
Abstract
Background and purpose
Despite a rapidly growing body of literature supporting the treatment of chronic subdural hematoma (cSDH) with middle meningeal artery embolization (MMAE), real-life data is still scarce. This study aimed to evaluate MMAE radiological and clinical outcomes, based on radiological characteristics.
Materials and Methods
Fifty-two cSDH patients, treated by MMAE as a post-CSDH evacuation therapy in a single tertiary center, were included. Radiological outcome was evaluated with cSDH thickness/volume difference at routine follow-up compared to pre-MMAE CT head imaging. The cohort was divided into groups pertaining to cSDH laterality (bilateral and unilateral cSDH) and pre-MMAE hematoma thickness (>15 mm and ≤15 mm) for analysis. Patients who underwent evacuation after MMAE were not included in the analysis to eliminate bias of surgical effect on hematoma progression.
Results
Thirty patients had bilateral, and 22 patients had unilateral cSDH treated with bilateral and unilateral MMAE respectively. Twenty-nine patients had >15 mm pre-MMAE hematoma thickness, and 23 had ≤15 mm pre-MMAE hematoma thickness. Mean cSDH volume was lower at all follow-up intervals when compared to baseline and was reduced by a factor of 10 at the 3–6-month interval. The mean cSDH thickness was significantly lower at all three follow-up intervals when comparing each group (bilateral and unilateral MMAE) (pre-treatment hematoma thickness >15 mm and ≤15 mm). Larger hematomas with a thickness of >15 mm had a significantly greater reduction in mean cSDH volume interval follow-up than hematomas measuring ≤15 mm (1–3 months—63 mm3, 40.6–85.69, P < .001). Unilateral cSDH and MMAE demonstrated greater cSDH volume reduction compared to bilateral cSDH and MMAE at 1–3 months (42, 15.2–68.8, .001) and 3-6 months (33.7, 5.2-72.7, .043). No procedure-related major complications or deaths or recurrences were observed.
Conclusions
Adjunctive MMAE after surgical evacuation appears safe and effective. MMAE is particularly effective for larger pre-treatment hematomas >15 mm (compared to ≤15 mm) and for unilateral cSDH and MMAE (compared to bilateral cSDH and MMAE).
Keywords
Introduction
Chronic subdural hematomas (cSDHs) involve the collection of blood and blood products within the potential space between the meningeal layer of the dura and the subjacent arachnoid mater. 1
The exact pathophysiology of cSDH remains controversial and is thought to be a response to an initial trauma to the dural border cell layer—a fibroblast-rich layer at the junction of the dura and arachnoid matters. 2 A series of pro-inflammatory and pro-angiogenic cascades is subsequently triggered, resulting in the formation of membranes and neovascular networks. These fragile vessels are the presumed source of hemorrhage. The introduction of blood and blood degradation products into this cavity is thought to further propagate these inflammatory and angiogenic cascades resulting in progression and/or recurrence.3, 4
The current management of cSDHs is guided by clinical presentation. Patients with absent or mild neurological symptoms may be managed conservatively with routine clinical and imaging surveillance. If neurological symptoms are moderate or more severe, surgical evacuation is the mainstay of treatment. Various techniques including twist drill or burr hole craniotomy, mini craniotomy, or craniotomy may be used to evacuate the collection.5,6–7
Until recently, there was no treatment targeting the etiology of the chronic bleed resulting in progression, recurrences, and need for further evacuations.8, 9 Meta-analyses and more recently announced preliminary data from randomized control trials (RCTs) suggest that middle meningeal artery embolization (MMAE) for cSDH is safe and efficacious in preventing hematoma progression and reducing recurrence.10, 11 Although this treatment is becoming widely accepted as an adjunct to current surgical evacuation, many details remain unclear. 12
The objective of the study was to examine whether bilateral MMAE for bilateral cSDH offers a volume reduction benefit when compared with unilateral MMAE for unilateral cSDH and if the degree of volume reduction following MMAE is influenced by initial hematoma thickness. The secondary objectives of the study were to evaluate the safety and efficacy of MMAE in the treatment of cSDHs.
