
Abstract
Purpose
The prognostic relevance of post-mechanical thrombectomy (MT) subarachnoid hemorrhage (SAH) remains controversial. This study aimed to investigate whether the thickness of the SAH clot affects clinical outcomes following MT for M2 occlusion.
Methods
A retrospective analysis was conducted on a prospective database of patients who underwent MT for isolated M2 occlusion. Patients were categorized into three groups based on the presence and thickness of SAH. Clinical and angiographical characteristics and outcomes were compared.
Results
Of the 36 patients included, SAH was observed in 15 (42%). When comparing patients with no SAH (grade 0) or thin SAH (grade 1) (N = 28) with those who had thick SAH (grade 2) (N = 8), patients with Grade 2 SAH required a higher number of passes and had a more severe angulation at M2. Patients with SAH Grade 2 had significantly worse NIHSS scores at 24 h (median, 4 vs. 14), but only one patient was identified as having a symptomatic intracranial hemorrhage. Patients with SAH Grade 2 were found to have a lower rate of favorable outcome (modified Rankin scale 0–2) (23% vs. 75%, P = 0.0026) and higher mortality (25% vs. 0%, P = 0.0499) at 90 days.
Conclusion
The study found that thick SAH prevents clinical recovery after MT for M2 occlusion, even in cases of successful recanalization, and is associated with an unfavorable outcome. Thick SAH after MT is also linked to an increase in the number of passes and severe angulation at the M2 segment.
Introduction
Numerous multicenter prospective randomized clinical studies conducted since 2015 have demonstrated the safety and efficacy of mechanical thrombectomy (MT) for patients experiencing large vessel occlusion. 1 However, further evidence is required to support the use of MT in more distal artery occlusions, also known as medium-vessel occlusions (MeVO). Despite this, MT is commonly performed in cases of MeVO stroke, particularly in patients with MCA M2 occlusion.2–4 Subarachnoid hemorrhage (SAH) is one of the major complications of MT.5–7 Studies have identified distally situated occlusion as a risk factor for SAH related to MT.8–10 The prognostic relevance of post-MT SAH remains controversial. Several reports suggest that post-MT SAH has no effect on clinical outcome.5,7,11 However, from the clinical studies with aneurysmal subarachnoid hemorrhage, large subarachnoid clot volume has been reported as a predictor of poor outcome or delayed cerebral ischemia.12–14 Thus, the relationship between post-MT SAH and functional outcome may contribute more to clot thickness and distribution than the presence or absence of SAH. The degree to which subarachnoid clot thickness impacts outcomes remains unexplored. Therefore, this study aimed to investigate whether there is a difference in outcome based on the thickness of the subarachnoid clot after MT on M2 occlusion.
Methods
This study received approval from the Ethics Committee of Yamaguchi University (approval number H2020-095-2). The requirement for written informed consent was waived as the study was retrospective. The study included a retrospective analysis of a prospective database of patients who underwent MT for acute ischemic stroke at the institution between January 2020 and March 2023.
Patients
The inclusion criteria were as follows: 1) patients with acute ischemic stroke (<24 h after last time known well) who underwent MT using a stent retriever (SR), an aspiration catheter (AC), or a combination of both as the primary treatment; 2) MCA M2 segment occlusion on angiography; and 3) prestroke modified Rankin scale (mRS) score ≤ 3. The M2 segment in this study was defined as the MCA segment from the genu to the circular sulcus of the insula; early MCA branches arising from the M1 segment before the genu was not considered.3,7
We collected the patients’ baseline characteristics, including age, sex, vascular risk factors (hypertension, diabetes, dyslipidemia, atrial fibrillation, and current smoking), IV tPA use, admission National Institutes of Health Stroke Scale (NIHSS) score, baseline Alberta Stroke Program Early CT Score (ASPECTS) on initial diffusion-weighted MRI image, time metrics, M2 divisions (superior, inferior, or both), and proximal/distal M2 location. The proximal and distal M2 segments were distinguished by a line delineating the mid-height of the insula. 7
Endovascular treatment
All procedures were performed using a transfemoral artery approach with local anesthesia or conscious sedation. An 8F or 9F balloon-guided catheter was used in all cases. All the patients were treated with SR alone or combined with CA. The choice of MT device and technique was left to the treating operator's discretion. In cases where the initially selected device failed to achieve successful reperfusion despite multiple attempts, rescue therapy was initiated by transitioning to the alternative strategy. Successful recanalization was defined as modified treatment in cerebral ischemia 2b/3.
