
Abstract
Objective
There are few studies on flow diverters with diameters >5 mm. We present our preliminary experience with the 5.5–8 mm Derivo Embolization Device (DED) implants for the treatment of cerebral aneurysms.
Methods
A consecutive series of 26 patients (median age: 60 years) treated for 32 aneurysms in 26 procedures was retrospectively analyzed for procedural characteristics, complications, and mid-term angiographic results.
Results
The median aneurysm size was 10.5 mm, 2 of 30 (6%) aneurysms were ruptured and 9 (28%) had a fusiform or dissecting morphology. DED implantation was performed in the internal carotid artery in 18 of 26 (69%) procedures and in the vertebrobasilar artery in 8 (31%). Device deployment failed in 1 (4%) procedure. The 7 and 8 mm implants were successfully deployed in 5 cases. Additional balloon angioplasty or stent implantation was performed in 3 (12%) cases to improve wall apposition. Complications included 1 (4%) major stroke and 2 (8%) minor strokes. Angiographic follow up at a mean of 6 months showed complete occlusion in 8 of30 (27%) aneurysms and favorable occlusion in 14 (47%).
Conclusions
The use of large diameter DEDs was safe and feasible. The mid-term occlusion rates are acceptable considering the complex subset of aneurysms studied. Further studies are warranted to define the indications for large-diameter DEDs and to evaluate their long-term efficacy.
Introduction
Flow diverters (FDs) have emerged as a well-established endovascular treatment option for intracranial aneurysms, particularly in complex cases such as wide-necked, large, fusiform, and dissecting aneurysms that pose challenges to traditional endovascular treatments.1–4 The basic mechanism involves exclusion of the aneurysm from the circulation by obstructing blood flow at the vessel wall defect, resulting in subsequent hemodynamic decoupling between the normal vessel and the aneurysm lumen. A good wall apposition of the FD in the parent artery is essential to promote endothelialization, prevent endoleaks, and facilitate aneurysm obliteration. 5
While the variety of FDs available has increased, there are still few implants larger than 5 mm in diameter. This limits the use of FDs in anatomies where the maximum unrestricted diameter of the stent is less than that of the parent artery, such as certain internal carotid or vertebrobasilar arteries, or in dysplastic and enlarged parent arteries.
The Derivo Embolization Device (DED; Acandis, Pforzheim, Germany) has been available in 5.5 and 6 mm implant diameters. Recently, 7 and 8 mm diameter implants have been introduced, but clinical data on these diameter implants have not been published. This study reports our preliminary experience with large diameter DEDs (≥5.5 mm), with a particular focus on the 7 and 8 mm implants.
Methods
This is a retrospective, observational, single-arm study of consecutive patients who received DED treatment with implant diameters of 5.5, 6, 7, or 8 mm for intracranial and cervical aneurysms between October 2017 and September 2023. There were no exclusion criteria. The local ethics committee approved the anonymous collection of patient data. Informed consent was waived for this retrospective observational study.
Procedure
The DED is an advanced flow diverter with diameters ranging from 2.5 to 8 mm, allowing treatment of vessels from 1.5 to 8 mm in diameter. The delivery system allows for subtotal resheathing and repositioning, even in the larger diameters.
The conventional 5.5 to 8 mm DEDs have an electropolished surface with oxide and oxynitride surface modifications to reduce device friction. They are also available with an additional nano-coating (“heal®”-coating, DED 2heal), that mimics the final step of the coagulation cascade, the conversion of fibrinogen to fibrin. 6 This results in a thin and fully polymerized network of fibrin with additional covalently bound heparin molecules on the device surface, potentially rendering the device inert to platelet adhesion and potentially promoting endothelial cell adhesion, as suggested by in vitro studies. 7
All patients were treated under general anesthesia using the transfemoral approach. After an initial intravenous heparin bolus (5000 IU), additional aliquots of 1000 IU/h were administered as needed until completion of the procedure. A triaxial system was used to insert either an 8F (Vista Brite Tip; Cordis, Santa Clara, CA, USA) or 7F (Envoy; Cerenovus, Irvine, CA, USA) guide catheter into the internal carotid artery or a 6F guide catheter (Envoy) into the vertebral artery. The 5.5–6 mm diameter devices were delivered via a 0.027” microcatheter (Headway 27; Microvention, Aliso Viejo, CA, USA, and Neuroslider 27, Acandis) while the 7–8 mm diameter devices require a 0.039” microcatheter (Neuroslider 39, Acandis). Distal access catheters were used for all used device sizes (Navien 058 Intracranial Support Catheter; Medtronic, Dublin Ireland, or Sofia Intermediate Catheter; Microvention). The Proximal Landing Zone (PLZ) and the Distal Landing Zone (DLZ) were measured on 3D volume-rendered images obtained during the procedure. In general, the selected FD diameter was aimed to exceed the largest diameter of the PLZ or DLZ by a few tens of millimeters. If the target vessel was dysplastic and had a diameter larger than the PLZ or DLZ, this diameter was also considered for device selection. Selective balloon angioplasty was used to improve wall apposition when deemed necessary. The neurointerventionalist used adjunctive coils and stents at his or her discretion. Successful device deployment was defined as complete coverage of the aneurysm neck with the DED and complete final wall apposition.
