
Abstract
Purpose
Neurointervention via transradial access (TRA) is less invasive than via transfemoral access. However, radial artery occlusion (RAO) may occur with TRA. The purpose of this study was to explore risk factors for RAO after coil embolization of unruptured intracranial aneurysms (UIAs) via TRA.
Methods
Forty-two consecutive patients who underwent coil embolization for UIAs via TRA between March 2021 and March 2022 and were available for angiographic evaluation 1 year after treatment were retrospectively reviewed. Multivariate logistic regression analysis was conducted to identify potential risk factors for RAO.
Results
Seventeen (40%) of the 42 patients showed RAO. Compared with the non-RAO group, radial artery size was significantly smaller (2.2 mm [interquartile range (IQR): 2.1, 2.4 mm] vs 2.6 mm [IQR: 2.5, 2.7 mm]; p = 0.001) and the incidence of radial artery spasm (RAS) was significantly higher in the RAO group. Multivariate analysis identified radial artery size (odds ratio [OR] 4.9 × 10−3, 95% confidence interval [CI] 6.4 × 10−5–0.38) and incidence of RAS (OR 14.8, 95%CI 2.1–105) as significant independent predictors of subsequent RAO. Based on receiver operating characteristic (ROC) curve analysis, the optimal cutoff for radial artery size was 2.5 mm (sensitivity, 82.4%; specificity, 76.0%; area under the ROC curve, 0.80 [95%CI 0.66–0.95]).
Conclusion
Radial artery size and RAS represent reliable parameters for predicting RAO 1 year after coil embolization for UIA via TRA. Prophylaxis against RAS and limiting neurointervention via TRA to patients with radial artery larger than 2.5 mm in diameter may reduce the risk of postoperative RAO.
Keywords
Introduction
Transradial access (TRA) has seen increasing use not only in the field of interventional cardiology but also in neurointervention compared with transfemoral access, reducing patient burden and healthcare costs associated with early discharge from hospital, facilitating procedures in obese patients, and reducing the risk of puncture-site complications.1–11 Even TRA, however, can cause puncture-site complications such as pseudoaneurysms, infection, acute compartment syndrome, and radial artery occlusion (RAO).12,13 Among these, RAO is mostly asymptomatic due to collateral blood flow from the palmar arch and rarely leads to severe hand ischemia requiring intervention, but the radial artery will no longer be available in the future as an access site for neurological and cardiovascular interventions, as a conduit for coronary bypass grafting, or as a fistula formation in hemodialysis patients. Appropriate prophylaxis of RAO and identification of its risk factors is thus important.
Previous studies in the field of interventional cardiology have shown that risk factors for RAO include dose of heparin, compression hemostasis time, age, sex, sheath size, and diameter of the radial artery. 14 On the other hand, several studies in the field of neurointervention have examined the frequency of postoperative RAO,15,16 but few have investigated risk factors for RAO. Neurointervention may involve potential inherent risk factors compared with interventional cardiology, due to the use of larger catheters, longer procedure times, and methods for administering antithrombotic agents. The purpose of this study was thus to explore risk factors for RAO after coil embolization of unruptured intracranial aneurysms (UIAs) via TRA.
Methods
Study design
A total of 58 consecutive patients who underwent coil embolization for UIAs via TRA at our institution between March 2021 and March 2022 were identified from the maintained database and retrospectively reviewed. Among the 58 patients treated via TRA, 14 patients (24%), including 10 patients with acute angle of common carotid artery origin and 4 patients with severe radial artery spasm (RAS), converted the access site to transfemoral access due to difficulty in directing the guiding sheath to the target vessel. Coil embolization was completed via TRA in 44 patients. After treatment, one patient was transferred to another hospital and one patient died, so follow-up angiography was not available. Ultimately, 42 patients with available angiographic assessment of the radial artery one year after treatment via TRA were included in the present study (Figure 1). All study protocols were approved by the institutional review board, and the need to obtain patient consent was waived because of the retrospective design.