We hypothesized that bilateral MMAE and a lower pre-treatment hematoma thickness may each result in a larger volume reduction effect and that MMAE has a favorable safety and efficacy profile.
Methods
This retrospective cohort study reviewed all consecutive patients diagnosed with a cSDH and treated with MMAE at a single tertiary neuroscience center between January 2020 and December 2023. A STROBE checklist was used as a guidance throughout.
The inclusion criteria were patients with the diagnosis of cSDH and treatment with MMAE after recent surgical evacuation, accessible electronic medical records, available pre- and post-procedural CT head imaging data, and a minimum clinical and radiological follow-up of 4 weeks. The exclusion criteria were patients who required post-MMAE surgical evacuation and/or those with insufficient Digital Imaging and Communications in Medicine (DICOM) data.
Moreover, 59 patients were initially reviewed: 7 patients were excluded as they underwent surgical evacuation post-MMAE which would otherwise lead to selection bias and overestimate the volume reduction benefit in these patients. In the data collection period of the cohort, we observed no occurrences of redo evacuation following MMAE.
Procedural technique
Ipsilateral MMA embolization was performed after the exclusion of dangerous anastomoses on catheter and microcatheter angiography. The frontal and parietal branches of the MMA were embolized at the operator's discretion of embolic material such as particles (Contour PVA particles, 50–150 micrometer range, Boston Scientific), Squid 18 or 12 (Balt, Montmorency, France) or Onyx 18 (Medtronic, Dublin, Ireland) with or without augmented dual lumen balloon pressure cooker technique or adjunct coil embolization.
Imaging evaluation
All images were reviewed by an interventional and diagnostic neuroradiologist with over 5 years of dedicated INR experience. Procedural fluoroscopic images were reviewed to identify any intra-procedural complications including vessel perforation and non-target embolization. Hematoma dimensions were measured on the non-contrast CT heads performed immediately before MMAE and at routine follow-up based on local protocol (intervals of 1–3 months, 3–6 months, and 6–12 months). 13
cSDH volume was determined using the formula ABC/2.14, 15 cSDH thickness (A) was determined on a representative axial slice near the center of the hematoma and defined as the maximum distance measured as a perpendicular line from the inner table of the skull to the lateral surface of the cerebral hemisphere. cSDH length (B) was determined on a representative axial slice near the center of the hematoma and defined as the maximum distance measured as a straight line between each corner of the hematoma. cSDH height/depth (C) was calculated as the number of axial slices the hematoma is visualized on multiplied by the slice thickness.
cSDH progression was defined as an increase in the hematoma volume on any consecutive CT imaging.
Clinical evaluation
Clinical data were obtained from a medical center research database, patient's electronic medical records, and clinic notes. This included parameters such as mortality, modified Rankin scale (mRS) at admission and on follow-up, need for repeat surgery, and procedural complications (intra and post) which may not have been identified on procedural fluoroscopy.
cSDH recurrence is defined as an increase in the hematoma volume/neurological deterioration requiring further surgical rescue evacuation.
Dementia was defined as any patient with a clinical diagnosis by a neurologist at the time of MMAE. Hepatic disease was defined as any patient with persistently deranged liver function tests at the time of MMAE and for more than six consecutive months. Antiplatelet or anticoagulation use was defined as any patient taking one of these classes of medication (or a combination of such) at the time of MMAE.
Statistical analysis
Data were analyzed using IBM SPSS Statistics 29.0.2.0. Software. Categorical variables were described by frequency and percentage. Continuous variables were described by mean value, standard deviation, and confidence interval.
The reduction in hematoma thickness and volume was analyzed in patients who underwent bilateral MMAE vs. unilateral MMAE and in those with an initial hematoma thickness >15 mm vs. ≤15 mm.
For each group, a paired t-test was performed to compare cSDH thickness and volume pre- and post-MMAE. An Independent t-test was done to compare cSDH thickness and volume difference between the groups.
