
Abstract
Background
At our hospital, we use the flow re-direction endoluminal device (FRED) to treat vertebral artery (VA) aneurysms. Some reports suggest that the treatment efficacy of FRED may be lower in patients with fusiform-type aneurysms. At our hospital, we compared the treatment outcomes of FRED for both fusiform- and saccular-type aneurysms occurring at the posterior inferior cerebellar artery bifurcation.
Methods
We included 29 of 245 patients treated with FRED for VA aneurysms (9 saccular and 20 fusiform) between June 2020 and November 2022. We assessed occlusion rates and background factors, including age, sex, hypertension, diabetes, dyslipidemia, and smoking history. Patients received 100 mg aspirin and 3.75 mg prasugrel for at least 7 days prior to surgery. Non-responders received a loading dose of aspirin or prasugrel before surgery. Follow-up evaluations included magnetic resonance angiography (MRA) at 3 and 9 months and digital subtraction angiography (DSA) at 6 and 12 months. For patients with contradictions to DSA, MRI was used for follow-up if the aneurysm was visible. Additional FRED procedures were considered for patients with poor occlusion evidence at 6 months.
Results
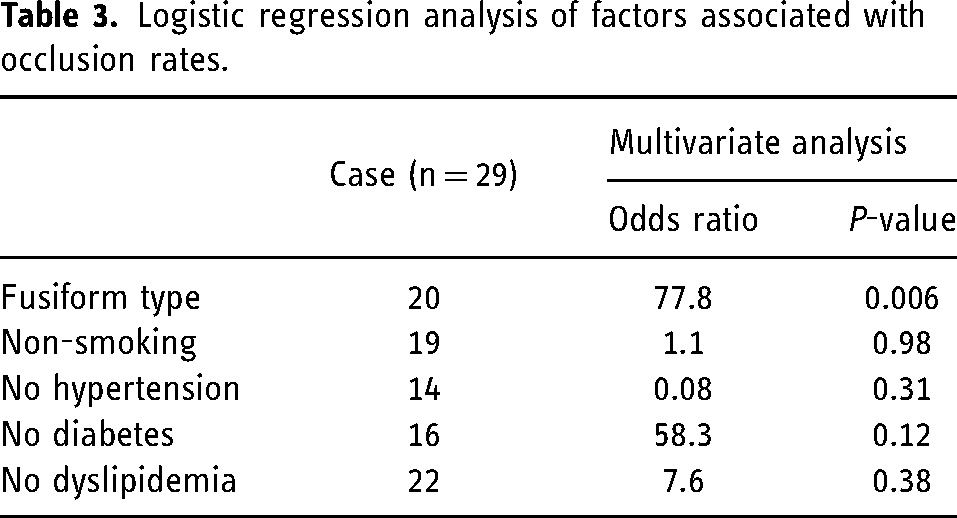
Patients with fusiform type were younger (P = 0.025), and their aneurysms were larger (P = 0.036) and had better obliteration rates (P = 0.007), compared with the saccular type. In the fusiform group, 18 out of 20 cases (90%) achieved good obliteration, whereas only 2 out of 9 cases (34%) in the saccular group did. Multivariate analysis indicated that fusiform aneurysm type was a significant predictor of good obliteration.
Conclusions
The treatment effect of FRED on the fusiform VA aneurysm appears to differ from the outcomes based on the pipeline device, suggesting the potential for achieving favorable results earlier in fusiform cases.
Introduction
Since the Pipeline Flex (Medtronic, Tokyo, Japan) was approved in 2015, the Flow-Redirection Endoluminal Device FRED (Terumo MicroVention, Tokyo, Tokyo, Japan) and Surpass Streamline (Stryker, Michigan, USA) instruments have also received approval. The indications for flow diverters (FD) have gradually expanded and now include treatment of blockages in the internal carotid artery (from the petrous part to the upper part of the floor) and vertebral artery, with FRED also being used for the middle cerebral and basilar arteries. Subsequently, the use of FD to treat vertebral artery (VA) aneurysms increased as well. There are reports that the treatment efficacy of FD is low in fusiform-type aneurysms. 1 Since its approval, we have been actively using FRED to treat VA aneurysms at our hospital. Here, we report the treatment outcomes for both fusiform and saccular-type aneurysms that occur at the posterior inferior cerebellar artery branch.
