
Abstract
Background and purpose
Meningiomas often contain a pial supply, and devascularization through preoperative transarterial embolization (TAE) is useful. However, the efficacy indicators of TAE for meningiomas with pial feeders remain unclear owing to their challenging quantification. Therefore, we propose a practical and quantitative intratumoral cerebral blood volume (CBV) from the pial supply, called pial-nCBV. This study aimed to identify the efficacy indicators of TAE against meningiomas in pial feeders using pial-nCBV.
Materials and methods
Between 2015 and 2021, 25 patients who underwent preoperative TAE and perfusion magnetic resonance imaging (MRI) for meningiomas with pial feeders were included in the study. We set 5 mm diameter round Region Of Interests as many as possible within the tumor at the border with the brain parenchyma, and calculated the intratumoral CBV from pial supply. The reduction rate was defined as primary outcome, termed Δ pial-nCBV. Additionally, we collected data on the injection behavior of the n-Butyl-Cyanoacrylate (n-BCA), including intratumoral embolization (IE) and feeder occlusion. We then analyzed the association between each variable and Δ pial-nCBV.
Results
The median Δ pial-nCBV was 25%. The n-BCA was applied in 22 (88%) cases, of which nine (36%) cases were injected into pial feeders. The use of n-BCA (p = .037), treatment with pial feeders (p = .002), and IE in meningeal feeders (p = .049) were associated with an increase in Δ pial-nCBV.
Conclusion
We proposed a practical indicator, pial-nCBV, and increasing Δ pial-nCBV was associated with treating pial feeder using n-BCA.
Introduction
Meningiomas often contain pial feeders, which also supply blood flow to the brain parenchyma.1–3 These pial feeders are associated with adhesion to the brain parenchyma and the development of brain edema around the tumor,3–5 resulting in difficulty in tumor removal. 1 Preoperative transarterial embolization (TAE) for meningiomas with pial feeders has been reported to be efficacious in reducing intraoperative blood loss.6–8 However, there are no reports addressing the indicators associated with the effectiveness of TAE for pial supplies. The complicated vascular dynamics of meningiomas with pial supplies, 8 makes it challenging to quantify the pial blood supply in meningiomas. Although devascularization during surgical removal is difficult to achieve, there are no robust indicators of the effectiveness of TAE for the pial supply of meningiomas.
The efficacy indicators of TAE is ambiguous, despite various findings based on angiography,9,10 gadolinium-enhanced lesion volume,1,11 and blood loss during surgical tumor removal.12,13 In recent years, cerebral blood volume (CBV) measured through perfusion magnetic resonance imaging (MRI) has gained significant attention.14,15 Intratumoral CBV is a valuable marker during tumor removal, facilitating accurate assessment of hemodynamics and demonstrating a correlation with intraoperative blood loss volume. 16 A previous study investigated the CBV in meningioma and found that the behavior of embolic agents were associated with effective TAE. 15 Intratumoral CBV may serve as a reliable indicator for assessing the hemodynamics of meningioma with pial feeders.
In this study, we propose a practical and quantitative intratumoral CBV from a pial supply, called pial-nCBV. We hypothesized that pial-nCBV would be useful for evaluating TAE in meningiomas with pial feeders characterized by complicated vascular dynamics. This study aimed to identify efficacy indicators of TAE for pial supply through pial-nCBV.
Materials and methods
Study design and patient selection
Between January 2015 and December 2021, we retrospectively evaluated 25 patients with meningiomas containing a pial supply. The patients underwent preoperative TAE and perfusion MRI before and after TAE. During the study period, 142 patients with meningiomas underwent tumor resection. Twenty-four patients were excluded without preoperative angiography, 82 patients were excluded without pial feeders, six patients were excluded without preoperative TAE, and five patients were excluded because of missing perfusion MRI data. Pial supply was defined as the presence of tumor staining through the pial artery, which is dedicated to the brain parenchyma. 1
Data collection
All data were obtained from medical and imaging records. We collected data on the following patient characteristics: age, sex, tumor side and location, presence of symptom, T2 low intensity, peritumoral edema, calcification, pial feeder supply, and tumor volume. Pial feeders were classified into three groups: the anterior cerebral artery (ACA), middle cerebral artery (MCA), and vertebral artery (VA). Tumor volume was defined as a gadolinium-enhanced lesion on a preoperative axial contrast-enhanced T1-weighted sequence (T1Gd) on MRI. We also collected intraoperative findings during TAE and tumor removal, including embolic agents, treated feeders, angiographic observations following the injection of n-Butyl-Cyanoacrylate (n-BCA), intratumoral CBV from the pial supply as described below, complications associated with the TAE procedure, operative duration, and blood loss volume. Angiographic observations following n-BCA injection were defined as intratumoral embolization (IE) or feeder occlusion (FO). 15 The angiographic observations and MRI findings were analyzed by two experienced neurosurgeons (TT and TN).
