
Abstract
Pediatric arteriovenous shunts can be challenging to embolize and the consequences of excess venous penetration disastrous. Moreover, the congenital nature of most shunts necessitates neonatal intervention whenever (medically refractory) heart failure occurs. Here, we describe current endovascular treatment strategies based on personal experience and literature review. While disparate, arteriovenous malformation, dural arteriovenous fistula (AVF), pial AVF, and vein of Galen aneurysmal malformation share unifying features such as high output heart failure and venous hypertension. This tutorial is divided into passages on Goals, Access, and Treatment which respect differences among pediatric arteriovenous shunts while maintaining a narrative economy.
Introduction
Arteriovenous shunts (AVS) can be challenging to embolize and the consequences of excess venous penetration disastrous. Moreover, the congenital nature of most shunts necessitates neonatal intervention whenever (medically refractory) heart failure occurs. 1 Here, we describe current strategies based on personal experience and literature review. Embolization beyond the neonatal stage aims to prevent hemorrhage and hydrovenous disorder (HVD), although these, unfortunately, serve as the initial presentation in many cases.
Heart failure presenting in the newborn period tends to be severe and refractory to medical treatment. The pathophysiology begins in the fetal first trimester due to a lack of complete capillary formation between the cerebral arteries and veins. The resulting high flow/low resistance AVS increases the rate of blood circulation through the brain, lungs, and heart. Large shunts that overwhelm the heart's compensatory mechanisms lead to pulmonary congestion/hypertension and end-organ ischemia due to cerebral steal from the remaining systemic circuit. Pruning this “circuit” by AVS embolization brings the system closer to equilibrium.
Cortical venous pressure normally measures approximately 10–15 mm Hg.2–4 Venous hypertension impairs drainage of the subtending neurovascular unit or even the whole cerebrum in large, uncompensated AVSs. In addition to expected sequelae such as hemorrhage, CSF resorption also decreases along the ventricular-venous gradient. Recent characterization of this so-called glymphatic system 5 bolsters pioneering work from decades prior.6,7 Together, congestion of both veins and CSF creates an unvirtuous cycle leading to hydrocephalus, epilepsy, and atrophy. Simply placing a ventricular shunt provides no benefit, and actually worsens the situation by encouraging more flow through the AVS. 8
High output heart failure 9 and venous hypertension 10 represent unifying features of these otherwise disparate shunts. Subsequent passages on Goals, Access, and Treatment respect differences among arteriovenous malformation (AVM), dural arteriovenous fistula (AVF), pial AVF, and vein of Galen aneurysmal malformation (VOGM) while maintaining narrative economy when feasible.
Goals
Complete occlusion of pediatric AVS is rarely practical (or desired) in a single embolization. Neonates simply cannot tolerate hours-long procedures: the sheath is often occlusive, the core temperature fluctuates, drip lines impair fluid/electrolyte balance, and iodinated contrast accumulates. Even when possible, rapid AVS occlusion predisposes to edema and hemorrhage, especially when it extends to the draining vein(s). Staged treatment should nevertheless be tailored to the clinical indication. For CHF and HVD, that means occluding the highest flow (i.e. largest) pedicles first.
Neonatal embolizations are performed every few days until the clinical presentation is not severe—this includes the baby being able to feed/gain weight and discharge home, while still on supportive medical therapy for heart failure and pulmonary hypertension. Close follow-up with pediatric cardiology is mandatory. Pulmonary hypertension can be reversed up to 6 months of life, allowing further sessions to be delayed until the child is ≥5 kg. The decision to withhold care is less algorithmic, involving a candid discussion with the family and all interested physicians. Lasjaunias et al. 11 created a score that seeks to predict the likelihood of response to treatment, and Bicetre < 8, predicts a high risk of permanent cognitive impairment and peri-procedural mortality.
