
Abstract
Background
The volume of mechanical thrombectomy (MT) performed at hospitals is used as one of the criteria for advanced-level designation for stroke care.
Objective
Our study sought to determine the relationship between annual MT procedural volume and in-hospital outcomes in acute ischemic stroke patients undergoing MT in the United States.
Methods
We analyzed the National Inpatient Sample from 2016 to 2020. The hospitals were grouped into quartiles based on the volume of MT procedures performed within the calendar year. We compared the rates of routine discharge/home health care; in-hospital mortality, and post-treatment intracranial hemorrhage (ICH) between the quartiles after adjusting for potential confounders.
Results
Patients undergoing MT ranged from 15,395 in quartile 1 to 78,510 MT in quartile 4. There were lower rates of discharge home/self-care of 22.5%, 20.8%, and 20.8% for quartiles 2, 3, and 4, respectively, compared with 34.9% in quartile 1. The odds of ICH increased to 1.81 (p < 0.001), 1.84 (p < 0.001), and 1.98 (p < 0.001) among the quartiles from lowest to highest procedural volumes. The odds of home discharge/self-care decreased to 0.66 (p < 0.001), 0.60 (p < 0.001), and 0.63 (p < 0.001) among the quartiles from lowest to highest procedural volumes. The odds of in-hospital mortality increased to 1.92 (p < 0.001), 1.99 (p < 0.001), and 1.84 (p < 0.001) among the quartiles from lowest to highest procedural volumes.
Conclusions
We observed a paradoxical relationship between adverse outcomes and the annual procedural volume of MT at the hospital presumably due to the higher severity of acute ischemic stroke treated at high-volume hospitals.
Introduction
Procedural volume for mechanical thrombectomy (MT) in acute ischemic stroke patients at individual hospitals has been used as a criterion for physician proficiency, certification of training programs, participation in clinical trials, and certification for Comprehensive Stroke Center and Thrombectomy-Capable Stroke Center.1–5 Both the Comprehensive Stroke Center and Thrombectomy-Capable Stroke Center are required to perform 15 MTs over the past 12 months (or 30 over the past 24 months). 6 Training programs require at least 30–50 MTs for acute ischemic stroke for trainees in neuro-interventional training programs.7,8 Analysis of data in registries has demonstrated an increase in rates of functional independence or in rates of surrogate markers for functional independence in hospitals with higher procedural volume for mechanical thrombectomy.9–16 However, the high rates of functional independence reported in acute ischemic stroke patients undergoing MT at low-volume centers ( < 15 procedures per year) in recent studies warrant a careful assessment of the relationship between hospitals procedural volume and outcomes.17–21
In this study, we sought to determine the relationship between a hospital's procedural volume and in-hospital outcomes in acute ischemic stroke patients undergoing MT in the United States.
Material and methods
This article was prepared in accordance with the recommendations of the STROBE criteria. 22
Data acquisition
The analysis was performed using the data from the Nationwide Inpatient Sample (NIS) from 2016 to 2020. The NIS is the largest all-payer inpatient care database in the United States compiled by the Healthcare Cost and Utilization Project (HCUP) at the Agency for Healthcare Research and Quality (AHRQ).23–29 The NIS provides a national estimate for hospital admissions data based on approximately a 20% stratified sample of United States hospitals, which translates into 5 to 8 million hospital stays from ∼ 1000 hospitals. The dataset includes more than 100 clinical and nonclinical variables associated with hospital stays, including primary and secondary diagnoses, primary, and secondary procedures, the patient's admission and discharge status, patient demographic information (e.g. sex, age, race/ethnicity, expected payment source, total charges, and length of stay). The data from the NIS can be weighted by the discharge weights to generate national estimates. Detailed information on the design of the NIS is available at http://www.hcup-us.ahrq.gov.26.
Hospital admissions
We used the International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) primary diagnosis code I63 to identify the hospital admissions where patients were diagnosed with acute ischemic stroke. Among these admissions, we included patients who also underwent MT (ICD-10-procedure code 03CG3ZZ, 03CG3Z7, 03CG4ZZ, 03CH3Z7, 03CJ0ZZ, 03CJ3ZZ, 03CK3Z7, 03CK3ZZ, 03CL3Z7, 03CL3ZZ, 03CL0ZZ, 03CP3ZZ, 03CY3ZZ, and 00C73ZZ) in the analysis. The hospital admissions where patients received intravenous (IV) thrombolysis were identified by ICD-10-procedure codes 3E03317 and 3E04317.
