
Abstract
Background
Recently, the angled-tip Zoom™ aspiration catheters were introduced. The tip is designed to improve suction force for clot retrieval. We evaluated the possibility of reducing procedure costs when using angled-tip catheters and compared the safety and angiographic effectiveness of angled-tip versus straight-tip catheters.
Methods
We conducted a retrospective single-center cohort study involving patients with acute ischemic stroke due to large and medium vessel occlusions. The patients were divided into two groups: the post-Zoom group, in which angled-tip aspiration catheters were used and the pre-Zoom group, in which traditional straight-tip catheters were employed.
Results
A total of 163 patients were included; 95 (58.3%) in the pre-Zoom group and 68 (41.7%) in the post-Zoom group. The groups were well-matched at entry. The post-Zoom group demonstrated a significant decrease in mean procedure cost ($9728 vs. $12,127; p = 0.002), shorter time to achieve modified thrombolysis in cerebral infarction ≥2b reperfusion (38.30 min vs. 53.26 min; p = 0.018), and shorter puncture to procedure completion time (46.42 min vs. 62.38 min; p = 0.022). Additionally, the mean procedural cost when using the ADAPT technique supported by the Zoom catheters was significantly lower than the Solumbra technique ($5754 ± $2806 vs. $13,498 ± $3244, p < 0.001). There were no differences in the rate of hemorrhage between the pre-Zoom group (17.9%) and the post-Zoom group (20.6%), p = 0.690.
Conclusion
The study demonstrated significant benefits, including cost reduction and shorter time to achieve reperfusion in patients treated with Zoom aspiration catheters. These findings support the use of angled-tip catheters in acute ischemic stroke management.
Introduction
Mechanical thrombectomy has emerged as a superior treatment for patients with acute ischemic stroke caused by large vessel occlusion, surpassing the efficacy of medical therapy, as proven by multiple randomized clinical trials.1–6 Traditionally, stent retrievers have been the primary devices used for thrombectomy. However, direct contact aspiration has emerged as a viable alternative with comparable outcomes.7–11 The COMPASS trial compared a direct aspiration first-pass technique (ADAPT) to first-line stent retriever treatment and demonstrated non-inferiority of ADAPT in terms of treatment outcomes for large vessel occlusions. 11 ADAPT also offers the benefits of faster reperfusion and lower costs.
Recently, the angled-tip access and aspiration catheters (Imperative Care Inc., Campbell, CA) were introduced as an innovative option for aspiration thrombectomy, featuring the Zoom™ 35–71 aspiration catheters, Zoom™ 88 Large Distal Platform (access catheter), Zoom PODTM, and Zoom™ pump. Emerging evidence suggests that the use of angled-tip Zoom aspiration catheters may lead to higher recanalization rates, shorter procedure times, and improved reperfusion outcomes.12–15 The unique angled-tip aspiration catheters, which are angled 60°, are specifically designed to enhance clot engagement through increased surface area. 16
However, there is limited data available regarding cost comparisons between the Zoom catheters and other thrombectomy devices, in particular stent retrievers. Therefore, the primary objective of this study is to evaluate the real-world experience before and after the introduction of the Zoom catheters at our institution and assess the associated costs of performing mechanical thrombectomy procedures during these two-time intervals.
Methods
Study design
This retrospective study was conducted at a single center. The stroke research protocol employed in this study received approval from our Institutional Review Board.
Data collection
We extracted deidentified data from our institutional stroke database, which was collected prospectively and securely stored. The dataset comprises comprehensive information on patient demographics, including age, gender, and relevant medical history. Additionally, it includes detailed data on occlusion location, performed procedures, and the time elapsed from arterial puncture to recanalization.
Patient population
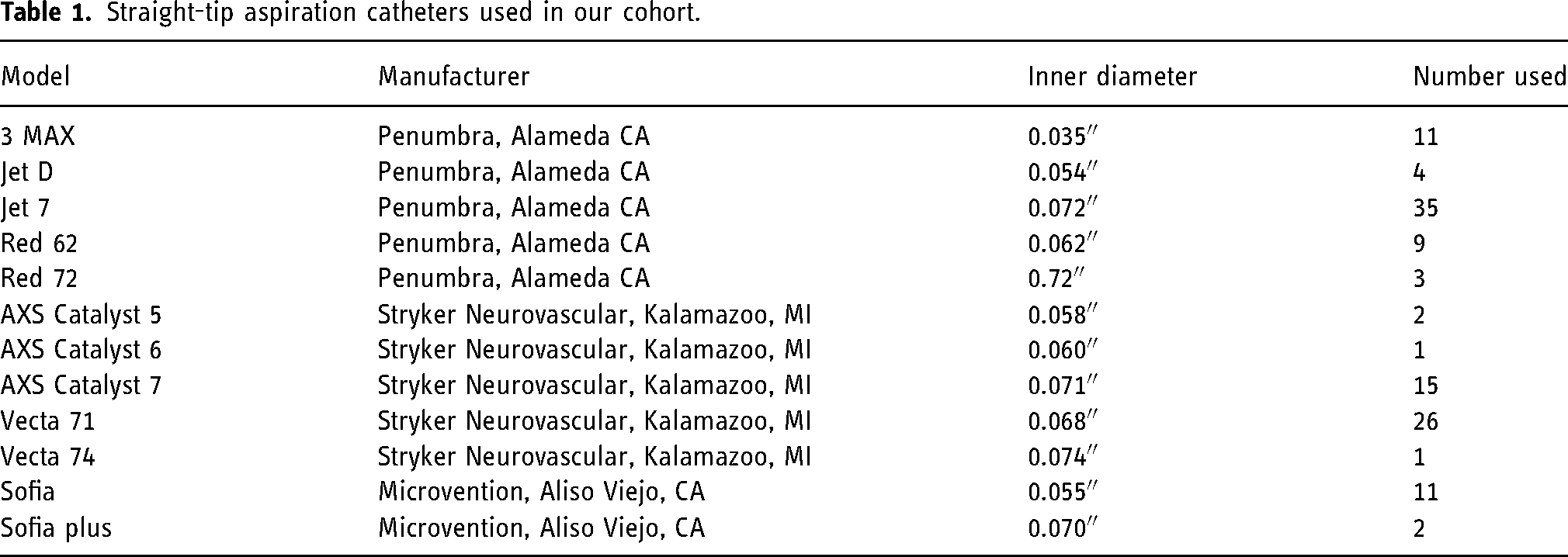
We included consecutive patients with acute ischemic stroke secondary to large and medium vessel occlusion, including tandem lesions. The occlusion locations included the internal carotid artery (ICA), middle cerebral artery (MCA), anterior cerebral artery (ACA), posterior cerebral artery (PCA), vertebral artery (VA), and basilar artery (BA). All patients were treated in our comprehensive stroke center by a single operator. Patients treated within the 18-month period preceding the introduction of the Zoom aspiration catheter using traditional straight-tip catheters were assigned to the pre-Zoom group, while those treated with the Zoom aspiration catheters (angled-tip catheters, Figure 1) were assigned to the post-Zoom group. A complete listing of all straight-tip and angled-tip catheters used in this study is provided in Tables 1 and 2, respectively.