Statistical significance was set at a p value < 0.05
Ethics
The Institutional Research Ethics Board approved this study (ID: 24-5029, January 2024). All data were anonymized. Individual patient written consent was waived due to the retrospective nature of the study. This study was done in compliance with the Declaration of Helsinki (1964), its amendments, or similar ethical standards.
Results
A total of 52 patients were included for analysis. The mean age was 72 years old (range 26–91). The patients had a varied history, comorbidities, and medication use which are outlined in Table 1. These parameters did not significantly differ between the groups and/or were unlikely to have a substantial effect on outcome. A significantly higher prevalence of concurrent anticoagulation or antithrombotic therapy was observed in the CSDH thickness >15 mm group (chi-test, P < .05, see Table 1).
Demographic, clinical and treatment characteristics of the cohort.
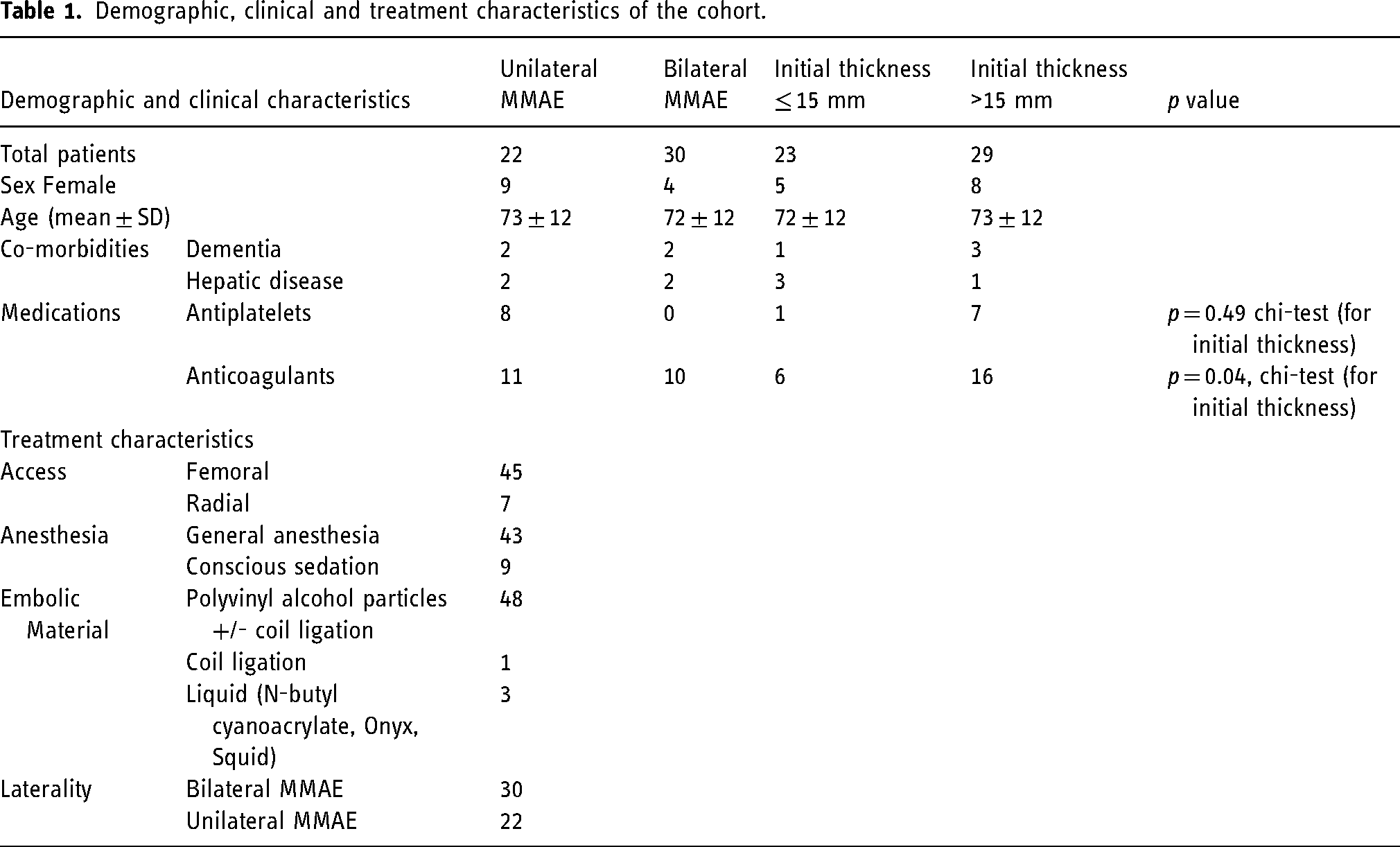
Thirty patients underwent bilateral MMAE, and 22 patients underwent unilateral MMAE. Twenty-nine patients had a pre-treatment hematoma thickness of >15 mm, and 23 cases (44.2%) had a pre-treatment thickness of ≤15 mm.