Hemorrhagic lesions often bleed from a high-risk feature such as nidal aneurysm/fistula (AVM), venous varix (pAVF), or cortical venous reflux (dAVF). These likewise serve as “priority targets” for embolization, in order to prevent further bleeding in the near term. Complete occlusion is eventually required to eliminate lifetime AVS morbidity. Endovascular means are sufficient in some shunts but must complement surgery or radiation in others. Finally, those that share draining veins with functional tissue represent an especially high-risk category12,13 and may not warrant occlusion at all. 14
Access
Few if any devices were designed with pediatrics in mind, making the sizes and lengths almost comically large. Increased radial access in adults has led to smaller OD sheaths (e.g. Prelude Ideal, Merit Medical, South Jordan UT). Forthcoming smaller diameter “MMA” intermediate catheters (e.g. Socrates 127 cm/0.038″, Scientia, West Valley UT; Sofia 0.044″, Microvention, Aliso Viejo CA) may likewise serve as a welcome update. Currently, a 4 Fr Prelude will stretch to accommodate DAC 044 (Concentric/Stryker, Salt Lake City UT), which can be inserted using a makeshift introducer cut from a less expensive 5 Fr sheath (Figure 1). This sheath/intermediate combination suffices for most pediatric interventions. Reaching the horizontal petrous or V4 segment is crucial, however, given the distal softness of the intermediate and tortuosity associated with most AVS. Tracking over an angled Glidewire (Terumo, Somerset, NJ) may prove difficult and risks dissection, so we routinely opt for an 027″ microcatheter (MC) and Aristotle 24 Soft wire (Scientia, West Valley UT). Having reached a satisfactory position, the DAC must be secured to drapes with a Tegaderm or it will slide back out. Wouldn’t it be nice to create a sheath whose check-flow could be exchanged for a rotating hemostatic valve?
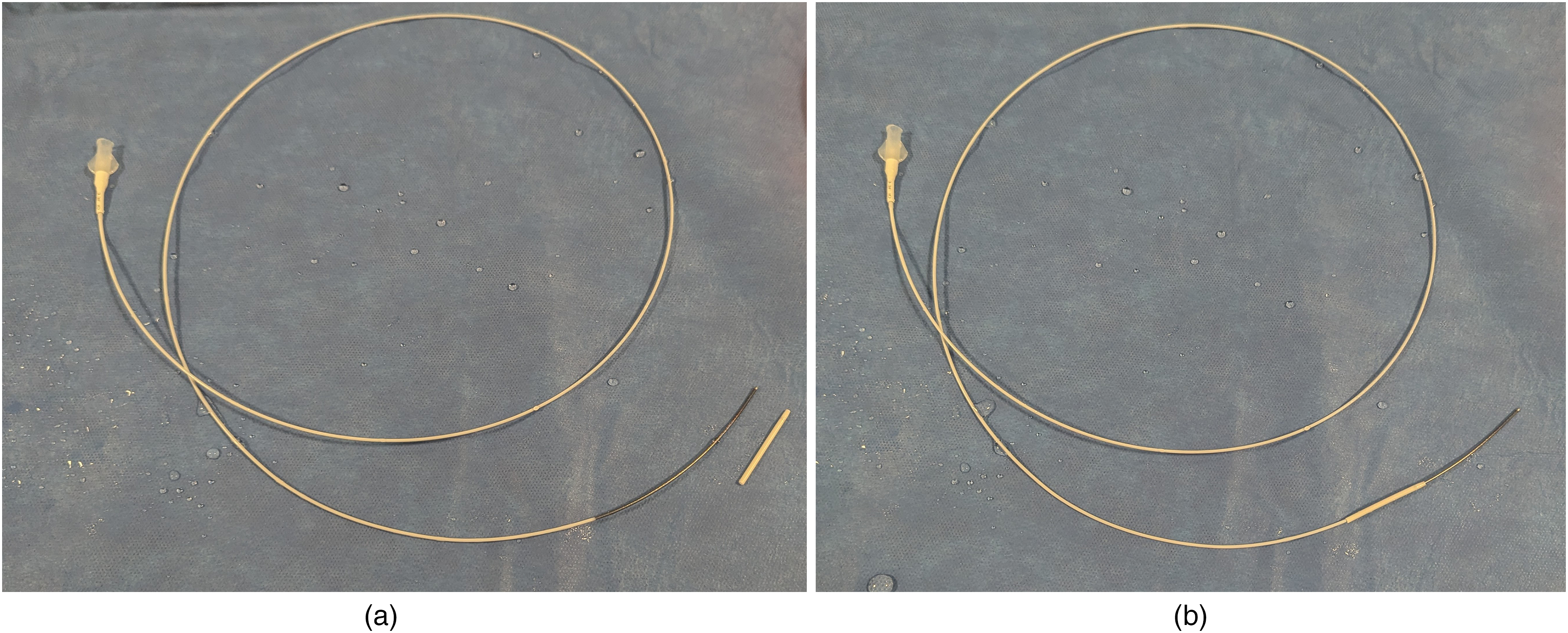
DAC 044 with adjacent (a) and loaded (b) “introducer” cut from an inexpensive 5 Fr sheath. The catheter and introducer should be thoroughly hydrated prior to insertion into the indwelling 4 Fr sheath. Once the soft portion of the DAC has traversed the sheath, the introducer can be slid proximally to its hub.
