
Abstract
Background
While recent studies suggest a benefit of mechanical thrombectomy (MT) for the treatment of patients with isolated large vessel occlusions presenting after 24 hours from the last known well (LKW), the effect of MT for acute cervical tandem lesions (TLs) beyond 24 hours remains unknown. We aimed to evaluate the safety and effectiveness of MT beyond 24 hours of LKW in patients with TLs.
Methods
We conducted a subanalysis study of patients with anterior circulation TL enrolled in a large, multicenter registry between January 2015 and December 2020. Patients were divided into 2 groups: MT beyond 24 hours versus MT 0–24-hour window. Outcomes of interest were functional independence (90-day modified Rankin scale 0-2), complete reperfusion (modified thrombolysis in cerebral infarction 3), delta NIH Stroke Scale (NIHSS), symptomatic intracranial hemorrhage (sICH), parenchymal hematoma 2 (PH2), in-hospital mortality, and 90-day mortality. Inverse probability of treatment weighting (IPTW) was used to balance the groups.
Results
Overall, 589 participants were included, with 33 treated beyond 24 hours and 556 treated in the 0–24-hour window. After IPTW, we found no significant difference in the rates of achieving functional independence (odds ratio (OR) = 0.51; 95% confidence interval (CI) 0.22–1.16; p = 0.108), complete reperfusion (OR = 1.35; 95% CI 0.60–3.05; p = 0.464), sICH (OR = 1.96; 95% CI 0.37–10.5; p = 0.429), delta NIHSS (β = −3.61; 95% CI −8.11 to 0.87; p = 0.114), PH2 (OR = 1.46; 95% CI 0.29–7.27; p = 0.642), in-hospital mortality (OR = 1.74; 95% CI 0.52–5.86; p = 0.370), or 90-day mortality (OR = 1.37; 95% CI 0.49–3.83; p = 0.544) across both time windows.
Conclusions
Our results suggest that MT appears to benefit patients with TLs beyond 24 hours from LKW. Future prospective studies are warranted.
Introduction
Tandem lesions (TLs) account for about 15% to 20% of all large vessel occlusions (LVOs).1–3 Mechanical thrombectomy (MT) is the first-line treatment for intracranial LVOs; however, due to the additional technical complexity of endovascular treatment of TLs, most patients with TLs were excluded from several landmark clinical trials.2,4 Nevertheless, the current evidence available from large international multicenter registries has demonstrated the safety and efficacy of MT in TLs.1,5,6
The American Heart Association/American Stroke Association guidelines and European Stroke Association guidelines provide a class I recommendation for the use of MT in selected ischemic stroke patients with LVOs up to 24 hours of last known well (LKW).7,8 Recently, the Analysis Of Pooled Data From Randomized Studies Of Thrombectomy More Than 6 Hours After Last Known Well (AURORA) patient-level meta-analysis confirmed this benefit. 4 Of note, the treatment effect of MT was stronger in patients randomly assigned within 12 to 24 hours than those randomly assigned within 6 to 12 hours, suggesting that the effect of MT may continue to be present beyond the 24-hour time window. 4 Therefore, recent retrospective cohort studies have shown that MT for LVOs beyond 24 hours from LKW is feasible and appears to be associated with similar outcomes as in late window trials.9–16
With the exception of one registry, 17 the current evidence of MT in patients with TLs is primarily limited to patients presenting within 8 hours from LKW.1,5,6 The role of MT for TLs beyond 24 hours of LKW and the impact of the time between LKW and puncture on patient outcomes is unknown. We aimed to evaluate the safety and effectiveness of MT beyond 24 hours of LKW patients with TLs compared to patients treated with MT in TLs treated in the 0 to 24-hour window.