Embolization technique
Indications for preoperative TAE were determined by four neurosurgeons (NK, RH, YO, and NK) and three interventional neurologists (TN, MT, and HN) based on the angiographic findings, risk of the procedure, and potential benefits. All TAE procedures were performed under local anesthesia using a biplane neuroangiographic unit (Allura, Philips Medical Systems, Best, The Netherlands). During the procedure, the activated clotting time was maintained at approximately 250 s using intravenous heparin. Five, six, or seven French guiding catheters were positioned in the main trunk of the internal carotid artery (ICA) or external carotid artery using the femoral artery approach. The order of embolization of either the meningeal or pial feeder was determined individually for each case. We used n-BCA as the primary embolic agent because of its low rate of hemorrhagic complications and ease of injection into distal feeders.11,17,18 Informed consent was obtained from all patients to use n-BCA as an embolic agent for meningiomas. Pial feeders were exclusively embolized using n-BCA, while meningeal feeders were treated with a combination of n-BCA, embospheres sized between 300 and 500 µm, and coil. To achieve effective n-BCA injection, a DeFrictor Nano catheter or Marathon microcatheter (Medtronic, Minneapolis, Minnesota, USA) was guided into the feeder over a 0.010-inch micro guidewire. It was positioned immediately near the tumor and wedged into the feeder to prevent unintended n-BCA reflux.19,20 A 15–20% diluted and warmed mixture of n-BCA with Lipiodol (Lipiodol Ultra Fluide, Guerbet, Roissy, France) was injected under the digital subtraction angiography. 21 The coil or 300–500 µm-sized embospheres (Merit Medical, Salt Lake City, Utah, USA) were applied to meningeal feeders for which n-BCA was inapplicable.
Perfusion MRI
All patients underwent perfusion MRI and conventional MR pulse sequences, including axial T1WI, T2WI, T2*WI, FLAIR, and T1Gd, with a 3-T MR unit (DISCOVERY MR 750; GE Healthcare, Milwaukee, WI, USA) using a 32-channel head coil. Perfusion MRI was performed using a T2*-weighted, single-shot, gradient-recalled, echo-planar imaging (GRE EPI) sequence. Perfusion MRI sequence parameters were as follows: TR/TE, 2000/13.3 ms; matrix, 128 × 128; flip angle, 60; section thickness, 5 mm; and acquisition time, 90 s. The contrast was injected with a standard dose of 0.1 mmol/kg body weight of meglumine gadoterate at a rate of 2–3 mL/s, followed by a saline flush using a power injector.
Calculation of intratumoral CBV from pial supply
Given the inability to quantify the intratumoral CBV from the pial supply, we proposed pial-nCBV as a practical indicator, considering the dissected plane during resection.22,23 The measurement procedure for pial-nCBV is described in Figure 1. All protocols were performed using a Synapse Vincent volumetric analyzer ver3.0. First, we placed 5 mm diameter circular Regions of Interest (ROIs) along the tumor's border with the brain parenchyma, as many as possible, on each cross section of the contrast-enhanced MRI. 24 These ROIs were then replicated onto corresponding cross section of the perfusion MRI. Prior to copying the ROIs, we performed image fusion to align contrast-enhanced and perfusion MRI. As a reference, a 5 mm diameter round ROI was placed in the contralateral paraventricular white matter.16,25,26 We calculated the normalized pial-nCBV using the following formula: pial-nCBV = mean value of each intratumoral CBV/contralateral paraventricular white matter CBV. Pial-nCBV reflects CBV at the surface of the brain parenchyma.
