
Abstract
We describe a case of a 22-year-old man with a traumatic occipital artery pseudoaneurysm revealed by a painful expanding neck hematoma after a penetrating knife injury. A neuroendovascular consultation was requested after a computed tomography angiogram showed active pseudoaneurysm bleeding. Anatomical considerations of the upper cervical region including dangerous anastomosis between the vertebral and internal carotid artery are discussed, illustrating how this impacted our treatment strategy. We also discuss other treatment modalities after a thorough literature review of traumatic occipital artery pseudoaneurysms.
Introduction
Traumatic occipital artery pseudoaneurysms are an infrequent condition related to head trauma, with fewer than 20 cases described in the literature. We present a case involving a 22-year-old male with an occipital artery pseudoaneurysm after a penetrating knife injury to the neck. Anatomical considerations of the occipital artery in the neck are very important for the management and treatment choice, particularly because of the dangerous anastomoses in the upper cervical region. Through this case, we describe important aspects relevant for neurointerventionists as it can help in determining the procedure indication, selecting the appropriate materials, and using the best technique.
Case presentation
A 22-year-old male presented to the emergency department after being stabbed with a knife by his roommate. His medical history was positive for illicit drug use (cocaine and marijuana). He received sutures for the subcutaneous and skin wound and a 24-hour in-hospital assessment for infections, vaccination, and other minor injuries from the altercation. The patient was prepared for discharge; however, the clinical team noted a bulging pulsatile enlarging mass at his posterior left neck (Figure 1A). A computed tomography angiogram (CTA) was performed and while waiting he developed hypotension. After hemodynamic stabilization in the intensive care unit (ICU), the CTA showed a left occipital artery pseudoaneurysm (Figure 1B). A request was then made for a neuroendovascular assessment.