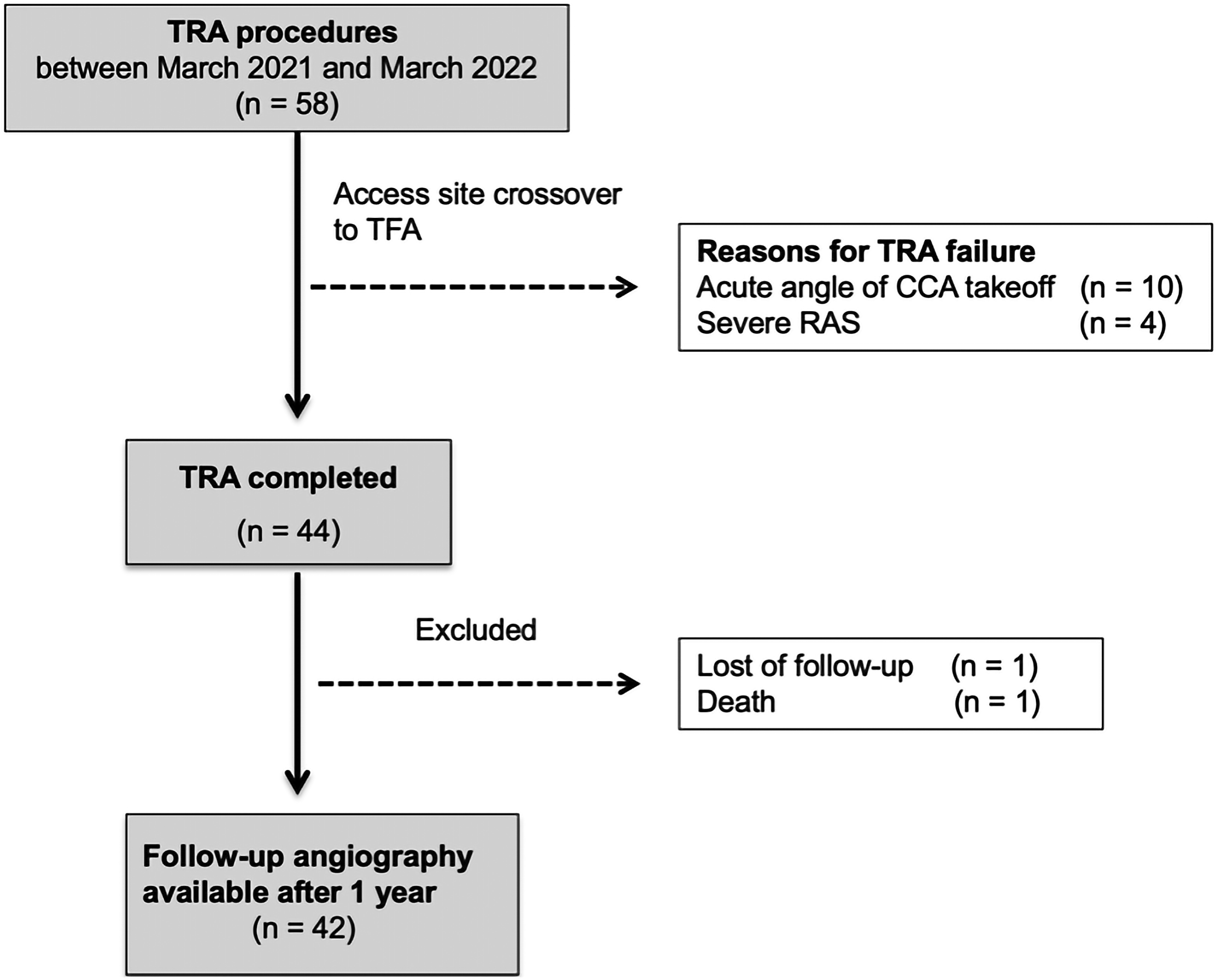
Patient selection algorithm for UIAs treated with coil embolization via TRA. A total of 58 consecutive patients with UIAs were treated with coil embolization via TRA. Among the 58 patients treated via TRA, 14 patients (24%), including 10 patients with acute angle of CCA origin and four patients with severe RAS, converted the access site to TFA due to difficulty in directing the guiding sheath to the target vessel. Coil embolization was completed via TRA in 44 patients. After treatment, one patient was transferred to another hospital and one patient died, so follow-up angiography was not available. Ultimately, 42 patients were available for angiographic evaluation of the radial artery one year after treatment. CCA, common carotid artery; RAS, radial artery spasm; TFA, transfemoral access; TRA, transradial access; UIA, unruptured intracranial aneurysm.
Endovascular treatment
Coil embolization was performed in a standardized fashion only by M.F. and R.T., certified interventional neurosurgeons who already had experience with diagnostic angiography via TRA in over 50 cases. As a rule, antiplatelet therapy consisting of aspirin (100 mg/day) and clopidogrel (75 mg/day) was started 2–4 weeks before coil embolization to prepare for unintended rescue stenting. All coil embolization procedures were conducted under general anesthesia. Intraoperatively, heparin was administered to maintain whole blood-activated clotting time above 250 s. Postoperatively, argatroban was administered for 24 h to prevent ischemic complications. If no stent was used, patients were maintained on a single antiplatelet drug (aspirin, 100 mg/day) for 4 weeks. If a stent was implanted, dual antiplatelet agents (aspirin, 100 mg/day, clopidogrel, 75 mg/day) were maintained for up to 6 months, followed by single antiplatelet agent (aspirin, 100 mg/day) for another 6 months.
TRA procedure details
In terms of indications, coil embolization via TRA was restricted to patients with a radial artery diameter ≥2 mm associated with well-developed collateral blood flow from the ulnar artery, which was confirmed by preoperative angiography. Neurointervention via TRA was standardized according to methods previously reported at our institution. 11
The procedure is briefly described as follows; under echo-guided puncture in a step-by-step manner, the small sheath was replaced with a larger sheath to insert a 6F straight-shaped guiding sheath (FUBUKI Dilator Kit [outer diameter, 2.7 mm; inner diameter, 0.090 inch; length, 90 cm]; Asahi Intecc, Aichi, Japan). Following sheath insertion, if a severe spasm occurred, 2 mg of isosorbide dinitrate was administered as a vasodilator over 1 min from the sheath. The guiding sheath was then directed coaxially into the target vessel using a 130-cm 5F Simmons-shaped catheter (Medikit, Tokyo, Japan) for the anterior circulation or a 130-cm 5F non-taper angle catheter (Terumo, Somerset, New Jersey, USA) for the posterior circulation. An intermediate catheter (TACTICS; Technorat Corporation, Aichi, Japan) was then guided as distal to the artery as possible. Subsequently, a microcatheter was guided into the aneurysm to complete the coil embolization. Hemostasis was achieved by a patent hemostasis method using a dedicated radial compression device (TR Band; Terumo) at the radial artery access site on the forearm at the end of the procedure. The patent hemostasis method has been described in detail in previous reports, 17 but in brief, the pulse oximeter was placed over the index finger, and the sheath was removed with the TR band fastened. The ipsilateral ulnar artery was occluded by compression, and the band was loosened until the plethysmographic signal returned to confirm radial artery patency. The band was deflated by withdrawing 2 ml of air every 30 min, and each time the access site was monitored for any bleeding. If bleeding occurred, 2 ml of air was injected again to achieve hemostasis. This procedure was repeated until the air was completely released, and hemostasis was achieved.