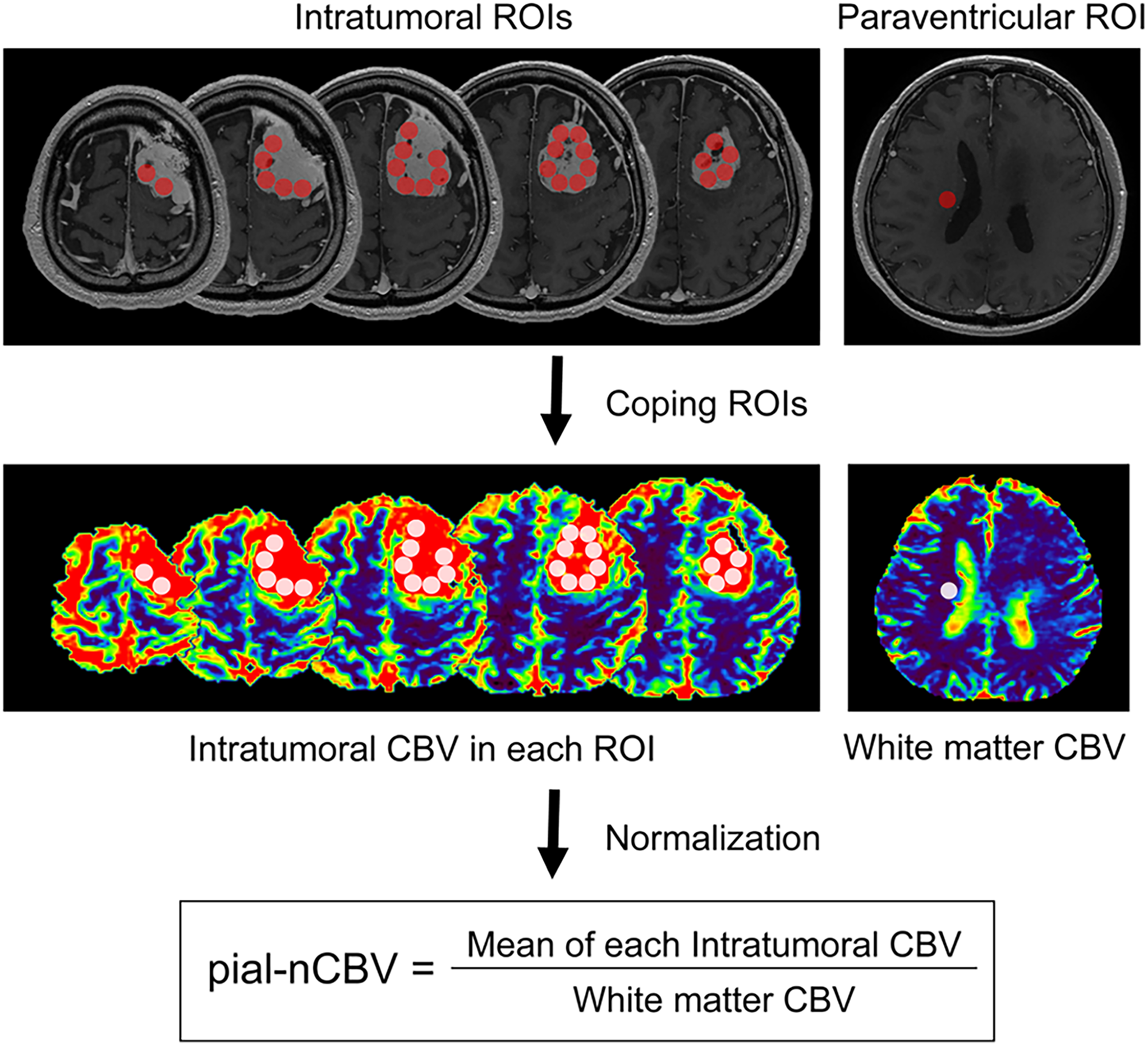
Measurement procedure for the pial-nCBV. We set 5 mm diameter round ROIs for the CBV measurements. In each cross section of the contrast-enhanced MRI, intratumoral ROIs (upper figure; red circle) were set as much as possible at the border with the brain parenchyma. A single ROI (upper panel, red circle) was placed in the contralateral paraventricular white matter as a reference. These ROIs were copied onto the perfusion MRI scans (lower figure, white circle). The mean of each intratumoral and white matter CBV was measured. Finally, normalization was performed and pial-nCBV was calculated using the following formula: pial-nCBV = mean value of each intratumoral CBV/contralateral paraventricular white matter CBV. All imaging analyses were performed using a Synapse Vincent volumetric analyzer ver3.0 (Fujifilm, Tokyo, Japan).
We also measured the pial-nCBV before and after TAE using perfusion MRI. Post-TAE perfusion MRI was performed 1–2 days after the procedure. Subsequently, we calculated Δ pial-nCBV as the percentage decrease in pial-nCBV, employing the formula: Δ pial-nCBV (%) = (1 − postoperative pial-nCBV/preoperative pial-nCBV) × 100. We set Δ pial-nCBV as the primary outcome as it quantified the TAE effectiveness of pial feeder.
