MOMA system or to employ distal protection with the SpiderFX device (Medtronic; Minneapolis, MN, USA) if technically feasible.
Definitions
Procedure time began at skin puncture and ended at access site closure. Fluoro Time was the total time during the procedure under live fluoroscopy. Bradycardia was defined as heart rate less than 60 beats per minute and hypotension was defined as systolic blood pressure less than 90 mmHg, documented at any point during the procedure or within 24 h following closure.9,10 Vasopressor use was determined via review of the electronic medication administration record for phenylephrine, norepinephrine, epinephrine, vasopressin, dobutamine, or dopamine when used post-procedurally. Stent restenosis was defined as at least 50% in-stent stenosis, determined via carotid duplex ultrasound (per Society of Radiology in Ultrasound consensus guidelines) or computerized tomography angiography of the head and neck (per NASCET criteria) at 3 months following stenting and at the latest available follow-up imaging.11,12 Recurrent stroke/TIA was determined via chart review of the comprehensive stroke center (CSC) admissions and the most recent CSC clinic notes or outside facility records where available, and was defined as clinically significant acute neurologic decline localizable to the vascular territory of the stent. Patients who underwent optical coherence tomography in addition to stenting were excluded from Procedure Time, Fluoro Time, and Radiation analysis.
Statistical analysis
Continuous variables are reported in tables as mean(±SD) or median[IQR]. Categorical variables are reported as frequency (proportion). Between groups, comparisons were made with Student t-test/Mann–Whitney U or Chi-square/Fisher exact test, as appropriate. Significance was set at p < 0.05. Univariate regression analysis was performed, with variables at significance p < 0.1 placed into a multivariable linear regression model to identify factors independently associated with procedure time. Statistical calculations were performed using IBM SPSS Statistics, version 28.0 (IBM Corp., Armonk/NY).
Results
Baseline characteristics
From July 2014 to November 2021, 196 patients underwent cervical carotid stent placement for symptomatic CAD or CaW at the local comprehensive stroke center. Of these, 78 patients were stented concomitantly or within 24 h of another endovascular procedure (e.g., thrombectomy, aneurysm embolization, etc.); these 78 patients were excluded, leaving a total of 118 patients included in the analysis. Eighty-eight of these patients were stented for CAD, and 30 patients were stented for CaW. Table 1 depicts the baseline characteristics between the two groups. Patients with CaW were younger (CaW 51.2 vs CAD 63.2 years, p < 0.001) and more likely to be female (CaW 73% vs CAD 28%, p < 0.001). They were also less likely to have vascular risk factors such as hypertension (CaW 28% vs CAD 73%, p = 0.001), hyperlipidemia (CaW 43% vs CAD 72%, p = 0.005), and Diabetes (CaW 10% vs CAD 40%, p = 0.003). The NIH Stroke Score at the initial ischemic event was higher in CaW patients (CaW 11 vs CAD 7, p = 0.039). All CaW patients were found to have mild pre-stent stenosis, described as less than 30% per NASCET criteria. 7 Comparatively, all CAD patients had pre-stent stenoses of at least 50%, with 29 (32.9%) falling in the high moderate category of 50%–69% stenosis, and 59 (67.0%) falling in the severe category of >=70% stenosis.
Baseline, procedural, and post-procedural characteristics.