Assessment methods for RAS and RAO
Radial artery spasm was evaluated by radial angiography taken at the time of sheath insertion via TRA during coil embolization for UIAs. Radial artery spasm was defined as any arterial spasm observed on radial angiography. 18 One year after treatment, patients treated via TRA underwent distal radial angiography or transbrachial angiography to simultaneously evaluate UIAs and the presence or absence of RAO by comparison with preoperative angiography. Radial artery spasm and RAO were assessed by two certified interventional neurosurgeons (M.F. and R.T.). If the two assessors disagreed, a third certified interventional neurosurgeon (A.T.) reviewed the radial artery for patency, and consensus was reached among the three interventional neurosurgeons.
Statistical analyses
Baseline characteristics between the RAO and non-RAO groups were compared using the Mann–Whitney U test or Fisher's exact test. Predictors of RAO after coil embolization of UIAs via TRA were evaluated using multivariate logistic regression analysis. This analysis was adjusted both for factors that were significant in univariate analyses performed in this study and for previously reported risk factors for RAO (age, sex, radial artery size, and compression hemostasis time). 14 Alterations in radial artery diameter in RAO were evaluated using receiver operating characteristic (ROC) curves and 95% confidence intervals (CIs). The optimal cutoff was specified as the value closest to the upper left corner of the ROC curve. All statistical analyses were performed using R and R Commander-based Easy R (EZR) software (Saitama Medical Center, Jichi Medical School, Saitama, Japan). 19 Values of p < 0.05 were regarded as significant.
Results
Among the 42 patients with angiographic assessment of the radial artery available one year after neurointervention for UIAs via TRA, 17 (40%) developed RAO.
Clinical and angiographic characteristics
No significant differences between groups were observed in terms of age, sex, body mass index, medical history, smoking and drinking history, medication, or blood test results (Table 1). No significant differences were seen between groups with respect to aneurysm characteristics, including aneurysm size, neck size, aneurysm volume, and aneurysm location. Likewise, no significant differences were observed in terms of surgical procedures, including the percentage of initial treatment, radial artery puncture site, brachioradial artery, endovascular technique, patent hemostasis method, procedure time, or compression hemostasis time (Table 2). Patients with previous treatment via TRA and radial artery loop were not included in the present study. Radial artery size was 2.2 mm (interquartile range [IQR]: 2.1, 2.4) in the RAO group and 2.6 mm (IQR: 2.5, 2.7) in the non-RAO group and was significantly smaller in the RAO group (p = 0.001) (Table 2). The percentage of radial artery ID/sheath OD < 1.0 (p = 0.02) and incidence of RAS (p = 0.001) were both significantly higher in the RAO group than in the non-RAO group (Table 2). In the RAO group, no patients received vasodilators for RAS. With regard to access-related complications, the percentage of patients who complained of forearm pain tended to be higher in the RAO group than in the non-RAO group (p = 0.059).
Baseline clinical characteristics in RAO and non-RAO groups.
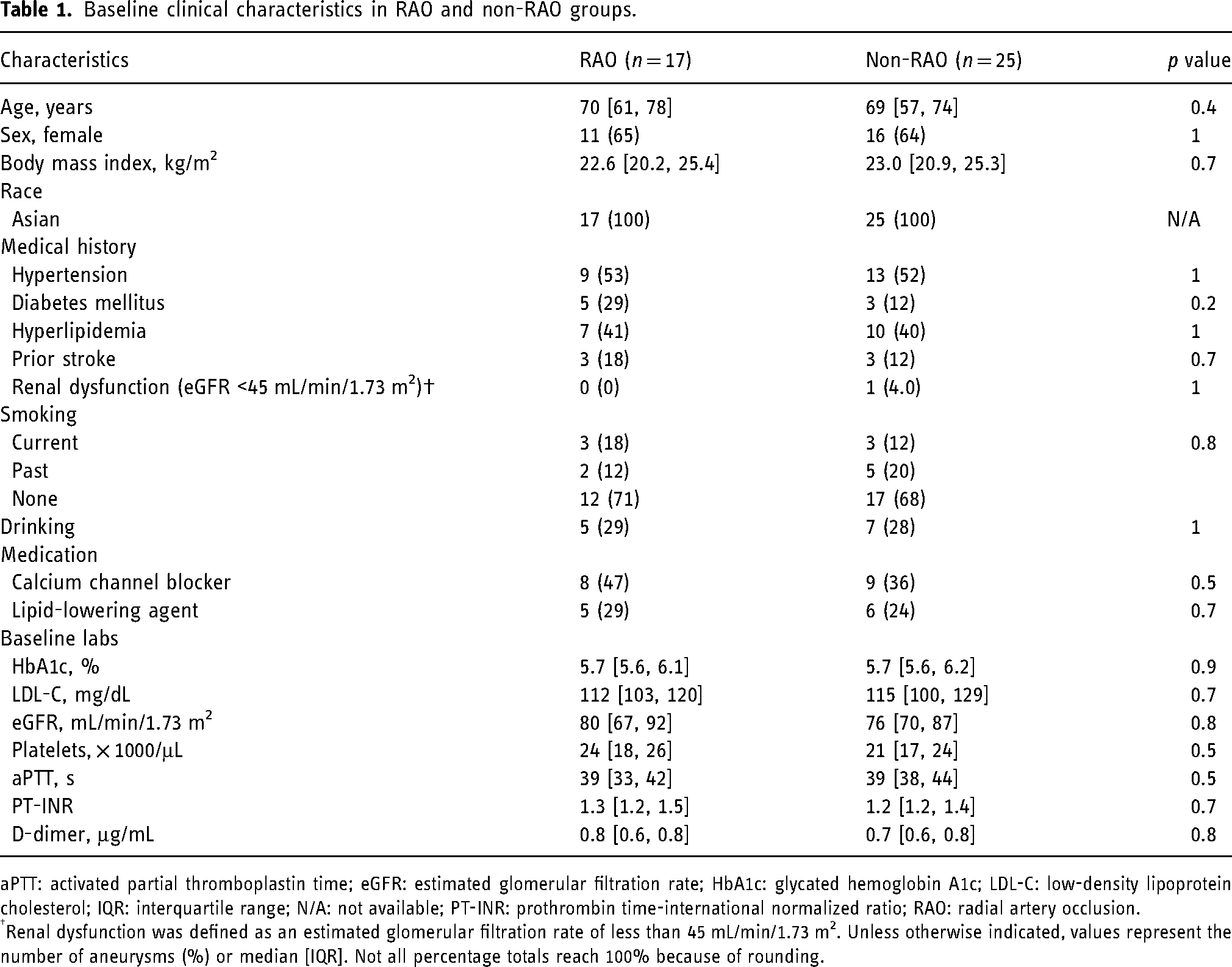
aPTT: activated partial thromboplastin time; eGFR: estimated glomerular filtration rate; HbA1c: glycated hemoglobin A1c; LDL-C: low-density lipoprotein cholesterol; IQR: interquartile range; N/A: not available; PT-INR: prothrombin time-international normalized ratio; RAO: radial artery occlusion.