Variables of interest
Clinical comorbidity variables for each admission were collected based on the ICD-10 codes or data available in the NIS as defined in Supplemental Table 1. We identified the following neurological deficits using ICD-10-diagnosis codes: aphasia (ICD-9-CM: 784.69, ICD-10-CM: I69.320, I69.920, R47.01), hemiplegia (ICD-9-CM: 342, ICD-10-CM: I69.35, G81), neglect (ICD-9-CM:781.8, ICD-10-CM:R41.4), somnolence, stupor and coma (ICD-9-CM:780.0, ICD-10-CM:R40), dysphagia (ICD-9-CM:787.2, ICD-10-CM:R13.1), and homonymous hemianopsia (ICD-9-CM:368.46, ICD-10-CM:H53.46) as indicators of clinical severity. We also evaluated the proportion of patients admitted to the teaching and non-teaching hospitals, and those admitted to rural hospitals. In the NIS database, the hospital's location and teaching status were obtained from the American Hospital Association Annual Survey of Hospitals. A metropolitan statistical area is considered urban, and a non-metropolitan statistical area is rural. Teaching hospitals have an AMA-approved residency program or have membership in the Council of Teaching Hospitals. The hospital bed sizes were classified in the NIS database into three subgroups (small, medium, or large) based on the location and teaching status of the hospital. Patients undergoing interhospital transfer were identified using the “TRAN_IN” variable. Hospital admission cost was determined by multiplying the total charge by the charge-to-cost ratio.
Outcomes of interest
The main outcome measures for this analysis were based on discharge disposition. Discharge disposition was categorized in the NIS into routine, home health care, short-term hospital, and other facility including intermediate care and skilled nursing home, or death. We assessed two outcomes: routine or home health care (excluding those with palliative care); and in-hospital death. The other endpoint was post-treatment intracranial hemorrhage (ICH), a composite of intracerebral or subarachnoid hemorrhage as identified using ICD-10-CM codes I60, I61, and I62.9 listed as any of the 15 secondary discharge diagnoses in patient records.
Statistical analysis
The hospital admissions with both acute ischemic stroke and 10 or more MT procedures each year were grouped into quartiles based on the annual volume of MT procedures performed within the calendar year. Hospitals where fewer than 10 procedures per year were performed were excluded because such a low procedural volume may have been due to coding errors. The quartiles were defined for each calendar year in the NIS because there was no linkage of hospitals or admissions across different years. We compared patient demographics, clinical characteristics, and post-discharge status between patients who underwent MT in strata based on the hospital's annual procedural volume. We used the Stata 13.0 (College Station, TX) to convert raw counts generated from the NIS database into weighted counts that we used to generate national estimates.
We used the chi-square test for categorical data and two-independent samples t-test to detect any differences in categorical or continuous variables and endpoints, respectively, among hospital strata based on annual MT procedural volume. The second, third, and fourth quartiles were compared with the first quartile (lowest annual MT volume). A logistic regression model was used to identify the association between hospital strata based on annual MT procedural volume and odds of death in all patients. A second logistic regression model was used to identify the association between hospital strata based on annual MT procedural volume and odds of discharge to home/self-care (excluding palliative care). A third logistic regression model was used to identify the association between hospital strata based on annual MT procedural volume and odds of post-treatment ICH. We adjusted for age, sex, race/ethnicity, nicotine dependence, alcohol misuse, weekend admission, season, primary expected payer, income quartile, hospital region, hospital bed size, rural hospital, teaching hospital, obesity, hypertension, hypercholesterolemia, diabetes mellitus, previous myocardial infarction, atrial fibrillation, previous stroke, peripheral vascular disease, chronic kidney disease, liver failure, chronic lung disease, cancer, dementia, atherosclerosis of aorta, and congestive heart failure; and aphasia, hemiplegia, neglect, stupor, dysphagia, and hemianopsia (clinical severity markers).