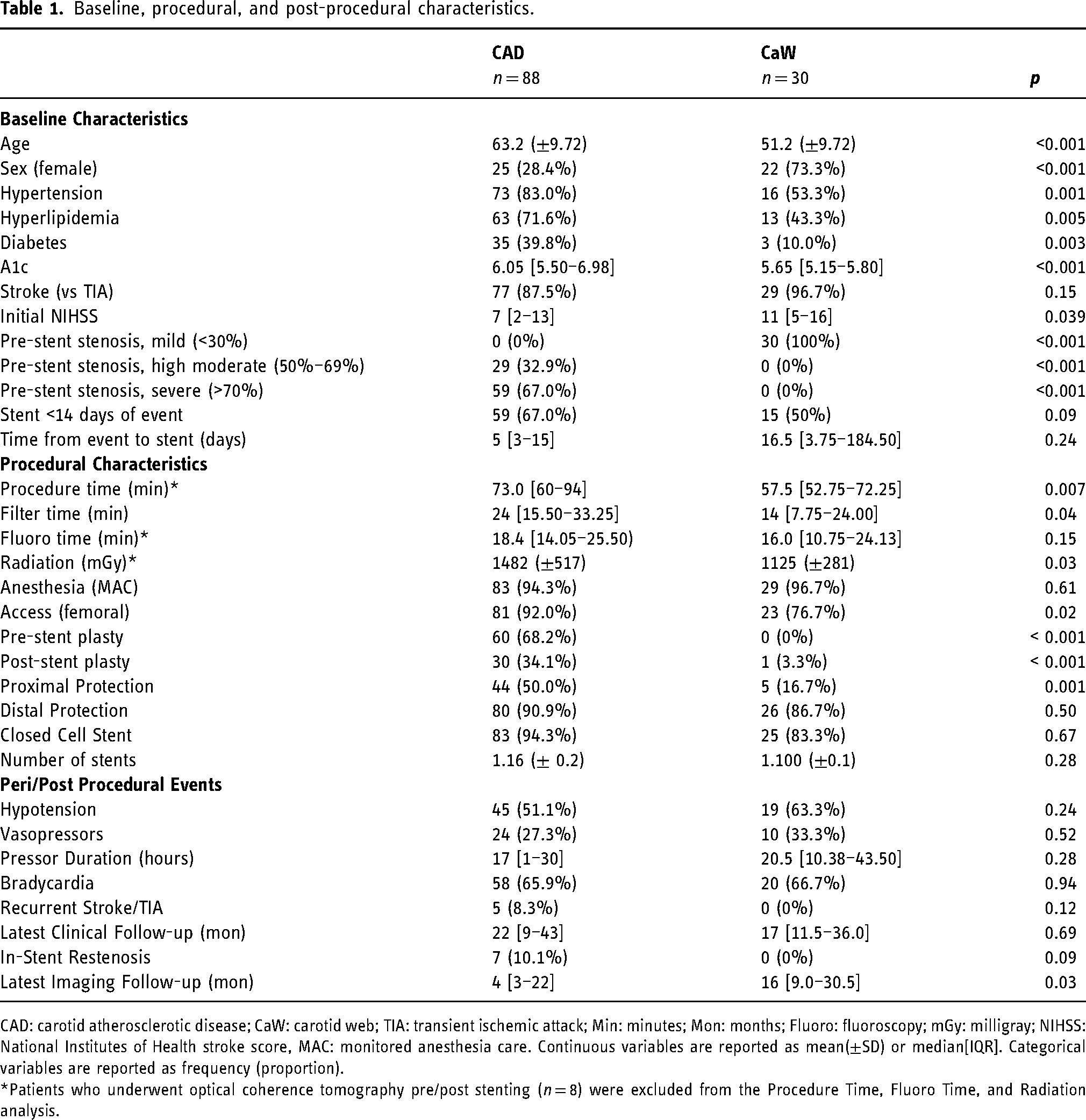
CAD: carotid atherosclerotic disease; CaW: carotid web; TIA: transient ischemic attack; Min: minutes; Mon: months; Fluoro: fluoroscopy; mGy: milligray; NIHSS: National Institutes of Health stroke score, MAC: monitored anesthesia care. Continuous variables are reported as mean(±SD) or median[IQR]. Categorical variables are reported as frequency (proportion).
*Patients who underwent optical coherence tomography pre/post stenting (n = 8) were excluded from the Procedure Time, Fluoro Time, and Radiation analysis.