Material and methods
Patients
Of the 245 patients treated with FRED at our hospital between June 2020 and November 2022, 29 with vertebral artery aneurysms (9 saccular and 20 fusiform) were included in this study (Figure 1). All patients adhered to the FRED indication criteria, and had an aneurysm with a maximum diameter of 5 mm or more. We analyzed the occlusion rate of the aneurysms and the background factors in these patients. The background factors extracted included age, sex, presence or absence of hypertension, diabetes, dyslipidemia, and smoking history.
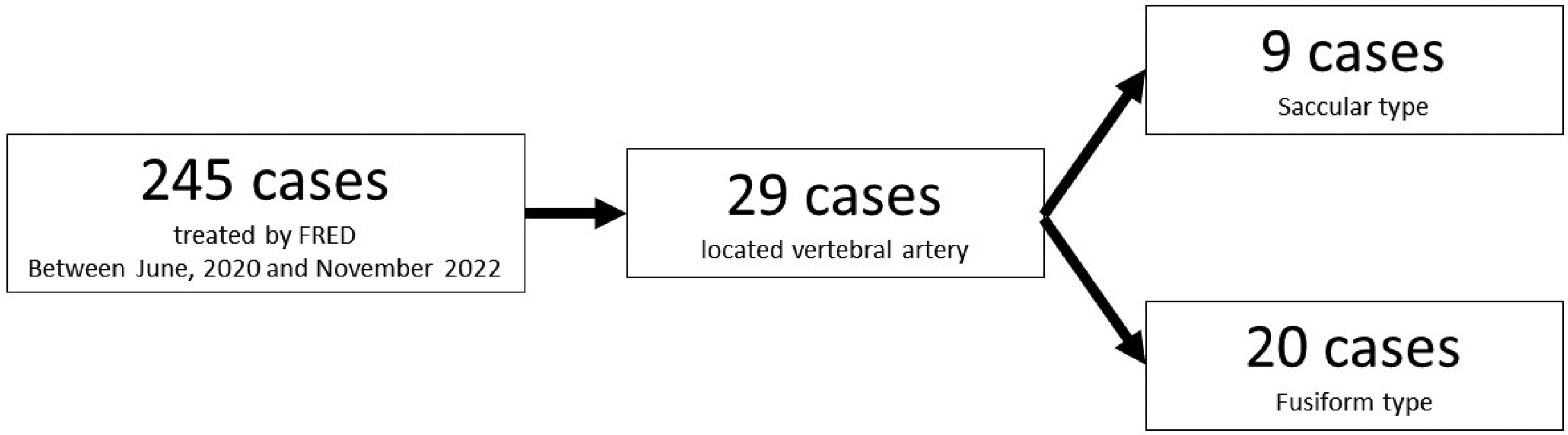
Patients background. Of the 245 patients treated with FRED at our hospital between June 2020 and November 2022, 29 with vertebral artery aneurysms (9 saccular and 20 fusiform) were included in this study.
Informed consent has been obtained from all individuals included in this study. The study adhered to the Declaration of Helsinki and was approved by the Ethics Committee (Approval No. 2020017).
Procedure
The patients were taking 100 mg aspirin and 3.75 mg prasugrel for at least 7 days prior to the operation. The onset of effect was evaluated using the VerifyNow Aspirin assay and VerifyNow P2Y12 (Accumetrics Inc, San Diego, CA, USA) before surgery. In the case of aspirin non-responders, a loading dose of 200 mg of aspirin was administered on the day before surgery, and in the case of prasugrel non-responders, 20 mg of prasugrel was administered on the day before surgery. The onset of effect was evaluated again on the day of surgery, and treatment was started when the onset of effect was favorable.
All patients received 5000 units of heparin intravenously in the form of a heparin-mixed saline solution that was administered via a perfusion line throughout the procedure.