Results
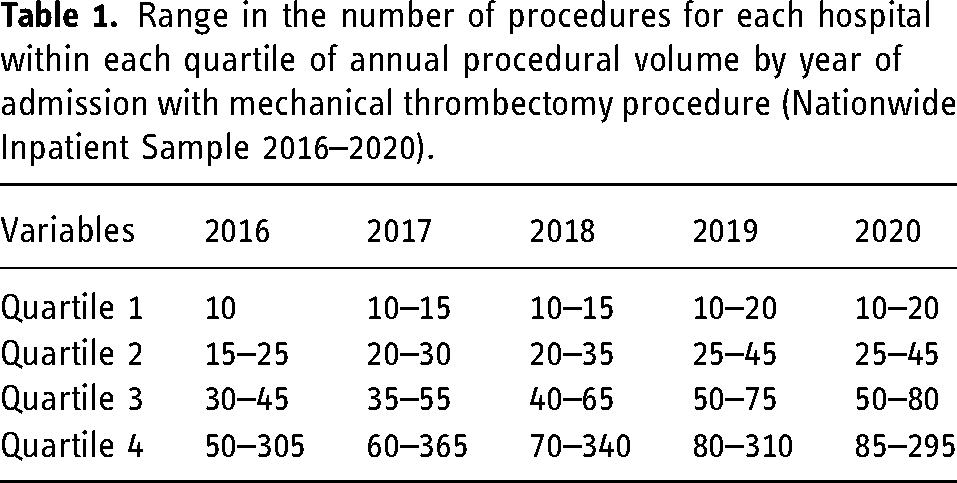
The number of MT procedures per year within each quartile based on the hospital procedure volume is shown in Table 1. There was a modest increase in the range of procedures for quartiles 1, 2, and 3 from 2016 to 2020.
Range in the number of procedures for each hospital within each quartile of annual procedural volume by year of admission with mechanical thrombectomy procedure (Nationwide Inpatient Sample 2016–2020).
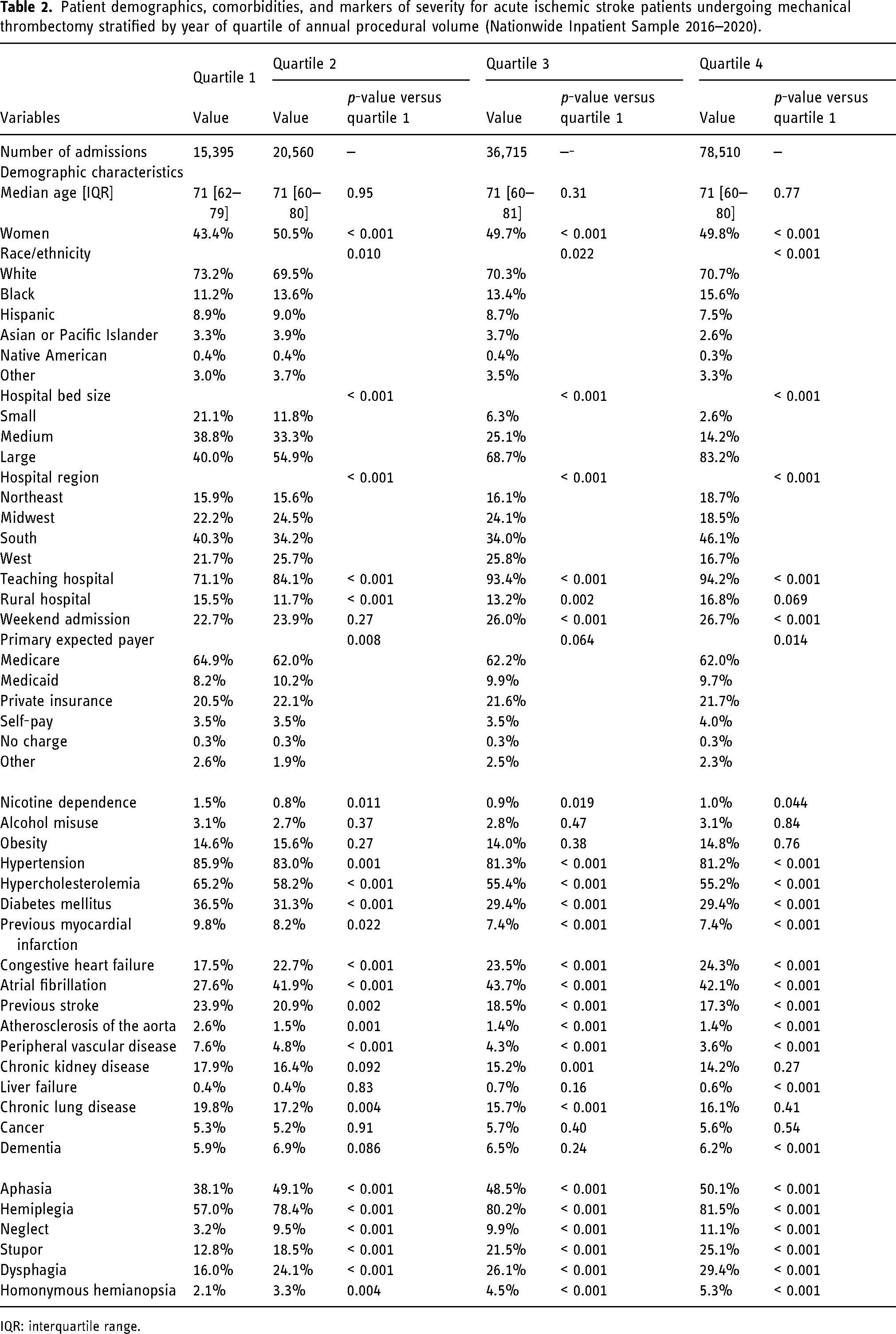
The patient demographics, comorbidities, and markers of severity for acute ischemic stroke patients undergoing MT stratified by quartile year of procedural volume are shown in Table 2. Patients undergoing MT ranged from 15,395 in quartile 1 (lowest annual procedural volume) to 78,510 MT in quartile 4 (highest procedural volume). There was no difference in age across the four quartiles (median age of 71 years). The proportion of women was lower in quartile 1 (43.4%) compared with 2 (50.5%, p < 0.001), 3 (49.7%, p < 0.001), and 4 (49.8%, p < 0.001). With increasing quartile of procedural volume there was a greater proportion of patients who were admitted to large size hospitals (quartile 1 40.0% to quartile 4 83.2%) and teaching hospitals (quartile 1 71.1% to quartile 4 94.2%). An increasing quartile of annual procedural volume was associated with a reduction in the proportion of patients with previous myocardial infarction and chronic kidney disease and an increase in those with congestive heart failure. The proportion of patients with aphasia was 38.1% of patients in quartile 1 and 50.1% of patients in quartile 4. The proportion of patients with hemiplegia was also significantly greater in quartile 4 compared with quartile 1 (81.5% vs. 57.0%, p < 0.001). A similar increase for quartiles 4 and 1 was observed for neglect (11.1% vs. 3.2%, p < 0.001), stupor (25.1% vs. 12.8%, p < 0.001), dysphagia (29.4% vs. 16.0%, p < 0.001) and homonymous hemianopsia (5.3% vs. 2.1%, p < 0.001).
Patient demographics, comorbidities, and markers of severity for acute ischemic stroke patients undergoing mechanical thrombectomy stratified by year of quartile of annual procedural volume (Nationwide Inpatient Sample 2016–2020).
IQR: interquartile range.