Procedure characteristics
Prior to stenting, all but one of the patients were on a dual antiplatelet regimen; the exception was a CAD patient with an aspirin allergy, who was revascularized on clopidogrel monotherapy. Stenting was performed within 2 weeks of the sentinel ischemic episode in 67% of CAD and 50% of the CaW patients (p = 0.09). Femoral access was overall more common, although CaW procedures utilized radial access relatively more frequently (CaW 23% vs CAD 8%, p = 0.024, Table 1). All cases involved either proximal embolic protection with a balloon guide catheter or Mo.Ma cerebral protection device, and/or distal embolic protection with the SpiderFX filter. CAD procedures were more likely to utilize proximal protection (CaW 16.7% vs CAD 50%; p = 0.001, Table 1). There was no significant difference between groups in use of distal protection, with 90.9% of CAD procedures and 86.7% of CaW procedures utilizing a filter device (p = 0.507). None of the CaW procedures included pre-stent balloon angioplasty (vs 68% CAD, p < 0.001), and only one CaW case (3.3%) utilized post-stent balloon angioplasty (vs 34% CAD, p < 0.001) (Figures 1 and 2
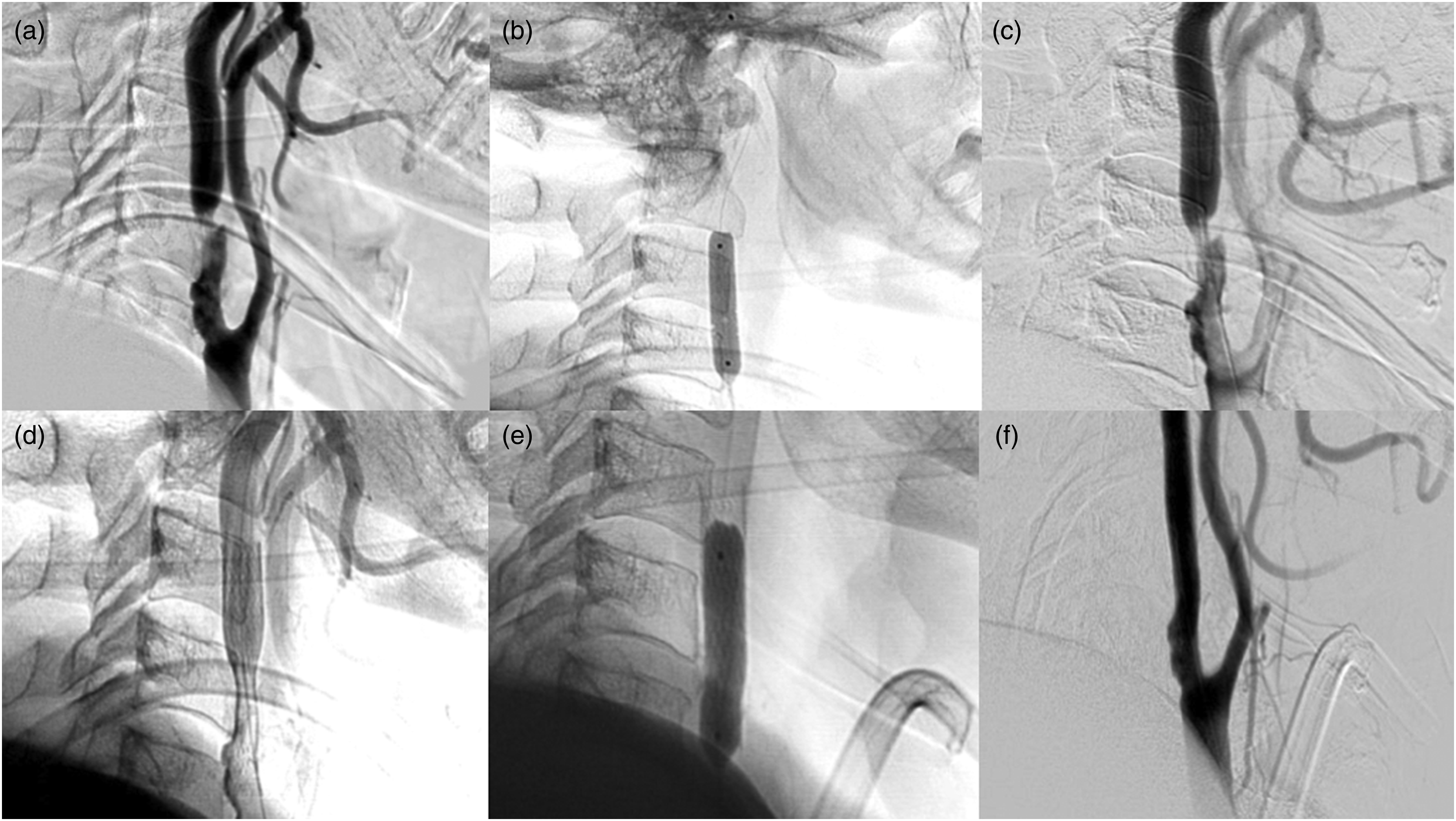
Stenting of carotid atherosclerosis under digital subtraction angiography. (a) initial run; (b) pre-stent balloon angioplasty with distal embolic protection device; (c) after initial angioplasty, pre-stent; (d) status-post stenting; (e) post-stent balloon angioplasty; (f) final run.
