
Abstract
Introduction
We aimed to explore if anatomical and technical features could interact and favor the chances of reperfusion according to the treatment strategy: combined technique (CoT) of mechanical thrombectomy (MT) with contact aspiration and stent-retriever (SR) versus SR alone.
Methods
Retrospective analysis of a prospective MT database for carotid terminus or MCA-M1 occlusion, first-line SR alone or CoT, and angiographic run with SR deployed on the first pass. The primary analysis involved the interaction between clinical and angiographic characteristics and first-line MT modality on first-pass effect (FPE; first pass eTICI2c-3).
Results
A total of 300 consecutive patients were included (SR alone, n = 210 vs CoT, n = 90). Baseline characteristics as well as baseline ASPECTS, CTA collateral score, clot burden score, FPE were similar amongst groups. Anatomical and technical variables (presence of reperfusion channel, frequency of SR position in dominant MCA division, angle of device-clot interaction, and clot length) were comparable between groups, with exception of SR opening (diameter across the occlusion) and length of SR purchase beyond the clot being more pronounced in the SR group. None of the clinical, anatomical, and technical factors were found to have an interaction with the MT strategy on the chances of FPE (P-interaction ≥ 0.001). Multivariable logistic regression showed that clot burden score ≥8 (aOR 3.02, P = 0.003), angle of interaction (aOR 1.01, P = 0.015) but not the MT modality were associated with FPE.
Conclusion
No specific anatomical or technical features were observed to predispose to benefit when combining contact aspiration and SR thrombectomy. Clot burden score ≥ 8 and angle of interaction were independent factors associated with FPE. Additional studies are warranted.
Introduction
The combined technique (CoT) involves the use of stent retriever (SR) plus contact aspiration (CA) in large vessel occlusion (LVO) stroke mechanical thrombectomy (MT). 1 CoT has been reported to present a favorable safety profile and to potentially allow for fast reperfusion in clinical practice.1,2 The randomized clinical trial ASTER 2 (Effect of Thrombectomy With Combined Contact Aspiration and Stent Retriever vs Stent Retriever Alone on Revascularization in Patients With Acute Ischemic Stroke and Large Vessel Occlusion) indicated that CoT lead to similar final reperfusion rates compared to stent retriever alone. 3 ASTER2 however, demonstrated higher expanded thrombolysis in cerebral infarction (eTICI) 2b-3 and 2c-3, and lower use of rescue therapy after three repeated passes with the assigned technique. 3 We aim to explore if anatomical and technical features can interact with a particular technique and facilitate reperfusion, allowing for the recognition of subpopulations that could particularly benefit from CoT.
Methods
Study population
A prospectively maintained MT database from July 2016 to December 2021 was reviewed. Consecutive patients with anterior circulation LVOS due to intracranial internal carotid artery (ICA) or middle cerebral artery (MCA) M1 segment occlusions who underwent MT with SR alone or SR + CA as first-line therapy and had a digital subtraction run with the retriever deployed in the first pass were included. CoT cases using non-CA (“local aspiration”), patients with >1 occlusion site, tandem lesions (involving extracranial carotid artery pathology leading to ipsilateral stenosis >70% according to NASCET [North American Symptomatic Carotid Endarterectomy Trial] or occlusion), 5 or baseline occlusions eTICI > 1 were excluded. The study was approved by the local institutional review board.
Radiological data based on pre-procedural NCCT was assessed for non-contrast CT (NCCT) Alberta Stroke Program Early CT Score (ASPECTS) and for the presence of hyperdense vessel sign (HDVS). 6 The baseline CT angiography was used to determine the occlusion site, CTA collateral score, 7 clot length, 8 clot burden score (10-point scoring system), 9 type of extracranial carotid as well as cavernous carotid tortuosity. 10
Additionally, technical and angiographic variables that could influence the response to device performance were collected based on the DSA run with the deployed SR: (A) SR placement in the superior vs inferior division 11 ; (B) SR placement in the dominant, co-dominant versus non-dominant division; (C) length (mm) of SR beyond the distal end of the clot; (D) proximal clot coverage by the proximal functional portion of the SR (dichotomous); (E) vessel angulation (based on the intersection of the longitudinal axis at the proximal and distal ends of the occlusion in the anteroposterior view; Figure S5); (F) diameter of the retriever opening proximal and distal to clot (for distal-to-proximal diameter ratio indicating vessel size mismatch); (G) presence of a perfusion channel; (H) SR opening (luminal diameter at the level of the clot); (I) clot lenght.