Statistical analysis
All statistical analyses were performed using R 3.5.2 for Windows (www.R-project.org; R Foundation for Statistical Computing, Vienna, Austria). We conducted an analysis presence of each patient variable associated with Δ pial-nCBV. Categorical variables are presented as frequencies (percentages) and continuous variables as medians and interquartile ranges. Fisher's exact test was used to compare categorical variables, and the Mann–Whitney U test was used to compare continuous variables. The Kruskal–Wallis test followed by the Steel–Dwass post-hoc test was used to compare more than two groups. Spearman's rho correlation coefficient and Spearman's test were used to evaluate the correlations between continuous variables. Statistical significance was set at p < .05.
Results
Patient characteristics
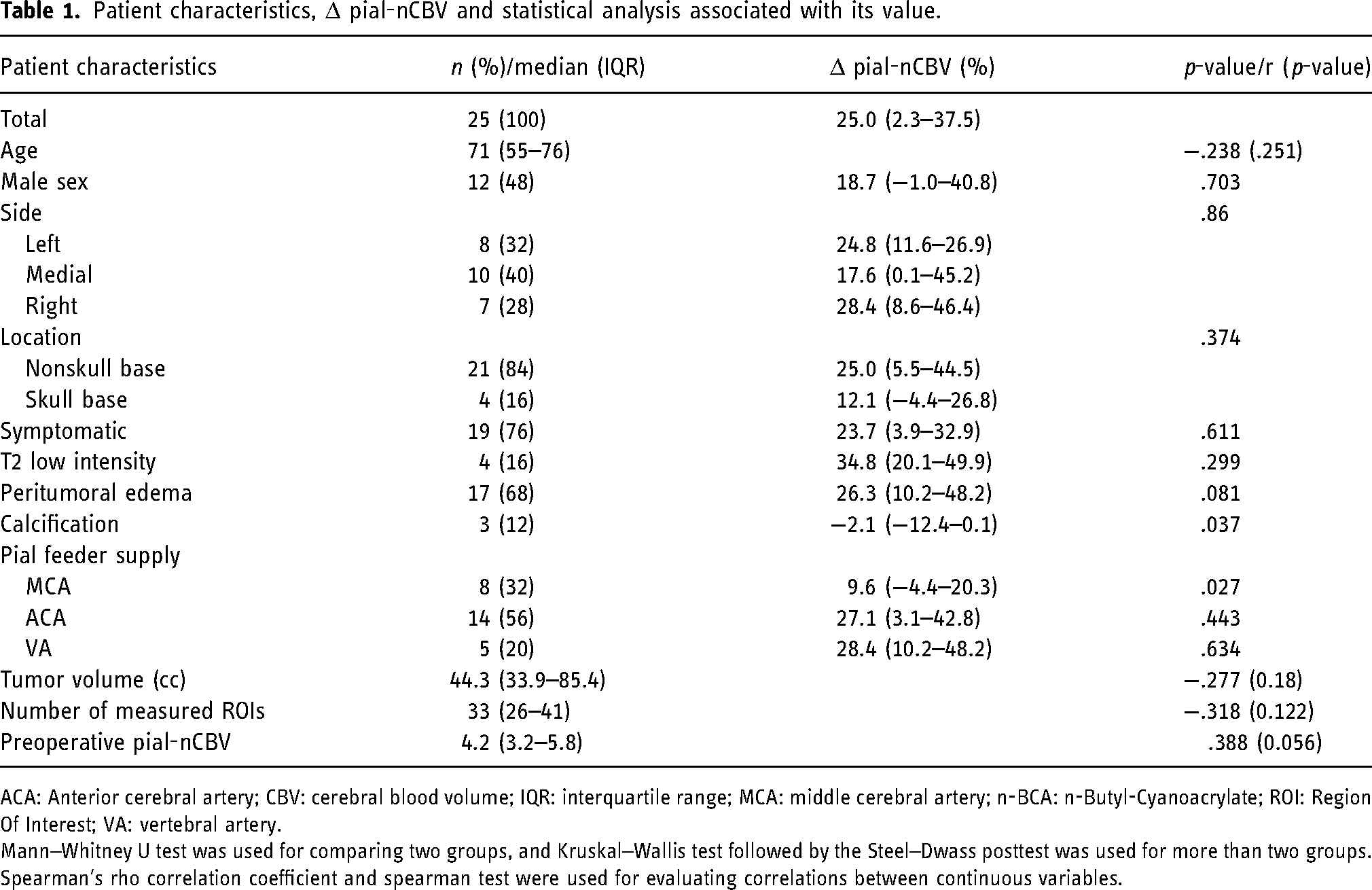
A total of 25 patients were enrolled in the study. Patient characteristics are presented in Table 1. The median age was 71 years and 12 (48%) were male. Nonskull base meningiomas accounted for 20 (80%) cases. Symptomatic patients were found in 19 (76%) cases, and edema around the tumor was in 17 (68%). The classification of pial feeders showed that ACA feeders were the most frequently observed in 14 (56%) cases. The median tumor volume was 44.3 cc. Intratumoral CBV data demonstrated that the median number of measured ROIs was 33, and the median preoperative pial-nCBV was 4.2.