The study used Trevo NXT 3 × 32 or 4 × 28 (Stryker, Kalamazoo, MI, USA), Solitaire X 3 × 40 or 4 × 40 (Medtronic, Minneapolis, MN, USA) as the SRs. The CAs used were 3MAX (Penumbra Inc., Alameda, CA, USA), AXC Catalyst 6 or Vecta 46 (Stryker), and Sofia 5F (MicroVention, Aliso Viejo, CA, USA).
Image analysis
A noncontrast brain CT scan was conducted within 24 h after MT to detect the presence of SAH and other hemorrhagic events. SAH was identified by observing hyperdensity in the subarachnoid space. Patients were then divided into three groups based on the severity of SAH on CT: Grade 0, no SAH; Grade 1, thin (<10 mm) SAH; and Grade 2, thick (≥10 mm) SAH (Figure 1). We selected 10 mm as the cut-off because the median blood clot thickness of SAH in this series was 10.1(IQR: 6.35-11.9) mm. We also considered the distribution of SAH, and defined as diffuse SAH whenever the hemorrhage was detected in more than one subarachnoid location, including the Sylvian fissure, the convexity, the interhemispheric fissure, and the perimesencephalic cistern {Renu, 2022 #20}. Hemorrhagic events other than SAH were defined according to the definitions published elsewhere {Hacke, 1995 #33} {Hacke, 1998 #17}. Hemorrhagic infarction 1 (HI1) was defined as small petechiae along the margins of the infarct; hemorrhagic infarction 2 (HI2) as confluent petechiae within the infarcted area but no space-occupying effect; parenchymal hemorrhage (PH1) as blood clots in 30% or less of the infarcted area with some slight space-occupying effect; and parenchymal hemorrhage (PH2) as blood clots in more than 30% of the infarcted area with substantial space-occupying effect.
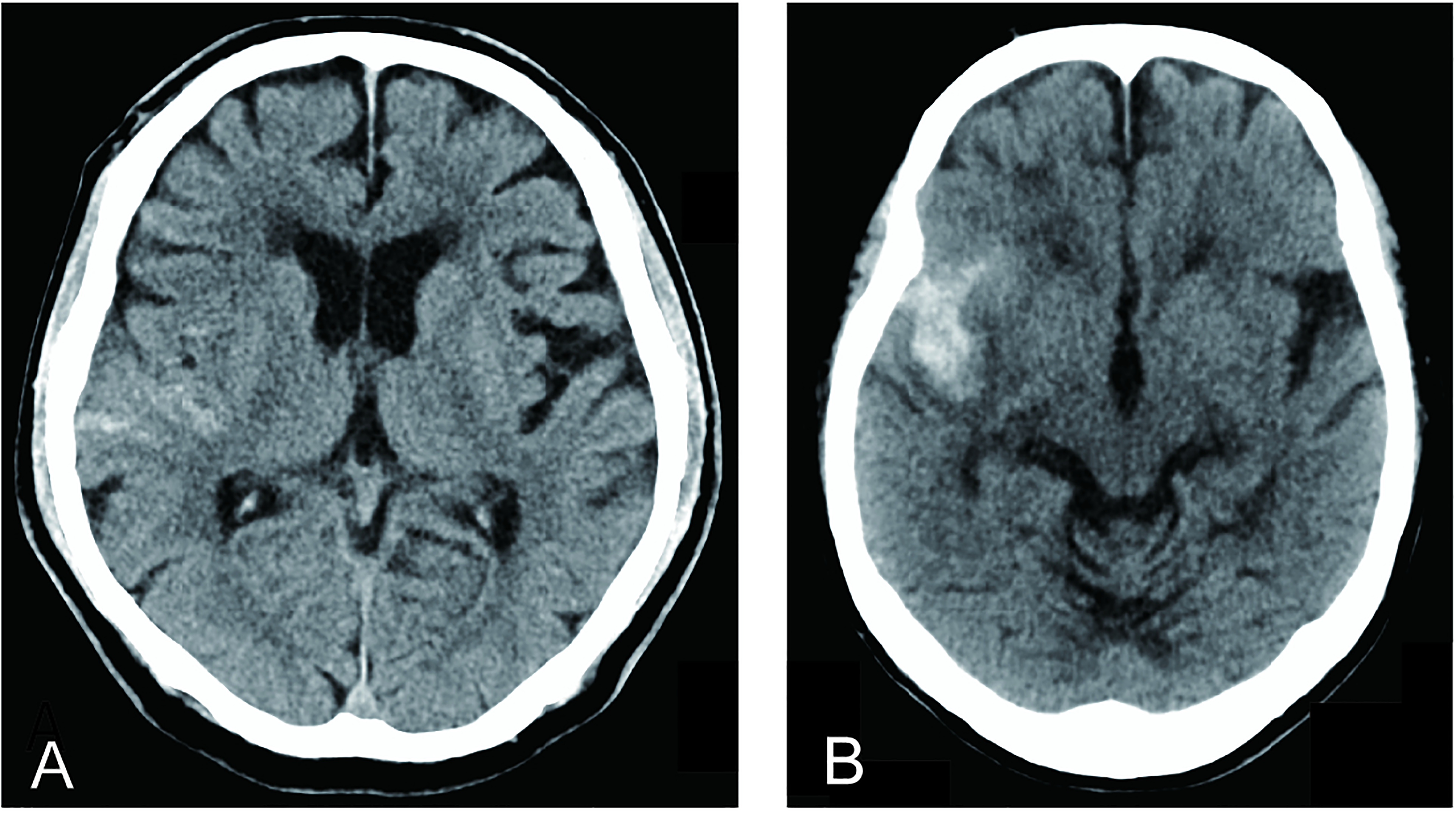
SAH classification. A: Grade 1-thin (<10 mm) SAH at the sulcus, B: Grade 2 thick (≥10 mm) SAH at the Sylvian fissure.
