
Abstract
Background
This study aimed to evaluate the periprocedural and postprocedural outcomes of endovascular treatments for cerebral vasospasm after subarachnoid hemorrhage using data from the Japan Registry of Neuroendovascular Therapy 4 (JR-NET4) (2015–2019).
Methods
In this retrospective multicenter study, procedures of endovascular treatment for cerebral vasospasms registered in JR-NET4 were analyzed. The procedure outcomes and complications for percutaneous transluminal angioplasty (PTA) and intra-arterial administration of vasodilators (IA-vasodilator) were compared. The factors associated with imaging and symptom improvement were assessed.
Results
Analysis of 1549 procedures revealed that 83.5% of procedures were IA-vasodilator and 16.5% of procedures were PTA. Postprocedural imaging improvement was achieved in 97.0% of patients, and 50.1% of patients experienced symptomatic improvement. The overall complication rate was 1.6%. No significant differences were detected in overall complication rates between patients who underwent PTA and intra-arterial administration of vasodilators; however, hemorrhagic complications were significantly more frequent in patients who underwent PTA. Shorter intervals from symptom onset and the absence of periprocedural complications were associated with improved imaging and neurological outcomes. Local anesthesia and prior treatment with endovascular embolization for ruptured aneurysms were associated with enhanced neurological improvements.
Conclusion
Endovascular treatment for cerebral vasospasm is safe and effective. Factors such as early intervention and treatment under local anesthesia may contribute to neurological improvements. However, caution is warranted for PTA due to the slightly higher incidence of hemorrhagic complications.
Keywords
Introduction
Subarachnoid hemorrhages (SAHs) are associated with severe morbidity and mortality. Cerebral vasospasms cause delayed cerebral ischemia (DCIs). DCIs occur within 4 to 14 days after the onset of SAH in approximately 30% of cerebral vasospasm cases.1,2 Medication, such as vasodilators and antiplatelet agents (nimodipine,3,4 fasudil hydrochloride,5,6 statin,7,8 and cilostazol9–11), and fluid and circulation management 4 are effective in treating vasospasm. For cerebral vasospasm refractory to medication therapy, endovascular treatments, including intra-arterial administration of vasodilators (IA-vasodilator) and balloon dilation (percutaneous transluminal angioplasty, PTA), are recommended. 12 The efficacy of endovascular treatment, especially intra-arterial administration of vasodilators, is often temporary and may require repeated treatments. High-level evidence regarding endovascular treatment for vasospasms is limited.
The aim of the Japan Registry of Neuroendovascular Therapy (JR-NET) is to understand the status of neuroendovascular treatments, analyze treatment outcomes, and identify factors influencing outcomes. Patients who underwent neuroendovascular treatment in Japan between 2005 and 2009 were enrolled and analyzed in JR-NET1 and 2. 13 The subsequent JR-NET3 reported data from 2010 to 2014. Imamura et al. reported that a shorter time from symptom onset to treatment was associated with more effective treatment and PTA was associated with mechanical hemorrhagic complications in endovascular treatment for cerebral vasospasm based on the JR-NET3 data. 14 Herein, we analyzed data from the JR-NET4, which registered patients from 2015 to 2019. We evaluated the periprocedural and postprocedural outcomes of endovascular treatment for cerebral vasospasms after subarachnoid hemorrhage and compared the results with those previously reported outcomes.
Methods
After excluding cases with insufficient data or duplicate registrations, 1549 (88.97%) of 1741 cases of endovascular treatment for cerebral vasospasms registered in JR-NET4 were analyzed. The following case details were collected: patient age and sex, prior treatment performed on the ruptured aneurysm (direct surgery or endovascular treatment), site of cerebral vasospasm where treatment was performed (anterior circulation, posterior circulation, or both), doctor responsible for performing the treatment (supervisory doctor, specialist certified by the Japanese Society of Neuroendovascular Therapy, or non-specialist), anesthesia (general or local), number of treatments (the first time or the second time or more), the interval between the onset of neurological symptoms and treatment (within 3 h, 3–6 h, or more than 6 h or unclear), and the treatment strategy (IA-vasodilator or PTA). The Japanese Society for Neuroendovascular Therapy has a certification system for Specialists and Supervisory doctors. To become a Specialist, one must complete specialized training, perform over 100 treatments (including as an assistant), and gain experience in over 200 diagnostic angiography procedures. Certification requires a review of case records and passing both written and oral exams. A Supervisory doctor is a Specialist who has performed over 200 procedures and meets additional requirements such as presenting at academic conferences and publishing papers related to neuroendovascular therapy. In this report, the term "Responsible physician" refers to the individual in charge of each treatment, and we have assessed whether they hold a specialist or supervisory doctor certification or are uncertified. For periprocedural outcomes, we analyzed procedure-related complications, postprocedural imaging improvement, and postprocedural neurological symptom improvement. Postprocedural imaging improvement refers to cases where, in both PTA or IA vasodilator, an increase in vessel diameter compared to pre-procedure was successfully achieved, and in IA vasodilator treatment, overall vessel dilation distal to the treated vessel and improved peripheral blood flow were observed. Postoperative neurological symptom improvement refers to any improvement in focal neurological symptoms or level of consciousness compared to the preoperative state. Additionally, intracranial hemorrhagic and ischemic complications were analyzed as neurovascular complications.