Antiplatelet regimen
For planned procedures, patients were prescribed 100 mg acetylsalicylic acid (ASA) and 75 mg clopidogrel for 5–7 days prior to the procedure. Platelet inhibition was assessed using ASA and P2Y12 assays (Verify Now, Accumetrics, San Diego, CA, USA), with adequate inhibition defined as 350–550 ARU for ASA and 30–60% for clopidogrel. In cases of inadequate response, adjustments included dose escalation (e.g. clopidogrel 150 mg/d) or prasugrel substitution (60 mg bolus, 10 mg/d). In emergencies, tirofiban (Aggrastat, Merck, West Point, PY, USA) was administered prior to DED placement and continued for 16–24 h after the procedure, followed by clopidogrel (300 mg) and ASA (250 mg) loading. Postinterventional antiplatelet therapy consisted of continuous ASA (100 mg/d) and either clopidogrel (75 mg/d) or prasugrel (10 mg/d) for 4 months.
Data collection
Patient demographics and procedural details were obtained by chart review, including details of previous aneurysm interventions, rupture status, number of DEDs used, use of adjunctive devices, complications, and functional outcomes. Both clinically symptomatic complications (e.g. stroke, hemorrhage, inguinal hematoma) and technical, asymptomatic events (e.g. thromboembolism, perforation, dissection, incomplete wall apposition) were documented. Major complications were defined as neurological symptoms persisting for at least 7 days, while minor complications were defined as complete resolution within 7 days. 8 Functional outcome was measured by modified Rankin scale (mRS), and morbidity was defined as an increase in mRS at discharge compared to baseline.
Digital subtraction angiography (DSA) was used to determine aneurysm location, size, neck width, dome-to-neck (D/N) ratio, and parent vessel diameter at the PLZ and DLZ.
This study reports angiographic results within a 1–12 month follow-up (FU) period, grading aneurysm occlusion according to the O'Kelly–Marotta (OKM) grading scale: A = total filling (>95%), B = subtotal filling (5–95%), C = entry remnant (<5%), and D = complete occlusion. OKM C and D were combined as favorable occlusion. Immediate contrast retention after FD implantation was graded as 1 = no stasis, 2 = moderate stasis, and 3 = severe stasis. Moreover, the occurrence of fish mouthing, device braid narrowing or collapsing, and intimal hyperplasia (mild: < 25% of FD inner diameter, moderate: 25–50%, severe: > 50%) were recorded.
The primary endpoints were the rate of major in-hospital complications as a safety endpoint and the rate of mid-term favorable aneurysm occlusion as an efficacy endpoint.
Statistical analysis
Descriptive statistics were used to report categorical data as numbers with percentages and continuous data as medians with interquartile range (IQR). Categorical variables were compared using the Fisher exact test with SPSS software (IBM SPSS Statistics for Windows, version 25.0, Armonk, NY, USA), with p < 0.05 considered statistically significant.
Results
Patient and aneurysm characteristics
Twenty-six patients who underwent 26 procedures for the treatment of 32 aneurysms were included. The median age of the patients was 60 years (IQR: 51–69 years) and 16 (61.5%) were female.
The most common aneurysm locations were the paraophthalmic internal carotid artery (ICA) in 17 of 32 (53.1%) cases, the basilar artery (BA) in 7 (21.9%), and the cavernosal ICA in 4 (12.5%). Two (6.3%) aneurysms were extradural in the cervical ICA. In both cases, FD treatment was performed because the cervical aneurysms were a source of thromboembolism.
Two (6.3%) aneurysms were ruptured and the patients had a World Federation of Neurosurgical Societies score of 4 and 5, respectively. One (3.1%) posterior inferior cerebellar artery aneurysm was recanalized after previous treatment with a Woven Endobridge (WEB; Microvention, Aliso Viejo, CA, USA) device. Morphology was saccular in 23 of 32 (71.2%) aneurysms, fusiform in 8 (25.0%), and dissecting in 1 (3.1%). The median aneurysm size was 10.5 mm (IQR: 6.3–19.3 mm), ranging from 2.0 to 31.0 mm, with 17 (53.1%) aneurysms larger than 10 mm. Baseline aneurysm characteristics are summarized in Table 1.
Baseline aneurysm characteristics.
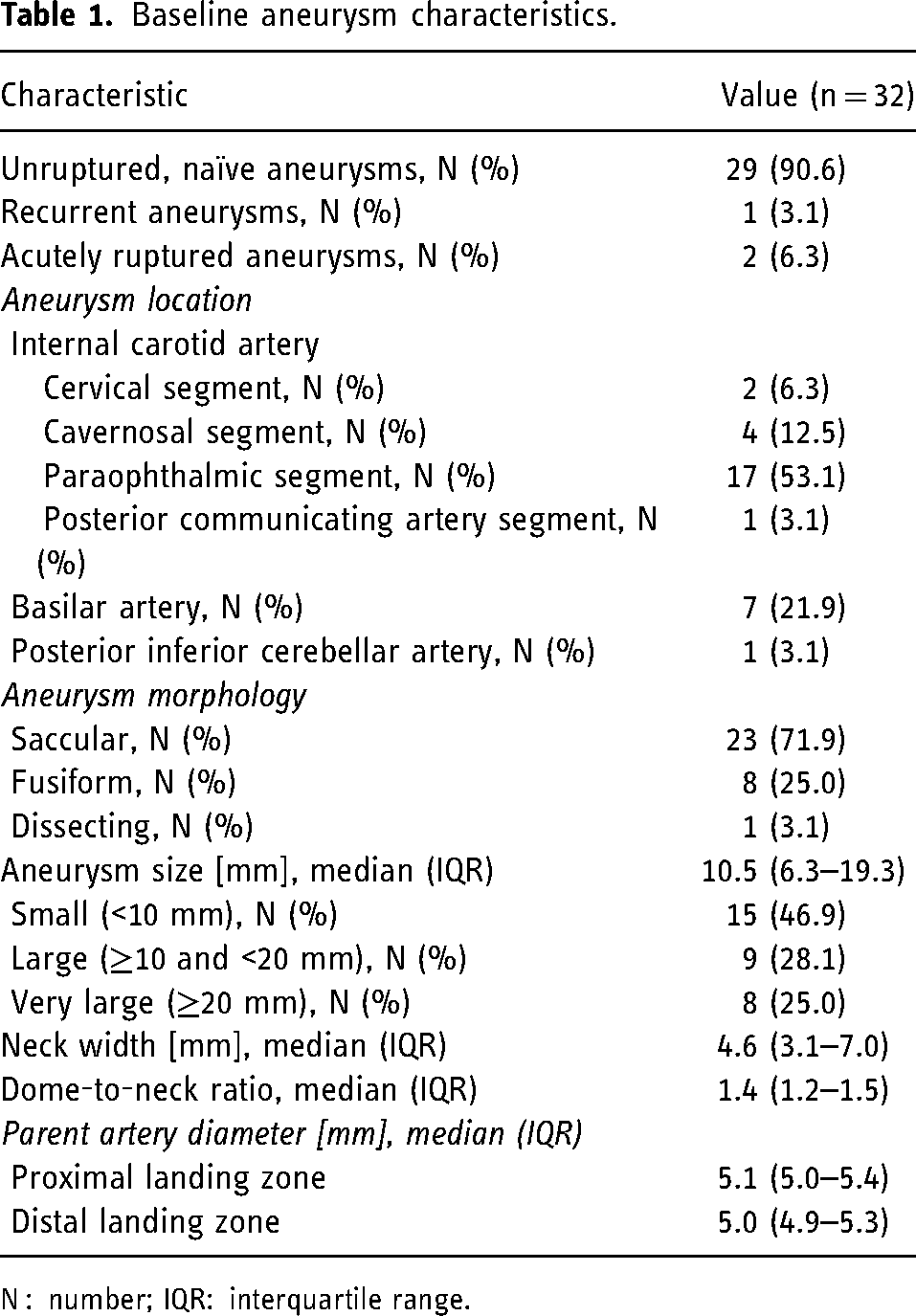
N : number; IQR: interquartile range.
Treatment