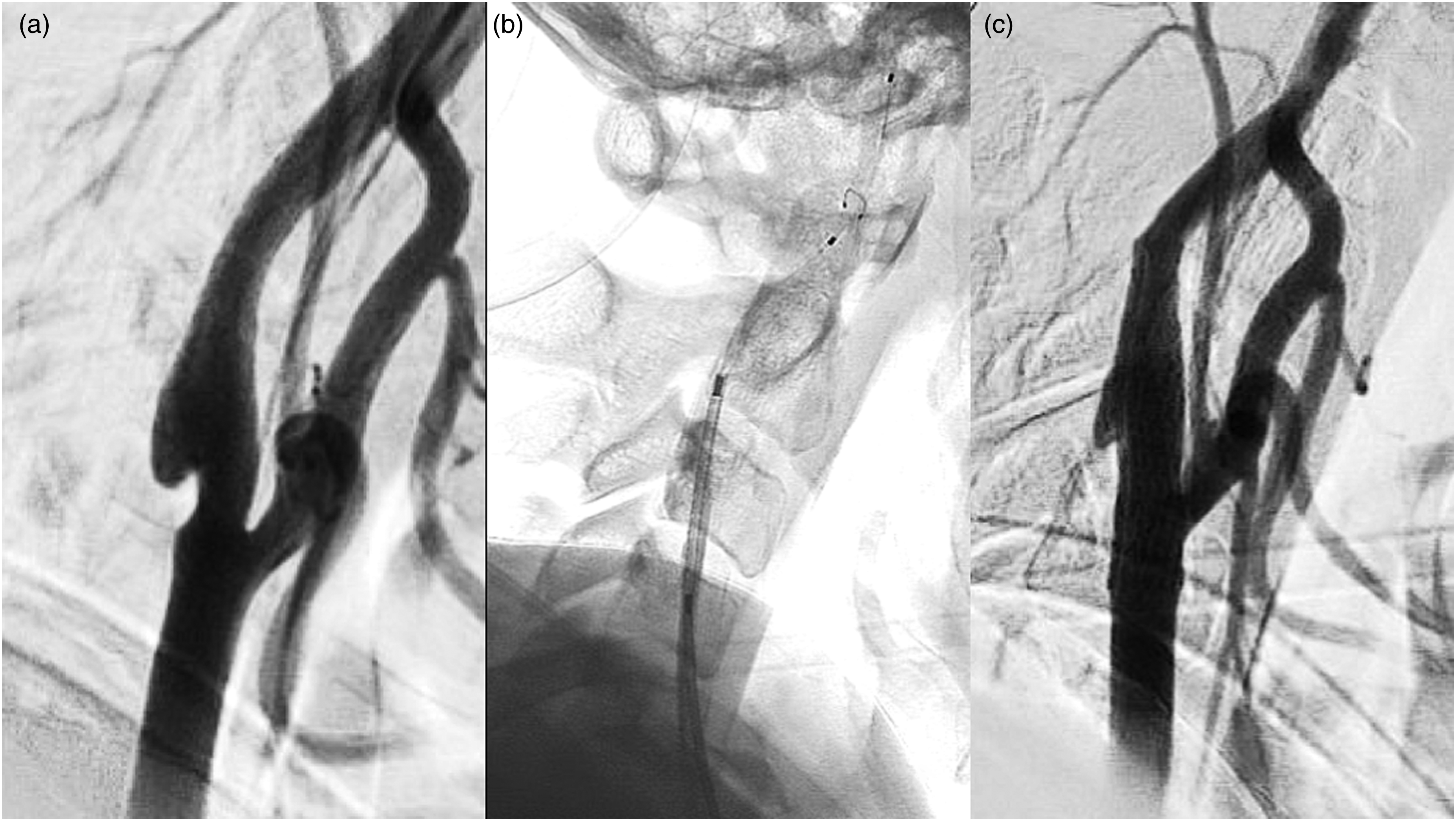
Stenting of carotid web under digital subtraction angiography. (a) initial run; (b) pre-stent with distal embolic protection device; (c) status post stenting.
Univariate and multivariable linear regression analysis was performed to identify factors associated with procedure time. CaW stroke etiology, female sex, and avoidance of post-stent balloon angioplasty were independently associated with lower procedure times per the multivariable analysis (Table 2).
Multivariable regression analysis for procedure time.
