
Abstract
Purpose
Intravenous (IV) thrombolysis and mechanical thrombectomy remain the only interventions shown to improve outcomes in acute ischemic stroke. This study evaluated the impact of commonly administered intraprocedural medications, each with putative neuroprotective mechanisms backed up by basic science literature, on outcomes in mechanical thrombectomy for acute ischemic stroke.
Methods and Results
A retrospective review of 284 patients utilizing univariate and multivariate analysis evaluated associations between administration of IV/intra-arterial (IA) tissue plasminogen activator (tPA), IV/IA heparin and IA verapamil as well as key outcomes: recanalization success, postoperative hemorrhage, and 90-day functional status. None of these medications were associated with favorable recanalization (TICI 2b/3) or functional outcomes (90-day modified Rankin score 0–2). IV tPA was associated with decreased rates of periprocedural hemorrhage (OR = 0.506, 95% CI [0.255–0.980], p = 0.046). Successful recanalization (OR = 2.22, 95% CI [1.03–.4.98], p = 0.046), presence of any hemorrhage (OR = 0.27, 95% CI [0.14–0.51], p = <0.001), lower age and lower NIHSS, were predictive of good outcome. Heparin was associated with an increased risk of hemorrhage (OR = 1.90, 95% CI [1.11–3.21], p = 0.02) and poorer outcomes (OR = 0.56, 95% CI [0.35–0.91], p = 0.018) in univariate analysis, with a similar trend in multivariate analysis (OR 0.57, 95% CI [0.30–1.06] p = 0.079).
Conclusion
Although several medications with basic science support for cerebroprotective effects are frequently administered during thrombectomy, the most effective strategies for improving functional outcomes remain prompt, successful recanalization and minimizing hemorrhage. With recanalization rates exceeding 80% and primarily determined by mechanical factors, targeting hemorrhage reduction appears critical for further outcome improvements. Evidence linking post-ischemic hemorrhage to blood–brain barrier disruption offers future avenues for research into interventions for this potentially reversible process.
Introduction
The advents of intravenous (IV) thrombolysis, endovascular thrombectomy, and, more recently, endovascular thrombectomy for large core infarcts have indisputably improved outcomes in acute ischemic stroke.1–5 However, even with optimal management, many patients still experience a significant decline in their functional ability. In the HERMES collaborative, rates of good functional outcomes, defined as modified Rankin score (mRS) 0–2, remain <50%. 6 This is supported by real-world data. 7 As such, there remains a need for neuroprotection to improve outcomes. Decades of neuroprotective therapies for acute ischemic stroke have been trialed, with the hope of providing improved outcomes via some form of cellular protection. Unfortunately, despite numerous promising candidates in animal trials, there has been no success in late-phase human trials aside from IV thrombolytics. 8
However, in the era of successful endovascular recanalization of large vessel occlusions (LVOs), there is renewed interest in adjunctive agents capable of preserving the integrity of the intracranial neurovascular bundle. Interventionalists routinely administer several intra-arterial (IA) medications during endovascular thrombectomy including tissue plasminogen activator (tPA), heparin, and verapamil. Each of these interventions have significant basic science evidence suggesting a cytoprotective effect but data on clinical outcomes related to these medications are mixed.9–12 These medications are given intraprocedurally for specific reasons, such as prevention of iatrogenic thrombi (heparin), vasospasm (verapamil), and to improve thrombolysis (tPA).
Here, we evaluate outcomes in patients who received any form of adjunct intra-procedural pharmacologic therapy while undergoing mechanical thrombectomy for acute large-vessel ischemic stroke at our institution in the era prior to large core thrombectomy. In addition, we use the term “cerebroprotection” in place of the more commonly used “neuroprotection” to highlight the need for preservation of not only neurons, but the adjacent vasculature and glial cells that comprise the intracranial neurovascular bundle. We believe this may be the key to bringing clinical outcomes in line with radiographic recanalization rates.
