
Abstract
Ascertaining the etiology of cervical spinal cord dysfunction presents a challenge to clinicians, as the list of differential diagnoses is extensive. Although compressive and inflammatory disorders are common and should be considered immediately, vascular causes are similarly important and acute. The overlap of clinical, magnetic resonance imaging, and cerebrospinal fluid features among the causes of myelopathies may lead to erroneous diagnoses. Such errors may be compounded if routine vascular imaging does not reveal the underlying vasculopathy. We present here three cases in which computed tomography angiography and magnetic resonance angiogram could not clarify the nature of an acute myelopathy, whereas digital subtraction angiography established the diagnosis of spinal cord ischemia.
Case reports
Case 1
An 18-year-old man with a history of neck and back pain attributed to motor-vehicle-associated trauma 2 years prior performed self-administered neck manipulations, after which he immediately noted severe neck pain and diffuse paresthesia below the neck. He also experienced chest pain, shortness of breath, and motor function loss, first in his right arm, then in both arms and legs. At admission, his neurological exam was consistent with an acute spinal cord injury, including a flaccid tetraparesis with a C4–C5 sensory level. Hyperacute magnetic resonance imaging (MRI) ruled out cord compression. Head and neck computed tomography angiography (CTA) were negative. Myocardial ischemia was excluded. Other tests were unremarkable (including lyme, HIV, influenza, C-reactive protein, and hepatitis serologies). 1 The patient was started on dexamethasone and admitted to an intensive care unit with a suspected diagnosis of spinal cord injury without osseous radiographic abnormality (SCIWORA). His condition did not improve; he developed pneumonia and required mechanical ventilation assistance on hospital day 1.
Spine MRI revealed abnormal cord signal extending between the C3 and T1 vertebral levels, involving the anterior and central aspect of the spinal cord and showing restricted diffusion (Figure 1(A)). There was no contrast enhancement. magnetic resonance angiogram (MRA) was unremarkable.

A 18-year-old man with an acute cervical spinal cord syndrome following self-administered neck manipulations. (A) MRI, sagittal T2-weighted image, revealing abnormal cord signal between C3 and T1. (B) DSA, right costocervical trunk injection, posteroanterior projection, early arterial phase, documenting the anatomy of the arterial spinal cord supply. The costocervical trunk consists of the supreme intercostal artery (black arrow) and its sizeable ascending branch, the deep cervical artery (large white arrow). The trunk of the inferior artery of the cervical enlargement (small white arrow) arises from the supreme intercostal artery and crosses the C6–C7 neural foramen. In this instance, it provides both an anterior radiculomedullary branch, the inferior artery of the cervical enlargement per se, and a posterior radiculomedullary branch. The anterior radiculomedullary branch divides at the C5–C6 level into ascending and descending rami, supplying the anterior spinal artery (white arrowheads). The posterior radiculomedullary has a parallel course and supplies the right posterior-lateral spinal artery (black arrowhead). (C) DSA, right costocervical trunk injection, posteroanterior projection, late arterial phase, revealing an early, and exaggerated capillary blush outlining the spinal cord contour, an angiographic marker of localized hyperemia. This image emphasizes the importance of the hemodynamic analysis offered by DSA. (D) DSA, right costocervical trunk injection, posteroanterior projection, early venous phase, showing the anatomy of the spinal venous drainage. The rapid opacification and conspicuity of the pial venous system indicate—in combination with the hyperemia mentioned above—the presence of a luxury perfusion phenomenon typical of the subacute period of ischemia. (E) DSA, right costocervical trunk injection, posteroanterior projection, nonsubtracted arterial phase. This image provides a better appreciation of vascular and skeletal topographic landmarks (same legend as Figure 1B). Note, in particular, the passage of the radiculomedullary branches under the right C6 pedicle (i.e., across the C6–C7 neural foramen). (F) MRI, axial gradient echo image across the C6–C7 intervertebral disc space, documenting a foraminal disc herniation with severe narrowing of the right C6–C7 neural foramen (circled area). DSA: digital subtraction angiography; MRI: magnetic resonance imaging.