Methods
This study was approved under the waiver of informed consent by the local institutional review board at each participating center, and it is reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 18
Study population
We conducted a subgroup analysis study using pooled data from a multicenter cohort registry. Patient eligibility and methods of collaboration have been reported previously. 17 Briefly, the cohort consisted of consecutive adult patients with TLs undergoing MT between January 2015 and December 2020. A TL was defined as an intracranial LVO (petrous, sigmoid, or terminus segment of the internal carotid artery (ICA) or M1 or proximal M2 segment of the middle cerebral artery) with a concomitant cervical carotid occlusion or extracranial ICA stenosis >50% as defined by the NASCET criteria. 12 Patients were eligible if they were ≥18 years and underwent MT for intracranial occlusion (isolated extracranial ICA lesions were excluded). The extracranial ICA lesion was evaluated on admission by computed tomographic angiography, magnetic resonance angiography, and/or intraprocedural digital subtraction angiography.
Patients were divided into two groups depending on the time from LKW to groin puncture: (1) >24-hour MT window group and (2) 0 to 24-hour MT window group. All intracranial occlusions were treated using a stent retriever and/or contact aspiration catheters. Cervical endovascular treatment and medical therapeutic interventions, including antiplatelet management and intravenous thrombolysis (IVT) administration, were performed according to the protocol of each institution under conscious sedation or general anesthesia and at the discretion of the neurointerventionalists.
Data collection
The variables included research center, demographics (age, sex, and race), comorbidities (hypertension), baseline National Institute of Health Stroke Scale (NIHSS), baseline modified Rankin scale (mRS), use of IVT, use of general anesthesia, ICA stenting, cervical ICA complete occlusion, cervical ICA lesion etiology, Alberta Stroke Program Early Computed Tomography Score (ASPECTS), and use of perfusion imaging (computed tomography perfusion or magnetic resonance perfusion).
Study outcomes
The primary study outcomes were functional independence and symptomatic intracranial hemorrhage (sICH) which were analyzed separately. Functional independence (90-day mRS 0-2) was obtained by board-certified vascular neurologists during a routinely scheduled clinical visit or by a certified nurse during a standardized telephone interview at each center. sICH was defined according to the European Collaborative Acute Stroke Study (ECASS-3) criteria. 19
Secondary study outcomes included: (1) successful reperfusion (modified thrombolysis in cerebral infarction (mTICI) 2b-3), defined as antegrade reperfusion of previously more than half and completely occluded target artery territory, respectively 20 ; (2) complete reperfusion (mTICI 3); (3) delta NIHSS, defined as the NIHSS at hospital admission minus the NIHSS calculated upon hospital discharge; (4) parenchymal hematoma type 2 (PH2) according to the Heidelberg Bleeding Classification 21 ; (5) in-hospital mortality; and (6) 90-day mortality.
Statistical analysis
Descriptive statistics were used to summarize continuous and categorical variables. We reported categorical variables as counts and percentages and continuous variables as means (SD) or medians (interquartile range). Shapiro-Wilk test and histograms were used to assess normality of distributions. For the univariable analysis, we used Student's t-tests or Wilcoxon rank-sum test for continuous variables and chi-square or Fisher's exact test for categorical variables, as needed.
Clinically relevant variables for the outcomes of interest were considered for adjustment. Missing data for these variables were handled through a multiple imputation by chained equations method if missing observations accounted for <20% of total observations. 22 Otherwise, they were not included in the analysis. Quality of imputation was assessed graphically through a density plot and a strip plot for original and imputed observations.