Procedure characteristics are shown in Table 2. DED implantation was technically successful in 25 of 26 (96.2%) cases, using the conventional DED in 21 (80.8%) cases and the DED 2heal in 5 (19.2%) cases. In the failed case of a posterior communicating artery (Pcom) aneurysm, both the DED 2heal 6 × 40 mm and a conventional DED 6 × 40 mm could not be pushed through the microcatheter due to high friction caused by the vessel tortuosity. The aneurysm was then successfully treated with a Flow-Redirection Endoluminal Device 5.5 × 32 mm (FRED; Microvention). In a second case, a DED 2heal 6 × 40 mm could also not be delivered, probably due to a technical defect, but the delivery of another DED 2heal of the same size was successful. Of the technically successful cases, 3 of 25 (12.0%) were treated with 2 DEDs. In 2 cases with large paraophthalmic ICA aneurysms ≥10 mm, a second DED was implanted due to insufficient contrast retention after implantation of the first device (OKM A1). The second DED induced contrast retention in the first case (OKM A2) and failed in the second case. In the third case, a second DED was implanted using the telescoping technique because the proximal end ended in a curve of the cavernous ICA with an indicated kinking of the artery. On average, 1.1 DEDs were implanted per aneurysm. The 5.5 mm diameter DED was used in 18 (69.2%) cases with PLZ and DLZ of 4.0–5.5 and 4.0–5.3 mm, respectively. The 6 mm diameter DED was used in 5 of 26 (19.2%) cases with PLZ and DLZ of 5.1–5.5 and 4.9–5.7 mm, respectively. The 7 mm diameter DED was used in 3 of 26 (11.5%) cases with PLZ and DLZ of 5.0–6.3 and 5.1–6.5 mm, respectively. The 8 mm diameter DED was used in 2 of 26 (7.7%) cases with PLZ and DLZ of 5.6–6.8 and 5.9–7.0 mm, respectively. The 5 cases in which 7 and 8 mm diameter DEDs were used (including one DED 2heal case) are presented in detail:
A complex saccular paraopthalmic ICA aneurysm (22 mm; PLZ: 6.3 mm, DLZ: 5.1 mm) was treated with a DED 7 × 50 mm with good wall apposition and immediate contrast retention (OKM A3). After the procedure, the patient presented with motor aphasia (mRS 1) and magnetic resonance imaging (MRI) showed a thromboembolic infarct (mRS 1). At 1-month follow up, magnetic resonance angiography (MRA) showed favorable occlusion (OKM C) and motor aphasia was completely resolved. This case is shown in Figure 1. A patient with a dysplastic intradural ICA has a small paraophthalmic artery aneurysm (3 mm) and a large lobulated Pcom aneurysm (11 mm, PLZ: 5.9, DLZ: 5.7). A 7 × 40 mm DED was implanted from the distal ICA to the petrous ICA. Angiographic control showed good wall apposition and immediate contrast retention (OKM A2). There were no complications. DSA after 7 months showed progressive occlusion of the Pcom aneurysm (OKM B3) and subtotal occlusion of the paraophthalmic aneurysm (OKM C3). This case is presented in Figure 2. A patient with subarachnoid hemorrhage (SAH) had a dysplastic basilar artery with 2 fusiform basilar trunk aneurysms (14 and 22 mm). A DED 2heal 7 × 40 mm was implanted extending from the basilar tip to the left V4. The coated version of this implant size was implanted as the treatment was performed in the acute setting of SAH and the patient did not receive antiplatelet loading before treatment. The procedure was performed under tirofiban administration followed by ASA and clopidogrel loading. The DED showed good wall apposition, but a narrowing in the basilar artery segment between the two aneurysms due to a pre-existing stenosis. Balloon angioplasty was performed to relieve the stenosis. There were no complications. Immediate contrast stasis was observed (OKM A2), which was considered sufficient to prevent early aneurysm rupture. Two-month follow up with computed tomography angiography (CTA) showed partial aneurysm occlusion (OKM B). A fusiform aneurysm (19 mm) at the proximal basilar trunk and dysplastic enlargement of the left V4 was treated with an 8 × 40 mm DED extending from the distal BA to the left V4. The PLZ was 6.0 mm and the DLZ was 5.1 mm, but the parent vessel diameters adjacent to the aneurysm were 7.6 mm proximally and 7.8 mm distally. Good wall apposition and contrast retention (OKM A2) were achieved and there were no complications. Six-month DSA showed complete aneurysm occlusion (OKM D) and mild in-stent stenosis caused by neointimal hyperplasia. This case is shown in Figure 3. A fusiform cervical ICA aneurysm (20 mm, PLZ: 6.6 mm, DLZ: 6.9 mm) was the source of a thromboembolic infarction. A DED 8 × 40 mm was implanted with adequate neck coverage, but there was insufficient wall apposition in the middle part and fish mouthing at the proximal end. Balloon angioplasty was performed to improve wall apposition in the mid-portion. Additional balloon angioplasty of the proximal fish mouthing did not improve wall apposition, so an additional Acclino Flex Plus stent 5.5 × 25 mm (Acandis, Pforzheim, Germany) was implanted in a telescoping technique with a good angiographic result (OKM A3). There were no clinical complications. CTA after 1 month showed partial aneurysm thrombosis (OKM C).