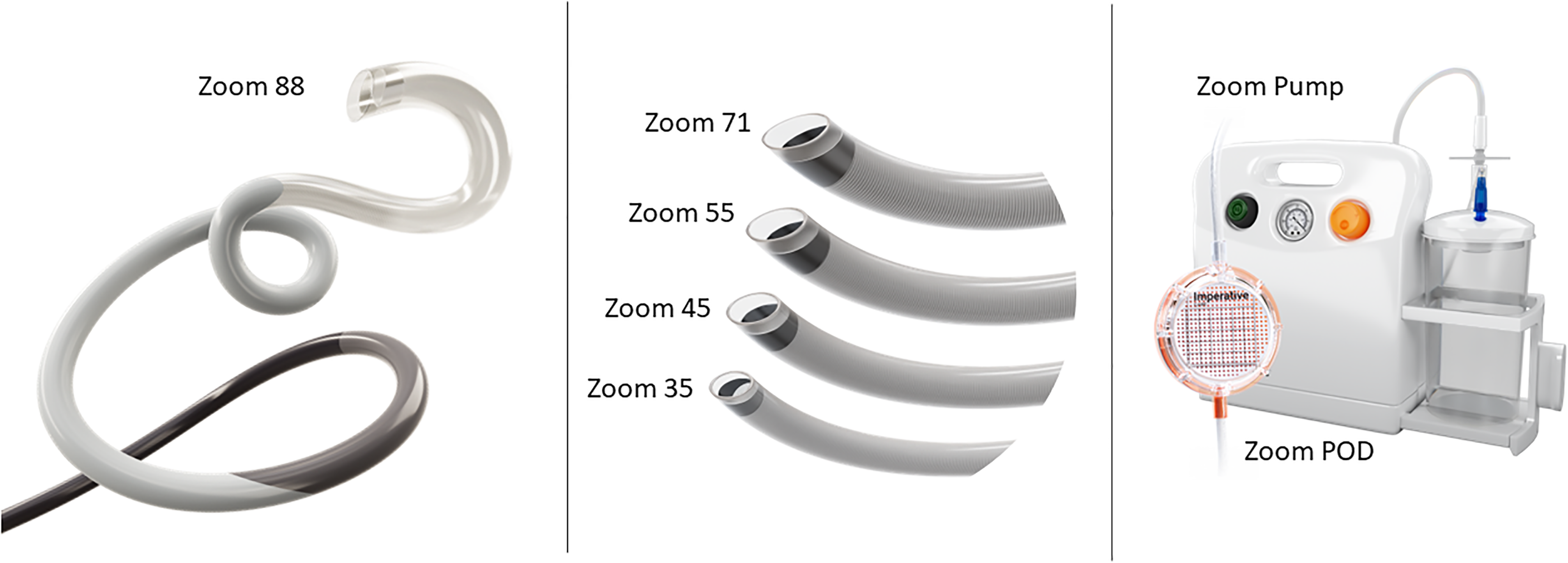
The angled-tip Zoom™ 88 large distal platform (left), the angled-tip Zoom™ aspiration catheters (middle), and the Zoom™ pump and Zoom™ POD (right). Image courtesy of Imperative Care (reprinted with permission).
Straight-tip aspiration catheters used in our cohort.
Angled-tip aspiration catheters used in our cohort.

Study assessments
Our primary analysis was a cost comparison between the pre- and post-Zoom groups using the list prices associated with each device employed in the procedures. The secondary analysis was focused on safety and procedural outcomes including self-adjudicated modified thrombolysis in cerebral infarction (mTICI) reperfusion scores and time from puncture to reperfusion. In patients where mTICI ≥ 2b or mTICI ≥ 2c reperfusion was not achieved, the procedure completion time was imputed to provide a conservative estimate of the time from puncture to reperfusion. We also assessed safety and effectiveness outcomes of the Solumbra technique which utilizes a combination of aspiration catheters and stent retrievers versus the ADAPT technique.