To compare the outcomes between groups, we performed matching using inverse probability of treatment weighting (IPTW) to generate pseudo-populations stratified by treatment. IPTW was selected based on variable balance, preservation of cases treated beyond 24 hours, and reduced bias in small sample sizes. 23 Propensity scores were estimated using a generalized boosted model with the following covariates: admission NIHSS, ASPECTS, perfusion imaging, and use of IVT. These covariates were measured before the assignment of treatment. They are also known to be associated with our primary study outcomes and were selected a priori based on previous literature11,24 and expert knowledge on the topic. 25 Variables that were only related to the exposure but not to the outcome were not selected. 25 Absolute standardized mean differences <0.1 were taken to imply the absence of substantial imbalance between the weighted treatment groups. 26 Baseline patient characteristics were compared again after IPTW. For each continuous variable, analysis of variance was used with weights coming from IPTW. For each categorical variable, a weighted logistic regression analysis was used. 27
To estimate the effect of MT >24 hours on the efficacy and safety outcomes, we used a survey-weighted generalized linear model. 28 We performed a secondary analysis comparing patients in the >24-hour window only with those in the 6 to 24-hour window since both populations probably shared similar hemodynamic pathophysiological features based on their selection methodology. 16 For this, we excluded patients with LKW times <6 h and performed IPTW adjustment. We then explored outcomes in the same fashion as outlined before. All the statistical analyses were considered significant at a two-sided alpha level of ≤0.05 set as statistical significance and were conducted using R version 4.1.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Baseline characteristics