Optimal working views may not be intuitive, such as when preexisting embolics obscure the vasculature. Many situations thus benefit from first performing a hand-injection 3DRA and determining C-arm angles at the workstation. A high-quality angiogram (≥ 75% contrast, ≥ 4 frames/second, geometric magnification, and ventilation paused) with the intermediate catheter tip at the bottom of the screen allows one to re-roadmap throughout the case. This strategy limits radiation and contrast dose. Once a MC is inserted, injecting through the intermediate becomes difficult and yields poor-quality angiograms. MC runs themselves are quite useless aside from confirming tip position immediately prior to embolization. MCs may even recoil out of position if injected too forcefully or damage fragile vasculature if their position is other than expected.
Although shorter than adults, one usually encounters more twists and turns navigating pediatric AVS given their distal location and high-flow remodeling effects. As torque translation diminishes, flow-directed techniques gain increasing utility. Magic (Balt, Montmorency, FR) exemplifies this tact but is only compatible with n-BCA glue. Less flexible MCs (Marathon and Apollo, Medtronic, Minneapolis MN) offer the versatility of EVOH and smaller profile coils (≤ 6 mm Barricade, Balt, Montmorency, Fr)—if they reach a suitable position. Flow direction can be enhanced by extending a coil from its tip, so long as the stiff pusher segment is not exposed, and advancing MC and “wire” as a unit 15 (Figure 2).
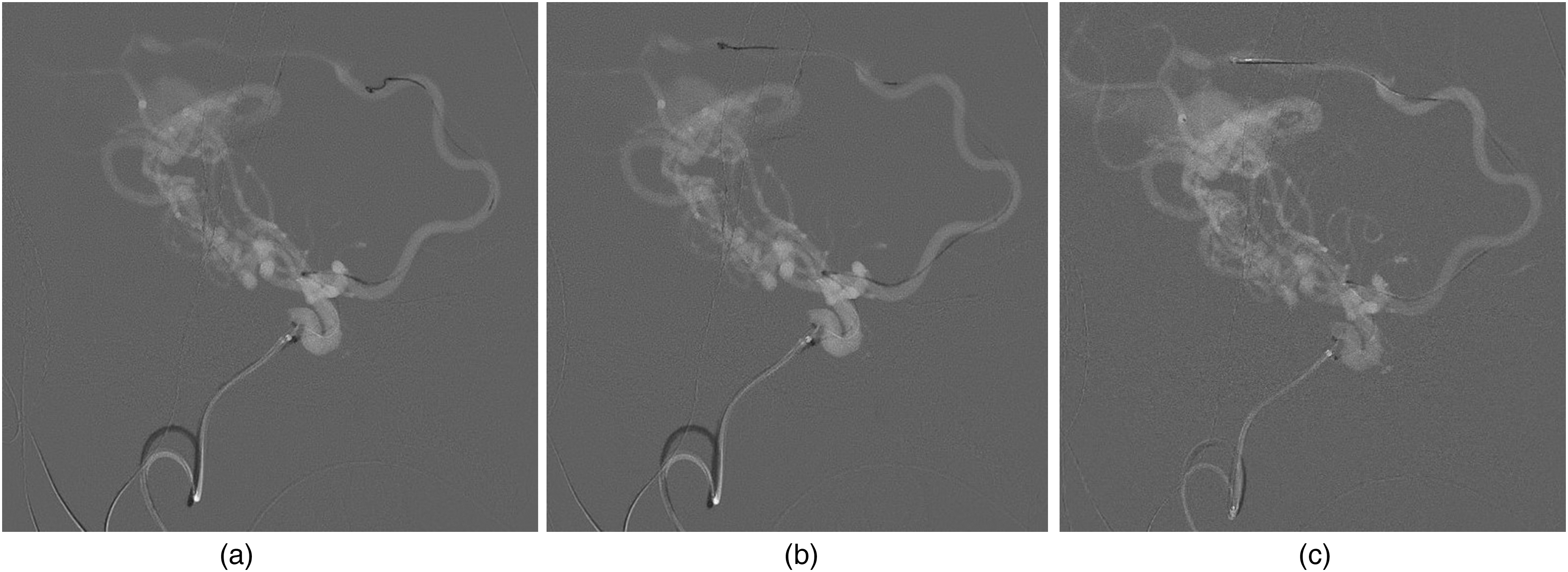
Navigating tortuosity using a “coil wire” technique. An hypertrophied ACA feeder to the prosencephalic vein proved difficult to traverse as the wire selected numerous side-branches and had lost all torque-ability. A 2 mm x 4 cm Barricade coil was advanced out the Marathon and allowed to elongate with the current of flowing blood. The RHV was cinched and the entire system advanced as a unit (a, b) until it reached a position abutting the fistulous point (c).