Continuous variables were expressed as means ± SDs. Patient characteristics, lesion characteristics, and complications were compared between the two treatment strategies (IA-vasodilator or PTA). Factors associated with imaging and neurological symptom improvements and neurovascular complications after treatment were analyzed. Chi-square and t-tests were used for univariate analyses. The multivariate analysis was performed using logistic regression analysis and included factors with p-values of <0.05 from the univariate analyses. A value of p of <0.05 was defined as significant. SPSS version 29 (IBM Corp., Armonk, New York, USA) was used for statistical analysis.
The funder of the study had no role in study design, data collection, data analysis, data interpretation, or writing of the report.
Results
Table 1 shows the overall patient characteristics and treatment details. The mean patient age was 60.23 ± 14.05 years, and the patient population included 1092 female patients (70.5%). Prior treatment for ruptured aneurysms included direct surgery in 708 patients (45.7%) and endovascular treatment in 818 patients (52.8%); 23 patients (1.5%) were untreated. Most cerebral vasospasms (91.0%, 1410 cases) were in the anterior circulation. The most common responsible physicians were supervisory doctors (96.4%); only 3.6% of procedures were performed by specialists or non-specialists. Endovascular treatments were performed under local anesthesia in 1433 cases (92.5%). The procedures included 1071 (69.1%) first-time treatments and 478 (30.9%) second or more treatments. In 512 cases (33.1%), patients were treated within 3 h of symptom onset. In 254 cases (16.4%) patients were treated 3–6 h after symptom onset, and more than 6 h elapsed or onset time was unclear in 883 cases (60.5%). Most patients (1294 patients, 83.5%) were treated with IA-vasodilators, whereas 255 (16.5%) patients underwent PTA. Vasodilation on imaging was obtained in 97.0% of patients, and symptomatic improvements were achieved in 50.1% of patients. Overall complications occurred in 38 patients (2.5%), including 9 (0.6%) patients with intracranial hemorrhagic complications and 16 (1.0%) patients with ischemic complications.
Procedure characteristics and treatment details and results.
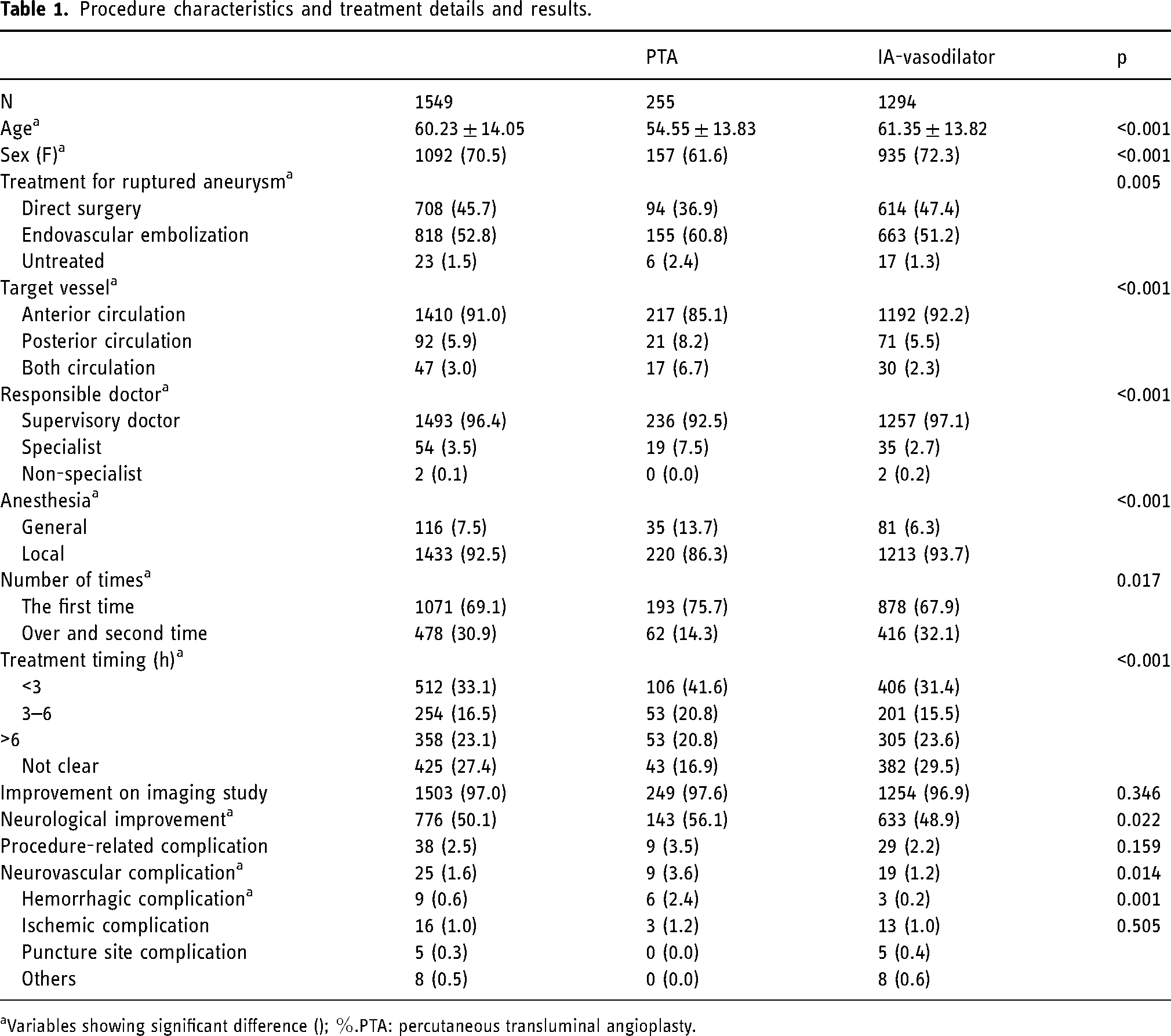
Variables showing significant difference (); %.PTA: percutaneous transluminal angioplasty.