Of the 691 patients from the registry, 102 were excluded (Figure 1). Of the 589 patients included, 556 were treated between the 0 and 24-hour window and 33 were treated >24 hours after stroke onset or LKW. Compared with the 0 to 24-hour window group, the group treated with MT beyond 24 hours from LKW were less frequently white (43.8% vs. 65.1%, p = 0.014), had a lower median baseline NIHSS (10 [4–17] vs. 16 [11–20], p = <0.001), were more frequently treated with ICA stenting (78.8% vs. 59.7%, p = 0.029), and more frequently required intravenous intraprocedure antiplatelets (57.6% vs. 31.3%, p = 0.008) (Supplemental Table 1). No significant differences were observed in the remaining baseline or procedural characteristics. After IPTW adjustment, there were no differences among the variables included in the IPTW (Supplemental Figure 1).
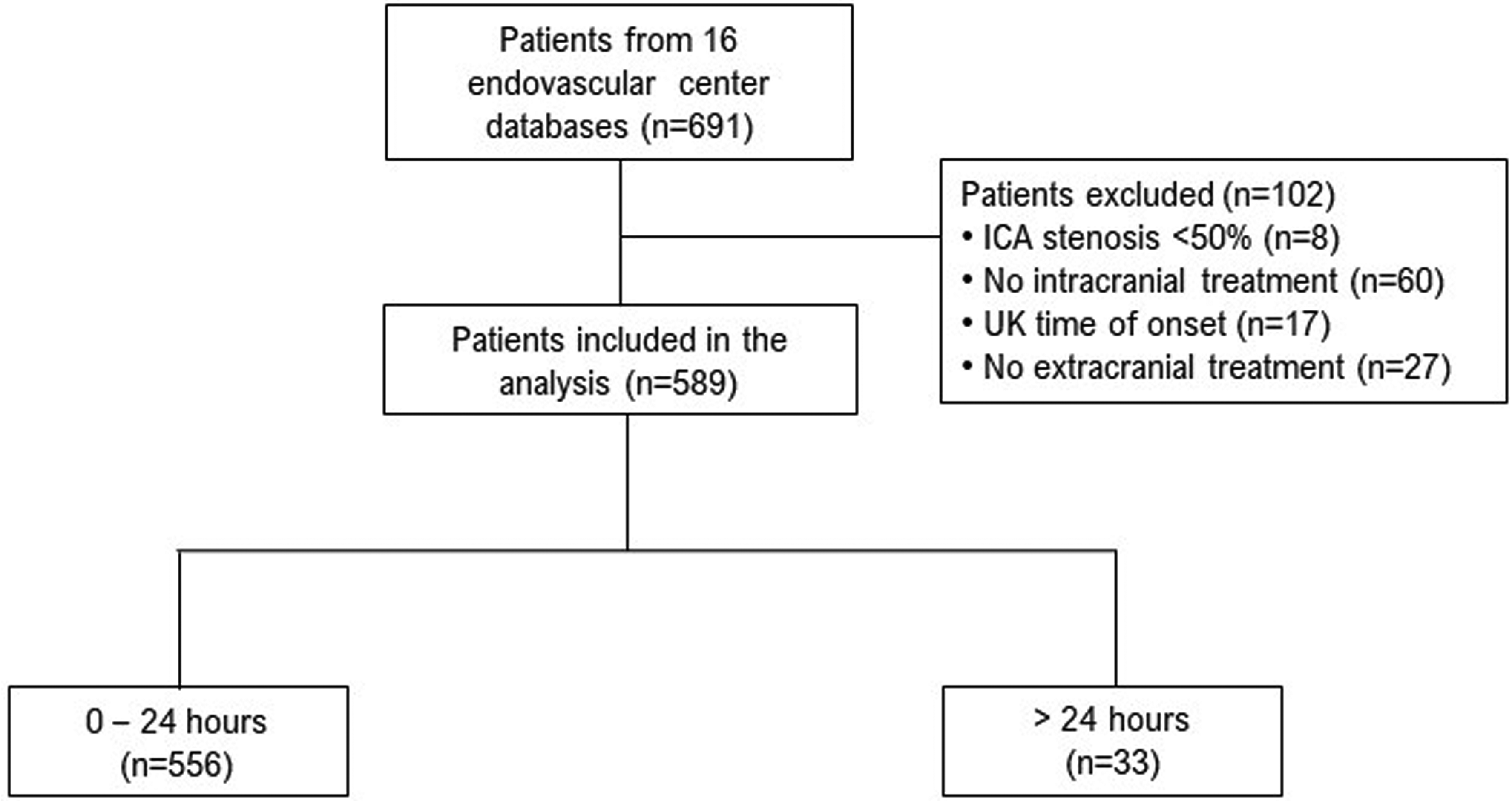
Flow diagram of patients included in the study. ICA: internal carotid artery; UK: unknown.
Primary analysis
Compared with the 0 to 24-hour window group, patients who underwent MT after 24 hour had similar mRS scores at 90 days (Figure 2). Then, to estimate the effect of >24-hour time window on outcomes and its standard error, we performed a survey-weighted generalized linear regression model. No significant difference was observed in the odds of achieving functional independence (odds ratio (OR) = 0.51; 95% confidence interval (CI) 0.22–1.16; p = 0.108), sICH (OR = 1.96; 95% CI 0.37–10.5; p = 0.429), complete reperfusion (OR = 1.35; 95% CI 0.60–3.05; p = 0.464), delta NIHSS (β = −3.61; 95% CI −8.11 to 0.87; p = 0.114), PH2 (OR = 1.46; 95% CI 0.29–7.27; p = 0.642), in-hospital mortality (OR = 1.74; 95% CI 0.52–5.86; p = 0.370) or 90-day mortality (OR = 1.37; 95% CI 0.49–3.83; p = 0.544) across both time windows (Table 1).