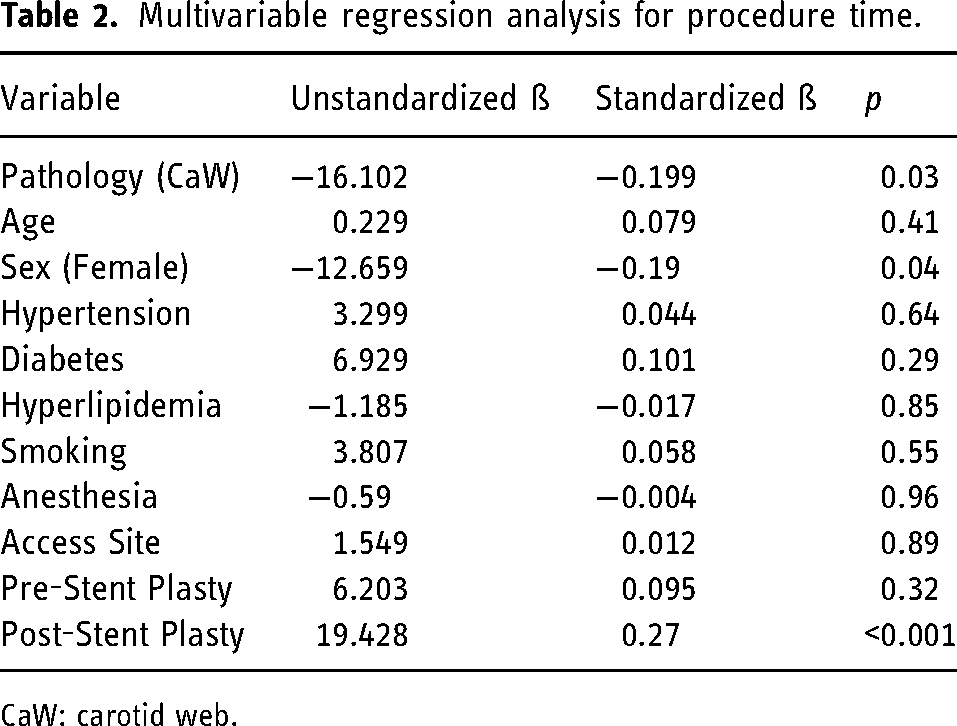
CaW: carotid web.
Peri-procedural complications
No significant difference was found between the two groups in periprocedural events such as hypotension, need for vasopressors, or bradycardia. A total of 33 patients required peri-procedural vasopressor support, with no differences between the two groups in terms of frequency of use or length of time on vasopressors (Table 1).
Of the 118 patients in the study, 69 CAD patients and 26 CaW patients had repeat vascular imaging with ultrasound or CTA at least 3 months after stenting. Of those, in-stent restenosis was found in six CAD patients (five moderate [50%–69% stenosis], 1 total [occlusion]) and was not observed in CaW. On review of the latest available follow-up imaging (CAD 4 vs CaW 16 months, p = 0.01), in-stent stenosis was noted in 7(10.1%) CAD vs 0(0%) CaW patients, p = 0.09.
No significant difference was found in the clinical follow-up interval between groups (CAD 22 vs CaW 17 months, p = 0.69). While five CAD patients were diagnosed with recurrent stroke or TIA in the vascular territory of the stent, no CaW patients were found to have recurrent events (8.3% vs 0%, p = 0.12). Of the five CAD patients who had recurrent stroke or TIA, no events occurred within 24 h of the procedure, while three occured within 2 weeks of stenting.
Discussion
This comparative analysis reports the largest single-center experience with stenting for CaW, and it corroborates the suggestion that stenting for CaW is safe and potentially effective in preventing recurrences. Moreover, it revealed that stenting for CaW did not confer an increased risk of baroreceptor dysregulation compared to stenting for CAD, was technically simpler considering the faster procedural times and the lower need for angioplasty, and was not associated with significant risk of intimal hyperplasia.
CaW was first described in 1968, but the first consensus guidelines recognizing this condition as a stroke etiology came over 50 years later.3,13 The guidelines endorse antiplatelet therapy as first-line for secondary stroke prevention, while acknowledging stenting as a secondary option, especially in recurrent stroke cases where antiplatelet therapy failed. The decision to revascularize has become more appealing since high stroke recurrence risk has been demonstrated with medical therapy. In one study, 30% of patients with symptomatic CaW receiving antiplatelet therapy had a recurrent ischemic event. 14 Another study demonstrated that 71% of the individuals with recurrent events were on an antiplatelet regimen. 4 The risk of recurrent ischemia on medical management was corroborated in a recent study that demonstrated a 27% 5-year cumulative risk on antiplatelet therapy without revascularization. 5 A multicenter experience of 24 patients stented for symptomatic CaW indicated that this procedure was technically feasible, and no recurrent events were noted in a median follow-up of 12 months. 15 Multiple other small series or case reports demonstrated similar findings.16–19 In the present study, 23 (76%) CaW patients had clinical follow-up data for at least 12 months following EVS, with no recurrent ischemic episodes.