Renal dysfunction was defined as an estimated glomerular filtration rate of less than 45 mL/min/1.73 m2. Unless otherwise indicated, values represent the number of aneurysms (%) or median [IQR]. Not all percentage totals reach 100% because of rounding.
Angiographic characteristics in RAO and non-RAO groups.
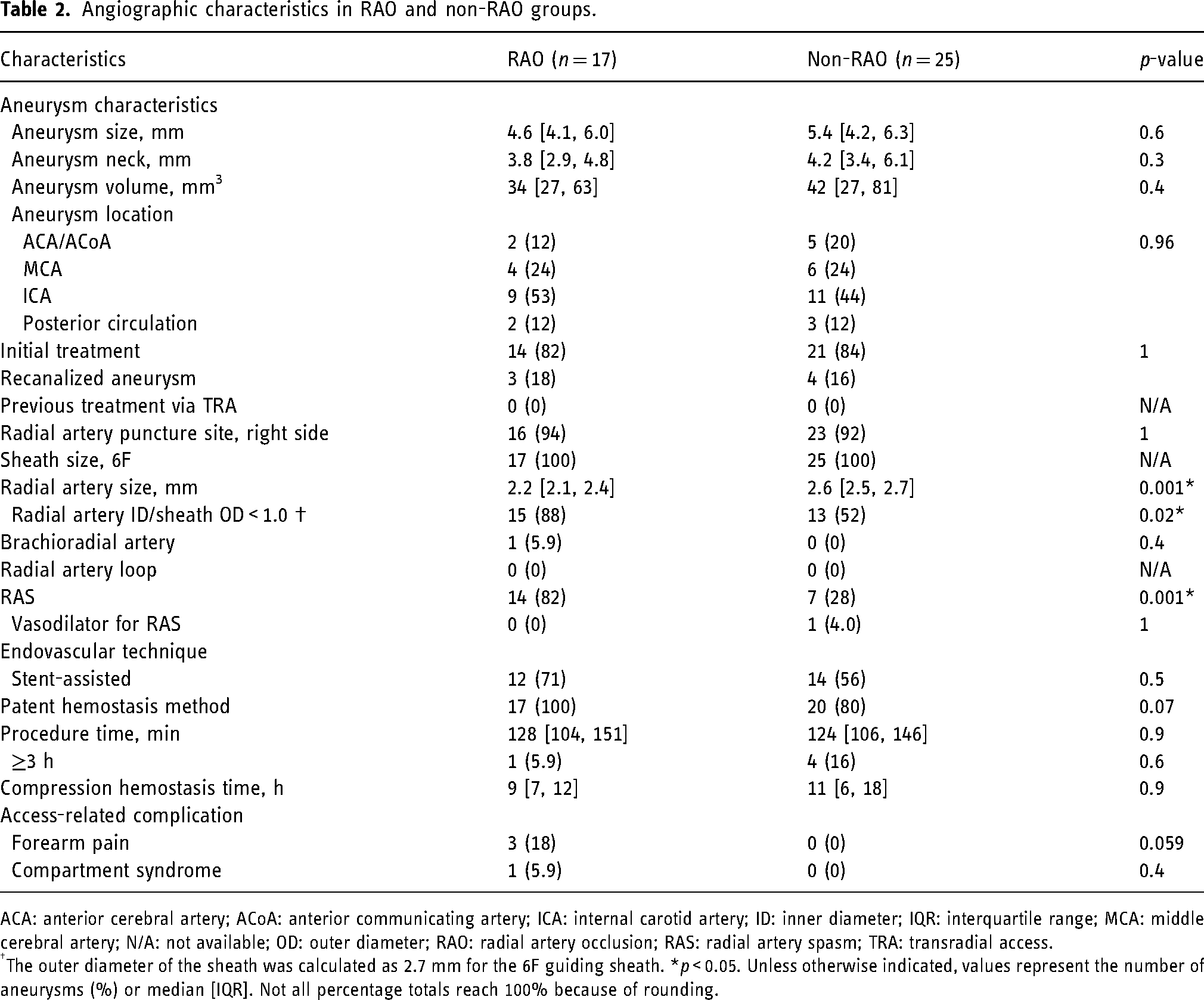
ACA: anterior cerebral artery; ACoA: anterior communicating artery; ICA: internal carotid artery; ID: inner diameter; IQR: interquartile range; MCA: middle cerebral artery; N/A: not available; OD: outer diameter; RAO: radial artery occlusion; RAS: radial artery spasm; TRA: transradial access.
The outer diameter of the sheath was calculated as 2.7 mm for the 6F guiding sheath. *p < 0.05. Unless otherwise indicated, values represent the number of aneurysms (%) or median [IQR]. Not all percentage totals reach 100% because of rounding.