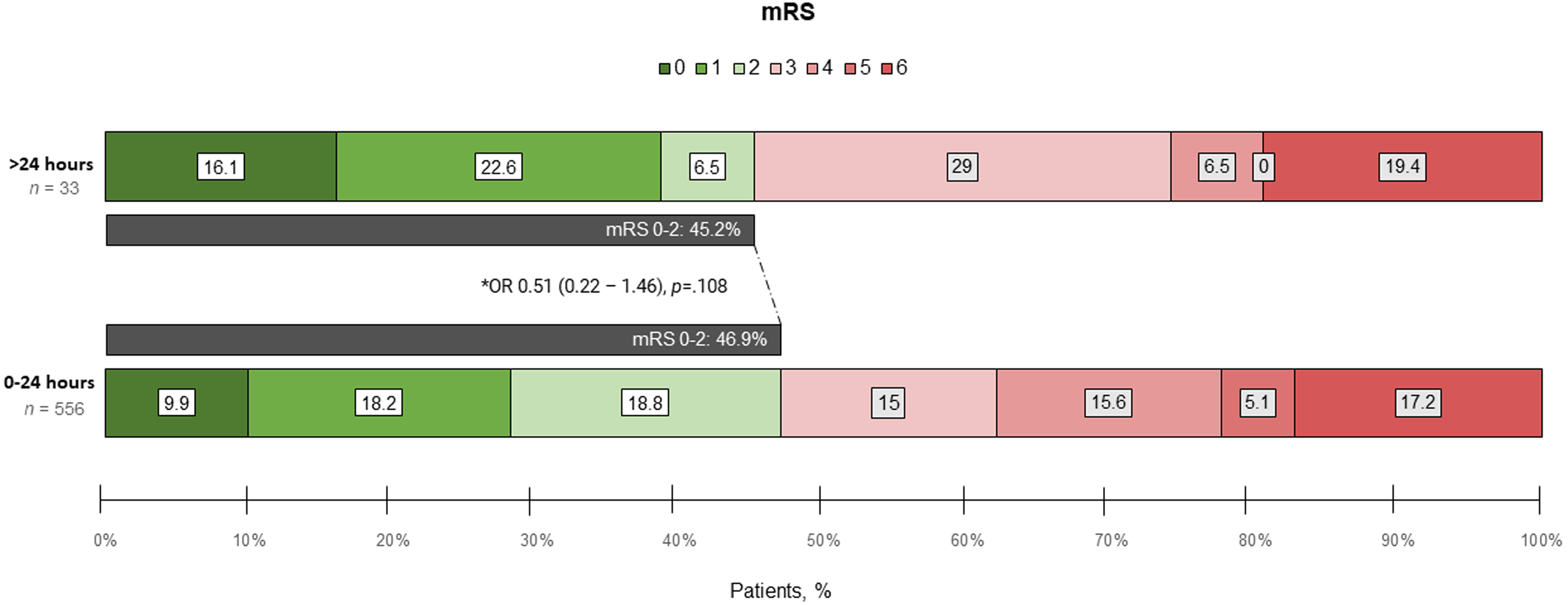
Distribution of the modified Rankin Scale (mRS) at 90 days comparing mechanical thrombectomy in the 0 to 24-hour and >24-hour time windows.
Outcomes of patients with endovascularly treated tandem occlusion stroke according to the treatment window: 0 to 24 versus >24 hours.
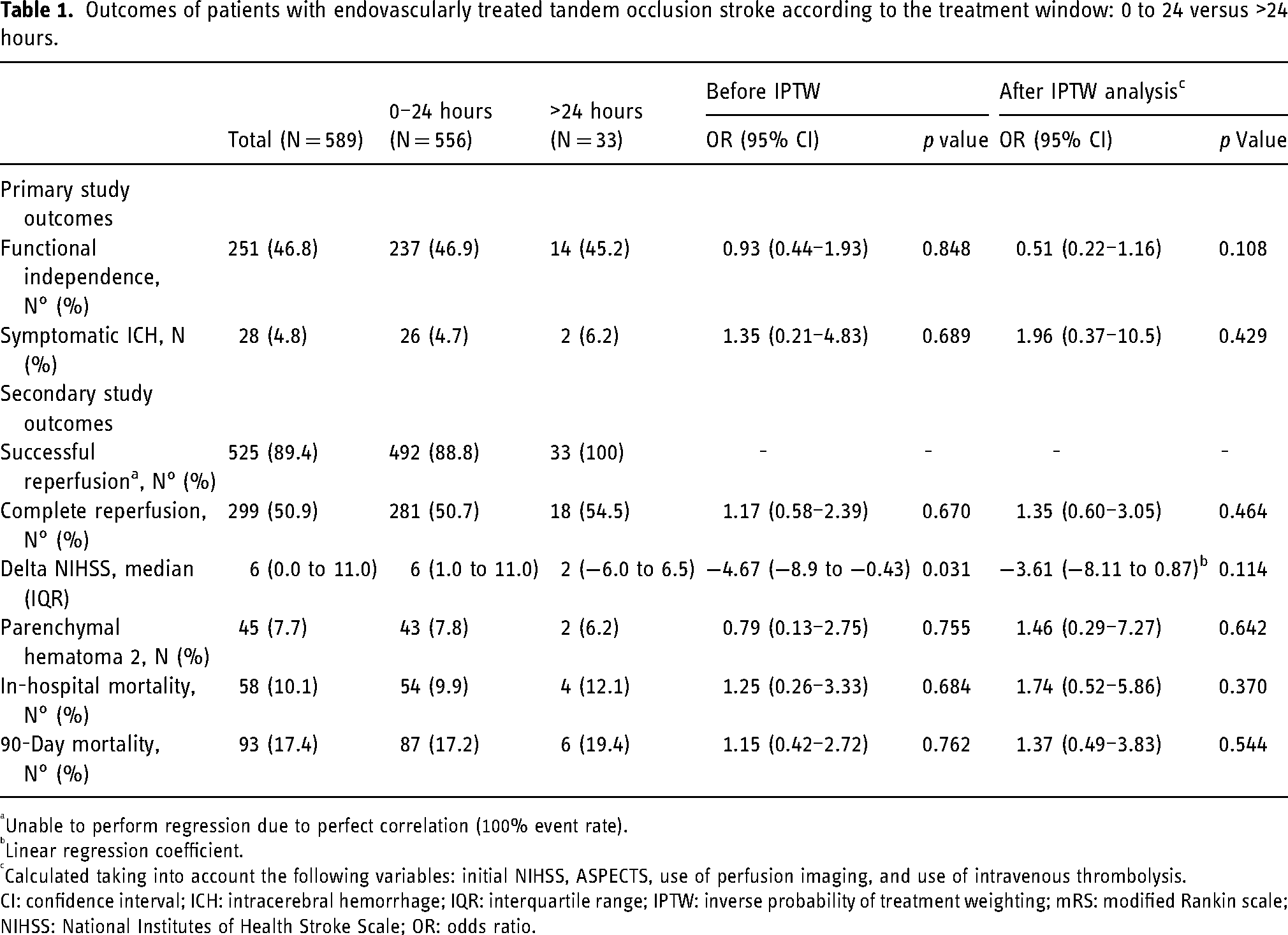
Unable to perform regression due to perfect correlation (100% event rate).
Linear regression coefficient.
Calculated taking into account the following variables: initial NIHSS, ASPECTS, use of perfusion imaging, and use of intravenous thrombolysis.
CI: confidence interval; ICH: intracerebral hemorrhage; IQR: interquartile range; IPTW: inverse probability of treatment weighting; mRS: modified Rankin scale; NIHSS: National Institutes of Health Stroke Scale; OR: odds ratio.
Secondary analysis
6–24-hour window versus >24-hour window
In the secondary analysis, patients in the 6 to 24-hour window were compared against patients treated with MT beyond 24 hour. Similar to the primary analysis, no significant difference was observed for functional independence, complete reperfusion, delta NIHSS, sICH, PH2, in-hospital mortality, or 90-day mortality across both groups (Supplemental Table 2).
Discussion
We conducted a subanalysis of a multicentric registry from 16 centers to compare the clinical outcomes of MT beyond 24 hours with those of treatment within 0 and 24 hours for TLs. Our findings suggest that MT performed beyond 24 hours is feasible and has similar rates of functional independence, complete reperfusion, sICH, PH2, and 90-day mortality compared with treatment between 0 to 24 and 6 to 24 hours from LKW.