As acute vessel angulation has been associated with an increased risk of SAH after MT, 7 we measured the angulation of the vessels using Fujifilm Synapse picture archiving and communication system (Fujifilm, Tokyo, Japan) tools for angle measurement. We measured the IC–M1, M1–M1′, M1–M2, and M2–M2′ angles according to previous reports, with some modifications.6,7 The IC–M1 angle was measured from the IC terminal to the proximal part of the M1 segment. The M1–M1′ angle was identified as the sharpest angle of the M1 segment. The M1–M2 angle was measured from the M1 segment as it turned superiorly (at the M1–M2 junction) to become the M2 segment into which the thrombectomy device was positioned as the vessel coursed toward the circular sulcus. The M2–M2′ angle was identified as the sharpest angle between the beginning and the occluded part of the M2 segment. To measure the angles, we used a final angiogram of the frontal projection for IC–M1, M1–M1′, and M1–M2 angles and of the lateral projection for M2–M2′ angles (Supplemental Figure 1).
Outcomes
The clinical assessment was conducted after 24 h using the NIHSS scale and after 90 days using the mRS scale. We considered an mRS score of 0–2 a favorable clinical outcome. The incidence of symptomatic intracranial hemorrhage (ICH) was tabulated to evaluate safety outcomes. Symptomatic ICH was defined as any intracranial hemorrhage associated with an increase of ≥4 points in the NIHSS score within 24 h. 15
Statistical analysis
The study aimed to determine the impact of thick SAH on the outcome. The study found no significant difference in the clinically favorable outcome between patients with SAH Grade 0 (no SAH) and those with SAH Grade 1 (thin SAH), with both groups having similar outcomes of 71% and 83%, respectively. Therefore, to analyze the outcome and background of patients, we combined patients with SAH Grades 0 and 1 into a single group and compared them with patients with SAH Grade 2 (thick SAH).