Trans-venous access represents the antithesis of a flow-directed approach and differs from the arteries in many other respects. Proximal (jugular) venotomies may be desirable once the neck has sufficiently developed so that inadvertently retained MCs may simply be cut at the skin. Access veins are much larger and so 5 Fr or even 6 Fr sheaths enable a wider range of guide catheters. Preludes still excel due to minimal sheath/dilator step-off, promoting entry into the awkwardly positioned neck. Large (035″–024″) wires facilitate retrograde navigation through the capacious dural sinuses, which may deflect less supportive devices. Intermediate catheters advanced over smaller microsystems also tend to engage on ledges such as the transverse/sigmoid junction. Rarely, a proboscis-shaped insert (Wedge, Microvention, Aliso Viejo CA) is needed to free them. Acute angulations such as the falcine sinus in VOGM favor pre-formed (e.g. Cobra-2) or steam-shaped guide/intermediate catheters. Extreme care must be taken when navigating thin-walled and delicate cortical draining veins, which are pressurized by the AVS. 16
Treatment
Satisfactory embolization straddles the arteriovenous shunt, whereas undesired effects occur with occlusion proximal or distal to this. Proximal occlusion incites neo-angiogenesis, eventually replacing the targeted pedicle with numerous small vessels that prove difficult or impossible to treat. The untoward effects of excess venous penetration are typically more acute: intracerebral hemorrhage and pulmonary embolism. Many techniques address this dilemma between occluding too close or too far, and the “right” one(s) depends on each case, the operator's experience, and his ancillary support.
By applying the Access strategies described above, we almost always reach the fistulous point. Achieving precise embolic deposition involves consideration of vessel diameter, flow rate, and linearity. All three correlate with distal penetration and require increasingly potent flow control maneuvers. Dural fistulas and plexiform AVM occupy one end of the spectrum, as an appropriate liquid embolic freely polymerizes within their narrow and tortuous feeders. Reflux poses a more pertinent problem. n-BCA concentration can be adjusted in light of the angiogram, whereas for EvOH we prefer the traditional “plug and push” technique. While balloon MCs have improved, trackability remains inferior and often leads to suboptimal (proximal) positioning. EvOH may also seep between the inflated balloon and vessel wall, encouraging over-inflation and potentially vessel rupture.