Evidence about the efficacy of MT in isolated LVOs beyond 24 hours is limited to findings from case series or retrospective studies with limited sample sizes.9–11,13–16,29 The multicenter retrospective cohort reported by Sarraj et al. showed that MT in patients with LVO treated beyond 24 hours from LKW was associated with higher odds of functional independence (90-day mRS 0–2) compared with medical management, despite increased odds of sICH. 15 Moreover, Dhillon et al. found that patients with LVO treated with MT beyond 24 hours from onset presented comparable safety and functional outcomes to MT between 6 and 24 hours, which is in line with the findings by Desai et al.10,11
In the case of TLs, Zapata et al. assessed the impact on MT for patients with TL presenting within 6 to 24 hours after LKW using the DAWN 30 or DEFUSE-3 31 eligibility criteria. 32 They reported a 90-day mRS 0–2 rate of 57.8% in patients with the atherothrombotic subtype and 42.9% in the cardioembolic subtype group. 32 In our study, we observed that in 33 patients with TLs treated with MT beyond 24 hours from LKW, the rate of functional independence (90-day mRS 0–2) was 45.2%. Despite the very late window presentation (>24 hours from LKW), a large proportion of patients underwent acute cervical stenting (79%), which has been associated with increased odds of better clinical outcomes. 17 Considering that atherothrombotic TLs were the predominant etiology in our population (78.5%), the functional independence rates in both the >24-hour (45.2%) and the 0 to 24-hour (46.9%) groups were lower than those reported by Zapata et al. 32 but similar to the AURORA meta-analysis (45.9%). 4
Recent evidence suggests that, as time progresses, the characteristics and composition of the clot changes over time and renders the thrombus less amenable to MT.33,34 This is a consequence of time-dependent formation of fibrin within the clot and of the neutrophil extracellular traps that consolidate its structure.35,36 We found that successful reperfusion (mTICI 2b-3) was achieved in all the patients treated beyond 24 hours (33/33), while complete reperfusion (mTICI 3) was achieved in 54.5%. Our successful reperfusion rate is higher than previously reported in isolated very late window (>24 h) LVO studies (range from 76% to 81%).9–11,13 Interestingly, the rate of successful reperfusion observed in our very late window group was also higher than that reported by Zapata et al. (93.6%). 32 This might be the result of the improved flow due the increased use of carotid recanalization using stenting (79%), and the frequent use (85%) of “aggressive” intraprocedural antiplatelet medication (intravenous or dual loading oral antiplatelet therapy) in patients who underwent MT beyond 24 hours. 37 In addition, differences in thrombi composition between carotid atherosclerotic plaques and large artery atherosclerosis38,39 may contribute to facilitating recanalization in carotid lesions in comparison with LVOs.
The sICH rate of 6.2% in patients undergoing MT beyond 24 hours is slightly higher than reported by Zapata et al. (4.7%) 32 but similar to that reported in studies of MT in LVO beyond 24 h (range from 5% to 9%).9–11 Additionally, our rate of sICH was similar to that reported in the AURORA meta-analysis (5.3%). 4 Currently, evidence about the effect of time on the risk of hemorrhage is conflictive. It has previously been reported that time from onset to reperfusion is a predictor of the risk of intracerebral hemorrhage and parenchymal hematoma in patients treated with endovascular treatment.40,41 However, a meta-analysis of three MT trials showed no effect of time on sICH. 42 In TLs the potential risk of hemorrhage is important due the combination of a large clot burden, the potential need for periprocedural antiplatelet therapy when acute carotid artery stenting is used, and the use bridging therapy with IVT.43–46 We observed that while both groups had a similar baseline ASPECT, the use of cervical stenting and any IV or dual loading antiplatelet therapy was significantly higher in patients treated with MT beyond 24 hours. However, we found no significant difference in the risk of sICH for patients in the very late window compared to the 0 to 24-hour group. Similarly, the risk of PH2 was not different between groups, suggesting that, not the use of antiplatelets but rather other factors including baseline core infarct and post-MT unstained hypertension after reperfusion may be more important factors associated with an increase incidence of reperfusion hemorrhage.