Statistical methods
Statistical analyses were performed using Minitab 21.4.0 statistical software (Minitab Inc., State College, PA). Aggregate data, including patient demographics, baseline characteristics, effectiveness, and safety were summarized by descriptive statistics. Mean and standard deviation were generally reported for continuous variables. p-values for differences between two groups were calculated using the two sample t-test for means. Fisher's exact test was used to compare frequencies. Values with p < 0.05 were considered significant.
Results
From January 2020 to March 2023, a total of 165 ischemic stroke patients were treated for intracranial occlusions in large and medium vessels. Two cases with missing data were excluded, resulting in a final analysis of 163 patients. Among these, 95 patients (58.3%) were treated using straight-tip catheters (pre-Zoom group), while the remaining 68 patients (41.7%) were treated using angled-tip catheters (post-Zoom group).
Baseline and procedure characteristics
No statistical differences were found between the two treatment groups regarding the baseline characteristics of the study patients (Table 3). The procedure characteristics of both treatment groups are presented in Table 4. The pre-Zoom group exhibited a significantly higher rate of ICA occlusions (24.2%, 23/95) compared to the post-Zoom group (5.9%, 4/68), p = 0.002. Additionally, there was a significant disparity in the utilization of larger diameter 0.018″–0.024″ guidewires, with 14.7% (14/95) in the pre-Zoom group and 77.9% (53/68) in the post-Zoom group, p < 0.001 (Table 2). Moreover, the utilization of the ADAPT technique was significantly lower in the pre-Zoom group (13.7%, 13/95) compared to the post-Zoom group (55.9%, 38/68), p < 0.001 (Figure 2).
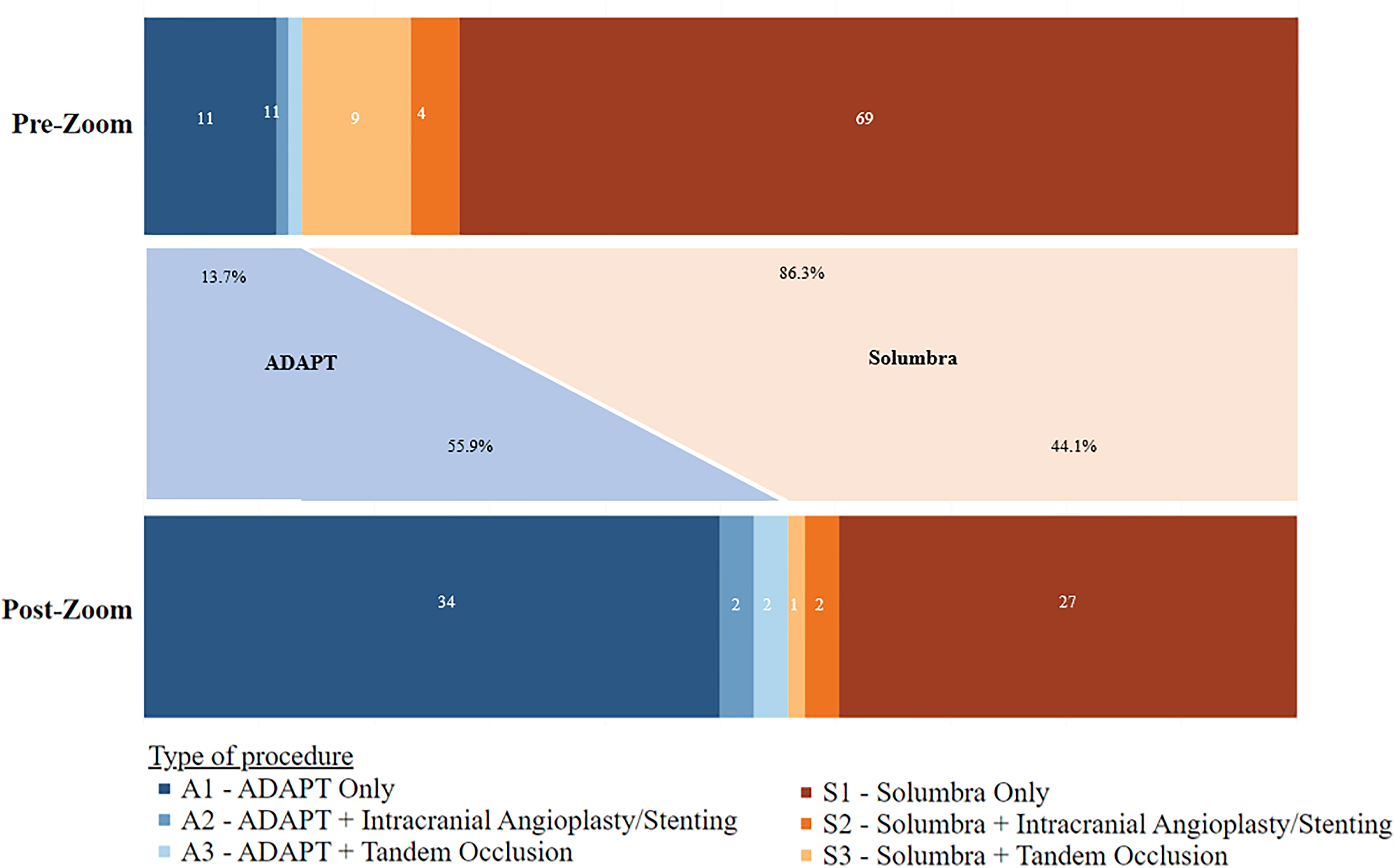
Shift in the utilization of the ADAPT before and after introducing Zoom™ catheters at our institution.