We used Prism 9 (GraphPad Software, San Diego, CA) to analyze all the data. Continuous variables were presented as mean ± standard deviation (SD) or median with interquartile range (IQR), while categorical variables were shown as frequency counts. The Mann–Whitney U test was used to evaluate the differences between clinical characteristics, and Fisher's exact test was used for intergroup comparisons of categorical variables. All 95% confidence intervals and P values were based on two-sided hypothesis tests, where P < 0.05 was considered statistically significant.
Results
This study included 36 patients who met the inclusion criteria. The mean age of patients was 76.3 ± 10.9 years, and 47% (17/36) were female. The successful reperfusion rate was 81%. No patient showed any visible vessel perforation or angiographic contrast extravasation during the procedure. Within 24 h after MT on noncontrast CT, SAH was detected in 15 patients (41.7%), including Grades 1 and 2. The baseline characteristics are presented in Table 1. There were no significant differences between the groups regarding demographics, cardiovascular risk factors, clinical severity using the NIHSS score, ASPECTS on the initial diffusion-weighted image on MRI, the use of intravenous thrombolysis, time from last time known well (LKW) to admission, or time from LKW to reperfusion time (Table 1). While the rate of successful reperfusion and the devices used in MT were comparable, the number of passes was higher in the SAH Grade 2 group (median [IQR], 1 [1–2] vs. 2 [1–3], P = 0.048) (Table 1).
Between-Group differences in clinical characteristics and outcomes.
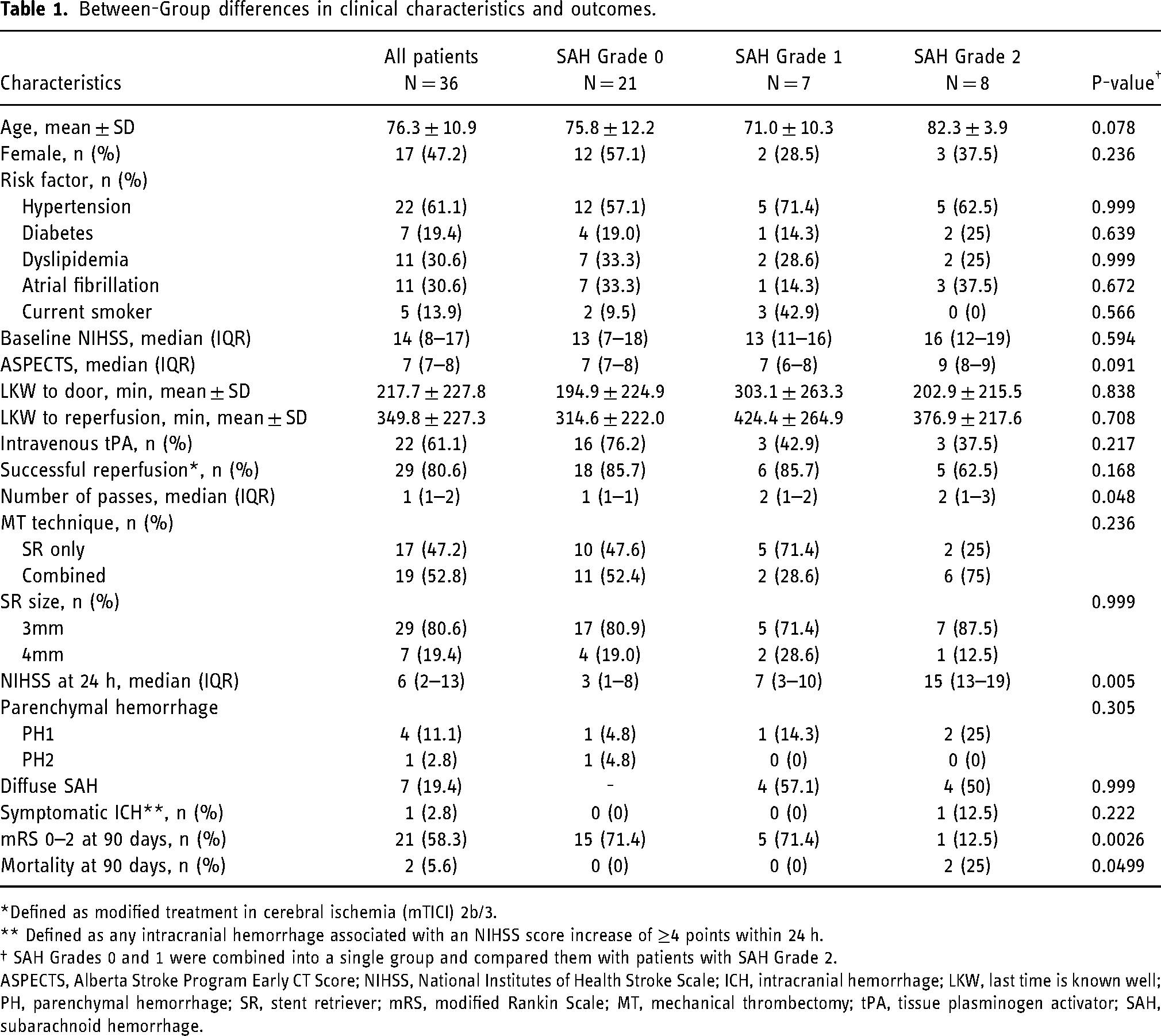
*Defined as modified treatment in cerebral ischemia (mTICI) 2b/3.