At this point (day 2), the patient was transferred to our hospital for further management. Additional serologies, including aquaporin 4 IgG, myelin oligodendrocyte glycoprotein IgG, Rho/La antibodies, and West Nile IgM and IgG antibodies, among others, were negative. A coagulation panel was normal. Digital subtraction angiography (DSA) obtained to assess a possible vascular myelopathy documented the cervical spinal cord supply, including the superior and inferior arteries of the cervical enlargement. The latter artery arose from the right costocervical trunk and reached the spinal cord by crossing the C6–C7 neural foramen. It supplied a portion of the spinal cord showing marked hyperemia and rapid venous return consistent with subacute ischemia and matching the lesion distribution documented by MRI (Figure 1(B)–(E)). The rest of the study, including both vertebral and carotid arteries, was normal.
A review of the MRI obtained at presentation disclosed a previously unappreciated foraminal disc protrusion (3 × 3 mm) at the right C6–C7 level, corresponding to the foraminal transit of the inferior artery of cervical enlargement (Figure 1(F)). These congruent findings identified acute disc herniation with vascular impingement as the ischemic event etiology.
Case 2
A 40-year-old man with no significant medical history developed acute triparesis after participating in a martial arts class. Early in the session, he experienced unusual soreness and fatigue in the left triceps region, but the symptoms resolved, and he could continue with the class. However, 2 hours later, he noticed similar symptoms affecting the right triceps region, followed by acute interscapular pain radiating to both shoulders. Within minutes, he developed bilateral hand and right lower extremity weakness. At the time of admission to a local hospital, he also complained of band-like thoracic paresthesia and acute urinary retention. Brain MRI was unremarkable. A spine MRI showed signal abnormality in the central cervicothoracic spinal cord. Head and neck CTA were negative. He received a dose of intravenous immunoglobulin for suspected acute inflammatory polyneuropathy or acute idiopathic transverse myelitis and was transferred to our institution for further management.
Upon arrival, his neurological exam was consistent with a central cord syndrome affecting both hands and the right leg, with preserved strength in the left leg, a right Babinski sign, and absent thermoalgesic sensation in the left leg. A new spine MRI confirmed a central cord signal abnormality extending between the C6 and T1 vertebral levels, with restricted diffusion confirming an ischemic etiology (Figure 2(A)).
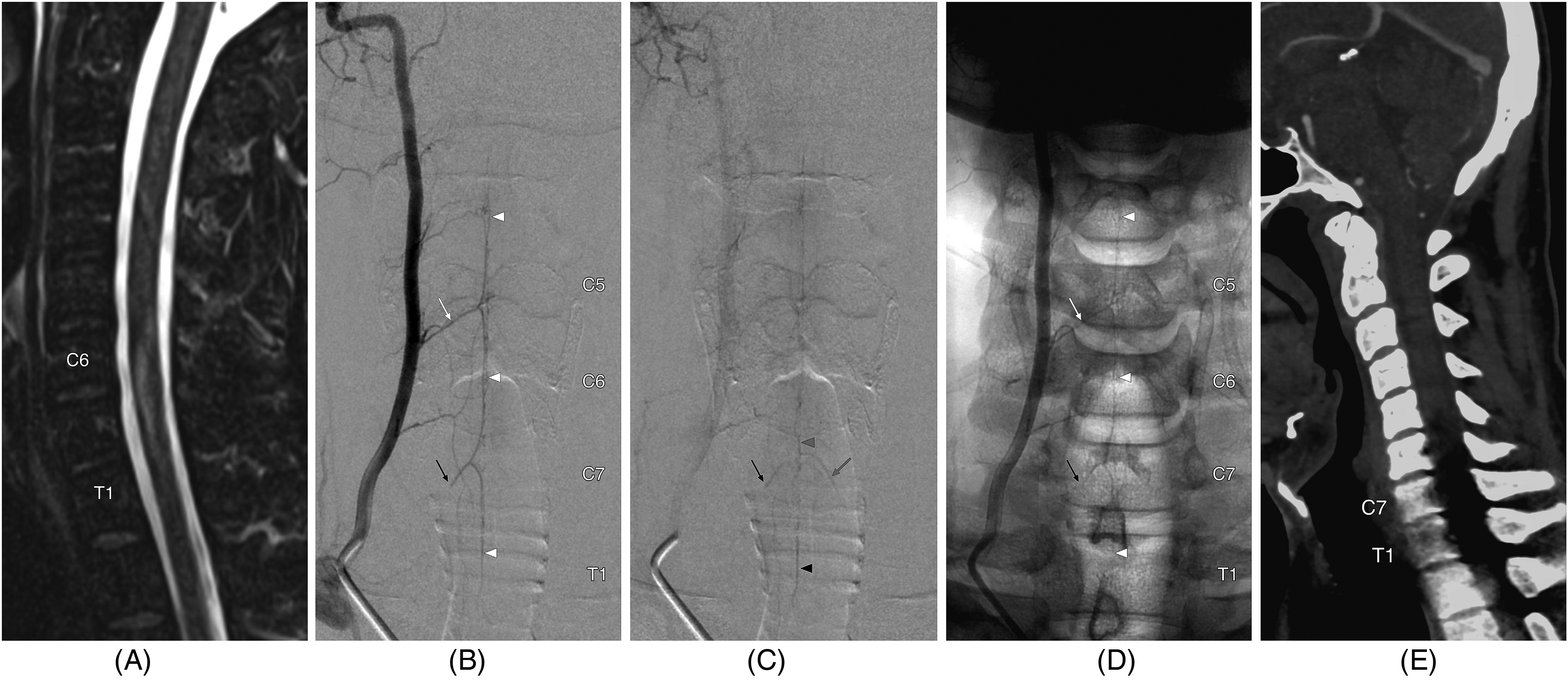