Baseline characteristics of study patients.
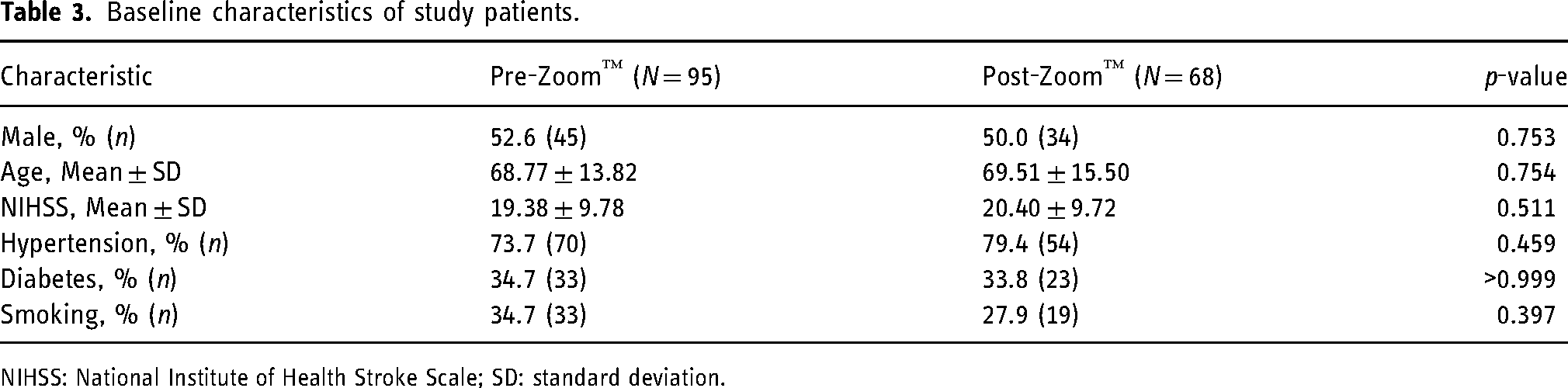
NIHSS: National Institute of Health Stroke Scale; SD: standard deviation.
Procedure characteristics in both treatment groups.
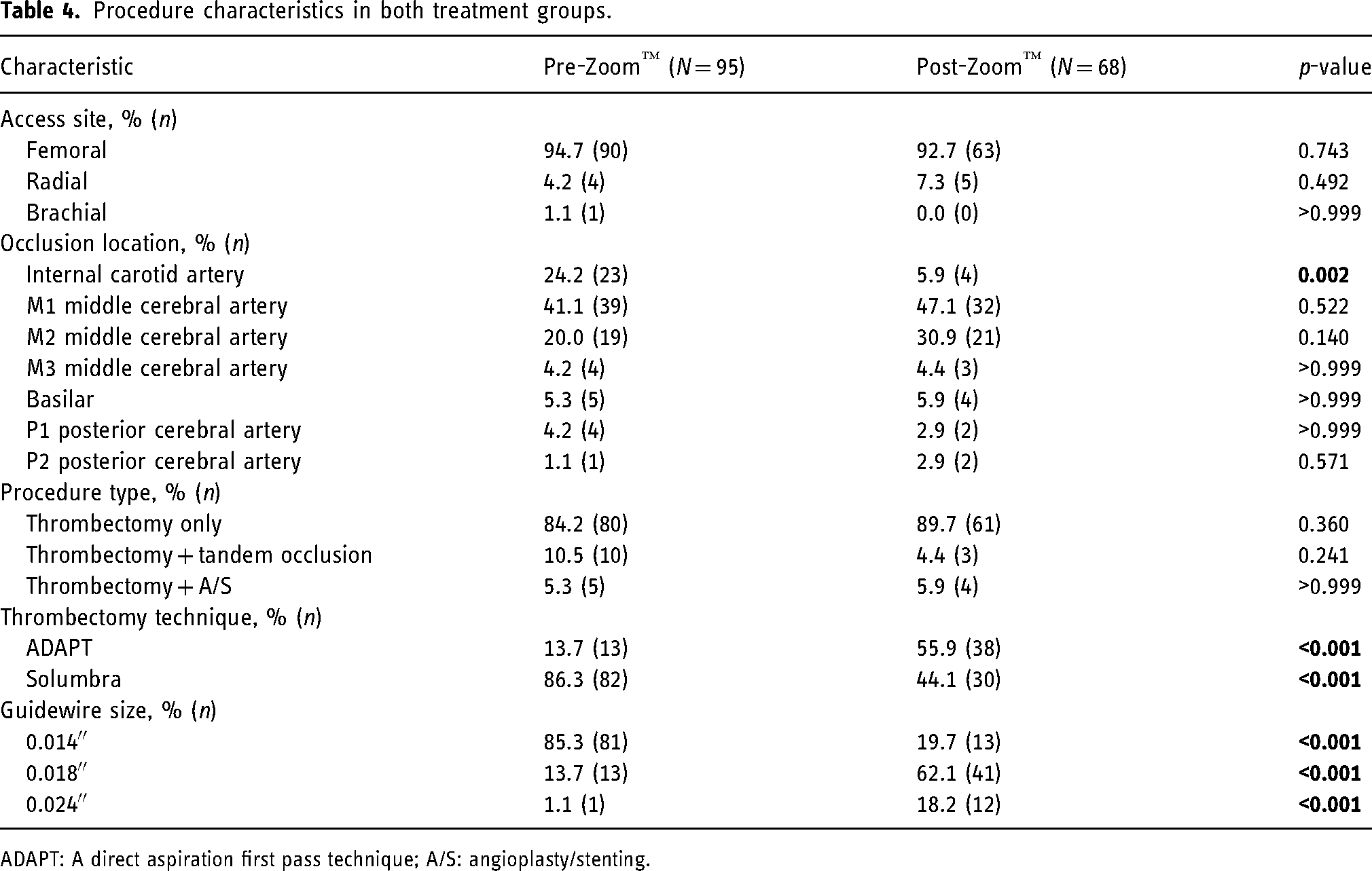
ADAPT: A direct aspiration first pass technique; A/S: angioplasty/stenting.