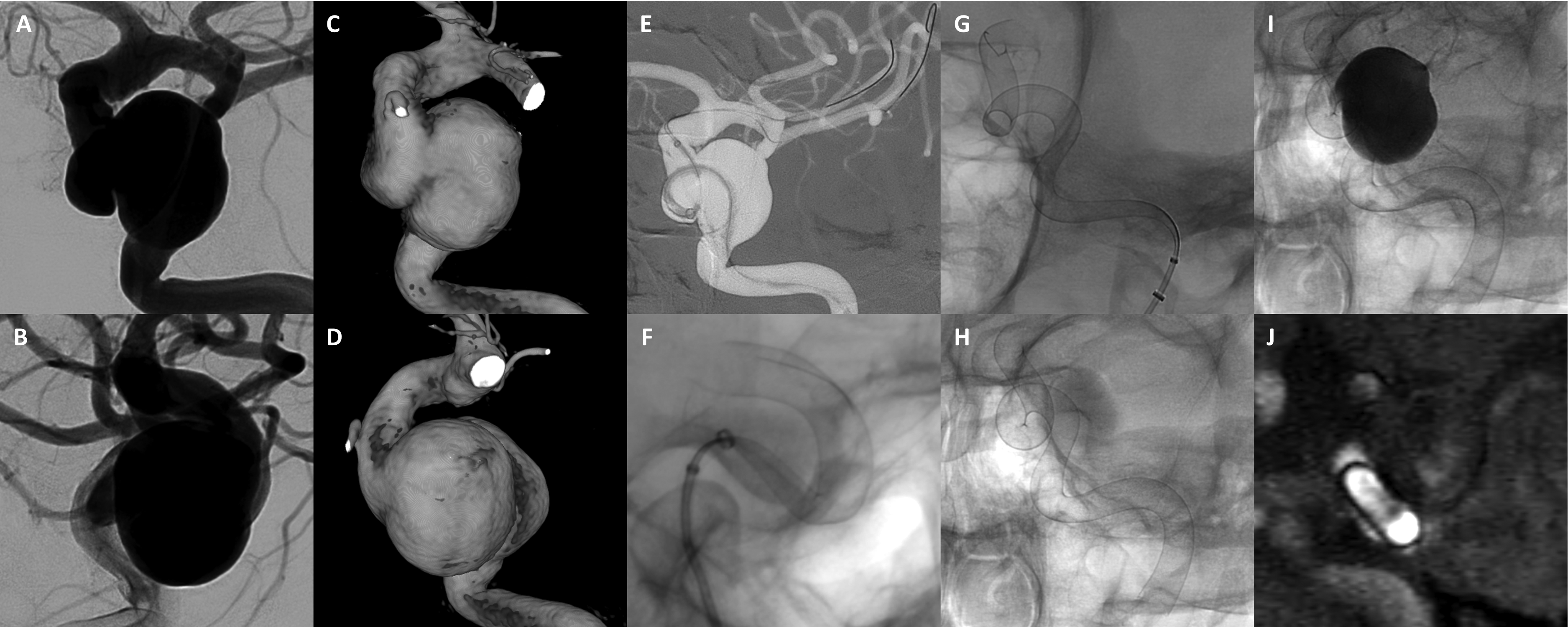
Digital subtraction angiography (A + B) and 3D reconstructions from rotational angiography (C + D) show a very large and very broad-based saccular paraopthalmic ICA aneurysm in anteroposterior (A + C) and lateral (B + D) projections. The aneurysm size was 22 mm with a proximal landing zone of 6.3 mm and a distal landing zone of 5.1 mm. Probing of the distal ICA was complicated by tortuous vessel anatomy (including tortuous cervical ICA, not shown). Finally, placement of the microcatheter in the distal ICA (Neuroslider 39) was achieved using two microwires (dual wire technique, E). Advancing the 7 × 50 mm DED was unproblematic and the DED was deployed in a stepwise fashion (F–H), achieving good wall apposition even through the numerous curves. Control angiography showed immediate contrast retention (I, OKM A3). One-month magnetic resonance angiography showed subtotal thrombosis of the aneurysm sac (J, OKM C). Notably, DED allows assessment of luminal patency due to low susceptibility artifacts. DED: Derivo Embolization Device; ICA: internal carotid artery; OKM: O'Kelly–Marotta.