Interaction subgroup analyses were performed to identify the variables associated with first-pass effect (mTICI2c-3 with the first pass - FPE) in both groups (SR alone and CoT). Secondary interaction analyses utilizing modified FPE (mTICI2b-3 with the first pass - mFPE) were pursued. A comparison between the SR and CoT arms was performed, as well as an analysis for predictors of FPE.
Statistical analysis
After assessing the normality of distributions by the Shapiro–Wilk test, continuous variables were expressed as mean ± SD or median (interquartile range) and compared with the Mann–Whitney U test or Student t test as appropriate. Categorical variables were reported as frequencies and percentages and were compared using Pearson X2, Fisher exact. Interaction subgroup analyses were performed to evaluate variables that could have interaction with the chances of reperfusion by each technique. The primary endpoint was FPE, while the secondary endpoint mFPE.
The association between first-line MT technique and angiographic outcome variables (odds ratio for FPE and mFPE) was analyzed across subgroups through logistic regression with treatment versus subgroup interaction terms. These analyses were adjusted for use of balloon guide catheter (BGC), baseline ASPECTS and site of occlusion. In the secondary analysis, we used logistic regression to identify the association of clinical and angiographic variables with FPE. These analyses, with one variable of interest at a time, were adjusted for balloon guide catheter, site of occlusion, baseline ASPECTS, MT technique and I.V-tPA.