Safety and effectiveness outcomes
There were no significant differences in the overall rate of hemorrhage between the pre-Zoom group (17.9%, 17/95) and the post-Zoom group (20.6%, 14/68), p = 0.690. The sub-group analyses for the hemorrhagic infarction (HI)1, HI2, parenchymatous hematoma (PH)1, and PH2 hemorrhage rates (Table 5) also did not show any significant differences between the two groups. Similarly, there were no significant differences in the achievement of complete reperfusion (mTICI 3) between the pre-Zoom group (61.1%, 58/95) and the post-Zoom group (60.3%, 41/68), p > 0.999.
Safety and effectiveness outcomes.
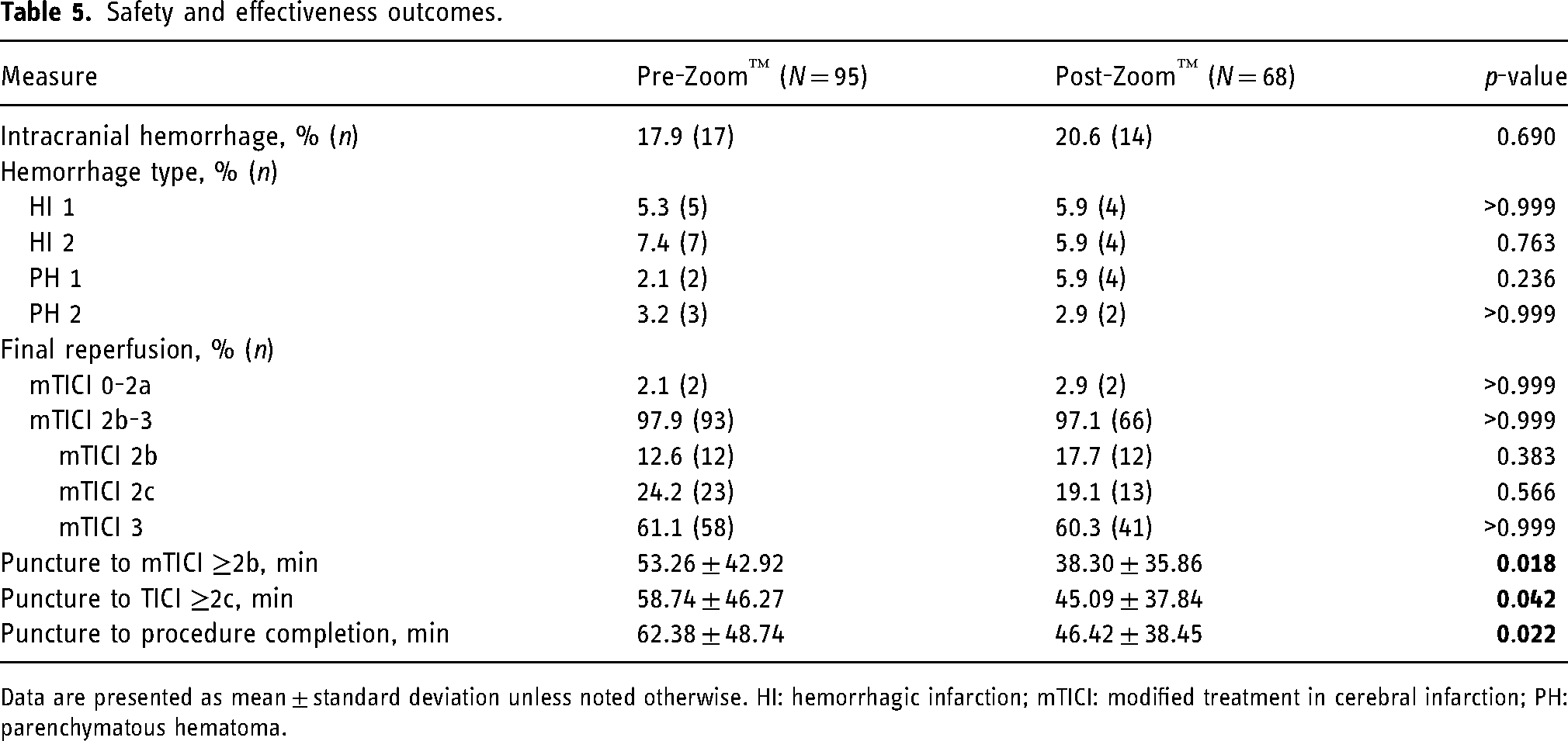
Data are presented as mean ± standard deviation unless noted otherwise. HI: hemorrhagic infarction; mTICI: modified treatment in cerebral infarction; PH: parenchymatous hematoma.