The mean pre-treatment hematoma thickness was 17.8 mm (range 3–35, SD 7.5). The mean pre-treatment volume was 100 mm3 (range 4–228, SD 49). At each consecutive follow-up time interval, there was a decrease in volume and thickness.
Forty-three cases were followed up at 1–3 months with a mean of 52 days, 22 cases at 3–6 months with a mean of 141 days, and 16 cases at 6–12 months with a mean of 251 days.
Difference in volume reduction in unilateral vs. bilateral MMAE
Unilateral MMAE demonstrated a greater reduction in hematoma volume at all time intervals when compared with bilateral MMAE. Strong statistical significance is seen when comparing the groups at the earlier 1–3 month follow-up interval (42% reduction, 95% confidence interval, 15.2–68.8, P = .001) and 3–6 months (33.7% mean reduction, 95% confidence interval 5.2–72.7, P = .043) and decreases at the later 6–12 month follow up interval (Table 2).
Independent t-test comparisons of volume reduction between unilateral and bilateral MMAE groups at three follow-up intervals.

Difference in volume and thickness reduction in pre-treatment hematoma thickness of >15 mm and ≤15 mm
MMAE in cSDH with an initial pre-treatment thickness >15 mm had a greater reduction in hematoma thickness and volume at all time intervals when compared with MMAE in cSDH with an initial thickness of ≤15 mm. This difference was statistically significant at all follow-up intervals (Table 3 and Table 4).
Independent t-test comparisons of
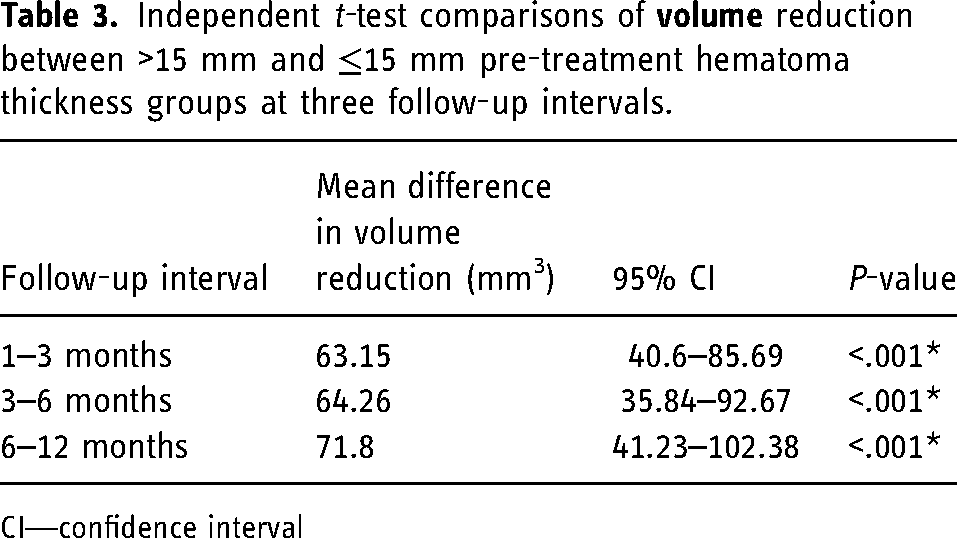