Methods
This is a retrospective exploratory analysis of our cohort of patients who underwent mechanical thrombectomy (n = 284) for LVO from August 2017 to September 2020. Details of the demographic, procedural, and outcome metrics for this cohort have been published previously. 9 All data were collected through retrospective review of the patients’ electronic medical records. The study was approved by the University of Rochester Research Subjects Review Board and was granted a waiver of informed consent. In this analysis, we evaluated the relationship among all infused medications, including IV and IA tPA, heparin, and verapamil, and two outcomes thought to represent cerebroprotection: absence of postoperative hemorrhage and good functional outcome. Hemorrhage includes both European Cooperative Acute Stroke Study (ECASS)-defined hemorrhage and subarachnoid hemorrhage (SAH). Good functional outcome was defined as mRS 0–2. Categorical variables were analyzed with a Chi-square test of independence or Fisher's exact test as appropriate. Continuous variables were analyzed with a Kruskal–Wallis test for three-way or greater comparisons. Univariate logistic regression was performed for relevant demographic, procedural, and outcome measures of good recanalization (TICI2b-3), good functional outcomes, and presence of hemorrhage. Candidate variables on univariate analysis with p < 0.2 were included in multivariate logistic regression model for predictors of postoperative hemorrhage and good functional outcomes. Adjustments to models were made with forward selection, using Akaike corrected Information Criteria to compare models, and variance inflation factors to evaluate for multicollinearity. Statistical significance was set at p < 0.05. Analyses were performed with Prism 10.2.2 (GraphPad, La Jolla, CA) and R-Studio (2024.12.0.467, R version 4.4.1). There was no follow-up with our patient cohort. We used the STROBE cohort checklist when writing our report. 13
Results
The cohort and subgroup demographics, comorbidities, procedural metrics, and outcomes are listed in Supplemental Table 1. There were 284 patients with a median age of 73 years [interquartile range—IQR 61, 83], 52% were female, and median NIHSS was 15 [IQR 11, 20]. This cohort precedes the large core thrombectomy era, so the median ASPECTS is 9 [IQR 8,10]. TICI 2b/3 recanalization occurred in 83.8%, with a hemorrhage rate of 30.2%. Outcomes were 90 day mRS 0–2 of 45.1% with a mortality of 21.5%. IV tPA was administered to 38% of embolectomy patients and was found to be inversely associated with hemorrhage in multivariate analysis (OR = 0.506, 95% CI [0.255–0.980], p = 0.046). There were no statistically significant differences in comorbidities between groups. There was a statistically significant lower rate of IV tPA administration for patients who received intraprocedural heparin in isolation (p ≤ 0.001). There was a statistically significant difference between groups for procedural metrics including time since last known well (LKWT) to recanalization, groin to recanalization, and number of passes. Patients who received heparin in isolation had a longer LKWT to recanalization time (median 534 min, IQR [265–962], p = 0.003). However, time from groin access to recanalization was lower in the heparin group (median 27 min, IQR [21–41], p = 0.002) (Supplemental Table 1). There was no relationship to recanalization (TICI2b/3) nor good functional outcomes (Table 1). Due to significant overlap in medications given during thrombectomy, we also performed analysis of patients who received heparin, IA verapamil, or IA tPA in isolation showed no statistically significant association with hemorrhage, TICI 2b/3 recanalization, or good functional outcome (mRS 0–2) (Supplemental Table 2).
Univariate analysis of periprocedural medications and three primary outcomes.
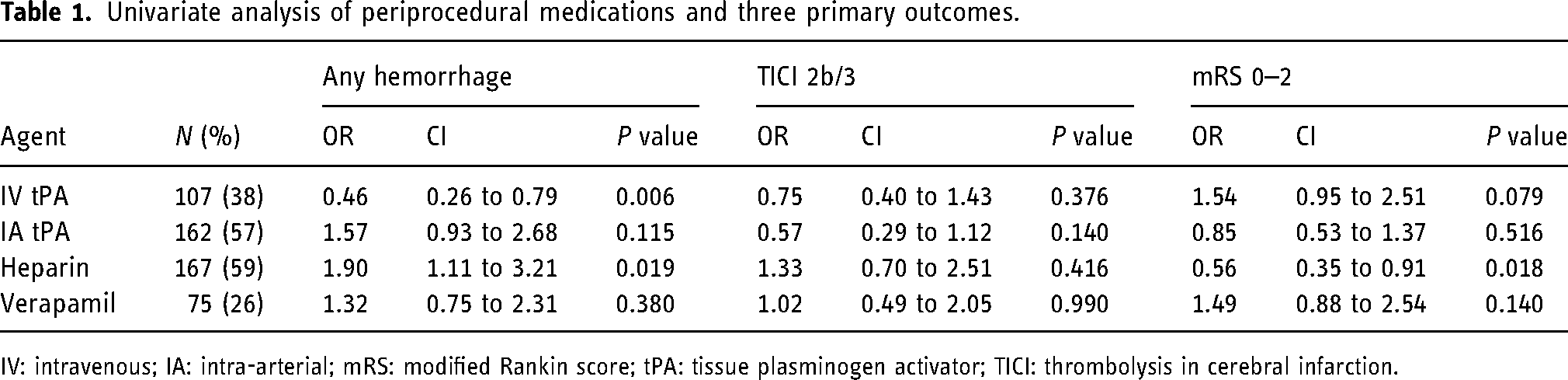
IV: intravenous; IA: intra-arterial; mRS: modified Rankin score; tPA: tissue plasminogen activator; TICI: thrombolysis in cerebral infarction.