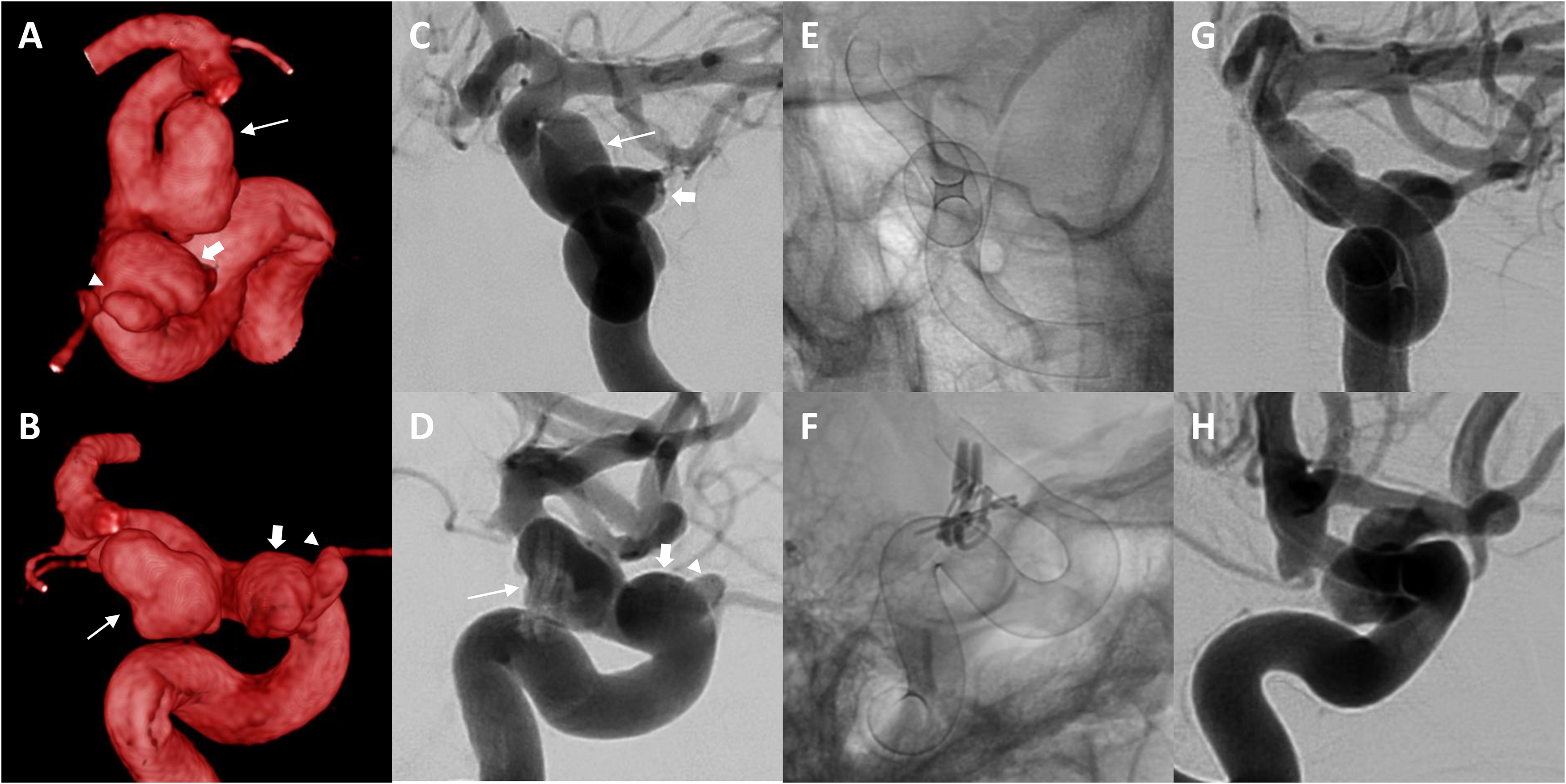
Three-dimensional reconstructions from rotational angiography (A + B) and DSA (C + D) show a large aneurysm at the posterior communicating segment of the left ICA (11 mm, arrow) and a dysplastic, fusiformly enlarged paraophthalmic segment (block arrow) with a small aneurysm (3 mm, arrowhead). The proximal landing zone was 5.9 mm and the distal landing zone was 5.7 mm, but the dysplastic segment measured 7.5 mm in diameter. A 7 × 40 mm DED was implanted from the distal ICA to the petrous ICA, the unsubtracted images show the full contour of the deployed DED (E + F). Note the overlaying aneurysm clip after clipping a contralateral middle cerebral artery aneurysm in F. DSA at 7 months showed progressive thrombosis within the posterior communicating ICA aneurysm (OKM B3) and subtotal occlusion of the paraophthalmic ICAaneurysm (OKM C3). There was no in-stent stenosis. DED: Derivo Embolization Device; DSA: digital subtraction angiography; ICA: internal carotid artery; OKM: O'Kelly–Marotta.