Risk factors for RAO in neurointervention via TRA
Radial artery size (odds ratio [OR] 4.9 × 10−3, 95%CI 6.4 × 10−5–0.38) and RAS (OR 14.8, 95%CI 2.1–105) were identified as independent predictors of RAO by multivariate logistic regression analysis (Table 3). Based on ROC curve analysis, the optimal cut-off for radial artery size was 2.5 mm (sensitivity, 82.4%; specificity, 76.0%; area under the ROC curve, 0.80 [95%CI 0.66–0.95]) (Figure 2).
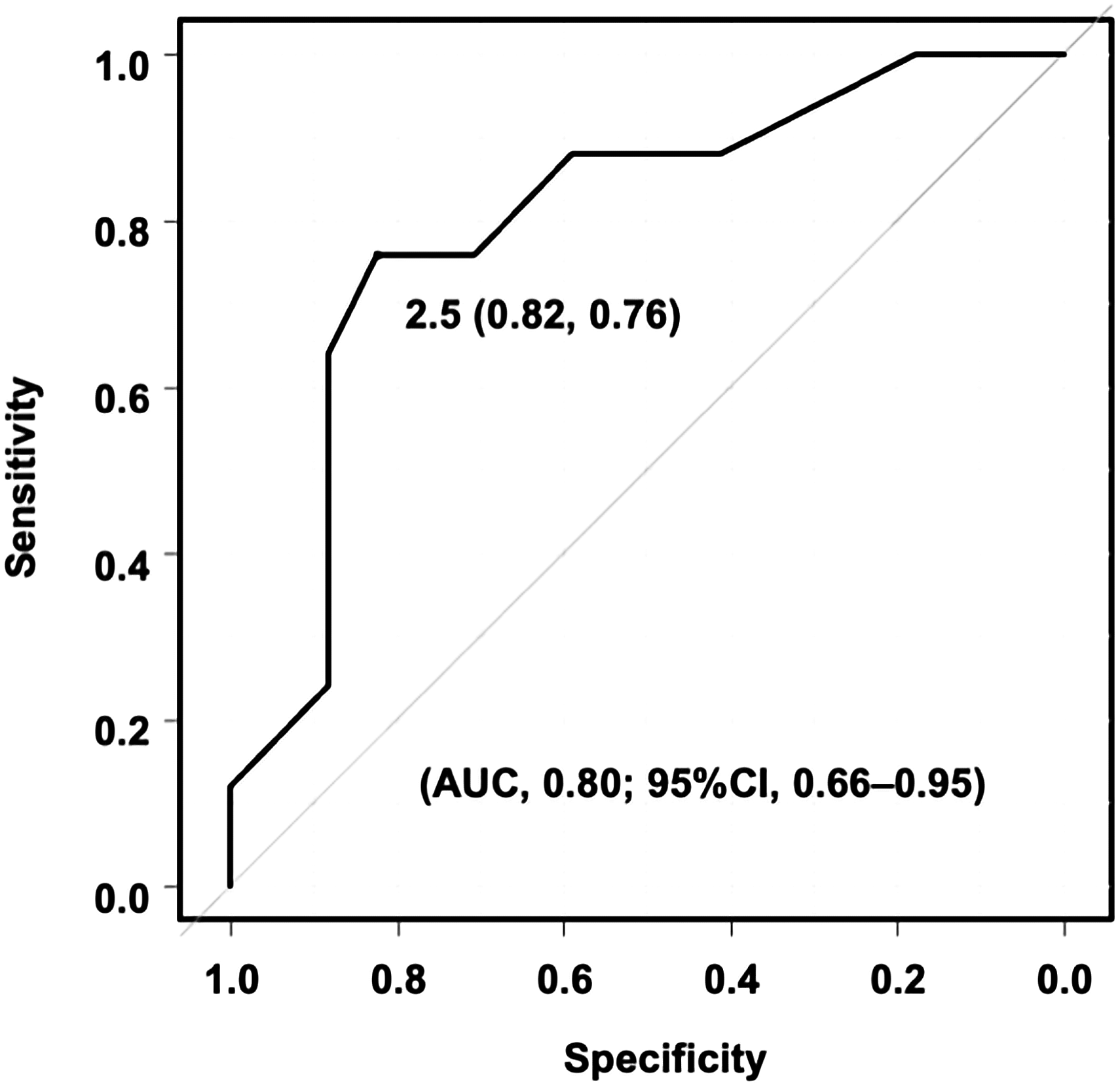
ROC curve of the optimal cut-off for radial artery size to distinguish between RAO and non-RAO groups. AUC, area under the curve; CI, confidence interval; ROC, receiver operating characteristic; RAO, radial artery occlusion.
Multivariate logistic regression analysis of risk factors for RAO.
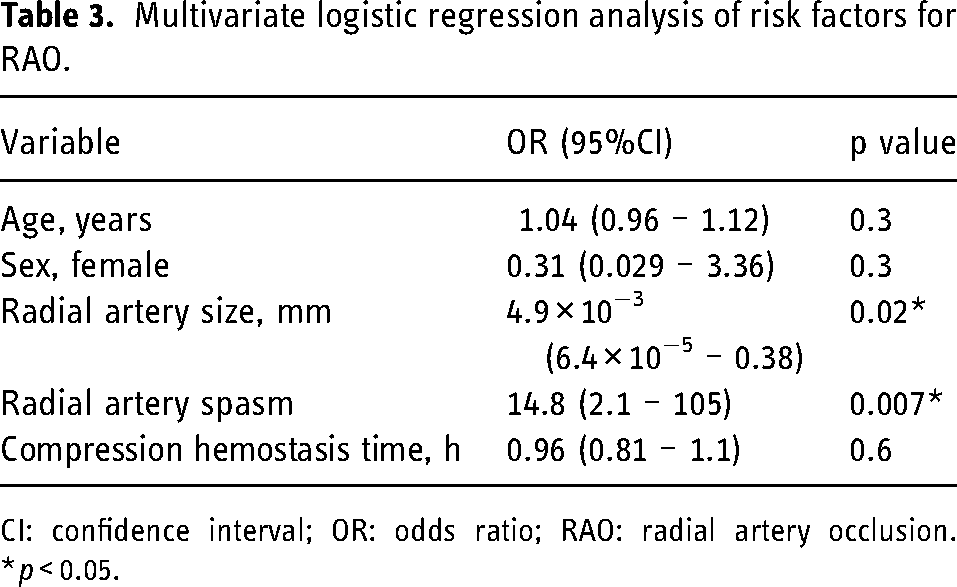
CI: confidence interval; OR: odds ratio; RAO: radial artery occlusion. *p < 0.05.