This study has several limitations. Being that it was a secondary analysis from a retrospective registry, there is an inherent risk of selection bias. This is especially true for our study groups, as patients were not standardized or randomized for the very late window treatment group. In fact, the increased use of perfusion imaging for selection of patients in the very late window confirms basic differences between both groups. To reduce this risk of bias, we used matching methods with good performance in relatively small sample sizes and ensured adequate balance among confounding variables associated with the outcomes of interest. 23 However, matching does not eliminate bias and may increase bias if confounding patient characteristics are not measured or included in the model. To ameliorate this risk, we included all variables previously reported in the largest TL registries.1,5,17,47 Moreover, the main result did not change when the comparison was made with a more similar TL cohort treated between 6 and 24 hours. An additional limitation relates to missing data. Even though we did not have any variables with a significant (>20%) number of missing observations, some required multiple imputations. While this method is less prone to bias as it uses remaining observations from the same and other variables to estimate missing values, it may be more prone to overfitting. Lastly, a majority of the patients (79%) in the 0 to 24-hour window group received endovascular treatment within the initial hours (within 12 hours from LKW).
Conclusion
Our results suggest that MT for TLs beyond 24 hours from LKW is feasible and appears to be safe in adequately selected patients. Given the small sample size, our findings should be interpreted cautiously and need to be validated in future prospective studies.
Supplemental Material
sj-docx-1-ine-10.1177_15910199231196960 - Supplemental material for Mechanical thrombectomy beyond 24 hours from last known well in tandem lesions: A multicenter cohort study
Supplemental material, sj-docx-1-ine-10.1177_15910199231196960 for Mechanical thrombectomy beyond 24 hours from last known well in tandem lesions: A multicenter cohort study by Aaron Rodriguez-Calienes, Ameer E Hassan, James E Siegler, Milagros Galecio-Castillo, Mudassir Farooqui, Mouhammad A Jumaa, Nazli Janjua, Afshin A Divani, Marc Ribo, Michael Abraham, Nils H Petersen, Johanna Fifi, Waldo R Guerrero, Amer M Malik, Thanh N Nguyen, Sunil Sheth, Albert J Yoo, Guillermo Linares, Yujing Lu, Juan Vivanco-Suarez and Santiago Ortega-Gutierrez in Interventional Neuroradiology
Footnotes
Declaration of conflicting interests
AEH: (1) Consultant/Speaker—Medtronic, Microvention, Stryker, Penumbra, Cerenovus, Genentech, GE Healthcare, Scientia, Balt, Viz.ai, Insera therapeutics, Proximie, NeuroVasc, NovaSignal, Vesalio, Rapid Medical, Imperative Care and Galaxy Therapeutics. (2) Principal Investigator: COMPLETE study—Penumbra, LVO SYNCHRONISE—Viz.ai, Millipede Stroke Trial—Perfuze, RESCUE—ICAD—Medtronic. (3) Steering Committee/Publication committee member: SELECT, DAWN, SELECT 2, EXPEDITE II, EMBOLISE, CLEAR, ENVI, DELPHI, DISTALS. (4) DSMB—COMAND trial. JES—Reports serving on the speaker's bureau for AstraZeneca. AAD—Received the following fundings: the University of New Mexico Center for Brain Recovery and Repair Center of Biomedical Research Excellence through Grant Number (NIH P20GM109089, Pilot PI), W81XWH-17-2-0053 (PI), 1R21NS130423-01 (PI). Ortega-Gutierrez–Grants: NIH-NINDS (R01NS127114-01), Stryker, Medtronic, Microvention, Methinks, IschemiaView, Viz.ai, Siemens. Consulting fees: Medtronic, Stryker Neurovascular.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.