Digital subtraction angiography in anteroposterior (A) and lateral (B) projections and 3D rotational angiography (C) show a fusiform aneurysm (19 mm) at the proximal basilar trunk and dysplastic enlargement of the left V4 and proximal basilar artery. The proximal and distal landing zones were 6.0 and 5.1 mm, respectively, but the parent vessel diameters adjacent to the aneurysm were 7.6 mm proximally and 7.8 mm distally. After probing the basilar artery with a Neuroslider 39 microcatheter with the tip in the left P1 (D), the aneurysm was treated with an 8 × 40 mm DED extending from the distal BA to the left V4. (E) and (F) Snapshots of the procedure in anteroposterior and lateral projection. At the sharp bend between V4 and BA, the proximal part of the DED did not open well initially, but with partial resheathing and gentle push on the microcatheter/flow diverter system, sufficient deployment with good wall apposition was achieved as shown in (G) + (H). Angiographic control shows a good reconstruction of the dysplastic V4/BA with the DED (G + H, arrows) and immediate contrast retention (OKM A2) was achieved. There were no procedural complications. Six-month DSA shows complete aneurysm occlusion (OKM D) and mild in-stent stenosis caused by neointimal hyperplasia (I, arrowheads). BA: basilar artery; DED: Derivo Embolization Device; DSA: digital subtraction angiography; OKM: O'Kelly–Marotta.
Procedural characteristics.
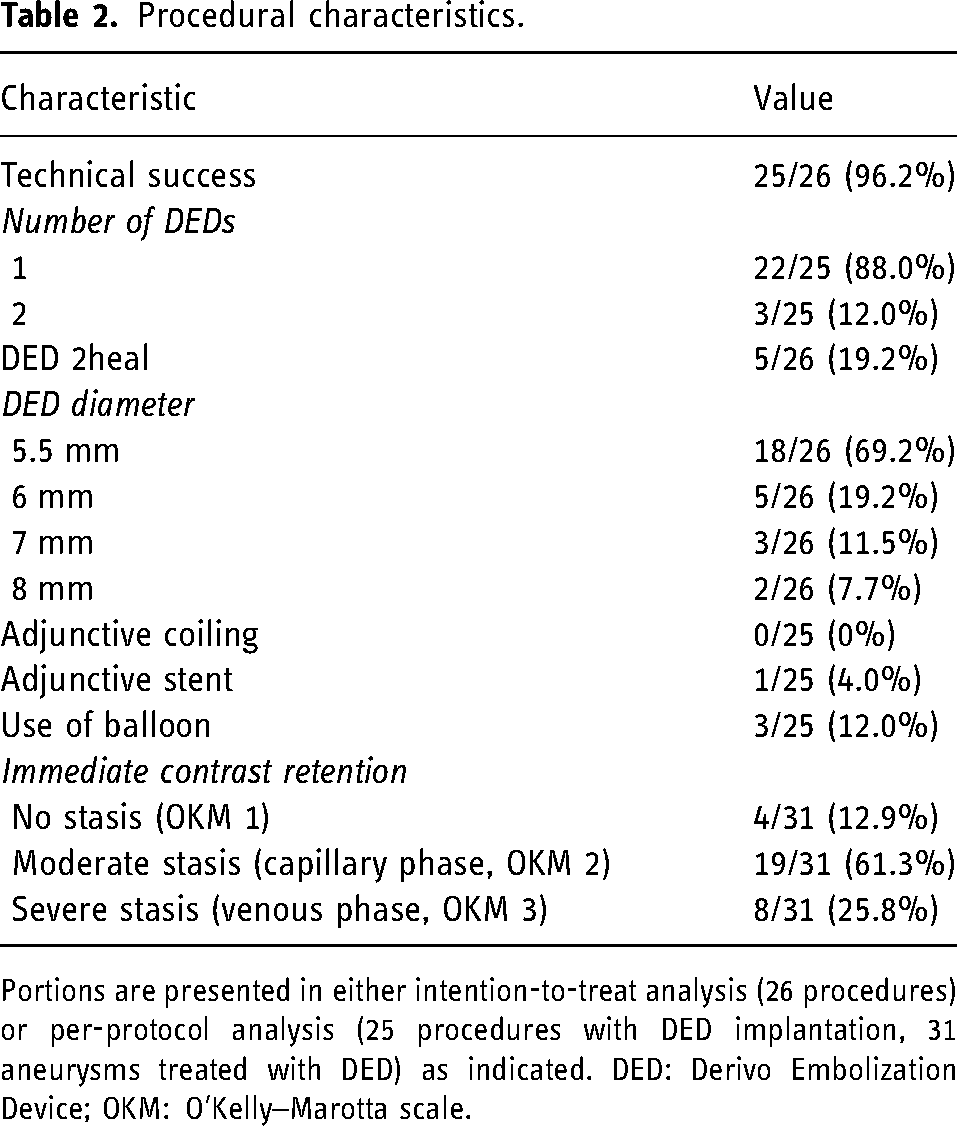
Portions are presented in either intention-to-treat analysis (26 procedures) or per-protocol analysis (25 procedures with DED implantation, 31 aneurysms treated with DED) as indicated. DED: Derivo Embolization Device; OKM: O’Kelly–Marotta scale.
No additional coils were implanted in any case. An additional stent was implanted only in the above case to improve the proximal fish mouthing (4.0%). Balloon angioplasty was performed in 3 of 25 cases (12.0%) to improve wall apposition, 2 of which were 7 and 8 mm devices as described above. Immediate contrast retention was observed in 27 of 31 (87.1%) aneurysms (Table 2).