Illustrative cases
Illustrative case for the RAO group
A 61-year-old man with a growing right posterior communicating aneurysm underwent coil embolization with stent-assisted technique using a 6F guiding sheath (FUBUKI) via right TRA (Figure 3(a)). The radial artery diameter was 2.2 mm, and the patient developed severe RAS during the procedure (Figure 3(b)). The aneurysm was completely embolized, and hemostasis was achieved in a total of 6 h by patent hemostasis method with TR band after the procedure. A right radial artery pulse was palpable at the wrist the day after treatment, but was not palpable 30 days after treatment, although the patient remained asymptomatic. Follow-up angiography 1 year after treatment showed the right radial artery had become occluded without recanalization of the aneurysm (Figure 3(c)).
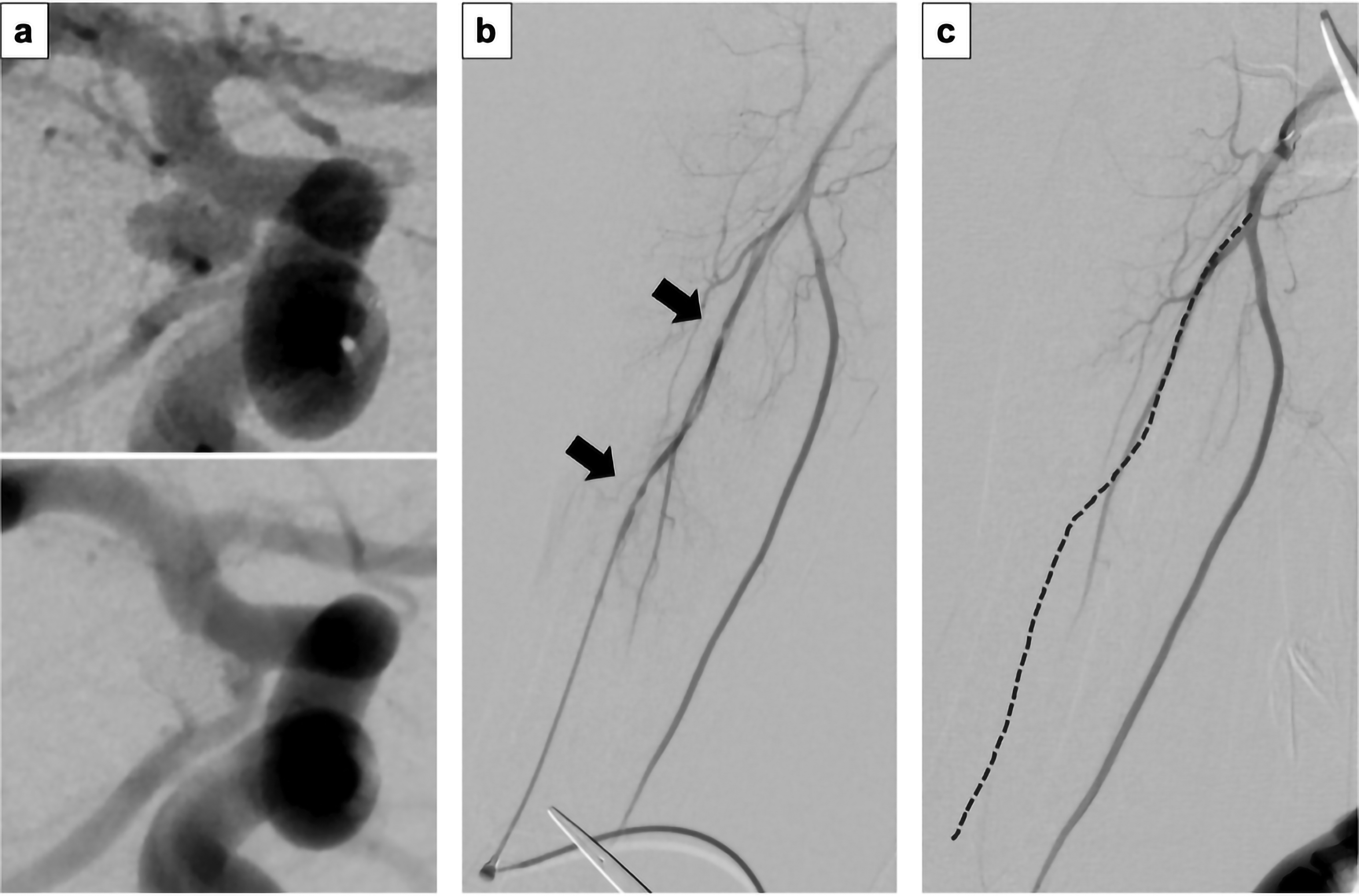
A 61-year-old man with a growing right posterior communicating aneurysm underwent coil embolization with stent-assisted technique using a 6F guiding sheath (FUBUKI) via right TRA. (a) Right internal carotid angiography images. Upper panel: before embolization; lower panel: after embolization. (b) Angiography from the right radial artery of the supinated right forearm, showing the radial artery diameter was 2.2 mm and the patient developed severe radial artery spasm during the procedure. (c) Follow-up angiography from the right brachial artery of the supinated right forearm 1 year after treatment, showing occlusion of the right radial artery. Arrow: radial artery spasm. Dotted line: original route of the radial artery. TRA, transradial access.