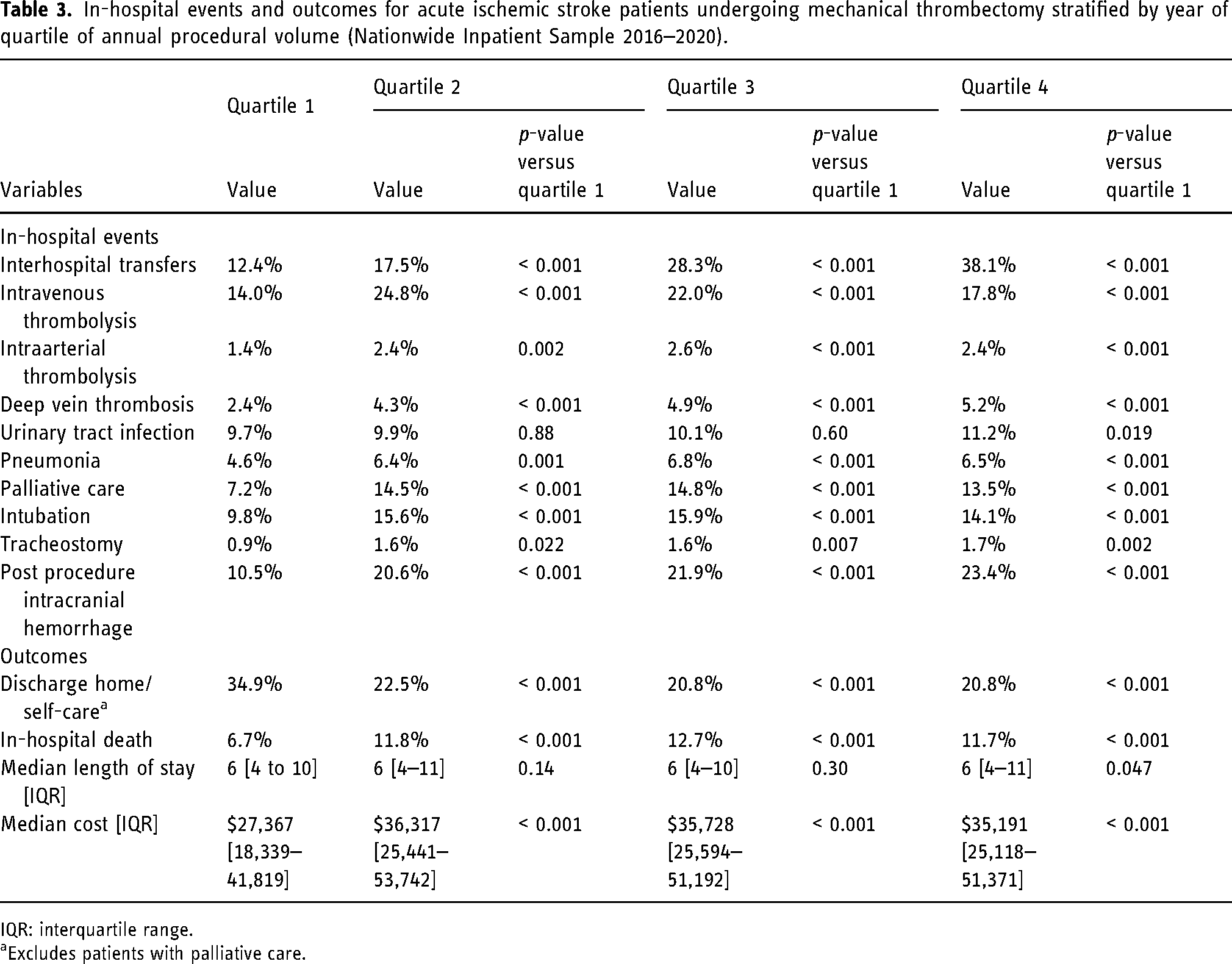
The in-hospital events and outcomes for acute ischemic stroke patients undergoing MT stratified by annual procedural volume are shown in Table 3. The proportion of patients with interhospital transfer was 12.4%, 17.5%, 28.3%, and 38.1%, for quartiles 1, 2, 3, and 4, respectively. Intravenous thrombolysis was most commonly used in quartiles 2 (24.8%) and 3 (22.0%). The proportion of patients with deep vein thrombosis events, urinary tract infections, and post-procedure ICH was higher with increasing quartile of procedural volume. Compared with quartile 1 with a rate of 34.9%, there were significantly lower rates of discharge home/self-care as follows: 22.5%, 20.8%, and 20.8% for quartiles 2, 3, and 4, respectively, (all p-values < 0.001). Compared with quartile 1 with a rate of 6.7%, there was significantly greater in-hospital mortality as follows: 11.8% for quartile 2, 12.7% for quartile 3, and 11.7% for quartile 4 (all p-values < 0.001). Median length of stay was 6 days for all quartiles and median cost was greater with increasing quartile of procedural volume from $27,367 in quartile 1 to $35,191 in quartile 4.
In-hospital events and outcomes for acute ischemic stroke patients undergoing mechanical thrombectomy stratified by year of quartile of annual procedural volume (Nationwide Inpatient Sample 2016–2020).
IQR: interquartile range.
Excludes patients with palliative care.