Male patient, 22-year-old, after penetrating neck injury. (A) Mass lesion at the left neck. (B)Large pseudoaneurysm with bleb (black arrow). (C) Internal carotid artery (ICA) injection (profile) before the procedure. (D) Left subclavian injection (anteroposterior) to verify potential occipital-vertebral artery anastomosis. (E) Left external carotid artery. The black arrow points to the splenial or posterior cervical branch, which may anastomose with the left vertebral artery. Measurements of the pseudoaneurysm and the artery were made for coil selection. (F) Occipital artery occlusion with microcatheterization of the occipital artery pseudoaneurysm. (G) Final angiogram control (profile) with occipital artery occlusion right after the splenial branch. (H) Postprocedure head computed tomography showing the coils artifact with local edema (double white arrow).
Occipital artery anatomy
The occipital artery typically originates from the posterior surface of the external carotid artery, which is usually located above the ascending pharyngeal artery (APhA), but sometimes they can be found together in a common trunk. This artery supplies muscular, cutaneous, and meningeal territories, and it can sometimes give rise to the stylomastoid artery, which is more commonly derived from the posterior auricular artery (Figure 2). When diminutive, the occipital artery can be replaced by branches from the vertebral, deep cervical, or posterior auricular arteries. 1
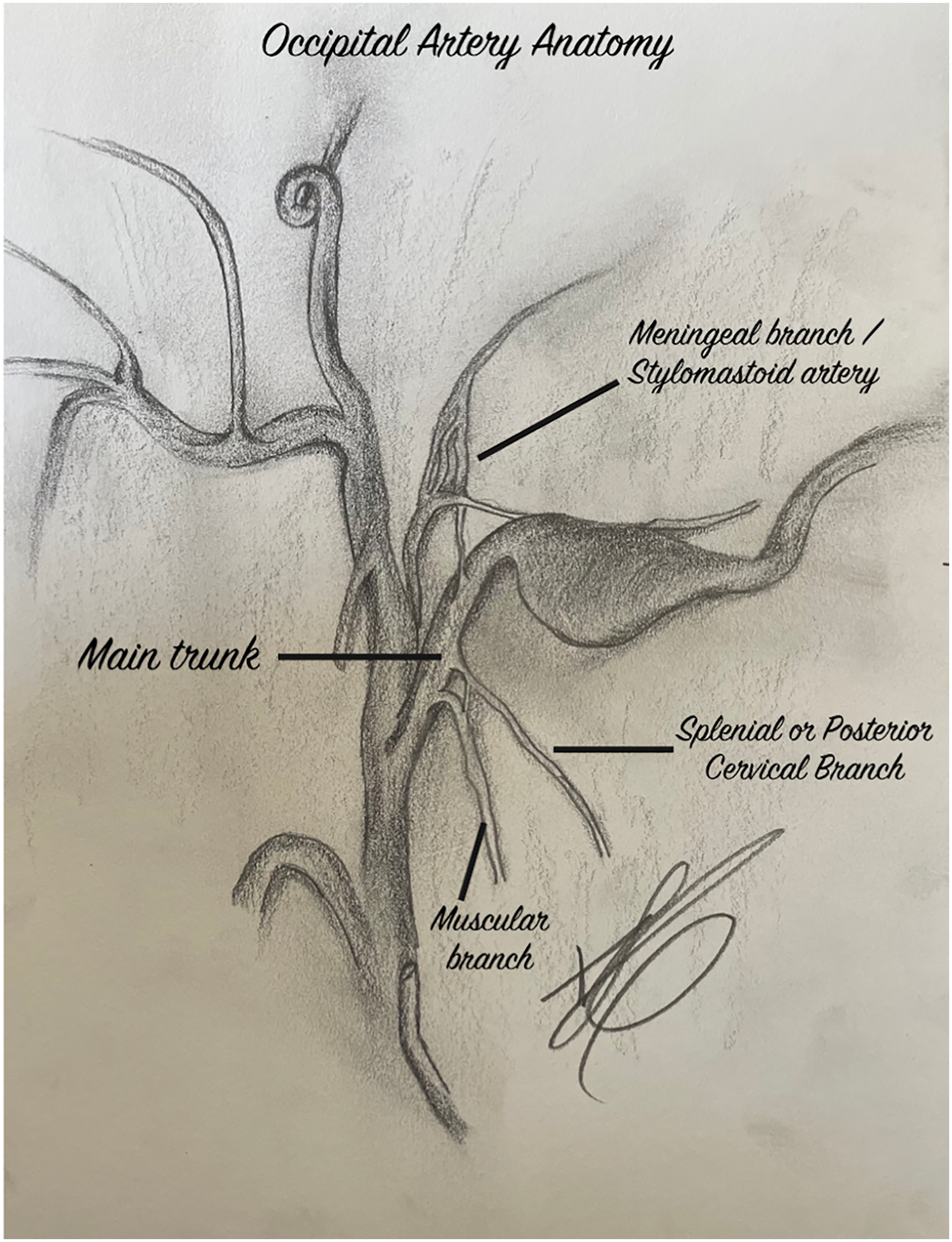
Occipital artery anatomical illustration with some important anastomotic branches.