Illustrative case for the non-RAO group
A 73-year-old woman underwent coil embolization with stent-assisted technique using a 6F guiding sheath (FUBUKI) via right TRA due to the appearance of a new bleb in the right posterior communicating aneurysm (Figure 4(a)). The radial artery diameter was 2.8 mm, and no RAS was observed intraoperatively (Figure 4(b)). The aneurysm was completely embolized, and hemostasis was achieved in a total of 20 h by patent hemostasis method with TR band after the procedure. A pulse in the right radial artery was palpable at the wrist both the day after treatment and 30 days later. Follow-up angiography 1 year after treatment showed patency of the right radial artery and complete occlusion of the aneurysm (Figure 4(c)).

A 73-year-old woman underwent coil embolization with stent-assisted technique using a 6F guiding sheath (FUBUKI) via right TRA due to the appearance of a new bleb in the right posterior communicating aneurysm. (a) Right internal carotid angiography images. Upper panel: before embolization; lower panel: after embolization. (b) Angiography from the right radial artery of the supinated right forearm, showing the radial artery diameter was 2.8 mm, and no radial artery spasm was observed intraoperatively. (c) Follow-up angiography from the right distal radial artery of the pronated right forearm 1 year after treatment, showing patency of the right radial artery. Arrow: radial artery. TRA, transradial access.
Discussion
In a large retrospective study of 1524 neurointerventional procedures via TRA, local transradial complications were described as radial artery extravasation in 0.3% (4 of 1524), hematoma in 0.3% (4 of 1524), pseudoaneurysm in 0.1% (1 of 1524), compartment syndrome in 0.1% (1 of 1524), infection in 0.1% (1 of 1524), avulsion of the radial artery in 0.1% (1 of 1524), severe RAS in 0.3% (4 of 1524), and RAO in 0.6% (10 of 1524). 12 Among these complications, the present study focused on RAO and identified the small radial artery and RAS as risk factors for RAO after coil embolization of UIAs via TRA.
Incidence of RAO
A meta-analysis in the field of interventional cardiology reported that the frequency of RAO ranges from less than 1% to 33%. 14 In the present study, RAO occurred in 40% (17/42) of patients who underwent coil embolization of UIAs via TRA. The relatively higher incidence of RAO could be attributed to three factors.
First, previous studies on RAO have analyzed the incidence of RAO, including treatment with smaller sheaths.12,14 On the other hand, in the present study, all procedures were performed using 6F guiding sheath applied. Differences in sheath size used between studies were reflected in differences in the incidence of RAO. In a prospective study treated with a 6F sheath, which is comparable in diameter to the sheath used in our study, the incidence of RAO was relatively higher at 30.5%, 20 comparable to our results. Second, the reason for the slightly higher percentage of RAO in the present study compared with those studies may be due to the fact that RAO was assessed by angiography. The majority of previous reports of RAO evaluation methodologies have adopted either palpation or ultrasound of the radial artery to determine RAO. 21 Compared with angiography, which is a more objective method of examination, the more subjective assessment of RAO by palpation or ultrasound may have been underdiagnosis. Third, this may be because the RAO in the present study was evaluated one year after treatment. Most of the previous reports have judged RAO between the time of discharge from the hospital and within 60 days of treatment. 21 The slightly higher incidence of RAO in our study may have included delayed RAO that occurred after 60 days postoperatively.
Notably, however, despite a relatively higher rate of RAO, none of the patients in the present study developed symptomatic RAO. This may be attributed to the preoperative angiographic confirmation of collateral blood flow from the ulnar artery and an intact palmar arch beforehand. 22
Risk factors for postoperative RAO
Risk factors for RAO have been identified in the field of interventional cardiology as lower dose of heparin, longer compression times, higher number of puncture attempts, age, sex, sheath size, and diameter of the radial artery.14,23 Spaulding et al. reported that coronary angiography via TRA in patients with radial artery diameters less than 2.7 mm was associated with a higher risk of RAO. 24 Furthermore, Saito et al. demonstrated that the incidence of RAO increases from 4% when the radial artery inner diameter/sheath outer diameter ratio was >1.07 to 13% for a ratio of <1.0. 25 The mechanism of RAO has been suggested to be thrombosis due to local endothelial injury and cessation of blood flow in the radial artery caused by insertion of the catheter and the sheath.26–28 The present study identified small radial artery diameter as an independent risk factor for RAO, and the ROC curve revealed a cutoff value of 2.5 mm. In addition, patients with a radial artery inner diameter/sheath outer diameter ratio <1.0 displayed a significantly higher risk of RAO than those with a ratio >1.0, supporting the results of Saito et al. The present study also identified RAS as an independent risk factor for RAO. Based on the above, in small radial artery and RAS, guiding catheters induced more local endothelial injury and cessation of blood flow, consequently resulting in a higher frequency of RAO. Furthermore, patients with postoperative forearm pain along the radial artery in the present study demonstrated a tendency toward higher incidence of RAO in univariate analysis, suggesting that the vascular pain may have been associated with vascular injury.
Prevention of postoperative RAO
High-dose heparin and shorter compression times in combination with the patent hemostasis method have been suggested to be effective in preventing RAO.14,24,29 Aykan et al. demonstrated a significantly higher risk of RAO in the 2500-IU heparin group than in the 5000-IU heparin group in a multivariate regression analysis (OR 9.8, 95%CI 1.2–80; p = 0.03). 30 Pancholy et al. showed that patients with compression hemostasis from the end of the procedure for 2 h compared with 6 h were associated with a significantly lower incidence of RAO without any increase in bleeding complications. On the other hand, the same study revealed that if the radial artery remained patent during hemostatic compression, compression time did not affect the incidence of RAO because the preservation of blood flow in the radial artery prevented thrombotic occlusion. 31 In the present study, heparin was administered during treatment, strictly controlled with an activated clotting time of 250 s or higher, and argatroban 60 mg/day was given continuously postoperatively. In addition, no significant difference in compression time was observed between the RAO and non-RAO groups, possibly because the patent hemostasis method was employed.