A 40-year-old man with an acute cervical spinal cord syndrome during a martial arts class. (A) MRI, sagittal T2-weighted image, showing abnormal cord signal from C6 to T1. (B) DSA, right vertebral artery, posteroanterior projection, arterial phase. The superior artery of the cervical enlargement (white arrow) arises from the right vertebral artery and passes through the right C5–C6 neural foramen to supply the anterior spinal artery (white arrowheads). Opacified blood flows retrogradely from the latter to opacify the distal portion of the inferior artery of the cervical enlargement, which is abruptly interrupted at the level of the C7–T1 neural foramen (black arrow). (C) DSA, right vertebral artery, posteroanterior projection, late arterial phase. There is early opacification of a portion of the anterior-median spinal vein (gray arrowhead) and a left C87–T1 radiculomedullary vein (gray arrow) and contrast stagnation in the inferior artery of the cervical enlargement (black arrow) and a portion of the anterior spinal artery at C7–T1 (black arrowhead). (D) DSA, right vertebral artery, posteroanterior projection, nonsubtracted arterial phase. This image shows vascular and osseous topographic landmarks (same legend as Figure 2B). Note the interruption of the inferior artery of the cervical enlargement near the right C7 pedicle, where it would normally emerge from the C7–T1 neural foramen. (E) CTA, midsagittal reconstruction image. This CTA, obtained shortly after symptoms onset, shows that the severe artifacts typically affecting the cervicothoracic junction (C7–T1) prevent a valuable analysis of the spinal cord and its blood supply. CTA: computed tomography angiography; DSA: digital subtraction angiography; MRI: magnetic resonance imaging.
An extensive laboratory workup was unremarkable, including lyme serologies, B12 level, and antineutrophil cytoplasmic antibodies. Similar laboratory evaluation for coagulopathy, including antiphospholipid antibodies and homocysteine levels, was unremarkable. DSA documented the cervical spinal cord supply, including the superior artery of the cervical enlargement at the right C5–C6 level. The inferior artery of the cervical enlargement, opacified retrogradely, showed an abrupt interruption at the level of the C7–T1 neural foramen (Figure 2(B)). An area of marked hyperemia and rapid venous return matching the lesion documented by MRI was consistent with subacute ischemia (Figure 2(C) and (D)). The rest of the study, including both vertebral and carotid arteries, was normal. Traumatic injury affecting the proximal segment of the inferior artery of the cervical enlargement was identified as the ischemic event etiology.
Case 3
A 5-year-old boy with normal development and no medical history fell approximately 9 steps, falling on his bottom and sliding down the steps on his back. He did not hit his head and was immediately able to get up and walk back up the stairs without assistance. After 30 minutes, he began to experience weakness and numbness in his arms and legs, first on the right side and then progressing to the left. His symptoms reached nadir over approximately 1 hour. He also complained of pain in the center of his back and acute urinary retention. After head and spine CT at a local emergency department demonstrated no traumatic injuries, he was transferred to a pediatric trauma center for suspicion of SCIWORA.