In the logistic regression analysis, the odds of post-procedure ICH increased to 1.81 (p < 0.001), 1.84 (p < 0.001), and 1.98 (p < 0.001) among the quartiles from lowest to highest annual procedural volumes after adjusting for potential confounders including clinical severity markers. The odds of home discharge/self-care decreased to 0.66 (p < 0.001), 0.60 (p < 0.001), and 0.63 (p < 0.001) among the quartiles from lowest to highest procedural volumes. The odds of in-hospital mortality increased to 1.92 (p < 0.001), 1.99 (p < 0.001), and 1.84 (p < 0.001) among the quartiles from the lowest to the highest annual procedural volumes (Table 4).
Adjusted odds of outcomes for acute ischemic stroke patients undergoing mechanical thrombectomy stratified by year of quartile of annual procedural volume (Nationwide Inpatient Sample 2016–2020).
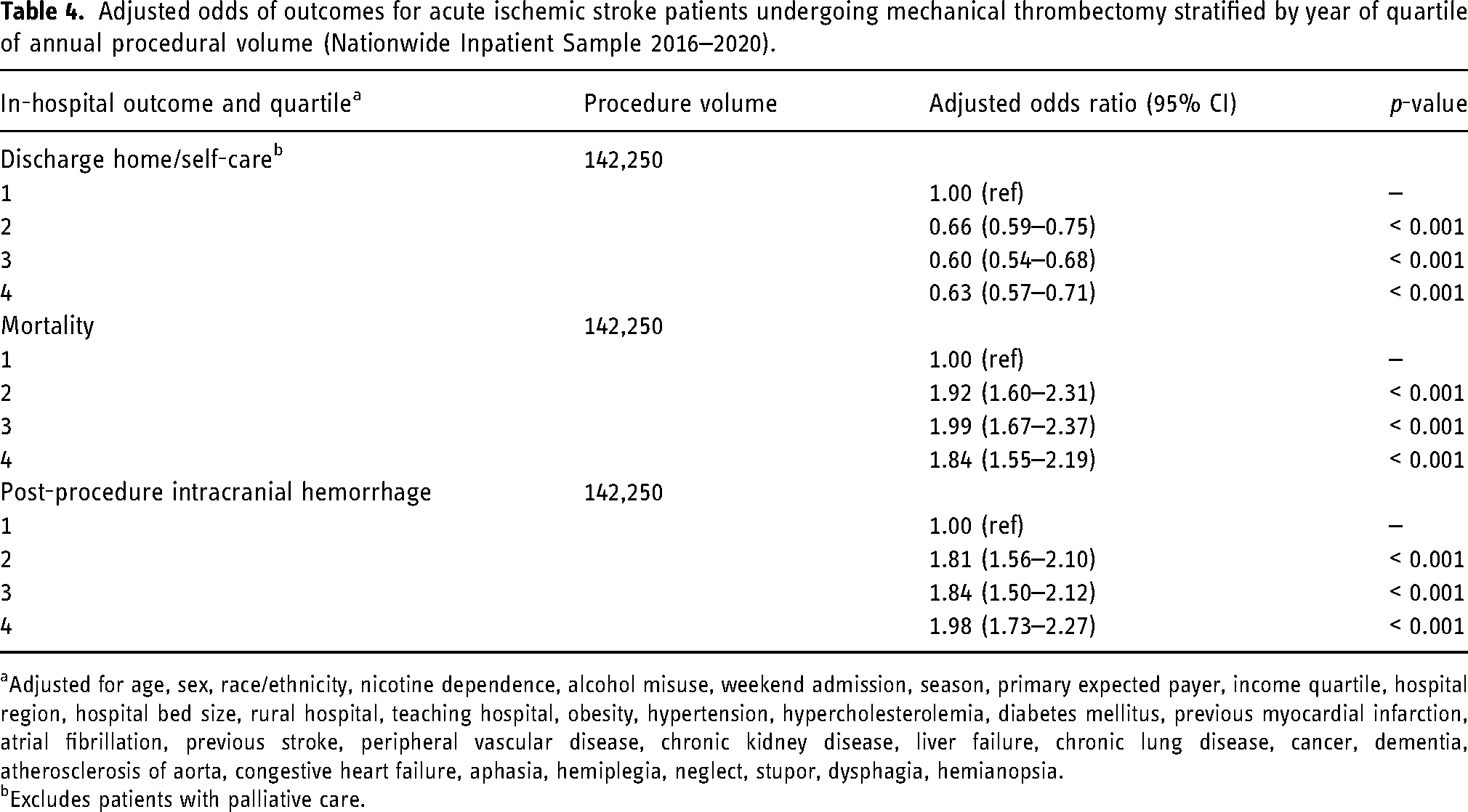
Adjusted for age, sex, race/ethnicity, nicotine dependence, alcohol misuse, weekend admission, season, primary expected payer, income quartile, hospital region, hospital bed size, rural hospital, teaching hospital, obesity, hypertension, hypercholesterolemia, diabetes mellitus, previous myocardial infarction, atrial fibrillation, previous stroke, peripheral vascular disease, chronic kidney disease, liver failure, chronic lung disease, cancer, dementia, atherosclerosis of aorta, congestive heart failure, aphasia, hemiplegia, neglect, stupor, dysphagia, hemianopsia.