Direct AV fistulae such as mural VOGM and pAVF occupy the opposite extreme. 17 A coil (e.g. Optiblock, Balt, and Montmorency FR) “basket” can be made of the varix in many pAVFs. Adding coils ± n-BCA will obliterate these simple shunts in an immediate or staged fashion, depending on the indication. More complex AVS architectures do not tolerate a vein-first approach. If the arterial side of the fistulous point can be reached with an 017″ MC, and it allows a coil (e.g. Optiblock, Balt, and Montmorency FR) to achieve a stable position, the same approach may be employed. Otherwise, rapid ventricular pacing (RVP) has proven highly effective at transiently reducing cardiac output in toddlers and older children.18–20 Neonates’ nominal resting heart rate of 120–160 bpm increases to ∼ 200 in the presence of AVS, hindering effective RVP as rates > 300 risk cardiac ischemia and arrhythmia.
RVP requires collaboration with a cardiologist adept at catheterizing the right ventricle and placing a myocardial electrode. Heart rate is modulated between 240 and 280 bpm until end-tidal CO2 decreases by 25%–40%. At this point, profound hypotension enables controlled deposition of n-BCA near the fistulous point over 40–60 seconds’ working time. Cardiac output rapidly normalizes once pacing ceases, so the cast must appose the vessel walls and harden beforehand. Torrential shunts still require ≥ 80% glue (0.25 oil: 1 n-BCA). Reflux indicates the lumen has been filled, and injections should continue until this goal is met. If necessary, a detachable tip MC may be used to prevent “gluing” the tip in situ, for example, Apollo or Sonic (Balt, Montmorency FR). 21