Complications and clinical outcome
Procedural symptomatic complications occurred in 3 of 26 (11.5%) procedures, all of which were thromboembolic infarctions after treatment of a paraophthalmic ICA aneurysm, respectively. The following uncoated DEDs were used: DED 7 × 50 mm in case 1, DED 6 × 25 mm in case 2, and DED 5.5 × 15 mm in case 3. All three patients had neurological symptoms immediately after the procedure and MRI showed punctate infarcts, but no thromboembolic event was noted during the procedure. At discharge, the patients had mRS scores of 0, 1, and 2, respectively. The complications were classified as major in 1 case (3.8%) and minor in 2 cases (7.7%). Complication rates were comparable between 5.5–6 and 7–8 mm devices (p = 0.5). There were no complications associated with the DED 2heal, no hemorrhagic complications and no mortality. Besides the technical problems described above, there were no technical asymptomatic complications such as asymptomatic thromboembolism, dissection, or perforation.
Of 24 elective procedures, 22 (91.7%) patients had a discharge mRS of 0, 1 (4.2%) had a mRS of 1, and 1 (4.2%) had a mRS of 2. The 2 patients with SAH had mRS scores of 0 and 5, respectively, in the latter case the poor outcome was SAH related and not treatment related.
Angiographic and clinical follow up
Angiographic and clinical follow up was available for 24 patients with 30 aneurysms. Angiographic control was performed by DSA in 20 of 24 (83.3%) patients, by CTA in 3 (12.5%), and by MRA in 1 (4.2%). The median follow up was 6 months (IQR: 2–6 months). Eight of 30 (26.7%) aneurysms showed complete occlusion (OKM D), 6 (20.0%) had an entry remnant (OKM C), 13 (43.3%) showed subtotal filling (OKM B), and 3 (10.0%) showed total filling (OKM A). Favorable occlusion (OKM C + D) was achieved in 14 of 30 (46.7%) aneurysms. Compete occlusion rates were 29.2% (7/24) among 5.5–6 mm devices and 16.6% (1/6) among 7–8 mm devices (p = 1.0). Distal fish-mouthing was observed in a single case (4.2%) of DED 2heal 5.5 × 20 mm implantation for treatment of a paraophthalmic ICA aneurysm. As the fish-mouthing was mild, no interventional therapy was required and the patient was followed up. There was no collapse of the device braid. Mild intimal hyperplasia was observed in 3 of 24 (12.5%) DEDs that were followed up (DED 5.5 × 25 mm in the BA, telescoping DED 5.5 × 20 and 5.5 × 25 mm in the paraophthalmic ICA, and DED 5.5 × 20 mm in the posterior inferior cerebellar artery). There was no moderate or severe intimal hyperplasia and no FD occlusion.
Twenty-two of 24 (91.7%) patients had an mRS score of 0 (thereof one improved from mRS 1 after procedural thromboembolic infarction), 1 had an mRS score of 1 (improved from 2 after procedural thromboembolic infarction), and 1 had an mRS score of 4 (improved from 5 after SAH).
Discussion
The present study demonstrates that implantation of a large diameter DED was feasible in 96% of cases, with adequate wall apposition achieved in these cases. The major complication rate was low at 3.8%. Complete and adequate aneurysm occlusion rates were 27% and 47%, respectively, at mid-term follow up. In particular, implantation of 7 and 8 mm DEDs was feasible in all cases with good wall apposition and no major complications.
Successful FD treatment includes complete coverage of the aneurysm neck while maintaining complete wall apposition along the entire stent length and avoiding proximal or distal fish-mouthing. 5 The difficulty of FD implantation increases with larger neck widths, fusiform morphology, or dysplastic and enlarged parent vessels because of the increased distance to be covered. As shown in this study, large diameter DEDs are predominantly used in situations with complex vascular anatomy. The median aneurysm size was 10.5 mm with a median parent artery diameter of 5.1 mm, which exceeds previous studies using unselected implant sizes. In the DED study by Kraus et al., the median aneurysm size was 8.9 mm with a parent artery diameter of 3.9 mm, and in the study by Trivelato et al., the median aneurysm size was 6.7 mm.9,10 The proportion of fusiform or dissecting aneurysms was also high at 28%, compared to 13% in the study by Trivelato et al. and 19% in the study by Kraus et al.9,10 When interpreting the results, it is important to keep in mind that a subset of complex procedures may confound the clinical and angiographic results.
In FD procedures, the maximum diameters of the PLZ and DLZ are key determinants in implant selection. Undersized devices carry the potential risk of endoleak, while significantly oversized devices may reduce the effectiveness of flow diversion.11,12 In general, we oversize the FD by 0.5 to 1 mm compared to the inner arterial diameter to improve wall apposition. However, in some 7–8 mm diameter DED cases, the FD diameter exceeded the PLZ or DLZ by more than 1 mm. This is because the parent artery at the site of the aneurysm was dysplastic with a consequently larger diameter than the PLZ and DLZ, which was also the rationale for treatment with a large-diameter FD.
In the present study, wall apposition was generally adequate but required balloon or stent assistance in 16%. To date, there is one study by Butt et al. that selectively analyzed the 5.5 and 6 mm diameter DEDs. 13 The mean aneurysm size was 19.8 mm with a neck width of 6.8 mm, which is comparable to the present study. Fusiform or dissecting aneurysms accounted for 21% and all aneurysms were located in the ICA (89%) or vertebrobasilar artery (11%). The PLZ was 5.4 mm and the DLZ was 4.5 mm, which is within the range of the present study. The authors reported that all procedures were technically successful, but adjunctive stents were required in 28% to improve wall apposition due to suboptimal proximal apposition or fish-mouthing. A mean of 1.1 stents were implanted per-procedure in the current study compared to a mean of 1.2 in the study by Butt et al. 13 Adjunctive coiling was performed in 43% in the study by Butt et al. while no additional coils were used in the current study. This large difference may be explained by differences in practice standards between institutions.