Neurological evaluation revealed loss of temperature sensation with relative preservation of proprioception in the bilateral upper and lower extremities and quadriparesis affecting the leg more than the arm and the right side more than the left, consistent with an incomplete anterior cord syndrome. Spine MRI demonstrated diffusion restriction and T2 hyperintensity from C5 through T3 consistent with an acute infarction. There was also STIR hyperintensity and fragmented appearance of the C6–C7 disc, suggesting traumatic injury without cord compression (Figure 3(A)). Diffusion-weighted imaging was positive (Figure 3(B)). DSA identified the inferior artery of cervical enlargement arising from the right costocervical trunk, providing both a dominant anterior radiculomedullary branch and a small posterior radiculomedullary branch with a focal irregularity and stenosis of the anterior radiculomedullary artery, suggesting an arterial dissection past the right C6–C7 neural foramen, in the vicinity of the herniated disc (Figure 3(C) and (D)). DSA also documented a cord blush with early venous drainage, indicating an area of luxury perfusion corresponding to the infarct identified by MRI.
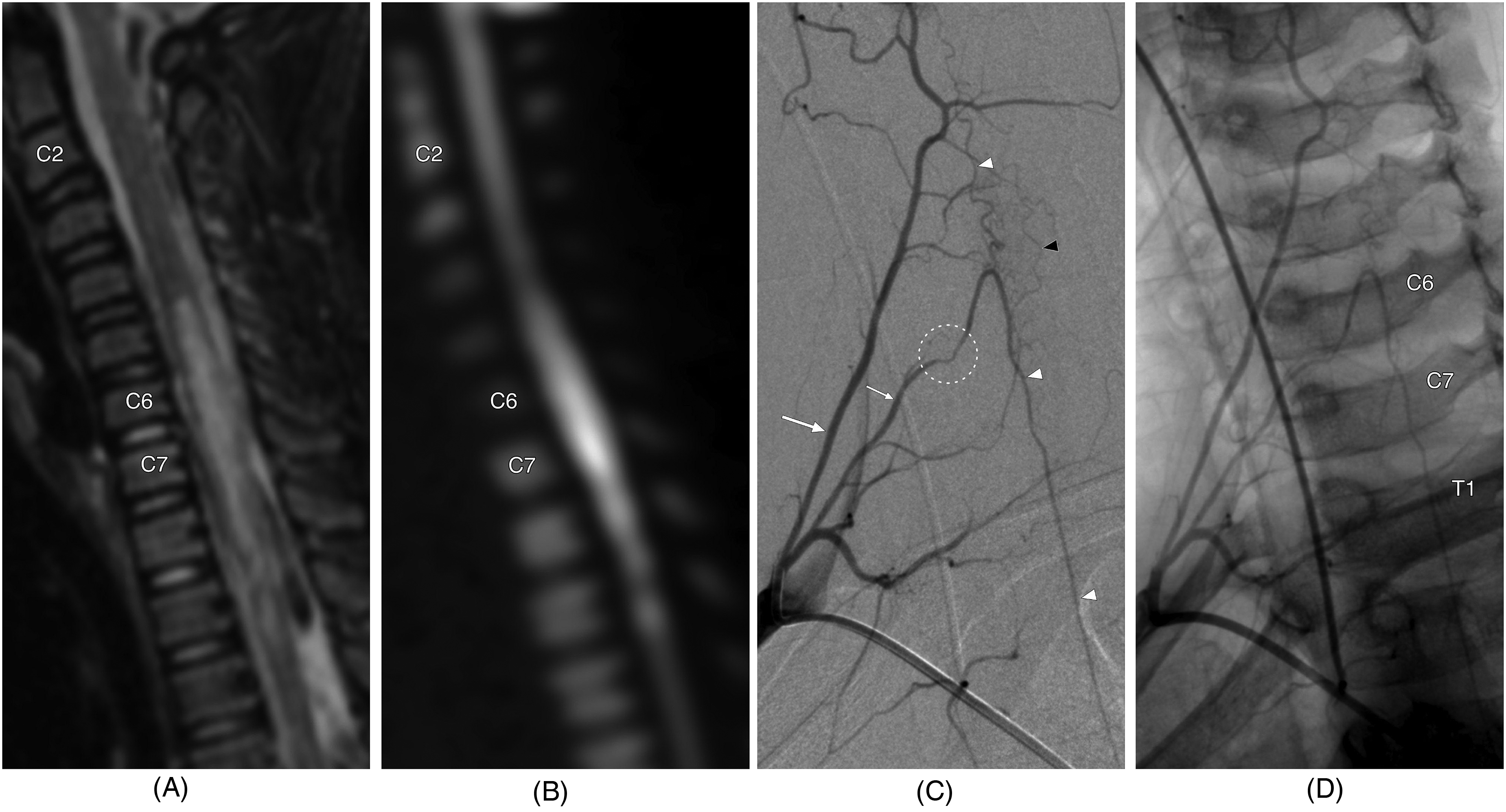
A 5-year-old boy with an acute cervical spinal cord syndrome after a fall. (A) MRI, sagittal STIR image, showing abnormal cord signal from C5 to T3 and a fragmented appearance of the C6–C7 intervertebral disc with posterior protrusion. (B) MRI, sagittal diffusion-weighted image, suggesting the ischemic nature of the lesion. (C) DSA, right costocervical trunk injection, right anterior oblique projection, arterial phase, showing a focal irregularity with stenosis (circled) of the inferior artery of the cervical enlargement (small white arrow) past the right C6–C7 neural foramen. The large white arrow indicates the deep cervical artery, the white arrowheads the anterior spinal artery, and the black arrowhead the right posterolateral spinal artery. (D) DSA, right costocervical trunk injection, nonsubtracted right anterior oblique projection, arterial phase, demonstrating the cervical spine anatomy and confirming the topography of the lesion at C6–C7. DSA: digital subtraction angiography; MRI: magnetic resonance imaging; STIR: short tau inversion recovery.
Discussion
Arterial supply of the cervical spinal cord
The cervical spinal cord has three sources of vascularization:
2