CI—confidence interval
Independent t-test comparisons of
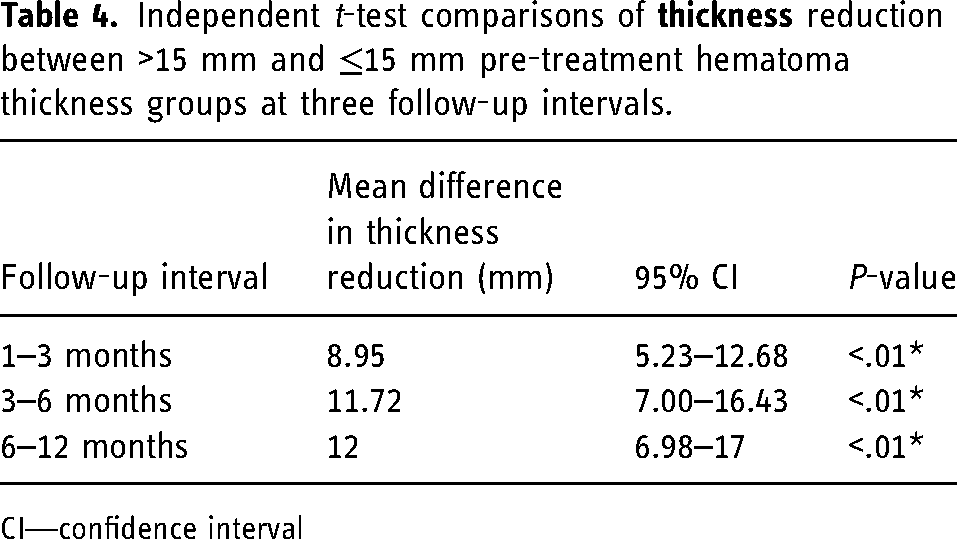
CI—confidence interval
The safety and efficacy of MMAE in the treatment of cSDH
There were no mortalities or major/long-term procedural complications (including non-target embolization or cranial nerve palsies) associated with the embolization procedure. Two patients (4%) had a minor procedural complication which was completely self-resolving. This includes a contrast-induced encephalopathy which resolved within 24 hours and a focal, non-flow limiting dissection of the common femoral artery.
No patients required rescue surgical decompression following MMAE. In addition, all patients with a baseline mRS of 0 remained at 0 on follow-up. All patients with a pre-MMAE mRS of ≤1 either improved or remained the same post-procedure. All 30 patients (58%) with a pre-MMAE mRS of ≥1 either improved or remained the same post-procedure. Of the 30 cases, 5 cases had mRS ≥3 at admission and all improved to mRS ≤2 restoring functional independence. This is summarized in Table 6.
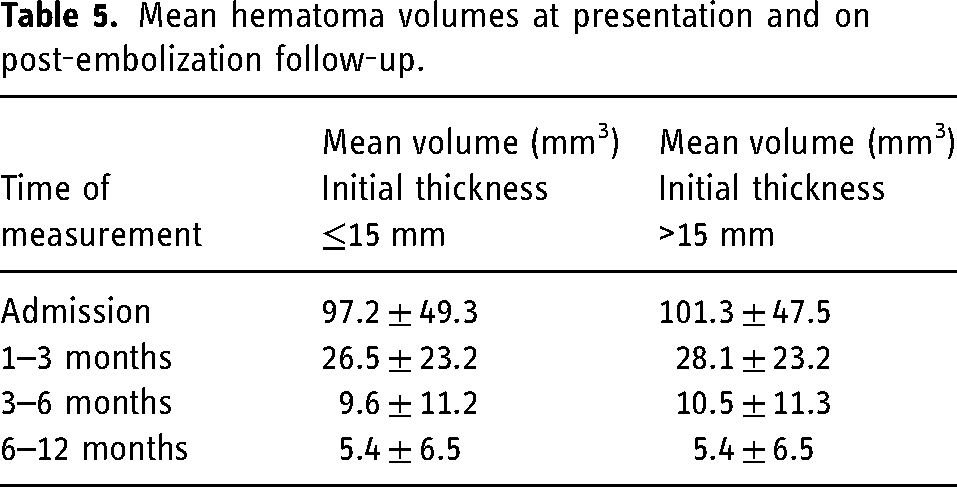
The progression rate of 0% was observed after 12 months of follow-up. This efficacy was deductedoncomparing the volume reduction within each cohort. Serial imaging follow-up consistently demonstrated a reduction in the volume or resolution of the hematomas. The mean cSDH volume was at a lower value at each follow-up interval compared to pre-MMAE volume as outlined in Table 5.