Table 1 shows the differences between patients treated with IA-vasodilator and patients treated with PTA. Patients treated with PTA were significantly younger (PTA vs IA-vasodilator: 54.55 ± 13.83 vs. 61.35 ± 13.82; p < 0.001) and had more prior endovascular treatments (60.8% vs. 51.2%; p = 0.005) compared with patients treated with IA-vasodilators. In addition, the frequency of posterior circulation was slightly higher in patients treated with PTA compared with patients treated with IA-vasodilators (8.2% vs. 5.5%; p < 0.001). More cases were performed by a specialist as a responsible doctor (not a supervisory doctor) in the PTA group compared with the IA-vasodilator group (7.5% vs. 2.7%; p < 0.001). More patients received general anesthesia in the PTA group compared with the IA-vasodilator group (13.7% vs. 6.3%; p < 0.001). PTA was the first treatment in more patients compared with the IA-vasodilator group (75.7% vs. 67.9%; p = 0.006). The time from symptom onset was within 3 h more frequently in the PTA group compared with the IA-vasodilator group (41.6% vs. 31.4%; p < 0.001). No difference in the frequency of improvement in imaging was detected between the groups (97.6% vs. 96.9%; p = 0.346), but neurological symptoms improved in more patients in the PTA groups compared with the IA-vasodilator group (56.1% vs. 48.9%; p = 0.022). No significant difference in the overall incidence of complications was detected between the two groups (3.5% vs. 2.2%; p = 0.159). Neurovascular complications, including hemorrhagic and ischemic complications, occurred more frequently in the PTA group compared with the IA-vasodilator group (3.6% vs. 1.2%; p = 0.014). Specifically, hemorrhagic complications were significantly higher in the PTA group compared with the IA-vasodilator group (2.4% vs. 0.2%; p ≤ 0.001); whereas no significant difference in the occurrence of ischemic complications was detected (1.2% vs. 1.0%; p = 0.505).
Factors associated with postprocedural image improvement are shown in Table 2. Univariate analyses revealed the following factors associated with image improvements: a supervisory doctor as the responsible doctor (improvement vs. non-improvement: 96.6% vs. 89.1%; p = 0.023), a shorter interval from symptom onset to treatment (<3 h: 33.6% vs. 15.2%; p = 0.018), and neurological complications (1.5% vs. 6.5%; p = 0.036). All significant factors from the univariate analyses were significant in the multivariate analysis. Using symptom onset of ≥6 h or unclear time from symptom onset as a reference, image improvement was significantly higher in patients treated in less than 3 h (OR 2.727; 95%CI 1.261–6.663; p = .012). No significant differences in improvements were detected between patients treated between 3–6 h or ≥6 h after symptom onset (OR 1.459; 95%CI 0.628–3.387; p = 0.374). Neurovascular complications negatively impacted image improvement (OR 0.216; 95%CI 0.061–0.766; p = 0.018).