Patient characteristics, Δ pial-nCBV and statistical analysis associated with its value.
ACA: Anterior cerebral artery; CBV: cerebral blood volume; IQR: interquartile range; MCA: middle cerebral artery; n-BCA: n-Butyl-Cyanoacrylate; ROI: Region Of Interest; VA: vertebral artery.
Mann–Whitney U test was used for comparing two groups, and Kruskal–Wallis test followed by the Steel–Dwass posttest was used for more than two groups. Spearman's rho correlation coefficient and spearman test were used for evaluating correlations between continuous variables.
Δ pial-nCBV and treatment outcome
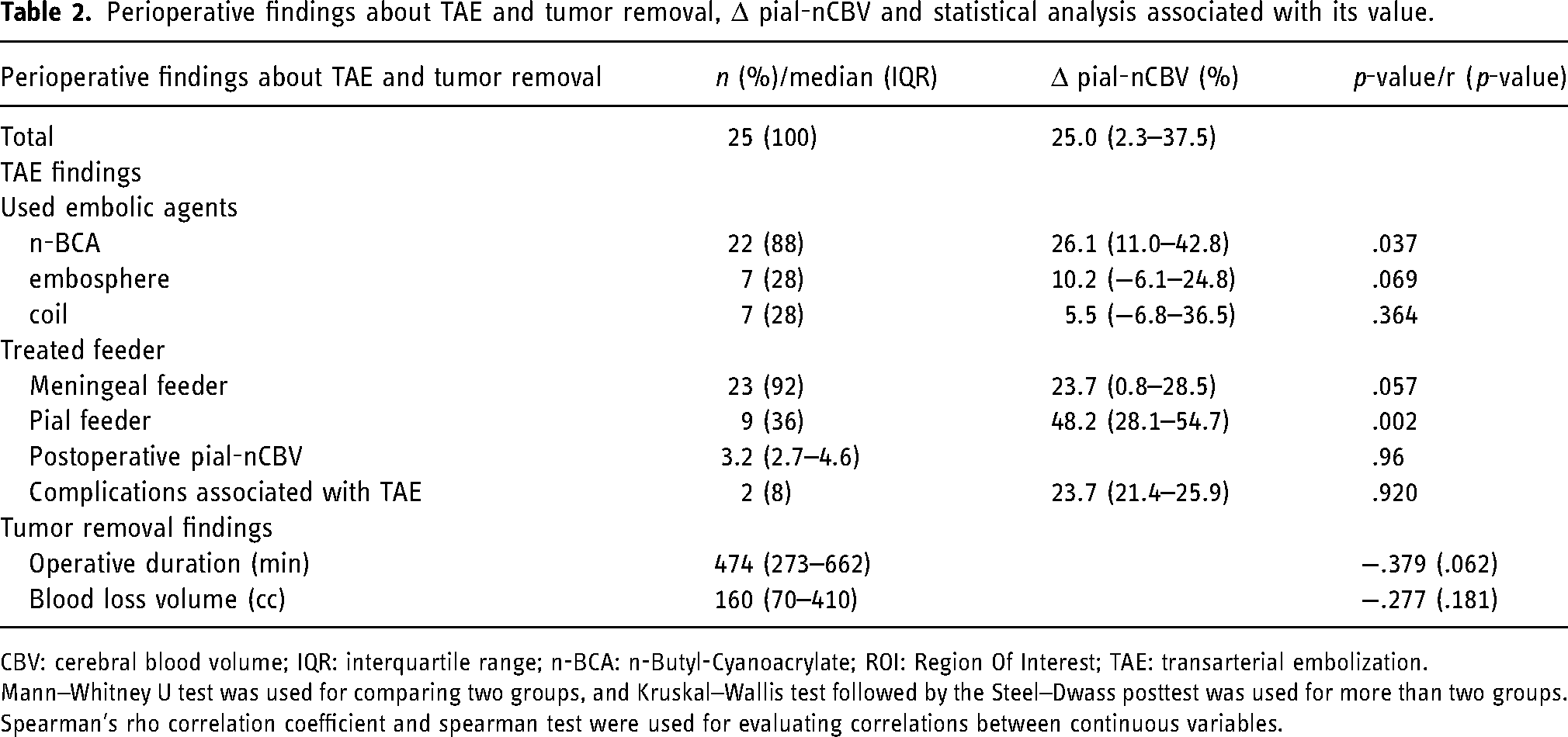
The perioperative findings regarding TAE and tumor removal are presented in Table 2. The n-BCA was applied in 22 (88%) cases, of which only nine (36%) cases were treated pial feeders. Six patients were treated with ACA feeders, and three cases were VA feeders. The coil and embospheres were applied only to the meningeal feeders, each of which had seven cases. The median pial-nCBV after TAE was 3.2, and the median Δ pial-nCBV was 25%. Procedural complications were found in two patients who were asymptomatic; one was an arteriovenous shunt, and the other was extravasation of the MMA. One patient presented with a shunt between the middle meningeal artery and vein, while the other presented with extravasation of the MMA. The median operative duration was 474 min, and the volume of blood loss was 160 cc.