In recent years, distal TRA (dTRA) has been promoting an alternative approach in the prevention of RAO. In the cardiovascular field, in the single-center randomized trial, the incidence of RAO was significantly reduced in the dTRA group compared with the TRA group (3.7% vs. 7.9%, respectively; p = 0.014). 32 However, in a large-scale, international, multicenter, randomized controlled trial (The DISCO RADIAL Trial) using the 6F Slender Sheath, 650 patients were treated with dTRA and 657 with conventional TRA, resulting in no difference in RAO between groups (0.31% vs. 0.91%; p = 0.29). 33 In their study, the RAO rate of TRA was as low as that of dTRA due to strict patent hemostasis, and the difference was not significant. Based on the above, the rate of RAO may not have decreased in the present study even if dTRA had been employed, because patent hemostasis method was implemented. In the future, further research on this issue is warranted in the field of neurointervention.
Management of RAS
This study revealed that RAS is a risk factor for RAO, so the management of RAS is important. Researchers have previously suggested optimal prophylaxis for RAS, including adequate sedation and analgesia, 34 prophylactic vasodilators, 35 subcutaneous injection of nitroglycerin,36,37 topical warm compress to induce vasodilation, 38 flow-mediated dilatation (inflating a sphygmomanometer above systolic pressure for 5 min and then rapidly deflating it) 39 and axillary brachial plexus or radial nerve block.40,41 Chen et al. demonstrated that the incidence of TRA-induced RAS is up to 20% for patients with no premedication but is lowered to approximately 4% with prophylactic administration of antispasmodic agents. 42 Candemir et al. prospectively indicated that subcutaneous administration of nitroglycerin reduced the frequency of RAS and significantly increased radial artery diameter. 37 In the present study, general anesthesia achieved adequate sedation and analgesia, but most patients were not given vasodilators to prevent RAS, and none of the patients were injected with subcutaneous nitroglycerine prior to puncture.
Regarding vasodilators, diltiazem, verapamil, and isosorbide dinitrate have been commonly administered. The spasmolytic agents to avoid spasm during transradial percutaneous coronary interventions (SPASM3) study showed, compared with diltiazem, verapamil, and isosorbide dinitrate reduced the incidence of RAS in TRA. 43 In addition, the VITRIOL (is Verapamil In TransRadial Interventions OmittabLe?) trial found no significant difference in the incidence of RAS between the verapamil and placebo groups. 44 Because of these findings, isosorbide dinitrate was adopted as the vasodilator for the prevention of RAS in the present study.
Among the 58 patients with UIA who were initially attempted to treat via TRA, four (6.9%) failed to complete procedure due to severe RAS. In addition, some of the patients who successfully achieved procedure despite resistance due to the RAS may have suffered vascular endothelial damage from forceful guidance during navigating of the guiding catheter, resulting in RAO. TRA operators should always keep in mind the possibility of concomitant RAS, and prophylactic administration of vasodilators and gentle procedures are essential. Based on the above, prevention and treatment of RAS by administration of vasodilators may reduce the incidence of RAO.
Limitations
First, all patients in the present study were treated using a 6F guiding sheath, which has a larger outer diameter compared with sheaths used in the field of interventional cardiology, and the risk of RAO with different sheath diameters was not evaluated. Larger sheath size can increase the risk of RAO,20,45 so treatment with a smaller catheter is preferred. However, the application of smaller catheters is accompanied by reduced support and smaller lumens, which greatly limits the adjunctive techniques sometimes required for coil embolization. As Matsushige et al. have pointed out, 46 coil embolization of UIAs has been generally accomplished under the support of an intermediate catheter at our institution for improved maneuverability of the microcatheter and dense coil packing. A 6F guiding sheath allows simultaneous insertion of one intermediate catheter (TACTICS; Technorat Corporation) and one microcatheter or micro-balloon. In the present study, a guiding sheath with a 2F reduction in device outer diameter was adopted to reduce the risk of RAO.47,48
Second, the number of attempted radial punctures could increase the risk of RAO within 30 days after treatment, 23 but was not measured in this study. The small radial artery and RAS, which were identified as risk factors for RAO in the present study, could potentially have influenced the increased number of punctures. 36 However, to avoid the need for more punctures, we punctured under ultrasound guidance, which has been shown to prevent puncture failures. 49
Third, despite the occurrence of RAS in 50% of patients in the present study, little consideration was given to the administration of vasodilators or treatment for RAS as described above. This is because the importance of RAS prevention had not yet been recognized in our institution, given that most neurointerventions were achieved even when RAS occurred. With recognition of the importance of RAS, prophylactic administration of vasodilators and gentle manipulation of catheterization should be kept in mind.
Fourth, the incidence of RAO during 1 year after endovascular treatment via TRA has not been assessed by longitudinal angiography because angiography can be an invasive procedure. In the present study, the radial artery was also imaged simultaneously during angiography as part of the post-embolization assessment of intracranial aneurysms to confirm the presence or absence of patency.
Finally, this study was conducted as a single-center, retrospective study of a moderately sized cohort. Future studies in the area of neurointervention need to be validated in larger prospective multicenter clinical trials, similar to those in the field of interventional cardiology. Despite these limitations, this study is worthwhile in showing that small radial artery and RAS are risk factors for RAO in neurointervention for UIAs via TRA using a 6F guiding sheath.
Conclusions
Radial artery size and RAS offer reliable parameters for predicting RAO 1 year after coil embolization for UIAs via TRA. Prophylaxis against RAS and appropriate indications for TRA in patients with a radial artery larger than 2.5 mm in diameter may reduce the risk of postoperative RAO.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.