We used a coaxial system with a 7-Fr Roadmaster guiding catheter (GOODMAN, Nagoya, Aichi, Japan), 5-Fr SOFIASELECT distal-access catheter (Terumo MicroVention, Tokyo, Tokyo, Japan), and Headway27 microcatheter (TERUMO, Tokyo, Tokyo, Japan). In all cases, only a single FRED device was placed.
Evaluation method
At our hospital, we followed up with patients who had undergone treatment for FRED using magnetic resonance angiography (MRA) and digital subtraction angiography (DSA). We performed MRA at 3 and 9 months and DSA at 6 and 12 months and evaluated the results. The DSA evaluation results were determined based on the O'Kelly–Marotta (OKM) grading scale 2 (Figure 2). In patients who were not able to undergo DSA due to various reasons such as contrast agent allergies, follow-up was performed using MRI alone only when the aneurysm could be confirmed on MRI. At 6 months post-treatment, if DSA shows no vascular stenosis, the regimen is switched to single antiplatelet therapy, which is then continued thereafter. In cases where there was little evidence of aneurysm occlusion on DSA at 6 months, FRED may have been performed again.
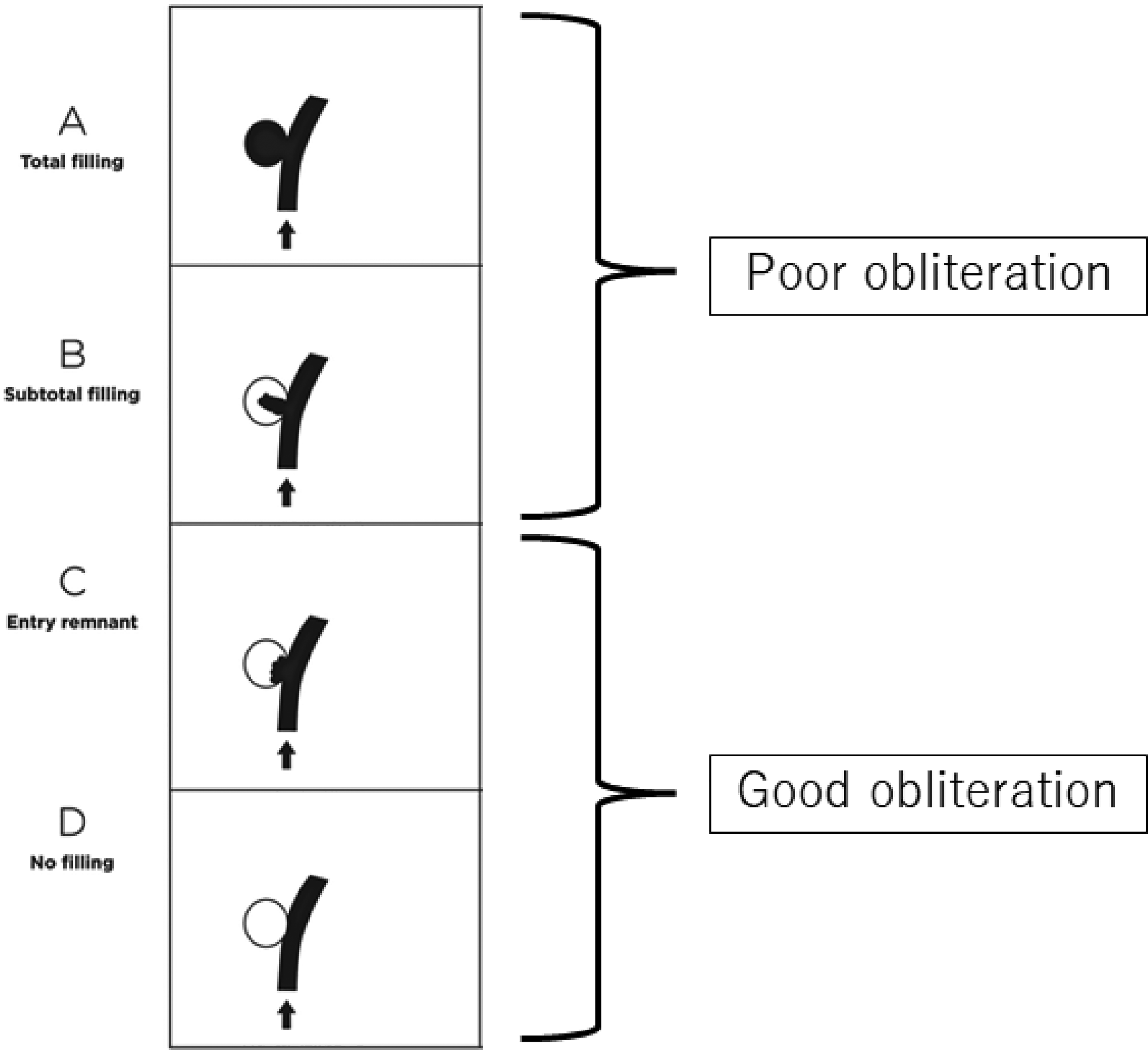
The O’Kelly-Marotta(OKM) grading scale. The group that was graded A or B on the OKM grading scale was classified as the poor obliteration group, and the group that was graded C or D was classified as the good obliteration group.