Notably, the occipital artery has three segments. The first or ascending branch passes backward to the posterior belly of the digastric muscle, in the retrostyloid space. This branch extends to the sternomastoid muscle and may join with other muscular branches from the external carotid artery (ECA) as well as with ascending branches from the subclavian artery. Moreover, in about 60% of cases, this segment also gives off the stylomastoid artery, which passes through the stylomastoid foramen with the facial nerve and ramifies in the tympanic cavity to supply the muscles, the semicircular canals, and the intracranial portion of the facial nerve.1,2 It also supplies the meninges of the posterior fossa and has anastomoses with other meningeal branches from the middle meningeal artery, the APhA, the inferolateral, and meningohypophyseal trunks from the ICA, and the posterior meningeal artery from the vertebral artery.3,4
The second or horizontal segment is separated from the vertebral artery through the rectus capitis lateralis muscle, and it gives rise to two important anastomotic pathways: an ascending or mastoid branch and a descending branch. The descending branch is also known as the posterior cervical artery or the splenial artery. It plays a crucial role in carrying important anastomoses with the vertebral artery. 1 Those anastomoses are C1 and C2 segmental arteries, which are considered remnants of type I and type II proatlantal intersegmental arteries, embryological arteries that serve as connections between the carotid and vertebrobasilar system in the fetal period.3,5 The ascending meningeal branch or mastoid branch gives small muscular branches and penetrates the skull through the mastoid foramen, just behind the sigmoid sinus. It nourishes the meninges from the subtentorial occipital convexity, with branches to the jugular foramen, where it shares territory with the jugular and hypoglossal branches from the ascending pharyngeal artery, and with posterior meningeal branches from the vertebral artery.3,4
The third or ascending segment (i.e. subgaleal) gives rise to lateral and medial terminal cutaneous branches toward the scalp, which has anastomoses with the opposite occipital artery, and with branches from the posterior auricular artery and the superficial temporal artery (Figure 2). 1
Angiogram, anatomical pearls, and endovascular technique
After a left internal carotid artery and vertebral injection to verify the presence of any open dangerous anastomosis, we placed our 06F guiding catheter (CERENOVUS, Johnson & Johnson, USA) at the ECA main trunk . The pseudoaneurysm (14.8 × 17.3 mm) was located immediately after the ascending meningeal branch in the horizontal or second segment of the occipital artery. We have decided to perform a parent vessel occlusion with coils alone without any type of liquid embolic agent, to avoid reflux into the meningeal branch or splenial artery. There are many strategies to perform parent vessel occlusion and we chose endovascular trapping with partial embolization of the pseudoaneurysm. This approach starts by crossing the pseudo aneurysm segment with a microcatheter and delivery of coils distal and proximal to the pseudoaneurysm.
We measured the diameter of the occipital artery before and after the neck of the pseudoaneurysm (average 2 mm). We decided to use HydroCoils (MicroVention Inc. Tustin, CA, USA) to increase packing density and then we deployed Axium™ Prime coils (Medtronic, Irvine, CA, USA) inside the aneurysm. The latter step was done to facilitate delayed thrombosis. After deploying two long Axium™ coils inside the aneurysm, we embolized the proximal occipital artery with three HydroCoils, immediately after the splenial artery at the horizontal segment. Final control revealed patent ICA branches and no thromboembolic complications. The patient was discharged from the ICU with no neurological deficits.
Discussion and literature review
Traumatic pseudoaneurysms of the occipital artery are a rare condition, with only 18 reports in the literature (Table 1). Different trauma mechanisms are associated with these lesions including falls,6–8 blunt head trauma, 9 spontaneous dissection, 10 ventriculoperitoneal shunt, 11 and even a paintball accident. 12 Considering scalp vessels, the superficial temporal artery (STA) traumatic lesions have far more reported cases 13 compared to the occipital probably due to muscular protection. 8 Specifically, in the region between the frontalis and temporalis muscle, the STA lies directly against the skull. 14 Pseudoaneurysms occur when there is partial disruption of an artery, causing blood to dissect through the vessel wall. They do not contain all layers of a normal artery and are not related to branch zones. 15 When caused by blunt trauma, they may take some time to form (days, 8 weeks,7,9,16 months, 12 or years17,18), because a fibrous pseudocapsule forms around the hematoma, which then liquefies and allows the capsule to recanalize with blood flow from the artery, leading to a pseudoaneurysm. 19 In our case, the clinical presentation was in the short term, which we attribute to the mechanism of trauma, a penetrating injury.
Case Reports of Traumatic Occipital Artery Pseudoaneurysm.