** Defined as any intracranial hemorrhage associated with an NIHSS score increase of ≥4 points within 24 h.
† SAH Grades 0 and 1 were combined into a single group and compared them with patients with SAH Grade 2.
ASPECTS, Alberta Stroke Program Early CT Score; NIHSS, National Institutes of Health Stroke Scale; ICH, intracranial hemorrhage; LKW, last time is known well; PH, parenchymal hemorrhage; SR, stent retriever; mRS, modified Rankin Scale; MT, mechanical thrombectomy; tPA, tissue plasminogen activator; SAH, subarachnoid hemorrhage.
The SAH Grade 2 group showed a significantly worse NIHSS score at 24 h (median [IQR], 4 [1–10] vs. 14 [12–17], P = 0.020). However, only one patient (13%) met the criteria of symptomatic ICH, which requires an increase in the NIHSS score by at least 4 points (Table 1). The clinical outcome 90 days after onset was significantly worse in the SAH Grade 2 group. The SAH Grade 2 group had a lower rate of favorable outcomes (75% vs. 23%, P = 0.0026). Additionally, a higher mortality rate (0% vs. 25%, P = 0.0499) was observed in the SAH Grade 2 group; however, SAH was not the primary cause of death in either case (Table 1).
The angiographical characteristics are presented in Table 2. The SAH Grade 2 group showed sharper angulation at the M2 segment (mean [SD], 131.3 [24.2] vs. 101.4 [34.9], P = 0.009), and the total angulation measured in this study was significantly smaller (mean [SD], 521.8 [51.6] vs. 470.3 [37.7], P = 0.013). There were no statistical differences in the rate of involvement of the superior division of M2 (46.4% vs. 62.5%, P = 0.691) and distal M2 occlusion (35.7% vs. 25.0%) between the two groups (Table 2).
Patients’ angiographical characteristics.