However, the introduction of Zoom catheters resulted in a significantly faster time from puncture to reperfusion compared to the use of straight-tip catheters. The post-Zoom group achieved mTICI ≥ 2b reperfusion in 38.30 ± 35.86 min, whereas the pre-Zoom group took 53.26 ± 42.92 min, p = 0.018. Significantly shorter times from puncture to excellent reperfusion (mTICI 2c) and procedure completion were also observed in the post-Zoom group (Table 5). In patients with ICA occlusions, which are often associated with more complex procedures, average time from puncture to mTICI ≥2c reperfusion was also significantly shorter in the post-Zoom group compared to pre-Zoom group (45.33 ± 10.79 vs. 106.90 ± 52.22, p = 0.006, respectively). Furthermore, time from puncture to mTICI ≥2b and time from puncture to procedure completion were also significantly shorter in the post-Zoom group (45.33 ± 10.79 vs. 91.90 ± 43.65, p = 0.012 and 45.33 ± 10.79 vs. 120.80 ± 47.15, p = 0.001, respectively).
Cost analysis
When comparing the pre-Zoom and post-Zoom procedure costs, a significant decrease in cost was observed with the mean cost decreasing from $12,127 ± $3896 to $9728 ± $5428 (p = 0.002; Table 6). Sub-group analyses were completed based on the type of procedure being performed with the thrombectomy only procedures also having a statistically significant decrease in mean cost moving from $11,426 ± $3704 to $9505 ± $5430 (p = 0.02) post-Zoom. The procedure techniques that included additional treatment for tandem occlusions and intracranial angioplasty/stenting also showed a numeric decrease in cost post-Zoom; however, due to the low sample size in these sub-groups statistical significance was not achieved.
Procedure cost of patients treated in our study population.
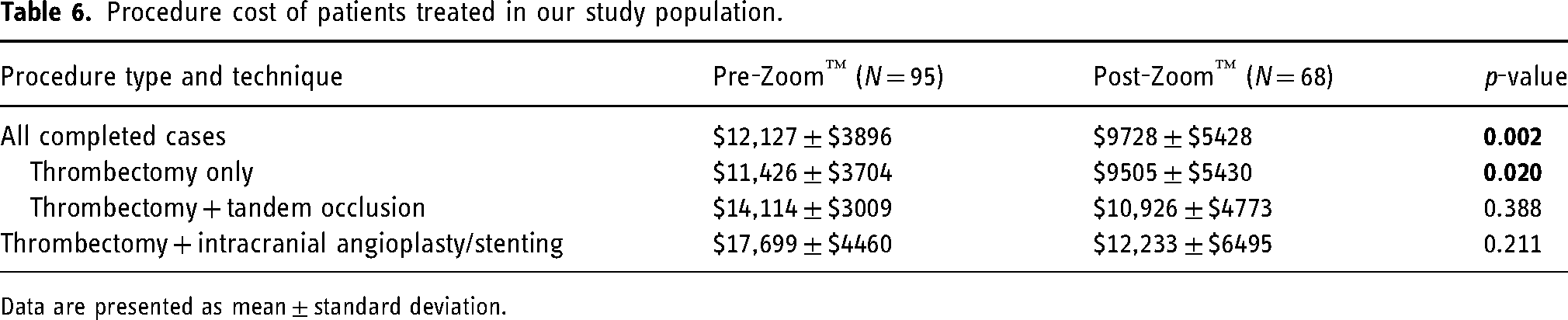
Data are presented as mean ± standard deviation.
Comparison of ADAPT and Solumbra techniques
In our patient population, there were no significant differences in the rates of intracranial hemorrhage between the Solumbra technique and the ADAPT technique (19.6%, 22/112 for Solumbra technique vs. 17.6%, 9/51 for ADAPT; p = 0.832). Both groups also achieved similar rates of final reperfusion (Table 7). The time from puncture to achieving mTICI ≥ 2b reperfusion was 54.65 ± 43.93 min for the Solumbra technique, compared to 29.44 ± 24.43 min for the ADAPT technique (p < 0.001). Furthermore, the procedure costs decreased significantly from a mean of $13,498 ± $3244 for the Solumbra technique to a mean of $5754 ± $2806 for the ADAPT technique.
Comparison of ADAPT and Solumbra safety, effectiveness and cost associated with the thrombectomy procedures.
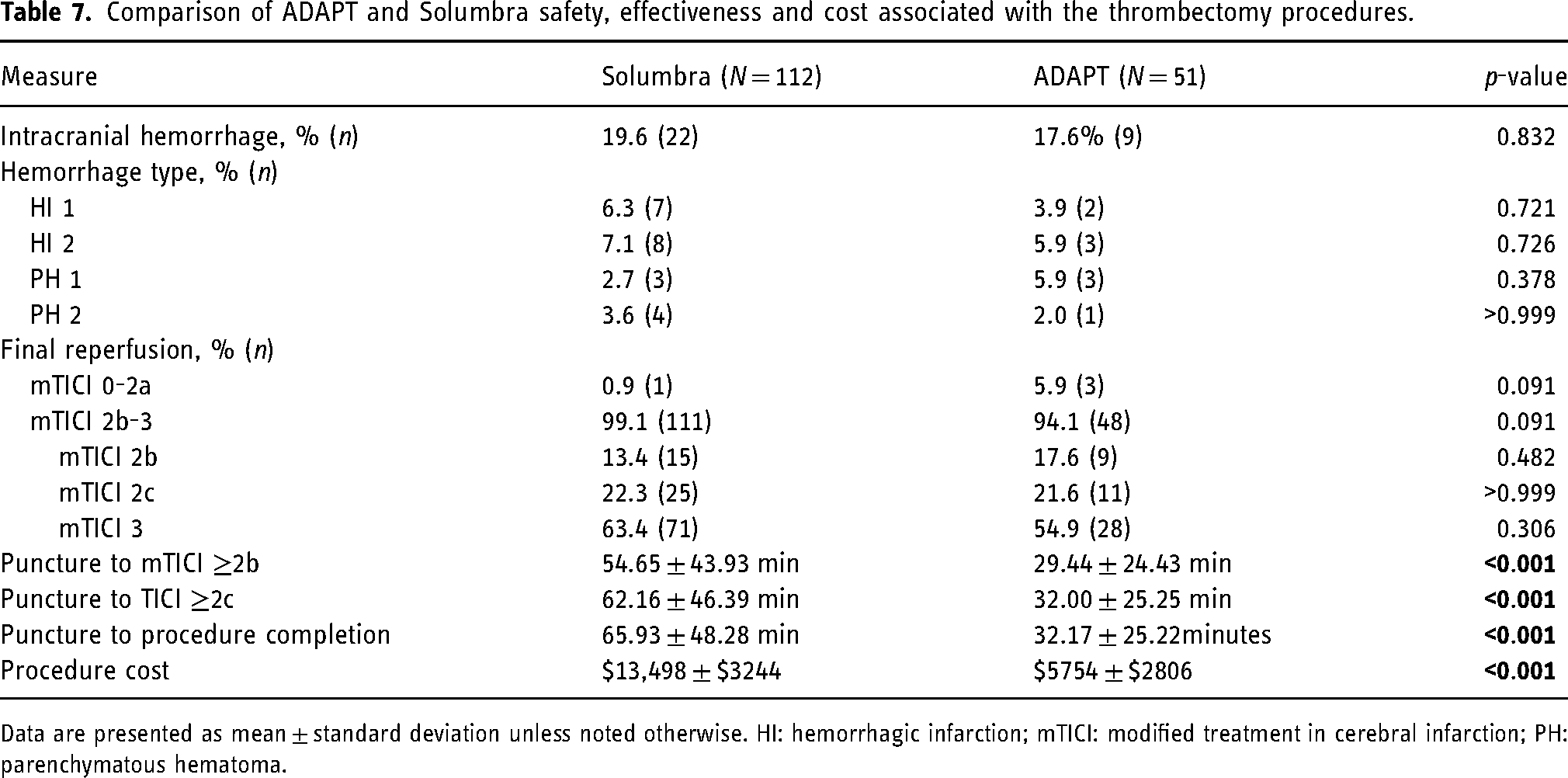
Data are presented as mean ± standard deviation unless noted otherwise. HI: hemorrhagic infarction; mTICI: modified treatment in cerebral infarction; PH: parenchymatous hematoma.
Discussion