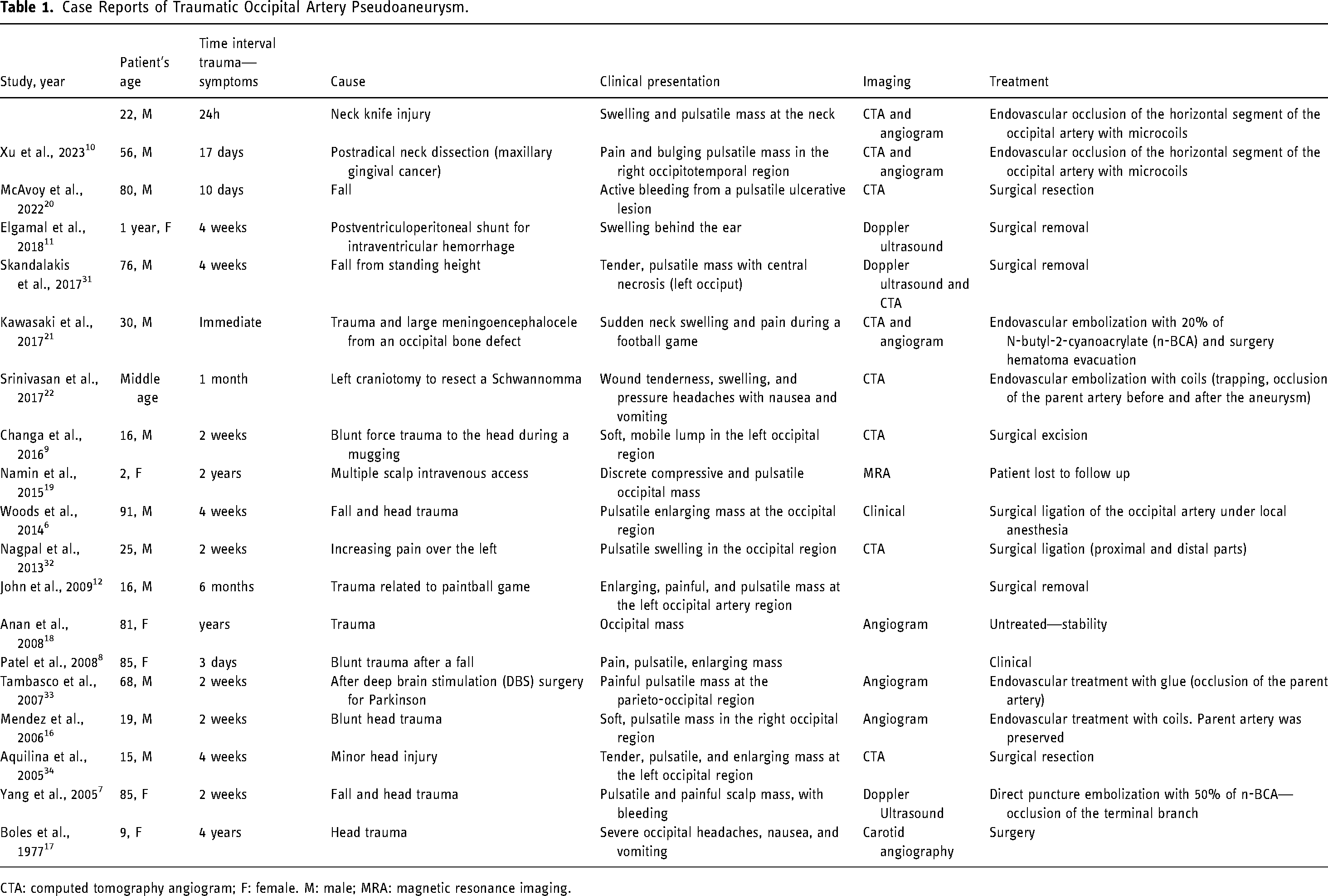
CTA: computed tomography angiogram; F: female. M: male; MRA: magnetic resonance imaging.