Perioperative findings about TAE and tumor removal, Δ pial-nCBV and statistical analysis associated with its value.
CBV: cerebral blood volume; IQR: interquartile range; n-BCA: n-Butyl-Cyanoacrylate; ROI: Region Of Interest; TAE: transarterial embolization.
Mann–Whitney U test was used for comparing two groups, and Kruskal–Wallis test followed by the Steel–Dwass posttest was used for more than two groups. Spearman's rho correlation coefficient and spearman test were used for evaluating correlations between continuous variables.
Treating pial feeders increases Δ pial-nCBV (%)
To clarify the factors associated with the effectiveness of TAE for pial supply, we analyzed the relationship between several patient variables and Δ pial-nCBV (%). Decreasing Δ pial-nCBV (%) was associated with the presence of calcification (p = .037) or MCA feeders (p = .027) (Table 1), whereas increasing Δ pial-nCBV was associated with the use of n-BCA (p = .037) and treatment of pial feeders (p = .002) (Table 2). Representative TAE cases for pial feeders using n-BCA are shown in Figure 2. The number of ROIs, preoperative pial-nCBV, tumor volume, operative duration, and blood loss volume were not strongly correlated with the Δ pial-nCBV (Tables 1 and 2).

A representative case of meningioma with a pial feeder that underwent TAE targeting the pial feeder. (A) An adult patient with left falx meningioma in axial contrast-enhanced MRI (upper) and perfusion MRI (lower) before TAE. (B) Lateral view of the angiogram in left ICA before TAE. Tumor stain was supplied from the pial feeder branched off from left pericallosal artery. (C) Lateral view of the superselective n-BCA injection. The behavior of n-BCA showed IE. (D) Lateral view of the angiogram in left ICA after TAE, showing the disappearance of the tumor stain. (E) Contrast-enhanced MRI (upper) and perfusion MRI (lower) after TAE, with a calculated Δ pial-nCBV of 28.1%.
Achieving IE in meningeal feeders increases Δ pial-nCBV (%)
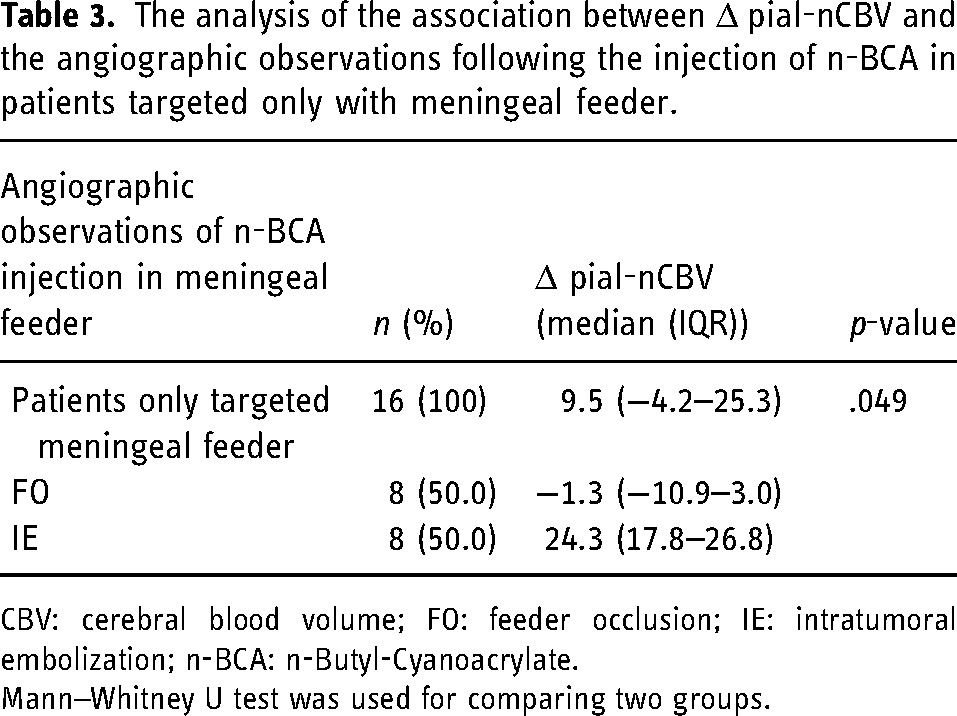
Although treating pial feeder was associated with increasing Δ pial-nCBV (%), only nine cases (36%) were found in this series, suggesting a limited indication. We then analyzed 16 patients who were targeted only by a meningeal feeder. We examined the association between Δ pial-nCBV (%) and angiographic observations after n-BCA injection. The median Δ pial-nCBV (%) with achieving IE in meningeal feeders was 24.3, whereas −1.3 with FO. There was a significant difference between the two angiographical observations (p = .049) (Table 3). These results suggest that achieving IE even in meningeal feeders could increase Δ pial-nCBV (%). Representative cases of IE in meningeal feeders are shown in Figure 3.