Mean hematoma volumes at presentation and on post-embolization follow-up.
Summary of efficacy and safety of the overall cohort (mRS—modified Rankin Scale).

Discussion
The advent of MMAE has initiated a paradigm shift in the standard management of chronic subdural hematomas. MMAE has established itself as a treatment option with a favorable safety profile. In our study of 52 patients, there were no recorded procedure-related mortalities or major complications when performed by an interventional neuroradiologist or endovascular neurosurgeon. This includes death and neurological morbidity including nerve palsies and ischemic stroke. This excellent safety profile is echoed in previous meta-analyses and the preliminary results of ongoing randomized control trials. 16
The degree of procedural efficacy and which patients would benefit the most from this treatment is yet to be clearly established. In our study, the mean cSDH volume was lower at each follow-up time interval when compared to baseline and was reduced by a factor of 10 at the 3–6-month interval (Table 5) We observed a 0% recurrence and progression rate which is certainly supportive of MMAE as an adjunctive therapy to standard management. This result should however be interpreted with some caution as it likely underestimates the true risk which is likely attributed to overall limited power of the study.
Recent preliminary data from randomized control trials including STEM, MAGIC-MT and EMBOLISE demonstrate that MMAE performed as an adjunctive or stand-alone treatment for cSDH has a recurrence rate ranging from 4.1% in EMBOLISE to 15.2% in STEM. This wide range is in part due to differences in trial designs including different conservative and surgical management protocols (e.g., burr hole and SEPS vs craniotomy—MMAE before surgery vs after) as well as differing definitions of progression and recurrence endpoints (e.g., 90 days vs 180 days). It is likely that the true recurrence and progression rates for cSDH treated with MMAE as an adjunct to surgical treatment will fall somewhere within this range. It is yet to be determined if MMAE as a stand-alone treatment for cSDH will have a similar outcome.
In our study, the mean cSDH thickness and volume were significantly lower at all three follow-up intervals compared to pre-treatment. This was observed with bilateral and unilateral MMAE, and for pre-treatment hematoma thickness of >15 mm, and ≤15 mm. Interestingly, our study demonstrated that larger hematomas with an initial thickness of >15 mm had a greater reduction in thickness and volume measurements at all follow-up intervals when compared to hematomas with an initial thickness of <15 mm (1–3 months—63 mm3, 40.6–85.69, P < .001). These results are contrary to our initial hypothesis that MMAE would be less effective in large hematomas.
These results are corroborated however by the preliminary data from the EMBOLISE trial which suggests that for MMAE performed as an adjunct to surgery, increased hematoma thickness at baseline is associated with almost a 4-fold reduction in NNT (from ∼16 to 4) from the smallest hematoma thickness to the largest in their cohort. EMBOLISE results also suggest that with higher sphericity (spherical in shape compared to thin and crescent) a similar reduction in NNT is seen therefore suggesting that MMAE is considered more effective in larger and more spherical hematomas. 16
Our findings suggest that MMAE is effective even at large hematoma volumes/thickness, particularly in the first 6 months. This should help guide patient selection and clinical decision-making going forward. This result may also suggest that MMAE as a standalone treatment may be theoretically possible, including for large-volume hematomas should the clinical presentation be mild. Although a dedicated RCT (standalone MMAE vs surgery with or without MMAE) is required.