Analysis of factors associated with improvement on imaging after treatment.
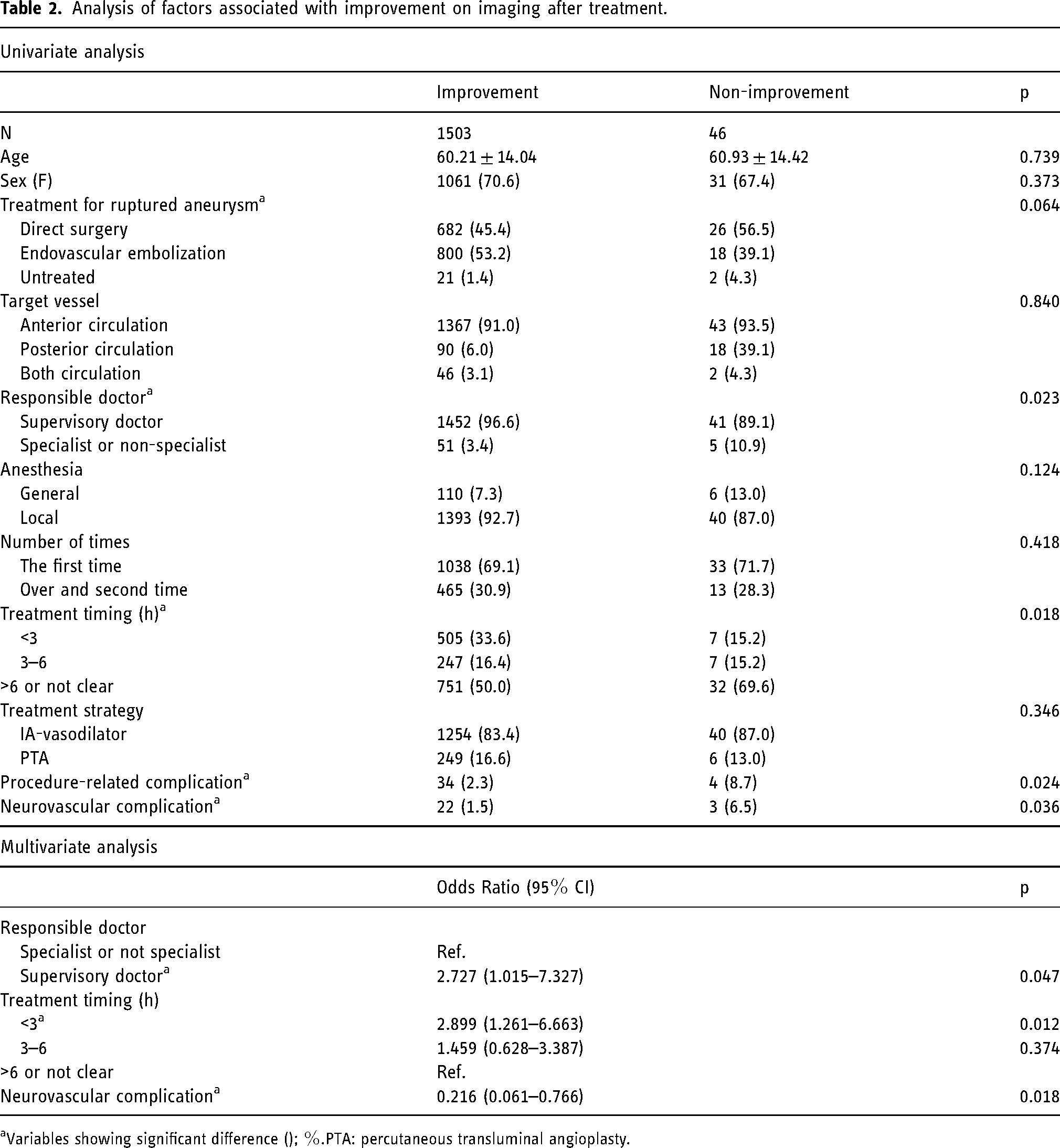
Variables showing significant difference (); %.PTA: percutaneous transluminal angioplasty.