The principal finding of this study is that the use of Zoom catheters was associated with a significant decrease in the average procedural cost compared to the cost of performing thrombectomy procedures in the 18-month period prior to the introduction of Zoom catheters. Significant reductions in procedural costs were observed when using the Zoom catheters in all compared cases and in thrombectomy cases without any adjunctive procedures. Similarly, a notable numerical cost reduction was observed in patients with tandem occlusions, intracranial angioplasty, or intracranial stenting when using the Zoom catheters. Due to the low sample size in these sub-groups where adjunctive therapy was needed, statistical significance was not achieved.
Several studies have consistently shown that ADAPT technique is the most cost-effective technique to perform thrombectomy.7,11 In a study conducted by Turk and colleagues, it was concluded that the ADAPT technique not only achieved technical success but also proved to be cost-effective for revascularization of large vessel intracranial occlusions. 7 The findings of the COMPASS trial further supported this notion by demonstrating that the ADAPT technique resulted in a mean cost reduction of $4541 compared to the stent retriever first-line group. 11 Moreover, the ADAPT technique achieved non-inferior functional outcomes at 90 days when compared to stent retriever first-line thrombectomy. Based on these results, the authors recommended direct aspiration as a viable alternative to stent retriever as a first-line therapy for stroke thrombectomy. In our own study, we observed an even greater reduction in mean cost when comparing the ADAPT and Solumbra technique sub-groups. The mean reduction amounted to $7744, with $13,498 for Solumbra and $5754 for ADAPT. This substantially larger cost reduction in our study can be partially attributed to the inclusion of adjunctive therapies within our cohort and a higher number of tandem occlusions treated with the Solumbra technique. Tandem occlusions necessitate additional devices such as angioplasty balloons and implantable stents, thereby driving up the overall procedure cost.
Despite our limited exposure to cases of ICA occlusions and a small number of patients with ICA occlusions in our cohort, it is noteworthy that the shift toward more frequent use of the ADAPT technique appeared to remain unaffected by anatomical considerations. Specifically, the use of the Solumbra technique for ICA occlusions was prominent in the pre-Zoom group, accounting for 95% of cases, while this percentage decreased to 33% in the post-Zoom group. Notably, all ADAPT cases within the post-Zoom cohort were completed without the need for stent retriever rescue therapy. Nevertheless, further clinical investigations into devices specifically designed to address the complexities of ICA and tandem occlusions are warranted.