Statistical analyses were performed using R software V2023.03.0 and SPSS Version 29.0.1.1(244). We did not perform imputation for missing data. Significance was set at P < 0.001 for the interaction analyses due to multiple testing. For the analysis of association of clinical and angiographic variables with FPE, an alpha of 0.05 was considered. All P values were two-sided.
Results
A total of 300 consecutive patients were included (SR alone, n = 210 vs combined technique, n = 90) (Figure 1).
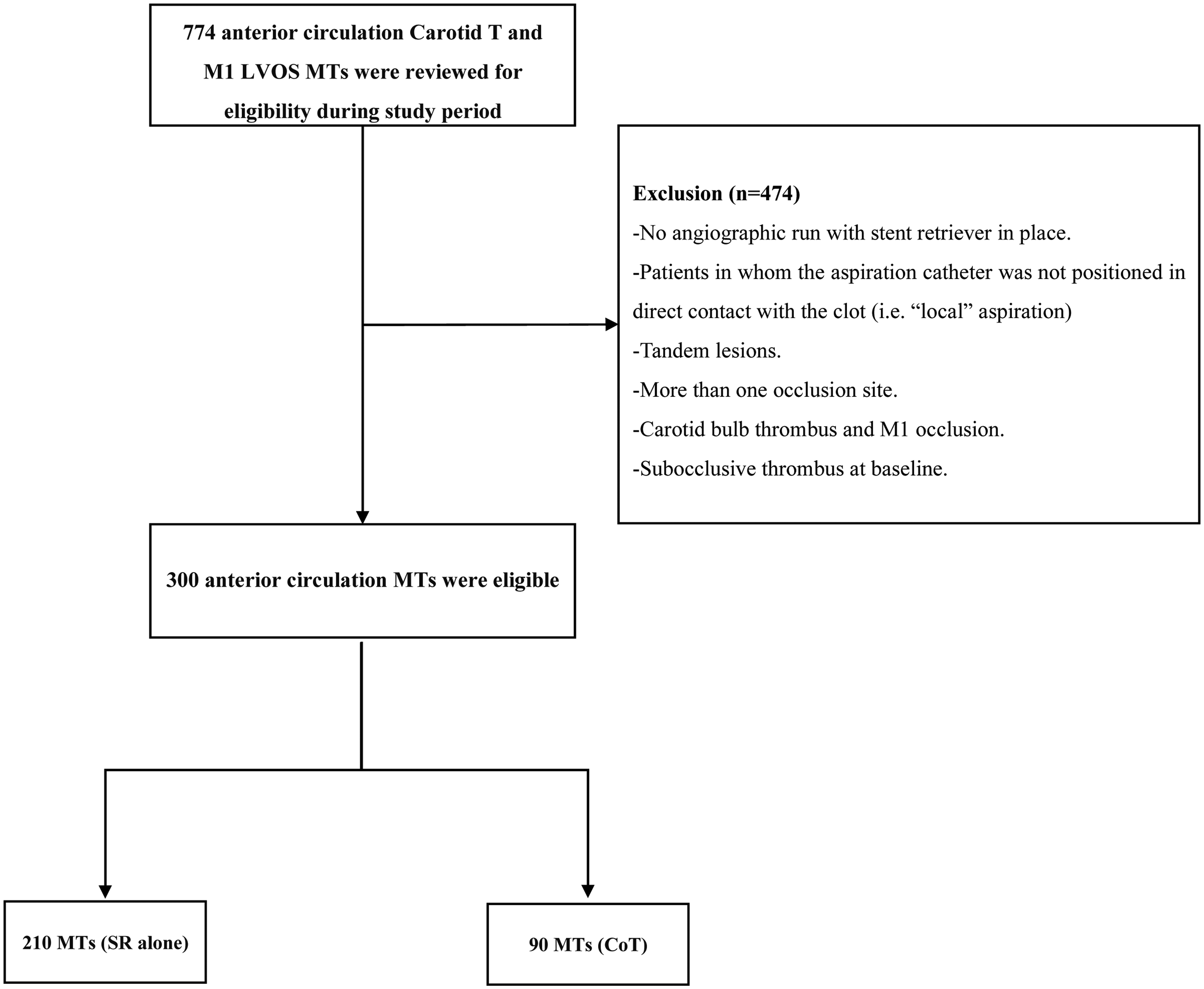
Study flowchart.
First pass effect
Multivariable regression indicated clot burden score ≥8 (aOR 3.02, P = 0.003) and angle of interaction (aOR 1.01, P = 0.015) associated with FPE (Supplemental Table S1).
Stent-retriever vs combined technique
The median aspiration catheter inner diameter was 0.070 inches [0.068–0.071 inches] and the median SR capture zone length was 30 mm [30–40 mm]. Demographics were comparable between groups with few exceptions (Table 1). The angioarchitectural characteristics were comparable between groups, with the exception of larger diameter of stent opening at the level of the thrombus (1.2 vs 1.0 mm, P = 0.007) and longer length of SR beyond clot (19 vs 15 mm, P = 0.001) in the SR cohort (Table 1). The frequency of parenchymal hematoma type-I was higher in the CoT arm.
Demographics, clinical and procedural characteristics among groups.