Factors associated with postprocedural neurological improvements are shown in Table 3. Univariate analyses revealed the following factors that were significantly associated with postprocedural neurological improvements: treatment methods for ruptured aneurysm (improvement vs. non-improvement: endovascular embolization: 56.6% vs. 49.0%; p = 0.004), supervisory doctor as the responsible doctor (98.3% vs. 94.4%; p < 0.001), local anesthesia (95.7% vs. 89.3%; p < 0.001), first-time treatment (71.3% vs. 67.0%; p = 0.040), shorter interval from symptom onset to treatment (<3 h: 47.9% vs. 18.1%; 3–6 h: 19.8% vs. 12.9%; p = 0.002), PTA treatment (18.4% vs. 14.5%; p = 0.022), and complications (1.3% vs. 3.6%; p < 0.001). Multivariate analysis revealed the following factors that were significantly associated with postprocedural neurological improvement: prior treatment in the endovascular embolization and untreated groups compared with direct surgery (OR 1.476; 95%CI; 1.118–1.848; p < 0.001 and OR 2.990; 95%CI; 1.212–7.376, respectively; p = 0.017) and local anesthesia compared with general anesthesia (OR 2.167; 95%CI; 0.806–3.559; p = 0.003). Using the time from symptom onset of 6 h or more or unclear as a reference, the frequency of neurological improvements was significantly higher in patients treated for <3 h from symptom onset (OR5.379; 95%CI 4.128–6.919; p < 0.001) or 3–6 h from symptom onset (OR3.170; 95%CI 2.340–4.294; p < 0.001). Neurovascular complications negatively impacted image improvements (OR 0.182; 95%CI 0.065–0.515; p = 0.001).
Analysis of factors associated with neurological improvement after treatment.
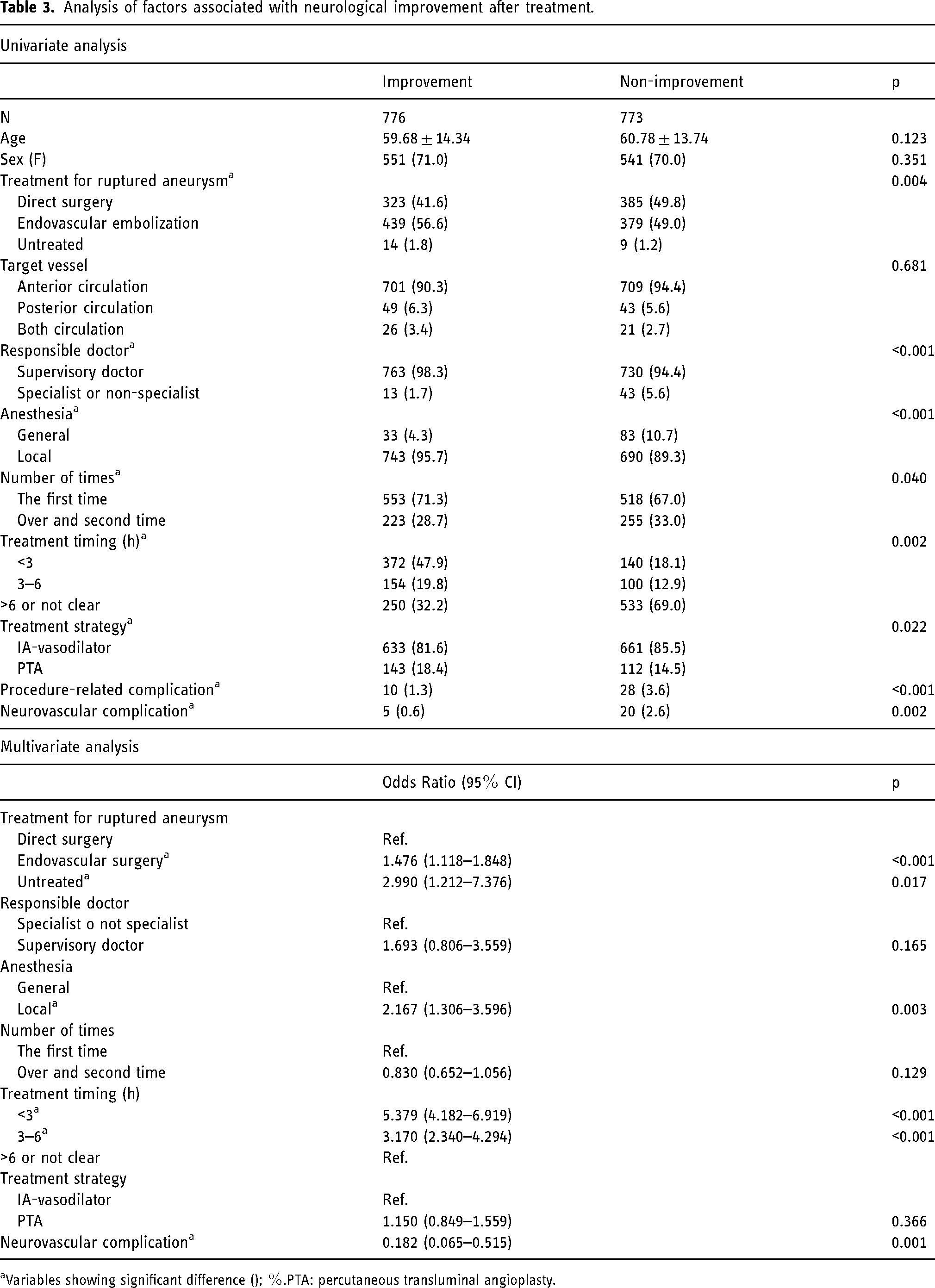
Variables showing significant difference (); %.PTA: percutaneous transluminal angioplasty.