The preferred method of thrombectomy is the one that achieves the fastest recanalization times with lowest complication rates and costs. Recent study showed that longer thrombectomy procedure times for acute ischemic stroke are associated with poor clinical outcome, increased intracerebral hemorrhage rate, and increased complication rates. 17 The proposed underlying mechanism suggests that prolonged procedures lead to greater ischemic damage to the brain. In our cohort, we successfully achieved significantly shorter procedural times by employing Zoom catheters in all three investigated domains. The utilization of Zoom reperfusion catheters resulted in an average time reduction from puncture to achieving mTICI ≥2b and mTICI ≥2c reperfusion of approximately 15 and 14 min, respectively. Additionally, the time from puncture to procedure completion was shortened by approximately 16. Our findings contribute to a growing body of published literature that demonstrates faster puncture to reperfusion time when utilizing the Zoom catheters.18,19
We recognize that time to mTICI reperfusions in our study is numerically slower than previous reports assessing the performance of Zoom catheters.18,19 We attribute this to inclusion of patients in need of adjunctive therapies in our cohort (i.e., tandem occlusions, stenting). However, we recognize the complexity of including patients with tandem occlusion and adjunctive therapies in our cohort. Interestingly, a subgroup analysis of these patients demonstrated a significantly shorter average total procedure time (75 min shorter) as well as shorter time from puncture to mTICI ≥2b (47 min shorter) and mTICI ≥2c (61 min shorted) reperfusion in the post-Zoom group. We recognize that our analysis in this subgroup is limited by the small sample size in both groups and warrants a more in-depth analysis of factors affecting time-related outcomes in this subgroup of patients. Additionally, we included patients with posterior circulation occlusions as well as more distal occlusions (distal of M1 segment of MCA) compared to the recent multi-center report that included only patients with M1 occlusion. 18 Interestingly, focusing only on patients without need for adjunctive treatment, the average time to mTICI ≥ 2b reperfusion in the Solumbra group decreased from 57.7 to 51.6 min; in the ADAPT group the same time decreased from 29.5 to 23.1 min. The faster time to reperfusion, coupled together with the significant cost reduction and similar safety outcomes justified our preference to continue using the Zoom Catheter over traditional straight-tip catheters in performing thrombectomy procedures at our comprehensive stroke center.
After the initial evaluation and introduction of Zoom catheters at our institution, the utilization of the ADAPT technique has significantly increased from 13.5% to its current rate of 55.9% (Figure 2). We compared the safety and angiographic reperfusion outcomes between the pre-Zoom and post-Zoom groups, as well as between the Solumbra and ADAPT groups, but found no statistically significant differences. Specifically, the intracerebral hemorrhage rate in this study did not show a significant difference. However, we did observe a numerical decrease in the occurrence of larger hemorrhages (HI2 and PH2) in the post-Zoom and ADAPT groups, which are more likely to exhibit symptoms. Vargas et al. compared two aspiration thrombectomy groups: those in whom traditional straight-tip catheter were used, and those in whom Zoom aspiration catheters were used. 12 The authors reported that patients who underwent thrombectomy with the Zoom aspiration catheters had a higher proportion of TICI 2c or better reperfusion, had a significantly lower modified Rankin Score (mRS) on discharge and at 90 days, and the stent retriever usage was lower. 12 In our cohort, self-adjudicated angiographic mTICI reperfusions were comparable between the pre-Zoom and post-Zoom groups, as well as between the Solumbra and ADAPT groups. We also observed lower usage of stent retrievers after the introduction of Zoom catheters at our center. While we did not assess mRS in our cohort, the findings from Vargas et al. suggest potential improvements in clinical outcomes associated with the use of Zoom aspiration catheters, supporting the need for prospective research in this area as well as the potential impact of the reduced procedure times achieved with the Zoom catheters on the rate of symptomatic intracranial hemorrhages.
Limitations
Although the results from our study support the safety, utility, and reperfusion success of the Zoom catheters, we recognize the limitations inherent in a single-center retrospective study, which could potentially introduce bias. Specifically, the relatively small number of patients, absence of core-lab adjudication, and lack of a 90-day follow-up period, including an assessment of functional outcomes, may affect the reliability, repeatability, and generalizability of our findings. However, we believe our report is valuable because it includes all patients treated with Zoom catheters, including our initial learning curve, by a single operator in a high-volume comprehensive stroke center, without selection bias, which makes technique variability less likely and adds to the strength of the study. We also included unsuccessful thrombectomy attempts with catheters that failed to navigate to the clot. Furthermore, data on the type of arch were not routinely collected and were not available for analysis. However, our primary aim was to examine the angiographic efficacy and cost-effectiveness of the Zoom aspiration system. To address some limitations of our report, including determining factors associated with clinical benefits of Zoom catheters across various patient populations and procedural scenarios, the data obtained from an ongoing prospective multi-center clinical investigation of the Zoom Reperfusion System (NCT04129125) could provide valuable additional insights into safety outcomes, core-lab adjudicated angiographic reperfusion outcomes, and functional independence for patients treated for acute ischemic stroke within an 8-h timeframe from the onset of symptoms.
Conclusion
In our study, the use of Zoom catheters led to a significant reduction in procedure costs, while also demonstrating a notable improvement in the time it took to achieve reperfusion. The Zoom catheters were found to be both safe and effective in achieving reperfusion in our group of patients. These findings emphasize the potential of Zoom technology as a valuable tool in treating ischemic stroke, providing economic advantages and positive treatment outcomes for patients.
Footnotes
Authorship contributions
Study concept and design, acquisition of data, and analysis and interpretation of data were done by Mohamad Ezzeldin. Initial draft of the manuscript was done by Riichi Ota and Saif Bushnaq. Review and critical edits of the manuscript were done by Mohamad Ezzeldin, Riichi Ota, Eric Riha, Adam Delora, Bader Alenzi, Victoria Gordon, Himanshu Gupta, Rime Ezzeldin, and Saif Bushnaq.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics/IRB approval
This study received approval from the Institutional Review Board of the Health Corporation of America (HCA) Healthcare Houston Kingwood Hospital. This research was supported (in whole or in part) by HCA Healthcare and/or an HCA Healthcare affiliated entity. The views expressed in this publication represent those of the author(s) and do not necessarily represent the official views of HCA Healthcare or any of its affiliated entities.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.