In lieu of RVP, some advocate a “kissing” approach to facilitate occlusion at the fistulous point by accessing both sides of the AVS. 22 The venous-side catheter reaches the artery in a retrograde fashion and deploys a coil basket; subsequently, the arterial-side catheter injects liquid embolic (Figure 3). We recently adopted a simpler approach whereby an 017″ MC traverses the fistula from vein to artery and detaches Optiblock and/or 0.018″ framing coils into the pedicle for flow reduction. Modest pharmacologic hypotension is then sufficient to infuse the basket with concentrated n-BCA from the same catheter. The glue cast will initially reflux before it expands to oppose the vessel walls, in reverse order to trans-arterial embolization. Once apposition is achieved, one may rapidly retract the catheter (Figure 4).
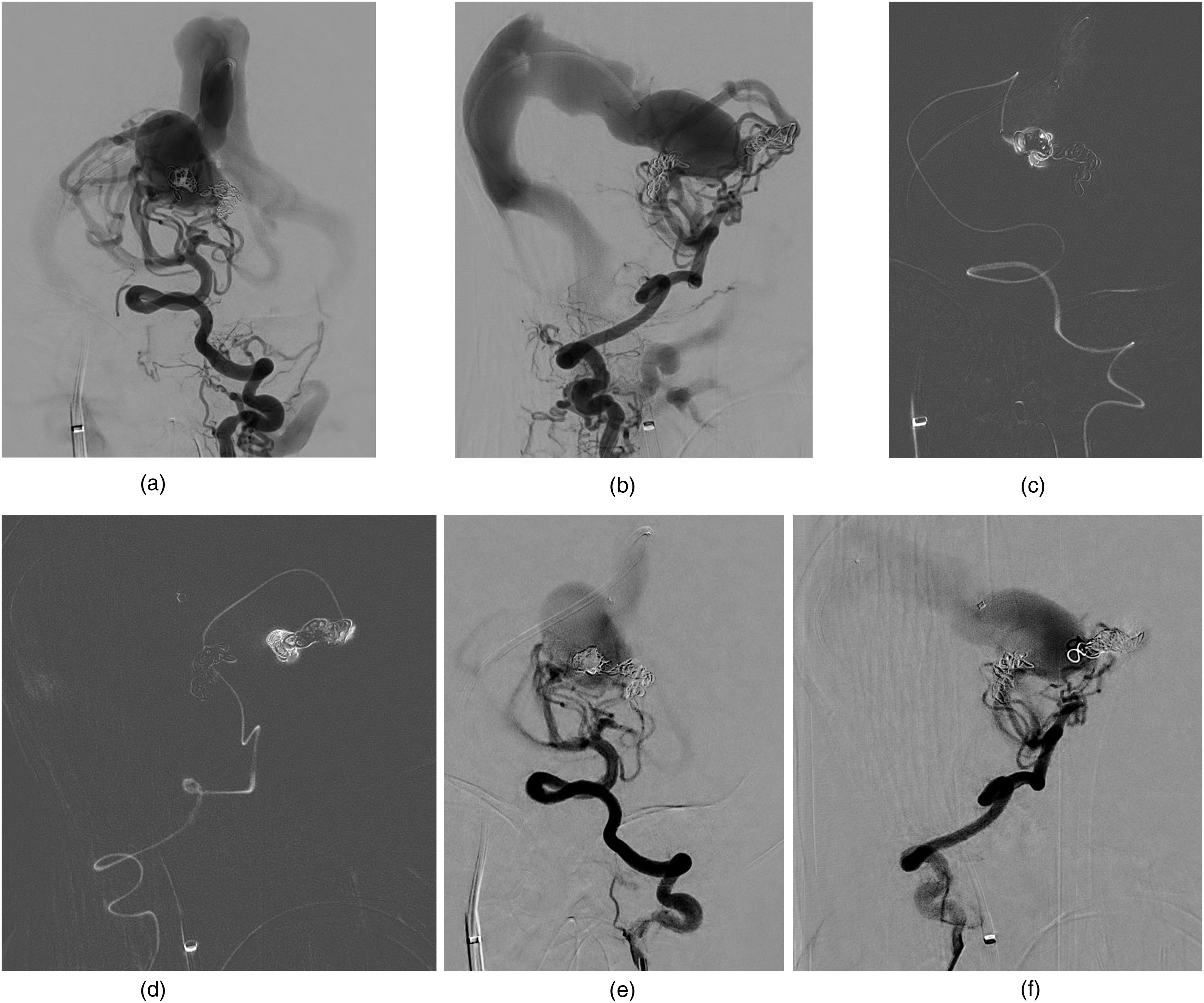
“Kissing” technique involving both arterial and venous access to the fistulous point. Mural type VOGM in AP (a) and Lateral (b) views following trans-venous coil placement into a feeder at the midline/anterior aspect of the prosencephalic vein. Trans-arterial approach to the same feeder via the left vertebral artery is used to subsequently inject n-BCA (c, d) into the coil basket. Post-embolization angiogram demonstrates occlusion of this shunt (e, f).