Statistical analysis
Statistical analysis was performed using JMP software, Version 14 (JMP Statistical Discovery LLC, Cary, NC, USA). The shape of the aneurysm was classified into two groups: saccular and fusiform. The occlusion rate was classified into two groups: OKM grades A and B as the poor obliteration group and grades C or D as the good obliteration group. Two groups were compared using the Chi-square and Wilcoxon tests. We analyzed the factors that contribute to the occlusion rate using logistic regression analysis. Statistical significance was set at p < 0.05.
Results
Patient background details are provided in Table 1.
Clinical characteristics of patients.
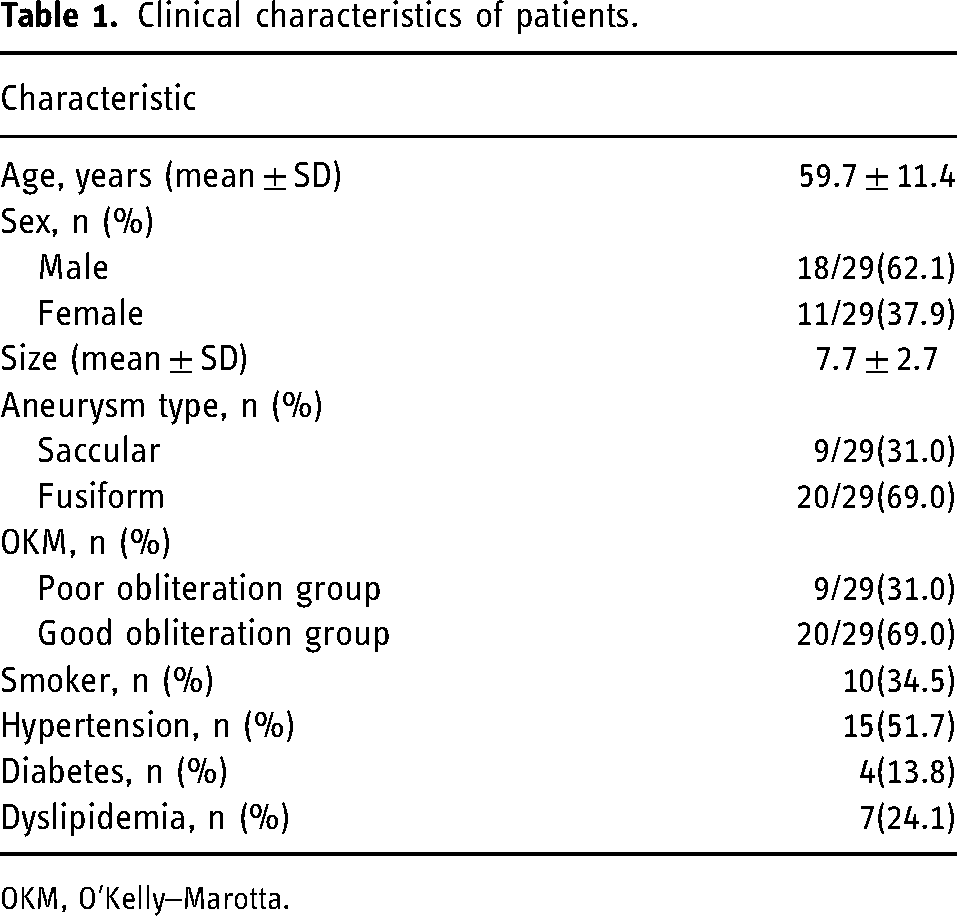
OKM, O'Kelly–Marotta.