The anterior vertebrospinal trunks arise from the terminal segment of the vertebral artery at C1 and supply the uppermost cervical cord (down to C3). The main trunk typically originates from the nondominant vertebral artery; less often, there is a robust trunk on each side. The superior artery of the cervical enlargement arises from the vertebral artery between C3 and C5. It supplies most of the cervical spinal cord (C3–C6). The inferior artery of the cervical enlargement originates from the supreme intercostal artery between C7 and T2. It supplies the lowermost cervical and upper thoracic spinal cord (C7–T2).
As variants, the superior and inferior arteries of the cervical enlargement may both arise from a vertebral or subclavian artery. There may also be more than one superior or inferior branch. The longitudinal delimitation of each supply territory can shift depending on the relative size and number of participating arteries, for example, a dominant superior artery of the cervical enlargement may extend its territory both cranially and caudally, while a robust vertebrospinal trunk can, in rare instances, take over most of the cervical cord supply. However, it is essential to remember that the superior, middle, and inferior portions of the cervical cord most often have different sources of supply. In our two cases, for example, the notion that the lower cervical and upper thoracic cord were vascularized by subclavian branches (via the supreme intercostal artery) was critical for accurate diagnosis.
Imaging of cervical arterial injuries
An acute ischemic lesion involving the cervical spinal cord in a traumatic context is generally assumed to result from a vertebral artery injury. Because this assumption is often correct, a cervical CTA should be obtained as soon as possible to document the morphology and patency of the vertebral arteries. DSA may be performed to further evaluate patients with negative CTAs or better characterize a detected anomaly (e.g. an arterial dissection or an arteriovenous fistula). In our experience, DSA can confirm the diagnosis of traumatic vascular injury by identifying subtle anomalies unnoticed on CTA because of the technique's limitations in spatial and temporal resolutions (Figure 2(E)). These technical shortcomings also prevent CTA from assisting with diagnosing cervical ischemia when the involved vessels are smaller than the vertebral arteries, such as the small radiculomedullary arteries of supreme intercostal artery origin shown in our two observations.
Conclusions
DSA is a valuable adjunct to CTA for the diagnosis of vascular anomalies leading to cervical spinal cord stroke. In particular, DSA is the only diagnostic method that can reliably detect injuries affecting the small subclavian branches that typically supply the lower cervical and upper thoracic spinal cord.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.