Neurovascular complications were encountered in 1.6% of patients (Table 4). Univariate analysis revealed the following factors that were significantly associated with neurovascular complications: the first treatment (without complications vs. with complications; 68.8% vs. 88.0%; p = 0.026) and PTA treatment strategy (16.1% vs. 36.0%; p = 0.014). In multivariate analysis, only PTA was significantly associated with neurovascular complications (OR 2.743; 95%CI 1.195–6.293; p = 0.017).
Analysis of factors associated with neurovascular complications.
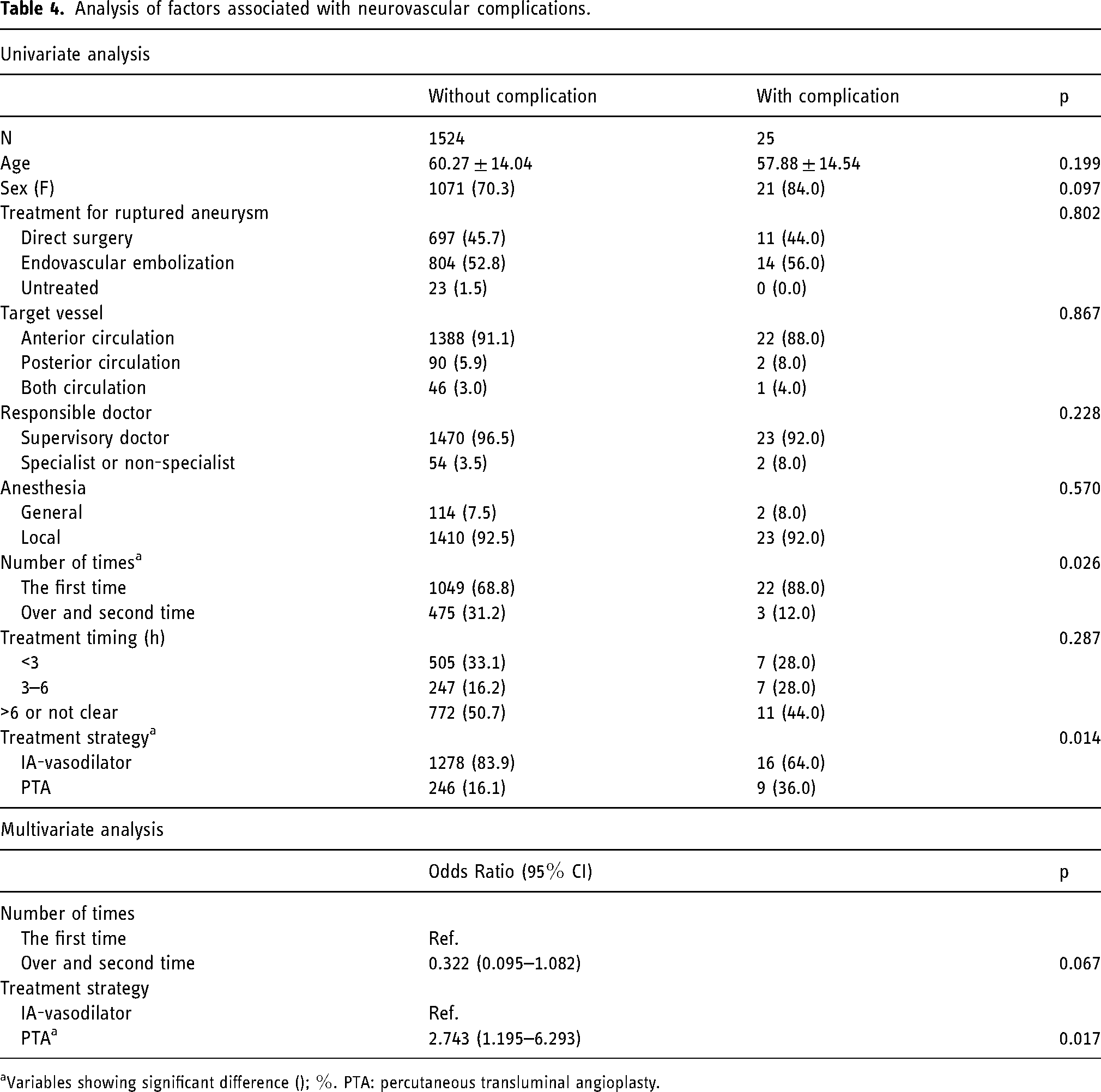
Variables showing significant difference (); %. PTA: percutaneous transluminal angioplasty.