The results of the comparison between various factors between the different aneurysm shapes are shown in Table 2. Patients with the fusiform type were younger (P = 0.025), and their aneurysms were larger (P = 0.036), and showed better obliteration (P = 0.007) than those with the saccular type. There were no complications associated with the treatment in either group. In the fusiform type, 18/20 cases (90%) were classified as good obliteration, whereas in the saccular type, this was only the case for 2/9 cases (34%). In the saccular group, all seven cases of poor obliteration were classified as OKM B, and none were classified as A. Reduction in the size of the aneurysm or intimal formation was observed. Specific examples of the saccular and fusiform types are shown in Figure 3. Multivariate analysis of the predictors of good obliteration showed that aneurysm shape was related to the fusiform type (Table 3).
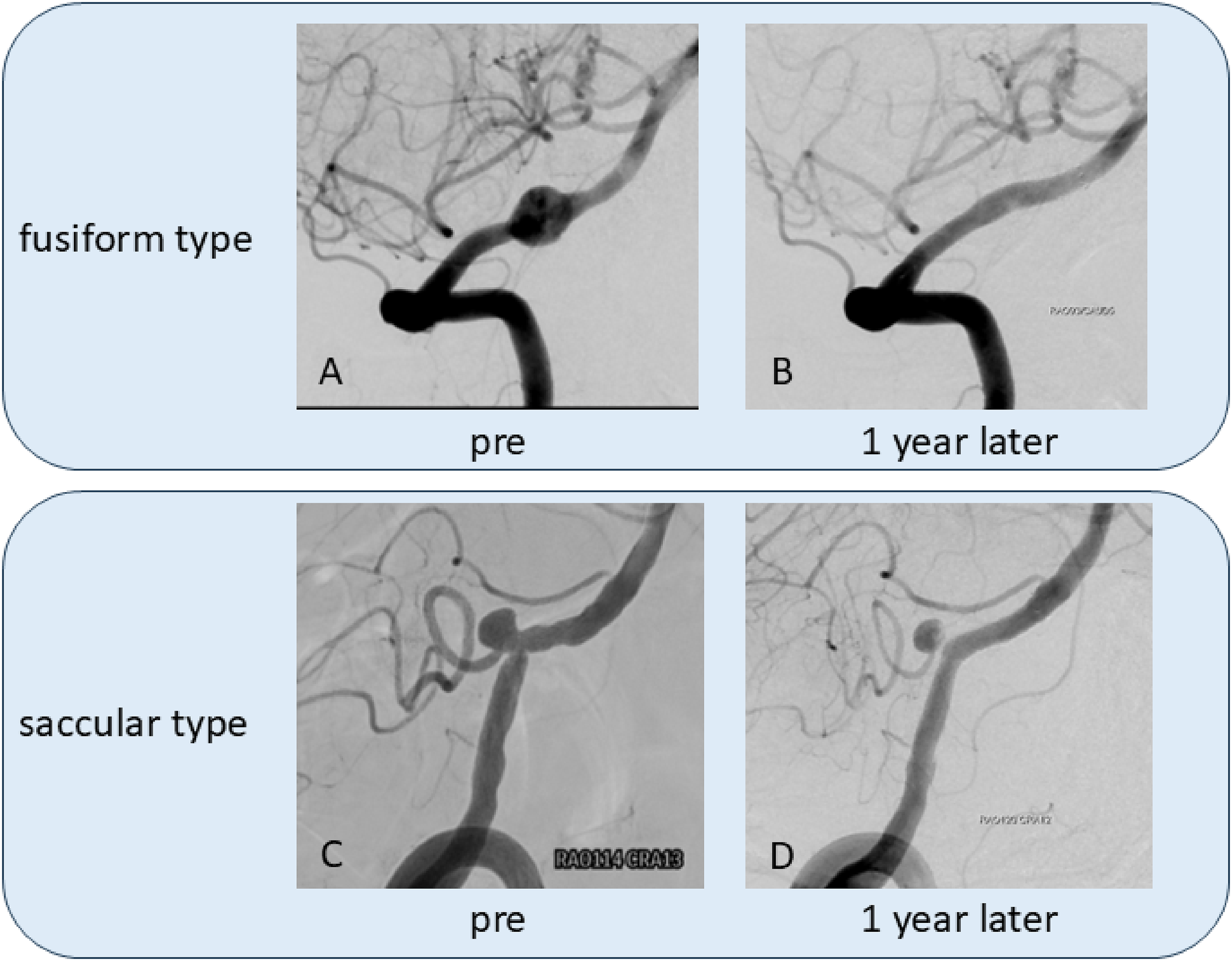
Representative cases of fusiform type and saccular type. A–B: 50-year-old male. FRED was implanted in a fusiform type aneurysm of 8.5 mm in the right VA. The aneurysm had disappeared on DSA one year later, and was judged to be OKM grade D. C–D: 69-year-old male. FRED was implanted in a 5.5 mm saccular type aneurysm in the right VA-PICA. One year later, DSA showed intimal formation in the neck of the aneurysm and a reduction in the aneurysm volume, but it was judged to be OKM grade B.
Comparison between the saccular and fusiform groups.
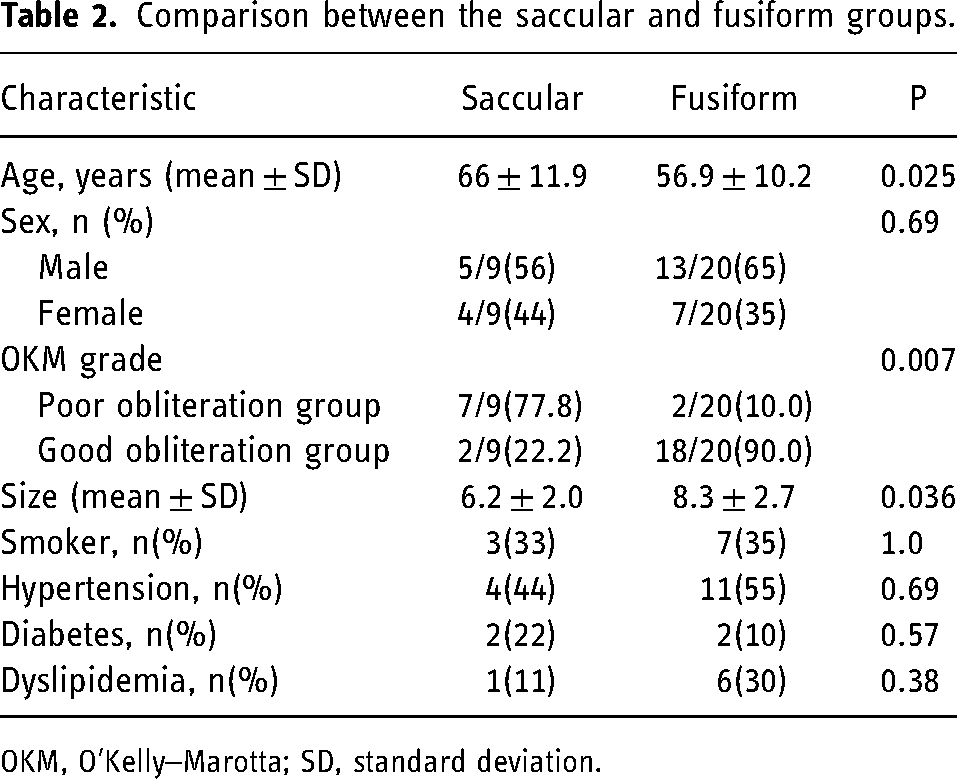
OKM, O'Kelly–Marotta; SD, standard deviation.