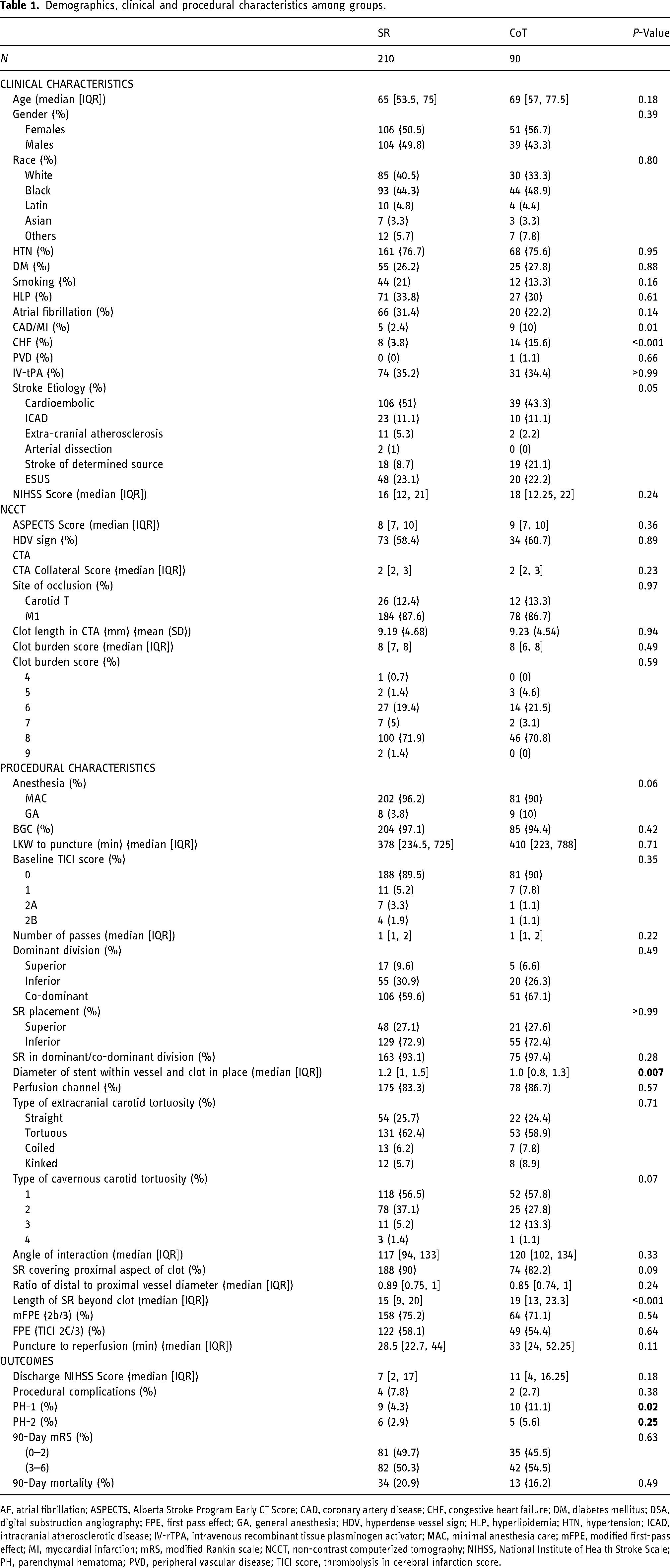
AF, atrial fibrillation; ASPECTS, Alberta Stroke Program Early CT Score; CAD, coronary artery disease; CHF, congestive heart failure; DM, diabetes mellitus; DSA, digital substruction angiography; FPE, first pass effect; GA, general anesthesia; HDV, hyperdense vessel sign; HLP, hyperlipidemia; HTN, hypertension; ICAD, intracranial atherosclerotic disease; IV-rTPA, intravenous recombinant tissue plasminogen activator; MAC, minimal anesthesia care; mFPE, modified first-pass effect; MI, myocardial infarction; mRS, modified Rankin scale; NCCT, non-contrast computerized tomography; NIHSS, National Institute of Health Stroke Scale; PH, parenchymal hematoma; PVD, peripheral vascular disease; TICI score, thrombolysis in cerebral infarction score.
Interaction analysis
Interaction subgroup analyses showed that none of the clinical (Supplemental Figure S1), non-invasive imaging (Figure 2) or conventional angiogram derived technical (Figure 3) features were associated with FPE according to technique. The analysis for mFPE demonstrated similar results (Supplemental Figures S2–S4).