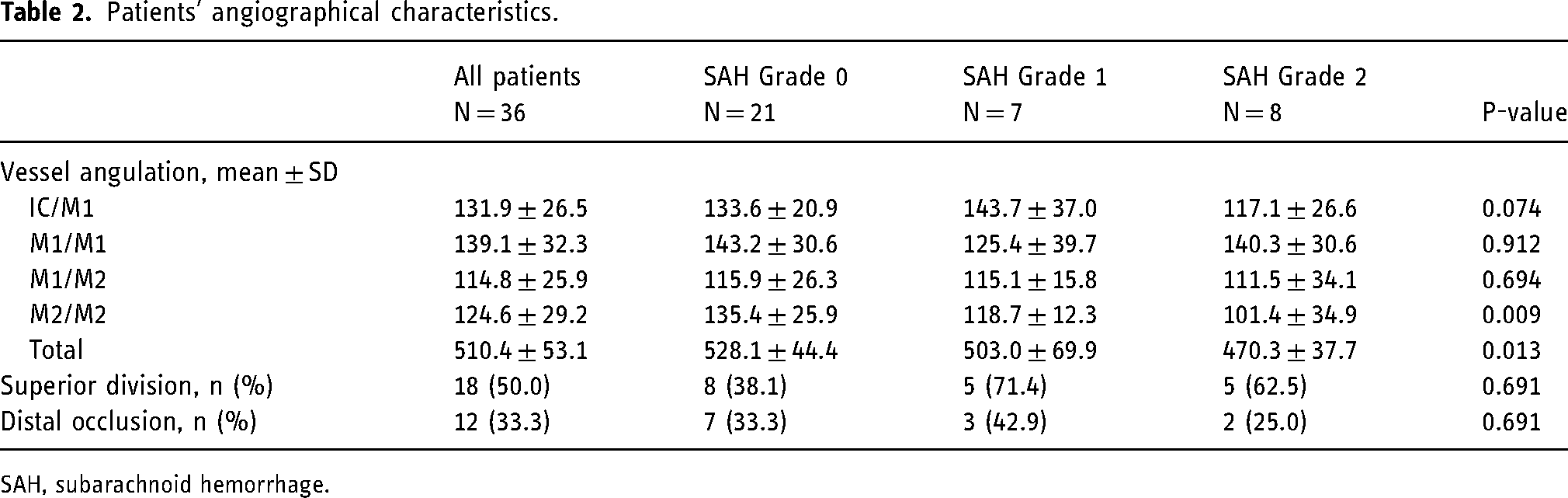
SAH, subarachnoid hemorrhage.
Discussion
During the study, we discovered that blood clot thickness plays a more significant role in the outcome of patients with M2 occlusion after MT rather than the presence of SAH. A thicker SAH prevented clinical recovery after restoring blood flow and worsened functional outcomes even in successful reperfusion patients.
The relevance of SAH post-MT in the prognosis of patients is a subject of debate. Although previous reports suggest that SAH does not necessarily lead to poor outcomes,5,7,16 a recent report by Ren et al. indicates that diffuse SAH, but not local SAH, is associated with poor outcomes and death. 10 In this study, the researchers focused on the thickness of the subarachnoid hematoma and found that thicker hematomas are associated with poor outcomes. Among the patients with aneurysmal subarachnoid hemorrhage, it is well established that thicker and more diffuse SAH is associated with poor outcomes.12,13 Although SAH after MT is not entirely the same as aneurysmal SAH, both experimental swine SAH models and patients with aneurysmal SAH have shown that subarachnoid clots are sufficient to induce spreading depolarization and cause partial cortical infarction. 17 Additionally, thick SAH could lead to vasospasm and delayed cerebral ischemia. 18 Based on the present and previous studies, the correlation between post-MT SAH and functional recovery can be influenced to a greater extent by clot thickness and/or distribution rather than solely by the presence or absence of SAH.10,17,18 Interestingly, we found that thick SAH was less likely to cause neurological worsening that would increase the NIHSS score by ≥4 points, which is often used as the definition of symptomatic ICH after reperfusion therapy. Nevertheless, thick SAH prevents neurological improvement even in patients who achieve successful reperfusion and leads to poor outcomes. Other factors that may have contributed to the low incidence of symptomatic ICH in this study included the inability of the NIHSS score to detect further neurological deterioration due to the high pre-treatment NIHSS score and, although not statistically significant, a lower recanalization rate in thick SAH group compared to the other groups. The other interesting point is that different from aneurysmal subarachnoid hemorrhage, there have been no reports on the occurrence of delayed vasospasm or delayed cerebral ischemia after subarachnoid related to MT. This may partly be due to the difference in pathophysiology: aneurysmal hemorrhage is bleeding from cerebral aneurysms with high blood flow, while subarachnoid hemorrhage related to MT is thought to be mainly from perforating branches with low blood flow. In addition, a similar reason as symptomatic ICH, because most post-MT SAH patients already suffer from cerebral infarction and neurological deficits, it might be difficult to diagnose further neurological deterioration even if vasospasm causes additional cerebral ischemia.