Discussion
Analysis of endovascular treatment for cerebral vasospasms in JR-NET4 showed that 83.5% of patients were treated with arterial vasodilator administration and 16.5% of patients were treated with PTA. Postprocedural imaging improvements were achieved in 97.0% of patients and symptom improvements were achieved in 51.0% of patients. These results were similar to previous results from JR-NET2 13 and JR-NET3. 14
Postprocedural imaging improved in most cases and was positively associated with a shorter time from symptom onset and the absence of periprocedural complications. These factors were also associated with postoperative neurological symptom improvement. These results were similar to the results from JR-NET3. These results indicate that early therapeutic intervention should be undertaken before the appearance of symptoms and the onset of irreversible ischemia. To strengthen treatment for cerebral vasospasm and prevent progression to DCI, cerebral vasospasms should be detected as early as possible. The diagnosis relies on image evaluation, but the use of noninvasive methods such as transcranial doppler15–17 and continuous electroencephalography 18 has also been reported. Early diagnosis before symptom manifestation, reinforcement of drug therapy, and timely intervention with endovascular treatment are crucial for preventing cerebral infarctions. Our results support these interventions.
One finding that diverged from the JR-NET3 results is the significant contribution of the use of local anesthesia instead of general anesthesia to improve neurological outcomes. In the previous report, the use of local anesthesia significantly improved the outcome in the univariate analysis but not in the multivariate analysis. The state of the impending cerebral vasospasm may be adversely affected by general anesthesia due to factors such as hypotension or sedative drugs. In situations where neurological symptoms have manifested, safely performing treatment under local anesthesia can be challenging. However, appropriate sedatives are preferable instead of general anesthesia. In the current study, the use of sedatives was included in the local anesthesia group.
The results of the current study concerning prior treatment for ruptured intracranial aneurysms were also distinct. More patients treated with endovascular embolization experienced postprocedural neurological symptom improvements compared with patients treated with direct surgery. Previous reports showed that patients who underwent endovascular embolization for ruptured aneurysms experienced a lower incidence of cerebral vasospasms compared with patients who were treated with direct surgery. 19 Direct surgery is more invasive to the cerebral vasculature than endovascular interventions and may be associated with more severe cerebral vasospasms, resulting in worse treatment efficacy. However, in the current study, the severity of subarachnoid hemorrhage and the severity of symptoms were not investigated. Thus, this possible explanation cannot be verified.
Cerebral vasospasms can be treated with IA-vasodilator or PTA. The differences between these two treatments were compared in this study. IA-vasodilators can be employed to treat distal vessels; however, the therapeutic effects are often transient, and repeated treatments are frequently necessary. Although PTA is limited to the treatment of proximal vessels, the effects are lasting for a longer time. However, PTA incurs a higher risk of severe hemorrhagic complications, including vessel rupture. In this study, PTA was associated with more neurovascular complications, including a higher frequency of hemorrhagic complications, compared with IA-vasodilator treatment. The choice of treatment technique and indications should be carefully considered. The univariate analysis showed a significantly higher improvement in neurological symptoms in the PTA group. However, this difference was not confirmed in the multivariate analysis. Mode of anesthesia, the responsible physician, and treatment timing were different between the two groups, which may have influenced the results. PTA may have been performed for more severe cerebral vasospasm in more proximal locations, but these aspects were not analyzed in this study. Thus, the results should be interpreted with caution.
Although many subjects underwent treatment with an IA-vasodilator in this study, the specific vasodilators were not obtained, which poses a limitation to the study. In Japan, papaverine or fasudil may be predominantly used for arterial administration. Several reports demonstrate the effectiveness of papaverine and nimodipine20–23. However, the use of nimodipine has not been approved in Japan. Fasudil may be widely used in Japan24–26. The risk of IA-vasodilators is lower than the risk for PTA. However, the short half-life of these drugs requires repeated treatments. Identifying the peak of cerebral vasospasms and intervening with treatment at the appropriate times are crucial keys to improving prognosis. Although various vasodilators with different mechanisms are being used, studies comparing their effectiveness are lacking. Overall, standard treatment protocols have not been established due to a lack of evidence, and safe interventions without complications are needed.
Medication therapy and endovascular interventions for cerebral vasospasm have changed recently. A randomized controlled trial conducted in Japan reported that the administration of clazosentan, an endothelin-1 receptor antagonist, reduced cerebral ischemic complications due to cerebral vasospasms and overall mortality rates for both direct surgery and endovascular interventions. 27 In the future, significant changes in medication therapy may influence the necessity and frequency of endovascular interventions performed as rescue measures. The application of novel endovascular devices may also be employed to treat vasospasms. The Comaneci device is a retrievable stent-type device designed to assist in the embolization of aneurysms. Salem et al. reported the effectiveness and safety of the Comaneci device for treatment of vasospasm based on outcomes in 40 patients with 122 vessels; no hemorrhagic complications occurred in this study. 28 Furthermore, the use of this device for treating distal vessels has also been reported. 29 The Comaneci device is not currently available in Japan, and PTA was performed using either compliant or noncompliant balloons in this study.