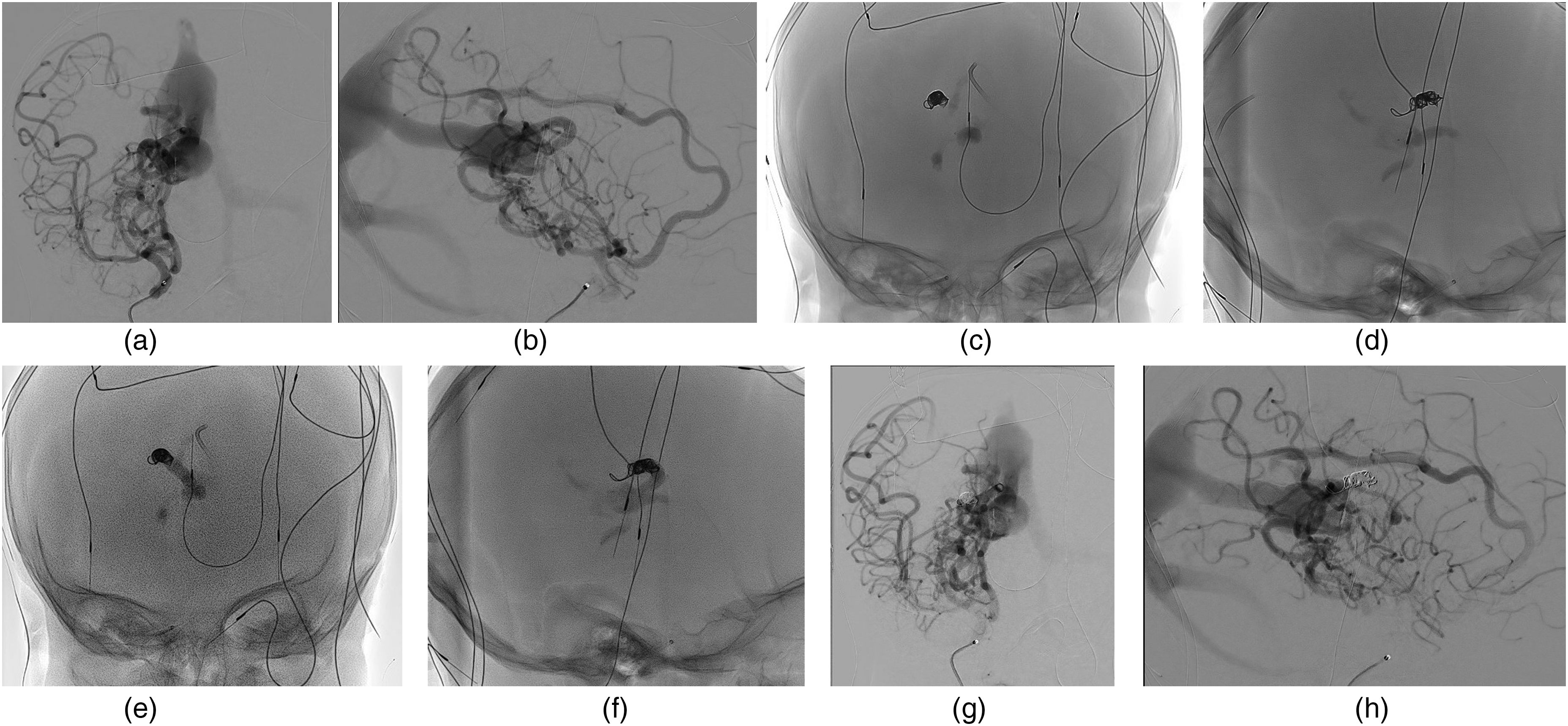
Trans-venous only “kissing the wind” technique in a mural VOGM. Right ICA angiogram demonstrates a large pedicle entering the right/anterior aspect of the venous sac (a, b). Following transvenous access to the pedicle, a coil basket is formed (c, d). Concentrated (>80%) n-BCA is then infused through the same MC, initially refluxing to occlude the fistulous point before hardening and expanding to fill the vessel (e, f). One removes the MC once all steps are accomplished. Post-embolization angiogram (g, h) demonstrates occlusion of the feeder.
Large fistulae approximate the main pulmonary arteries in caliber and casts may embolize there if dislodged from the AVS (heed preceding advice to avoid this). Such plugs require surgical embolectomy as they far outsize the access sheath, let alone any thrombectomy devices inserted therein. Attention should instead be focused on determining the patency of the left main stem bronchus. CHF dilates the left atrium, which in turn compresses (and may obstruct) this bronchus. As pulmonary blood flow shadows ventilation, an embolus often occludes the right PA. ET tube repositioning into the left main stem bronchus restores ventilation to the left lung. Single lung function may support sternotomy/embolectomy without emergent ECMO.
Footnotes
Authors’ note
Jesse Jones is a consultant for Cerenovus, Scientia, TG Medical, MIVI, and Protara.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.