In clinical settings, occipital artery pseudoaneurysms typically manifest as a pulsatile mass that gradually enlarges, sometimes accompanied by pulsatile tinnitus. 23 They may or may not be painful. In some cases, active bleeding can occur, which can be life-threatening. 21 Diagnosis may be clinical, and/or with noninvasive imaging, like CTA, magnetic resonance imaging, and duplex ultrasound. 11 However, there is still ongoing debate about whether to perform noninvasive vascular imaging on patients with blunt head and neck trauma. This is due to the low prevalence of cerebrovascular lesions (0.18–2.4% of 122.176 hospital admissions in a meta-analysis) after blunt trauma, as well as the absence of uniform criteria for screening. 24 Most available screening relies on the presence of certain factors such as head trauma, basilar skull fracture, cervical spine injury, cervical abrasion, Glasgow coma score less than 8, facial fracture, thoracic or abdominal injuries, and neurologic deficits. 24 However, not all patients with external carotid arteries pseudoaneurysms caused by blunt trauma will exhibit these symptoms. Hence, medical professionals must maintain a high level of clinical suspicion. For cases of penetrating neck injuries where there is a violation of the platysma and the patient is hemodynamically stable, noninvasive vascular imaging such as CTA should still always be included in the initial clinical approach.25,26
The most-described location for occipital artery pseudoaneurysms is distal, between the second (horizontal) to third (subgaleal) segments of the occipital artery, probably due to the lack of artery mobility in that region, surrounded by dense connective tissue. 9 As this region is easily accessed, we believe it justifies why most described cases were treated with open surgery, even with local anesthesia, 6 although direct puncture embolization may also be a good option with better cosmetic results 7 and less risk of posterior occipital neuralgia. 23 In addition, when dealing with pseudoaneurysms accompanied by a large hematoma that might make scalp dissection difficult, endovascular treatment might be a better option. 22 However, if the lesion requires hematoma evacuation or if the pseudoaneurysms are accompanied by skin necrosis, open surgery might be a better choice. 20
In our case, the pseudoaneurysm was of the second segment of the occipital artery, which is appropriate for an endovascular procedure. Careful anatomical understanding is important for the indication and the appropriate selection of the embolic agent. Given the abundant anastomosis with the vertebral artery through the stapedial artery and proatlantal remnants, and with the ICA through the mastoid and stylomastoid branches, it is important to avoid nonadhesive liquid embolic agents (N-butyl cyanoacrylate, N-hexyl cyanoacrylate, Glubran 2) 27 and particles, which could reflux into these anastomoses, risking stroke and cranial nerve deficits. 3 A recent systematic review evaluating Onyx and glue for facial arteriovenous malformations embolization found a higher rate of complications such as cranial nerve deficits when Onyx was the agent of choice (0% for glue and 14% for Onyx). 28 Trapping with coils was the approach we have chosen for this case, and it is deemed to be a good strategy. Although there are literature reports of external carotid artery pseudoaneurysm embolization with glue 7 and Onyx,29,30 due to potentially dangerous anastomosis with intracranial arteries, we do not recommend it for lesions of the second segment of the occipital artery. Additionally, when dealing with large pseudoaneurysms, it is important to pay attention to the possible mass effect after packing the pseudoaneurysm with embolic material. For this reason, we performed loose packing with relatively few coils inside the aneurysm. Our main goal was the parent artery occlusion without intracranial reflux, with late pseudoaneurysm thrombosis. Moreover, for small stable aneurysms in minimally symptomatic patients, treatment may be conservative. 8
In summary, although open surgery is an excellent choice for distal and easily accessible occipital artery pseudoaneurysms or lesions with associated skin necrosis, an endovascular approach allows successful less-invasive treatment for more proximal lesions. In these cases, the technique and embolic agent choice should consider the potentially dangerous anastomosis from the occipital artery with intracranial arteries as this knowledge is crucial to avoid thromboembolic complications.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.