Logistic regression analysis of factors associated with occlusion rates.
Discussion
To date, the fusiform type has been cited as a predictor of incomplete obliteration of aneurysms using FD. 1 However, this study has shown the effectiveness of treating the fusiform type using the FRED. In the aforementioned study, a pipeline was used as the FD device, and it is possible that the differences in the characteristics of the devices led to the discrepancy between the findings of our study and their study. Stent placement for dissecting aneurysms is thought to change the blood flow into the aneurysm, and thrombosis is induced due to the stagnation of blood flow within the aneurysm, leading to occlusion. 3 One of the factors contributing to this is parent vessel straightening. 4 In this study, all fusiform-type cases that underwent FRED placement showed straightening, and we believe that this was one of the factors that led to a good obliteration effect. In addition, the VA is not surrounded by surrounding structures such as the dura mater and bone, and therefore is believed to be easier to straighten than the internal carotid artery.
In this study, patients with the fusiform type were significantly younger than those with the saccular type. Although dissection is thought to be one of the causes of fusiform-type aneurysms, 5 considering the age at which vertebral artery dissection commonly occurs, the fusiform type may also occur at a younger age. Incomplete obliteration is predicted in patients aged 70 years and over,6,7 and fusiform type aneurysms are more common in younger patients than saccular type aneurysms. Consequently, younger age is thought to be one of the factors that cause good obliteration. Notably, patients with large fusiform aneurysms with partial thrombosis were excluded from the study. Large aneurysms are considered a factor in incomplete obliteration, 8 and this may be one of the reasons for the fusiform type demonstrated higher treatment efficacy in this study.
In this study, the overall obliteration rate was 69%, which was slightly lower than that of the SAFE trial.9,10 One reason for this is that the majority of the saccular types showed poor obliteration. Notably, all patients with poor obliteration were graded as grade B on the OKM scale. Grade B is a broad category, with a range of 5–95% residual aneurysm volume. This study considered evaluations after one year, and all cases with grade B showed a reduction in the size of the aneurysm. It has also been reported that aneurysms close over time as evident during long-term follow-ups 1-year after FD treatment. 11 Additionally, it is possible that the OKM grading scale for the saccular type will improve if a longer-term course is followed up. However, the presence of branch vessels has been cited as a predictor of incomplete obliteration of the fusiform type,8,12,13 and this may contribute to the difference in occlusion rates between the fusiform and saccular types.
Limitations
The limitations of this study include the fact that it was a single-center, retrospective study with a small number of cases and that the maximum diameter of the aneurysms was 10 mm or less, which is considered small.
Conclusion
Our analyses reveal significant differences in treatment outcomes and challenge existing assumptions about the efficacy of FDs in fusiform aneurysms. We observed a high rate of successful obliteration in fusiform cases, suggesting that device characteristics may significantly influence treatment outcomes. These results will contribute to the ongoing discussion regarding optimal treatment strategies for various aneurysm types and highlight the need for further investigation into the factors affecting treatment success.
Footnotes
Author contributions
Kosuke Takigawa designed the study, the main conceptual ideas, and the proof outline. Yoshimasa Fukui, Kousei Maruyama, Takashi Fujii and Yoshiya Hashiguchi collected the data. Hidetoshi Matsukawa and Noriaki Tashiro aided in interpreting the results and worked on the manuscript. Kiyoshi Kazekawa supervised the project. Kosuke Takigawa wrote the manuscript with support from Masahiro Yasaka, Hiroshi Aikawa and Yoshinori Go. All authors discussed the results and commented on the manuscript.”
Consent for publication
Informed consent has been obtained from all individuals included in this study.
Consent to participate
Informed consent has been obtained from all individuals included in this study.
Data availability statement
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
The study adhered to the Declaration of Helsinki and was approved by the Ethics Committee (Approval No. 2020017).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.