Excludes patients with palliative care.
Discussion
In our analysis of nationally representative data from the United States, the odds of post-procedure ICH and in-hospital mortality increased and of home discharge/self-care decreased among the quartiles from lowest to highest annual procedural volumes of mechanical thrombectomy after adjusting for potential confounders including clinical severity makers. The median length of stay was similar for all quartiles, but the median cost was greater with the quartile of higher procedural volumes ranging from $27,367 in quartile 1 to $35,191 in quartile 4. Our results are somewhat different from results derived from multicenter registries.9–13,15,16 There are two studies that have evaluated the relationship between the annual procedural volume of MT and outcomes in acute ischemic stroke patients at a regional or national level.2,14 Asaithambi et al. 2 analyzed data from the Paul Coverdell National Acute Stroke Program between 2008 and 2018. Patient outcomes were compared across low-volume ( < 15 procedures per year), medium-volume (15–30 procedures per year), and high-volume hospitals (> 30 procedures per year). When compared with medium-volume hospitals, high-volume hospitals had a higher (p < 0.0001) and low-volume hospitals had a lower (p < 0.0001) percentage of patients discharged to home. 2 Stein et al. 14 analyzed inpatient Medicare data sets from 1 January 2016 to 31 December 2017, for USA individuals aged ≥ 65 years. For every 10 more hospital procedures, patients had 2% lower odds of in-hospital mortality and 2% greater odds of good outcome (disposition of inpatient rehabilitation or better). However, McCarthy et al. 27 analyzed Medicare datasets from 1 January 2016 through 31 December 2019 and reported that among hospitals with high procedural volume, higher volumes were associated with higher in-hospital mortality despite higher rates of intravenous thrombolysis and MT utilization when only high-volume hospitals were analyzed.
There are several potential explanations for the relationship between adverse outcomes and the annual procedural volume of MT at the hospitals. Higher volume centers may treat acute ischemic stroke patients who have high severity of neurological deficits, high-risk characteristics (delayed presentation or large ischemic core), or high burden of concurrent medical illnesses. 28 Surrogate markers of severity such as aphasia, hemiplegia, neglect, stupor, dysphagia, and hemianopsia were more prevalent among patients admitted to the hospitals in the quartiles of higher annual procedural volumes in our analysis. There was an increase in the rates of inter-hospital transfer among the quartiles from the lowest to highest procedural volumes. The proportion of patients with interhospital transfer was 12.4%, 17.5%, 28.3%, and 38.1%, for quartiles 1, 2, 3, and 4 respectively. Several studies have reported that patients who are treated with MT after interhospital transfer have a longer time interval from symptom onset to treatment.30–34 Froehler et al. 33 analyzed data from STRATIS (Systematic Evaluation of Patients Treated with Neurothrombectomy Devices for Acute Ischemic Stroke), a prospective, multicenter, observational, single-arm study of real-world MT for acute ischemic stroke at 55 sites. 33 Median onset-to-revascularization time was significantly higher among patients treated after inter-hospital transfer (202.0 min for direct admission patients vs. 311.5 min for interhospital transfer patients, p < 0.001). The proportion of patients achieving functional independence was lower among patients treated after inter-hospital transfer (52.2% for interhospital transfer patients and 60.0% for direct admission patients; p = 0.02). 33 George et al. 35 analyzed data from NIS (2009–2014) and reported that patients receiving MT after interhospital transfer had greater odds of symptomatic ICH compared with those with direct admission. 34 However, there were no differences in rates of in-hospital mortality. 35 Higher procedural volume hospitals may have catchment areas involving patients with low socioeconomic status or poor access to healthcare which may increase the rates of adverse outcomes due to multiple medical comorbidities.29,36,37 Another reason maybe that high-volume hospitals may be more likely to treat patients outside the criteria used in clinical trials. Such patients are at higher risk of death or disability regardless of expertise and efficiency of treating hospitals. 38 Most of the training programs are also located in hospitals with high procedural volume resulting in the involvement of less experienced operators (although under supervision) in the procedure.