A representative case of meningioma with pial feeder that underwent TAE targeting the pial feeder. (A) An adult patient with a right falx meningioma, shown on axial contrast-enhanced MRI (upper) and perfusion MRI (lower) before TAE. (B) Lateral view of the angiogram in left ICA before TAE (left, arterial-phase; right, capillary-phase). Tumor was stained in the capillary-phase (arrowhead), and there were no feeder of sufficient intravascular diameter to guide a microcatheter. (C) Lateral view of the angiogram in left ECA before TAE. Tumor stain was supplied by the anterior convexity branch of middle meningeal artery and superficial temporal artery. (D) Lateral view of the superselective n-BCA injection from middle meningeal artery. The behavior of n-BCA showed IE. (E) Lateral view of the angiogram in left ECA after TAE, showing the disappearance of the tumor stain. (F) Contrast-enhanced MRI (upper) and perfusion MRI (lower) after TAE, with a calculated Δ pial-nCBV of 25.0%.
The analysis of the association between Δ pial-nCBV and the angiographic observations following the injection of n-BCA in patients targeted only with meningeal feeder.
CBV: cerebral blood volume; FO: feeder occlusion; IE: intratumoral embolization; n-BCA: n-Butyl-Cyanoacrylate.
Mann–Whitney U test was used for comparing two groups.
Discussion
We propose a practical and quantitative intratumoral CBV from a pial supply, called pial-nCBV. Additionally, we calculated Δ pial-nCBV (%) to represent the percentage decrease in pial-nCBV following TAE as efficacy indicators. The endovascular treatment of pial feeders is effective in increasing Δ pial-nCBV. Furthermore, achieving IE in meningeal feeders also increased Δ pial-nCBV, even if the pial feeder was untreatable. Focusing on intratumoral CBV from the pial supply is useful for evaluating the effectiveness of preoperative TAE.
pial-nCBV reflects blood supply in the parenchymal plane of the meningioma
We analyzed the CBV, which reflects the pial supply within the parenchymal plane of the meningioma. A previous study evaluated the intratumoral CBV from the pial supply by classifying the ROI based on the differences in perfusion curves obtained from perfusion MRI and angiography. 27 However, this study set a single ROI; thus, the total CBV from the pial supply was unclear. In this study, we spread 5 mm ROIs all over the brain surface for all axial perfusion MRI images and then calculated the average of all ROIs. Except for the involvement of meningeal feeders, our proposed measure has been previously reported for evaluating the pial supply. Although the accurate quantification of CBV from a pial feeder remains challenging and requires consideration of the involvement of meningeal feeders, our proposed measure of pial-nCBV serves as a practical indicator, focusing on the dissected surface of the tumor and brain parenchyma during surgical removal. This approach has the potential to provide a more refined evaluation of pial feeders than previous studies.
Treating pial feeder increases Δ pial-nCBV
We demonstrated that embolization of pial feeders increased Δ pial-nCBV. Interventional neurologists often hesitate to embolize pial feeders due to the risk of embolic material migrating into normal pial arteries through intratumoral anastomosis.28–30 However, embolization of pial feeders is a critical preoperative procedure, facilitating safer and facile tumor resection. This is attributed to their deep position within the surgical field, which presents challenges for dissection through arachnoid destruction or cerebral edema.1,3,5,7 In this study, successful embolization of the pial feeder with n-BCA was accomplished in nine patients, with no subsequent neurological complications. Appropriate selection of treatable pial feeders may be helpful in reducing the pial supply before tumor resection.