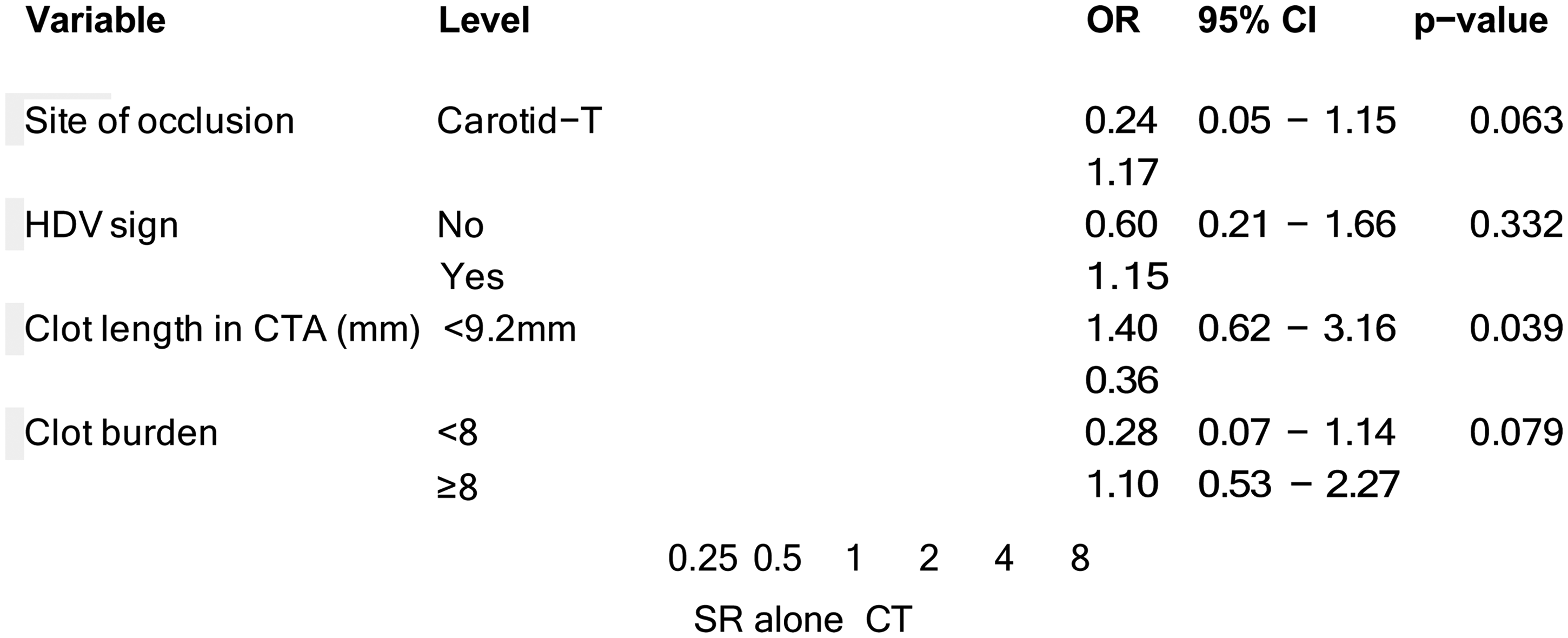
Interaction analysis for technique and FPE (Imaging Characteristics). *Adjusted for BGC, Baseline ASPECTS, site of occlusion.
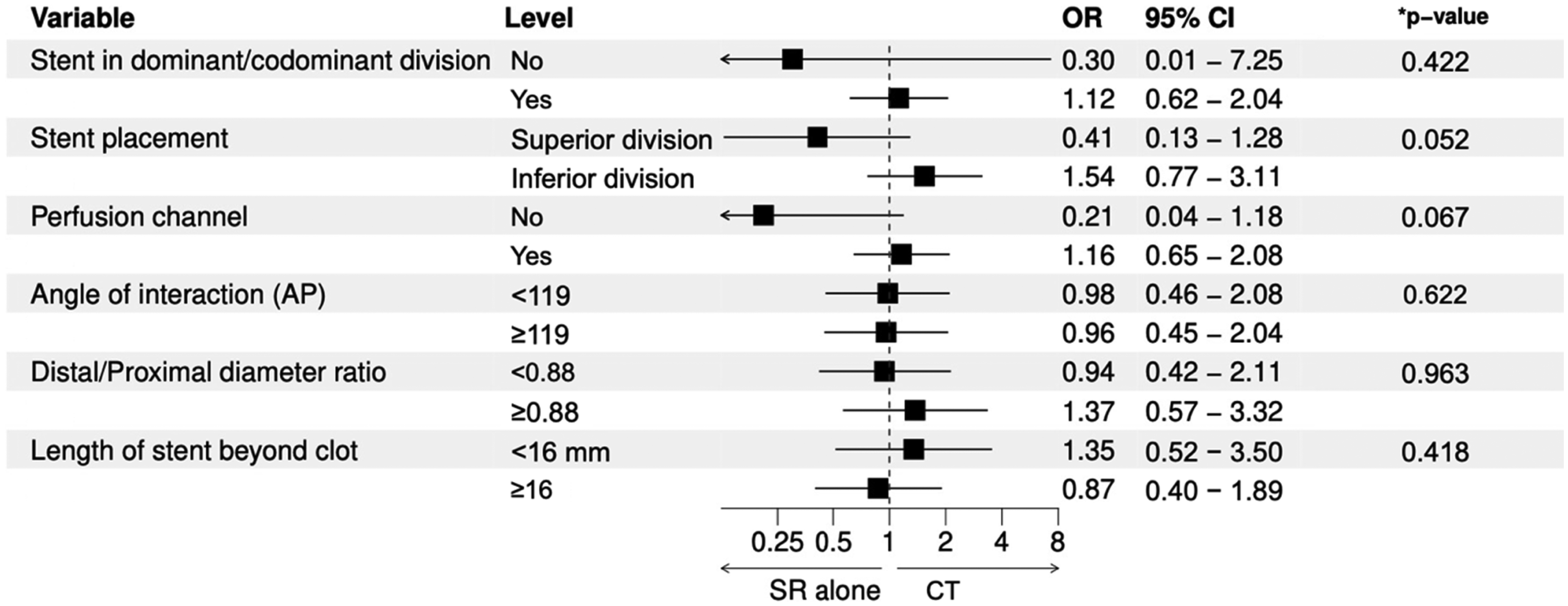
Interaction analysis for technique and FPE (Procedural Characteristics). *Adjusted for BGC, Baseline ASPECTS, site of occlusion.
Discussion
We observed that increased clot burden score and wider angle of interaction were associated with first pass reperfusion in anterior circulation LVO due to carotid terminus or proximal MCA(M1) occlusions. No anatomical or procedural features were noted to have an interaction with the technique (SR vs CoT) to mediate reperfusion.
FPE is an important predictor of good clinical recovery and has been associated with MCA M1 occlusions (vs ICA terminus),13–15 use of BGC, intravenous thrombolysis, 16 decreasing age and increasing ASPECTS. 15 We observed that increased clot burden affected the changes of FPE/mFPE significantly, in line with previously published data. 17 We demonstrated that the angle of interaction of device-thrombus affected the chances of reperfusion, which has been previously reported with the use of MERCI retriever, and also with the use of contemporary techniques such as stent-retriever and CA.18–20 The technique (CoT vs SR) was not found to be influence the chances of FPE in the present analysis.
In a multicenter retrospective series, transitioning to CoT after two SR failed was associated with higher chances of reperfusion as compared to a third SR pass. 2 Pre-specified analyses of the Combined Use of Contact Aspiration and the Stent Retriever Technique versus Stent Retriever Alone for Recanalization in Acute Cerebral Infarction (ASTER 2) randomized clinical trial demonstrated increased eTICI2b-3 and eTICI2c-3 after the assigned initial intervention alone, a trend toward higher mPFE and significantly lower frequency of rescue treatment utilization with CoT compared to SR. 4 Although clear overall benefits of a given technique have not been demonstrated, 21 it possible that a subgroup of patients could benefit more substantially from CoT.