Limitations
This was a retrospective multicenter registration study, and the choice of treatment methods, treatment indications, and selection of devices and drugs were left to the discretion of the facilities and physicians. Image evaluation and symptom assessment were subject to judgments at each facility, which may have led to significant variability. In cases of PTA procedures, it is likely that some involve the concurrent use of intra-arterial vasodilators. However, detailed information regarding such cases was not fully collected. The collected data were mainly related to endovascular treatment, and other aspects of treatment, such as intravenous drugs and oral medications, were not investigated. The number of treatment sessions varied among patients; however, this study presented results based on each treatment procedure. The impacts of treatment frequency and the intervals between multiple treatment sessions on the final prognosis were not verified. In addition, the severity of subarachnoid hemorrhage, vasospasm-related symptoms, and the condition of patients before treatment were not investigated. Although local anesthesia may contribute more to symptom improvement compared to general anesthesia, the smaller size of the general anesthesia group and potential differences in severity and other factors should be considered. However, the possible confounding factors have not been examined and could not be excluded, which should be noted when interpreting the results. Improvements in neurological symptoms after treatment primarily focused on immediate improvements, and the duration of this improvement and its impact on outcomes were not examined. Finally, the data was from over 5 years ago, and there may have been differences compared to current treatment conditions and devices.
Conclusions
Our results demonstrated that endovascular treatment for cerebral vasospasm is safe and effective. Factors such as early intervention and treatment under local anesthesia may contribute to neurological improvements. However, caution is warranted for PTA due to the slightly higher incidence of hemorrhagic complications.
Footnotes
Acknowledgements
The JR-NET4 Study Group: Principal investigator, Nobuyuki Sakai, Kobe City Medical Center General Hospital, Kobe, Japan; Investigators, Koji Iihara and Hirotoshi Imamura, National Cerebral and Cardiovascular Center, Suita, Osaka, Japan; Akira Ishii, Kyoto University, Kyoto, Japan; Yuji Matsumaru, Tsukuba University, Tsukuba, Ibaraki, Japan; Chiaki Sakai, Kobe City Medical Center General Hospital, Kobe, Japan; Tetsu Satow, Kindai University, Osaka-Sayama, Japan; Shinichi Yoshimura, Hyogo Medical University, Nishinomiya, Hyogo, Japan; and Certified Specialist of Japanese Society of Neuroendovascular Therapy.
Consent for publication
Not applicable
Contributors
HH was involved in data acquisition, data analysis, drafting and critical revision of the manuscript. HI, NS, KI, AI, CS, TS, SY, HY, and YM were involved planning, conduct, conceptualization and design of this study. YI, MH, AM, and YM were acquisition of the data and critical revision of the manuscript. All authors reviewed the manuscript and approved the final version.
Declaration of conflicting interests
All authors who are members and nonmembers of the Japan Neurosurgical Society (JNS) have registered self-reported COI disclosure statements through the JNS website. Nobuyuki Sakai reports research grants from Biomedical Solutions, Medtronic, Terumo, and TG Medical; lecturer's fees from Asahi-Intec, Biomedical Solutions, Daiichi Sankyo, Kaneka, Medtronic, and Terumo; membership on the advisory boards for Johnson & Johnson, Medtronic, and Terumo outside the submitted work. Koji Iihara reports research grants from Idorsia Pharmaceuticals Japan Co., Ltd. Outside submitted work. Dr Satow reports a research grant from CANON medical systems, a lecturer's fee from Medtronic, and a consulting fee from Kaneka Medix. Dr Yamagami discloses research grants from Bristol-Myers Squibb; lecturer's fees from Stryker, Medtronic, Johnson & Johnson, Medico's Hirata, Daiichi Sankyo, Bayer, and Otsuka Pharmaceutical; and membership of the advisory boards for Daiichi Sankyo. The other coauthors have no conflict of interest for this manuscript.
Ethical approval and consent statements
This study was approved by the Institutional Review Board (IRB) of Kobe City Medical Center General Hospital (No.:zn200107). The Institutional Review Board at each center approved the retrospective use of patient data. An opt-out approach was used to obtain consent.
Funding
This study was supported in part by a research grant from the Japanese Society of Neuroendovascular Therapy and by the Kobayashi Foundation, Osaka, Japan.
Data availability statement
The data could be made available by contacting the corresponding author.