Using n-BCA increases Δ pial-nCBV
We demonstrated that n-BCA increased Δ pial-nCBV. In the pial feeders, only n-BCA was used as an embolic agent. The n-BCA, enable to injection through a microcatheter of thin inner diameter, facilitates the navigation of the catheter into diminutive pial feeders, a crucial aspect for their embolization. 11 Although applied on a limited nine cases, we embolized pial feeders only when the microcatheter was guided in the immediate neighborhood of the tumor and wedged in the feeder to prevent unintentional reflux of n-BCA. In contrast, using coils and embospheres was inappropriate for effective embolization because of the large diameter and multiple neovascularizations of the pial feeders. 8 Using n-BCA in preoperative TAE is suggested to be a valuable strategy for the embolization of pial feeders under appropriate conditions.
Achieving IE following the injection of n-BCA in meningeal feeders increases Δ pial-nCBV
We also demonstrated that achieving IE in meningeal feeders increased Δ pial-nCBV, regardless of the presence of treated pial feeders. A previous study demonstrated that achieving IE following the injection of embolic agents was associated with decreasing intratumoral CBV. 15 Furthermore, the injection of ethylene vinyl alcohol into the meningeal feeder copolymer obliterated the pial supply via the feeder network. 31 Compared to the particle embolic agents, n-BCA has the ability to achieve IE by high permeability. 17 Therefore, achieving IE with n-BCA may have resulted in a decrease in pial supply through the feeder network. We also revealed that achieving FO only in the meningeal feeder decreased the CBV. This result could be attributed to the subsequent increase in blood flow to the pial supply after TAE with meningeal feeders. 29 Our study suggests that achieving IE in meningeal feeders using n-BCA would provide an alternative to reduce the pial supply through the feeder network in cases of difficulty in treating pial feeders.
Limitations
There are some limitations in this study. First, we excluded patients with pial feeders who did not undergo TAE and those with missing perfusion MRI data. Therefore, we may have excluded patients who did not undergo angiography. Patient selection may have caused a selection bias. A prospective study is required to resolve this problem. Second, Δ pial-nCBV did not show strong correlation against operative time and blood loss. Although there is no definition of the effectiveness of TAE, these results should be considered carefully. Third, it is unclear why calcification and MCA feeders were associated with Δ pial-nCBV reduction. None of the patients with these factors was treated with pial feeders, suggesting a potential confounding factor. A multivariate analysis to reveal confounding factors was not appropriate for this study, which included only 25 patients. Therefore, further case studies are necessary. Finally, the pial-nCBV proposed in this study may not strictly reflect intratumoral pial supply. Our evaluation of CBV from the pial supply focused on the dissected surface of the brain parenchyma from a practical perspective, with tumor removal in mind. Consequently, we could not confirm whether all the CBV within the placed ROIs originated solely from pial feeders. Although previous study have shown that perfusion MRI can differentiate of pial and meningeal supply based on bolus passage at the blood–brain barrier, 32 it creates arbitrariness in the placement of the ROI. 27 Difficulty in accurate separation of the tumor region supplied by the pial feeder is a potential problem in CBV analysis.
Conclusion
We propose a practical indicator, pial-nCBV, as an intratumoral CBV from the pial supply. An increase in Δ pial-nCBV was associated with the treatment of pial feeder and achieving IE in meningeal feeder with using n-BCA, which serves as an alternative approach for treating pial feeders. Accumulating more case data with a focus on CBV may help further clarify the effectiveness of preoperative TAE in meningioma treatment.
Footnotes
Author contributions
Conceptualization: TT and TN; data curation: TT, TN, MT, YO, NKi, RH, YM, SY, TF, RN, TM, HN, and NKa; formal analysis: TT; investigation: TT, TN, MT, YO, NKi, RH, YM, SY, TF, RN, TM, HN, and NKa; methodology: TT, TN, AA, and HT; project administration: TT; software: TT; visualization: TT, TN, MT, YO, NKi, RH, YM, SY, TF, RN, TM, AA, HT, HN, and NKa; writing—original draft: TT; writing—review and editing: all authors; supervision: HK.
Data availability statement
The datasets analyzed during this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and informed consent statements
This retrospective study was approved by the Clinical Research Review Committee of Osaka University (Approval No. 14184-10).
Consent to participate
Informed consent was obtained in the opt-out approach.