Given that the parent artery was dysplastic in 3 of 5 cases using 7 and 8 mm diameter DEDs, implantation of these devices was successful in all cases, but required additional modeling with balloon and/or stent due to inadequate wall apposition in 2 procedures. In all 5 cases, the technical challenge was to achieve adequate deployment and wall apposition of the entire stent length, which was either 40 or 50 mm. This length typically included one or more curves in the ICA, which further complicates DED deployment as the device may show suboptimal opening behavior in those settings. In these situations, simultaneous pushing the partially deployed DED into the curve in conjunction with the microcatheter improved device deployment. The ability of subtotal resheathability allows for multiple delivery maneuvers, and the stent can be deployed in a stepwise fashion. The 7 and 8 mm DEDs must be delivered through a 0.039” catheter, and we used the Neuroslider 39 from the same manufacturer. The tip of this microcatheter is sufficiently soft and flexible and we had no problems catheterizing the ICA and BA. Of note, the large-diameter DEDs are usually not needed for more distal arteries, which typically have smaller arterial diameters, even if they are dysplastic.
In the present study, the mid-term complete and favorable occlusion rates were 27% and 47%, respectively. These rates are lower than those reported by Butt et al. who reported mid-term complete and favorable occlusion rates of 63% and 75%, respectively. 13 These higher rates may be explained in part by the higher proportion of aneurysms treated with adjunctive coiling in the Butt et al. series.
However, occlusion results with the large-diameter stent are lower than in the unselected DED trials. Mid-term complete occlusion rates were 81% in the study by Trivelato et al., 75% in the study by Pinana et al., 89% in the study by Taschner et al,. and 67% in the DED 2heal study by Goertz et al.10,14–16
It should be noted that large aneurysms and fusiform aneurysms are a risk factor for incomplete aneurysm obliteration after flow diversion and may take longer to achieve complete occlusion. 17 Of note, progressive aneurysm occlusion (including subtotal filling) was observed in 88% in the present study. Therefore, it could be speculated that complete and favorable occlusion rates will increase with longer follow up, which needs to be investigated in further studies. At this point, additional coiling—if technically feasible—could be advocated if rapid aneurysm obliteration is desired.
Flow diverters typically have high braid stability due to their densely woven structure. In the meta-analysis by Ortega-Gutierrez et al., fish-mouthing was reported in 3% and device braid narrowing, collapse or deformation in 9%. 18 One could speculate that large diameter FDs may be associated with lower braid stability for structural reasons, but our data showed fish mouthing in only 4.2% and high braid stability, which is within the range of the cited meta-analysis. Of note, there was no fish mouthing or braid changes at follow-up among the 7 and 8 mm devices. Procedural thromboembolic complications arise from the substantial metal coverage of FDs and are a significant concern in flow diversion procedures. Advanced FDDs have undergone structural and modifications to mitigate the thrombogenic potential of the treatment. In this context, the DED demonstrated major complication rates of 5% in the study by Trivelato et al., 4% in the study by Pinana et al., and 3% in the study Taschner et al.10,14,15
In the present study, major complications occurred in 4% (1 major stroke), which is well within the range of the DED studies cited above. Consistent with this, there was no morbidity in the large-diameter DED study by Butt et al. 13 Given that large aneurysm size and fusiform morphology are also risk factors for ischemic complications, these results suggest that large-diameter DEDs have a reasonable safety profile despite their high metal content due to their large diameter and length.
In conclusion, implantation of large-diameter DEDs was feasible and reasonably safe. However, further studies are needed to define their long-term efficacy, especially with regard to aneurysm obliteration. To date, the 7 and 8 mm DEDs stand out, as there are no competing FDs with these implant diameters. While the SILK (Balt Extrusion, Montmorency, France) and the Pipeline Vantage Embolization Device (Medtronic, Dublin, Ireland) are also available in 6 mm diameter, the maximum diameter of the Flow-Redirection Endoluminal Device (FRED; Microvention) is 5.5 mm and that of the first-generation Pipeline Embolization Device (Medtronic) is 5 mm. The large-diameter DEDs represent an important addition to the neurointerventional armamentarium, enabling endoluminal therapy of complex vascular geometries, such as large and fusiform aneurysms and dysplastic parent arteries, which might otherwise require parent vessel occlusion or surgical therapy.
Limitations
The major limitations of the study are its single-center and retrospective design. The study group is inhomogeneous with a large proportion of complex cases, including large aneurysms, fusiform aneurysms, and dysplastic parent vessels. These features may lead to worse clinical and angiographic outcomes. Clinical and angiographic follow up is lacking in several cases, particularly with 7 and 8 mm devices, which may bias the results. Although the present study shows promising feasibility and safety and acceptable medium-term efficacy, further studies are needed to define the clinical impact of large-diameter FDs.
Conclusions
Implantation of large-diameter (≥5.5 mm) DEDs was feasible and safe, and acceptable mid-term occlusion rates were achieved given the complex subset of aneurysms studied. Overall, wall apposition was sufficient with only a minority requiring additional balloon angioplasty or stent implantation. The 7 and 8 mm DEDs are particularly noteworthy because there are no comparable devices available from competing manufacturers. However, they do have clinical utility, for example, in large-diameter ICA and vertebrobasilar arteries, large and fusiform aneurysms, and dysplastic parent vessels. Further studies are needed to define the indications for these devices and to evaluate their mid- and long-term efficacy.
Footnotes
Data statement
All data will be made available upon request in an anonymized manner.
Declaration of conflicting interests
CK serves as consultant for Acandis GmbH (Pforzheim, Germany) and as proctor for MicroVention Inc./Sequent Medical (Aliso Viejo, CA, USA). DZ is on the speaker’s bureau of Philips (Amsterdam, the Netherlands) and lecturer for Amboss GmbH (Cologne, Germany). The other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.