We analyzed multiple features from non-invasive imaging in an attempt to evaluate potential interactions between different variables and the technique. Contrary to ASTER 2, which showed that CoT performed better in carotid terminal occlusions, we could not replicate this finding. This could be explained by the difference in the median clot burden score in the carotid T occlusion who underwent CoT in ASTER2 vs the present sample (5 vs 8), as well as the median clot length (19 mm vs 9 mm), respectively. 4 Although HDVS, indicating RBCs rich clot, has been associated with better reperfusion with SR as compared to CA, 6 we did not find that its presence would interact with the CoT versus SR techniques. 22
Considering that a smaller mismatch between the vessel diameter proximal and distal to the occlusion could lead to better chances of SR-thrombus integration, we investigated the impact of SR deployment in the dominant/codominant division as well as the ratio of the arterial diameter pre- and post-occlusion. A previous study has shown that placement of the SR in the dominant division or co-dominant division was associated with better rates of FPE and mFPE. 11 We did not observe that the division placement had an impact on the performance of any of the techniques (SR and CoT), which may be explained by the fact that almost 95% of our cohort had the SR placed in either the dominant or codominant division. A previous study (n = 89) has demonstrated that the SR placement in the inferior trunk in M1 occlusions was associated with a high rate of first-pass near-complete/complete reperfusion when using Stent retriever Assisted Vacuum-locked Extraction (SAVE) technique. 23 Another study (n = 90) investigating SR placement in M1 occlusions indicated no difference when SR was placed in the superior versus inferior division. 11 We observed that the placement in the superior or inferior divisions did not influence FPE/mFPE, and that there was no interaction with the applied technique.
In the ESCAPE-NA1 Trial, the presence of a perfusion channel upon SR deployment has been found to be strongly associated with successful reperfusion. 24 Contrarily, we didn’t find it to predict FPE or to interact with the investigated techniques. Longer stent retrievers have been described to lead to higher rate FPE and modified FPE compared with their shorter counterparts. 25 In the present study, the length of SR beyond the occlusion was not observed to increase the chances of FPE or to interact with the thrombectomy technique.
A more aggressively angled MCA M1 has been associated with unsuccessful reperfusion with the use of the MERCI retrieval system. 18 The same principle appears to be applicable to more modern techniques, such as CA and retrievers thrombectomy. A previous study has shown that the effect of direct thrombo-aspiration is related to the angle of interaction between the aspiration catheter and the clot (more obtuse angles leading to improved vector for clot contact). 2 A SR-based study has demonstrated that non-reperfused (TICI 0–2a) patients showed significantly larger ICA-to-M1, as well as proximal M1-distal M1 and M1-to-M2 angles than patients with successful reperfusion (TICI 2b/3). 20 We found that each degree of angulation increases the odds of FPE by 1%. No association between the angle of interaction of SR with the chances of reperfusion in different techniques.
The present study has some limitations related to its single-center design, retrospective nature and limited sample size for subgroup analyses. Further studies are warranted to evaluate potential factors that could influence response to a particular technique and its associated risks.
Conclusion
No specific anatomical or technical features were observed to predispose to benefit when adding CA to SR thrombectomy. Clot burden ≥8 and angle of interaction were independent factors associated with FPE. Additional studies are warranted.
Supplemental Material
sj-docx-1-ine-10.1177_15910199241298325 - Supplemental material for Combined technique versus stent-retriever alone: Interaction analysis of angioarchitectural and technical features
Supplemental material, sj-docx-1-ine-10.1177_15910199241298325 for Combined technique versus stent-retriever alone: Interaction analysis of angioarchitectural and technical features by Mohamed A. Tarek, Mateus Damiani Monteiro, Pedro N. Martins, Mahmoud H Mohammaden, Jonathan A. Grossberg, Jay Dolia, Aqueel Pabaney, Alhamza Al-Bayati, Raul G. Nogueira and Diogo C. Haussen in Interventional Neuroradiology
Footnotes
Contributors
Conceptualization: MAT and DCH. Methodology: MAT and DCH. Formal analysis: MAT, SR, PM, MHM, and DCH. Investigation: MAT, MDM, PM, MHM. Data collection: MAT and MDM. Data curation: all authors. Writing—original draft: MAT and DCH. Writing—review and editing: All authors. Visualization: MAT, PM and DCH. Project administration: MAT. Supervision: DCH. Guarantor: DCH. Other co-authors: critical revision of manuscript. All authors gave final approval of the version to be published and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Data availability statement
Anonymized data that support the findings of the study are available from corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
This study involves human participants and was approved by Emory University institutional review board IRB00090915. The IRB waived patient consent.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.