This research has identified that an increased number of passes and severe angulation at the M2 segment can be risk factors for thick SAH. These findings are consistent with previous reports.6,7,10 When attempting to pass a microguidewire or other devices through occluded tortuous thin vessels, increasing the number of passes may raise the risk of perforation or dissection of arteries. Although clear contrast extravasation on DSA was not detected during the process, microperforation or dissection of the small vessels may cause delayed occult SAH. 6 Furthermore, acute angulation results in more friction between the vessel wall and device, which may cause increased vessel stretching and the avulsion of small perforating branches or venules during clot retrieval. The more times the device is passed, the greater the risk of such a traction injury.7,10,19 Several reports suggest that aspiration catheters and stent retrievers help avoid SAH. Theoretically, SRs tend to cause more extensive endothelial damage compared to aspiration catheters during stent retrieval due to their continuous radial pressure against the vessel wall.8,20,21 Moreover, SRs may apply more traction forces on the vessel, which potentially causes deformation in the adjacent anatomy and leads to the stretching and rupture of small arterioles or venules. 7 Using ACs has been reported to be effective in avoiding traction injury.7,22,23 Even if an SR is used, capturing the stent into the AC would decrease the radial and tractional forces exerted by the SR and reduce the risk of SAH; however, this is not yet well established.22,23
The occurrence of SAH in this study was relatively high at 42% as compared to a previous study. The frequency of post-MT SAH could vary due to differences in the technique of thrombectomy, the definition of hemorrhage, and the timing and modality of follow-up neuroimaging.10,23,24 Furthermore, recent reports suggest that the distal location of vessel occlusions such as M2 is associated with a higher risk of post-MT SAH than large vessel occlusions.7,10 Another reason for the relatively high frequency of SAH could be the older age of the patients enrolled in this study. The mean age of all patients in this study was 76 years and 82 years for patients with SAH Grade 2 alone. Several systematic reviews found higher rates of ICH after MT in patients aged 80 years.25,26 Vascular tortuosity increases with age, 27 which may increase the risk of tractional injury and the number of passes required to achieve successful recanalization, thereby increasing the risk of SAH, consistent with our present study.
Several limitations should be acknowledged. First, the study's small sample size, lack of long-term follow up, and single-center, retrospective, observational study design necessitate careful interpretation of the results, although the patients were consecutively enrolled. Especially, given the small sample size, caution should be exercised in interpreting results that do not show significant differences, such as the frequency of involvement of superior division of M2, as well as those that do show statistical significance. Second, no multivariate analysis was performed to account for confounding factors such as comorbidities, pre-existing vascular conditions, or procedural variables during MT in between-group comparisons; however, due to the small number of patients in this study, it is impossible to guarantee the reproducibility of the analysis. Finally, measuring vessel angles using 2D angiogram images provides only an approximation of vessel angulation, which can vary depending on the degree of angulation of the tube or a slight rotation of the patient's head.
Conclusions
After MT for M2 occlusion, thick SAH can still cause neurological symptoms even if the recanalization is successful, and it is also linked to an unfavorable outcome. Thick SAH can occur due to increased passes and severe angulation at the M2 segment during the procedure. More research is needed to confirm these findings and identify other procedural factors that may cause SAH, as well as ways to prevent it.
Supplemental Material
sj-docx-1-ine-10.1177_15910199241270706 - Supplemental material for Degree of subarachnoid hemorrhage affects clinical outcome after mechanical thrombectomy for M2 occlusion
Supplemental material, sj-docx-1-ine-10.1177_15910199241270706 for Degree of subarachnoid hemorrhage affects clinical outcome after mechanical thrombectomy for M2 occlusion by Fumiaki Oka, Takuma Nishimoto, Naomasa Mori, Akiko Kawano and Hideyuki Ishihara in Interventional Neuroradiology
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author discloses receipt of the following financial support for the research, authorship, and/or publication of this article: grants from the JSPS KAKENHI grant (23K08499).
Japan Society for the Promotion of Science, (grant number 23K08499).
This study received approval from the Ethics Committee of Yamaguchi University (approval number H2020-095-2).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.