Several factors for CaW stenting may contribute to lower procedure times, filter times, and radiation exposure as compared to CAD stenting. CaW typically has preserved lumen with no significant stenosis.4,20 Contrary to the generally irregular borders of atherosclerotic lesions, the endoluminal surface of the CaW is smooth and facilitates easier microwire lesion crossing. 21 Pre-stent and post-stent angioplasty also constitute embologenic steps, and were found to be unnecessary in CaW cases where the outward radial force of self-expanding stents was sufficient.
Peri- and post-procedural hemodynamic depression are known to be associated with carotid artery angioplasty and stenting, and have been demonstrated to be at increased risk in older patients and individuals with decreased cardiac ejection fraction. 22 Our findings indicate that despite being younger and with less comorbidities, stenting for CaW had comparable rates of baroreceptor dysregulation as for CAD. Post-stent intimal hyperplasia is thought to occur due to stress and shearing on the vessel wall from stent contact. 23 Angioplasty and stenting can produce in-situ inflammation at the level of the endothelium, setting the stage for a hyperplastic response from the tunica intima. 24 In our study, CaW patients were not found to develop intimal hyperplasia; the decreased need for angioplasty in CaW cases and/or the impaired endothelial function in CAD could partially explain this discrepancy. 25
Our study is limited by the single-center and retrospective study design. Despite emerging as an independent factor associated with shorter procedural time, CaW was younger compared to individuals with atherosclerotic etiology, and therefore the finding of shorter procedural times could be partially attributed to a less tortuous/elongated arterial anatomy. 26 Moreover, procedural time was shorter in women as compared to men, which could theoretically indicate another bias. Conversely, considering the unusual nature of CaW, it was relatively common for patients with CaW to have their contralateral carotids and/or renal arteries to be angiographically imaged (which is not part of the local protocol for angiography in patients with atherosclerotic lesions), which could have artificially increased the procedural times on CaW cases. The clinical follow-up was short and inconsistent, as a result of reliance on retrospective analysis of prospectively collected data.
Conclusion
Stenting for carotid web is technically simpler as compared to stenting for atherosclerotic disease. Faster procedural and filter times, lower radiation exposure, and lower utilization of balloon angioplasty were observed. CaW stenting does not confer increased risk of hemodynamic depression compared to stenting for CAD. Intimal hyperplasia was uncommon in CaW cases.
Footnotes
Author contributor statement
DCH conceptualized the study, working out most of the technical details with EO. EO procured much of the raw data, performed the statistical analysis, and wrote the initial and final drafts of the manuscript. NK, SKA, DL, and QAS helped collect and categorize the raw data and also aided in reviewing the final manuscript. DCH, RGN, AA, and JG produced the raw data and aided in reviewing the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval statement
This study was approved by the Emory University Institutional Review Board (approval ID IRB00091421). There were no external or internal sources of funding for this study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
The authors whose names are listed immediately below report the following details of affiliation or involvement in an organization or entity that may have a financial or non-financial interest in the subject matter or materials discussed in this manuscript.
Diogo C Haussen MD
Raul G Nogueira MD- Principal Investigator, Stryker Neurovascular (DAWN trial [no compensation], Trevo-2 trial), Cerenovus/Neuravi (ENDOLOW trial, no compensation); consultant to Stryker Neurovascular; steering committee member, Stryker Neurovascular(no compensation), Medtronic (SWIFT trial, SWIFT Prime trial [no compensation]), Cerenovus/Neuravi (ARISE-2 trial, no compensation); angiographic core lab, Medtronic (STAR trial); executive committee member, Penumbra (no compensation); Physician advisory board, Cerenovus/Neuravi, Phenox, Anaconda, Genentech, Biogen, Prolong Pharmaceuticals, Allm Inc.(no compensation), Viz-AI (stock options).
Jonathan Grossberg MD- Cognition (stock options), Grant Support: Department of Defense, Emory Medical Care Foundation, Georgia Research Alliance, Emory Neurosurgery Catalyst.