In our study, it was demonstrated that unilateral and bilateral MMAE were both effective at reducing hematoma volumes and preventing recurrence and progression. Interestingly, unilateral MMAE demonstrated a larger volume reduction when compared with bilateral MMAE at all follow-up intervals. This was statistically significant at 1–3 months and 3–6 months Anecdotal experience outside of this cohort seemed to show that some patients with unilateral cSDH may benefit more from bilateral MMAE, with a lesser risk of recurrence caused by potential contralateral recruitment of dural vessels that could feed the cSDH membranes. Further trials will likely address this question.
It is unclear as to why there is a larger reduction in thickness and volume seen in the larger compared to smaller hematoma thickness groups and in the unilateral compared to the bilateral MMAE. We postulate that it may be due to the difference in dural blood supply and surface area available for the resorption of the hematoma.
We understand that the source of cSDH is a fragile neovascular network formed on neo-membranes, however the resorption process remains poorly understood. cSDH form within an inner avascular and an outer vascular hematoma membranes.17–19 Hematoma resorption is thought to occur by osmosis through venous and/or lymphatic vascular channels.18, 20 MMAE acts by occluding the fragile capillary hemorrhage points but also decreases the blood supply through the remainder of the dural arterial network 21 This reduction in arterial blood supply to normal dura might result in decreased venous drainage and may therefore slow the process of cSDH resorption.
In bilateral procedures, there may be a higher likelihood of drainage stasis due to decreased dural blood supply to the dural network which may result in decreased hydrostatic pressure and reduction of venous outflow. In unilateral procedures, the contralateral arterial blood supply remains patent, which may contribute to better drainage outflow and subsequent hematoma resorption. Additionally, bilateral subdural collection can also represent an alternative etiology of intracranial hypotension spectrum, which should prompt a different diagnostic and treatment approach. 22
Still, the exact underlying pathophysiology remains unclear, and this explanation is simply our postulation which requires further studies to understand the resorption process of cSDHs. Nonetheless, the results of this study, which are corroborated in some of the preliminary data released from recent RCTs, may begin to help identify which patients would benefit the most from MMAE and provide clinicians with guidance on patient selection.
A notable difference in our study compared with the RCTs is the choice of embolic material used. In our study, this choice was operator-dependent. We observed 92% of treatments performed with PVA particles ± coil ligation compared with liquid embolic used in the RCTs. Our series demonstrates that at the very least, particles have a similar safety and efficacy profile to liquid embolic described in the recent literature. Particles are easy to use and safe in experienced hands, providing clinicians with an economical alternative should this be required. The use of particles also eliminates the need for DMSO which may pose an issue if performing these procedures under local anesthesia and may also result in the need for multiple catheters and super-selective catheterization of each pedicle. 23 Recent analysis failed to show a differcne in efficacy or safety profile between particles and onyx. 24 Similarly, simple coiling of the MMA may potentially yield the same results 25 and needs to be further characterized in future trials to determine if one agent is more effective than another.
Limitations
The limitations of our study are its retrospective nature and inherent biases, including a relatively small cohort and non-uniform approach to MMAE timing and methodology in terms of embolic agent and MMA branches targeted, as well as the lack of a historic control group of patients who underwent cSDH evacuation without MMAE.
Conclusion
Taken together, the outcomes of our study are strongly supportive of MMAE as an adjunctive treatment to standard management of cSDH with a favorable safety and efficacy profile. Patients presenting with larger hematomas (thickness >15 mm) and those undergoing unilateral MMAE procedures demonstrate the most significant volume reduction. To conclude, considering data from recent randomized controlled trials, as well as real-life experience publications, the data presented in our study has the potential to influence the existing guidelines on CSDH management, adding adjuvant MMAE to prevent hematoma recurrence. In addition, focus of hematoma volume and thickness can drive further studies focusing on MMAE efficacy, with the latter being able to serve as robust markers of hematoma progression and regression.
Footnotes
Abbreviations
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.