Our results raise concerns regarding the use of the annual procedural volume of MT alone as a surrogate for quality care and better outcomes for hospitals that treat acute ischemic stroke patients.6–8 Indirectly, the analysis highlights the limitations of using procedural volume as a measure for qualification and certification in the absence of additional quality measures. Further efforts are required to better understand how procedural volume should be used in relation to other markers of the quality of care. Most certification pathways do not align procedural volume with outcomes or define a minimum threshold for achieving functional independence and mortality.6,39 Our results support expanding the metrics of the quality of care among acute ischemic stroke patients beyond annual procedural volumes. Future studies need to identify the underlying reasons for higher rates of adverse events in high-volume centers to improve rates of functional independence following MT. Improvements in outcomes in such hospitals are expected to enhance overall outcomes since a large proportion of acute ischemic stroke patients receive MT at high-volume centers in the United States of America. If additional studies demonstrate that a high proportion of inter-hospital transfers is increasing the rate of adverse outcomes due to delays incurred in the transfer process, strategies such as transferring the neurointerventionalist or bypassing hospitals to arrive directly at high-volume hospitals may be used.40,41 Furthermore, regional customization of stroke systems of care (SSOCs) to address differences in resources, hospital certifications, geography, and population density may be required. 42
Certain aspects of the analysis may have direct implications for interpretation. We used the data from the NIS, which provides minimal details on the severity of neurological deficits, diagnostic study results, and procedural details (site of occlusion and recanalization).38,43 Therefore, the exact reasons for differences in outcomes between hospitals with different annual procedural volumes for MT cannot be determined. The NIS also does not provide details regarding the certification status of the hospitals such as whether these hospitals are Acute Stroke Ready Hospitals, Primary Stroke Centers, Thrombectomy Capable Stroke Centers, or Comprehensive Stroke Centers. The NIS data also depend on the accuracy of ICD-10 diagnosis and procedure codes assigned in the data collection system. ICD-10 diagnosis codes have a high positive predictive value to identify acute ischemic stroke from the primary discharge diagnosis 44 and procedure codes can identify 98% and 87% of all patients receiving intravenous thrombolysis or those receiving MT, respectively. 45 Discharge destination can identify patients with death or disability defined by a modified Rankin scale score (mRS) at 90 days post-stroke with high predictive values and likelihood ratios. 46 For example, the predictive values of discharge to a rehabilitation facility/nursing home have ranged from 72% to 93% for identifying patients with death or disability defined by a mRS ≥ 3 at 90 days in previous studies.43,47,48 However, we acknowledge that discharge destination cannot match serial assessments of the National Institutes of Health stroke scale score or mRS grade at 90 days for identifying death or disability.
Conclusions
We observed an increase in adverse outcomes with increasing annual procedural volumes of MT at the hospitals which may have implications for using procedural volume as a surrogate measure of quality of care and functional independence in acute ischemic stroke patients.
Supplemental Material
sj-docx-1-ine-10.1177_15910199241288611 - Supplemental material for High mechanical thrombectomy procedural volume is not a reliable predictor of improved thrombectomy outcomes in patients with acute ischemic stroke in the United States
Supplemental material, sj-docx-1-ine-10.1177_15910199241288611 for High mechanical thrombectomy procedural volume is not a reliable predictor of improved thrombectomy outcomes in patients with acute ischemic stroke in the United States by Adnan I Qureshi, Hamza Maqsood, Daniel E Ford, Camilo R Gomez, Daniel F Hanley, Ameer E Hassan, Thanh N Nguyen, Farhan Siddiq, Alejandro M Spiotta, Syed F Zaidi and Chun Shing Kwok in Interventional Neuroradiology
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.