Next, we evaluated the ways in which three intraprocedural medications were administered. IA tPA was used in 57% of embolectomy patients, with a wide range of doses, most frequently 5 mg (Figure 1). Heparin was used in 59% of embolectomies, with 5000 units being the most frequent dose. This was administered via the sheath (IA) or by the anesthesiologist (IV). IA Verapamil was used in 26% of embolectomy cases, most frequently 5 mg followed by 10 mg.
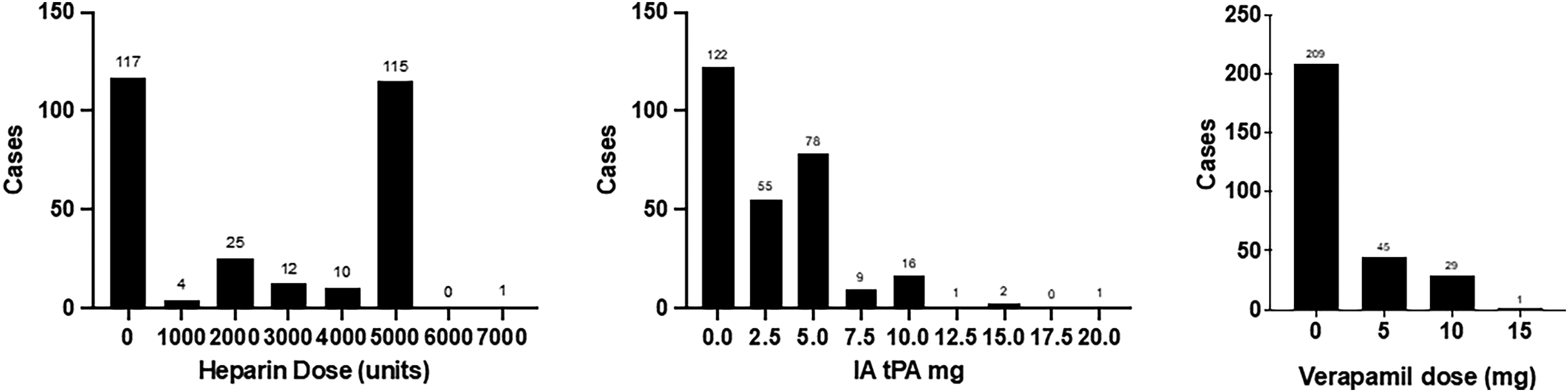
Frequency and dose of intra-arterial medications administered during mechanical thrombectomy.
We next evaluated the relationship of each medication to our outcomes. We focused on good clinical outcome (mRS 0–2) and on hemorrhage as none of the medications had statistical significance on recanalization in univariate analysis (Table 1). For IA tPA, there is no significant relationship to hemorrhage (OR = 1.57, 95% CI [0.93–2.68], p = 0.12), nor to good outcome (OR = 0.85, 95% CI [0.53–1.37], p = 0.52). Heparin is associated with increased hemorrhage on univariate analysis (OR 1.90, 1.11–3.21, p = 0.02) but this was not seen in the multivariate model. (Table 2). Heparin had a negative relationship to good outcomes on univariate analysis (OR = 0.56, 95% CI [0.35–0.91], p = 0.02). This lost significance in the multivariate model but continued to trend toward worse outcome (OR = 0.57, 95% CI [0.30–1.06], p = 0.14). IA Verapamil was not a significant predictor of any outcome on univariate or multivariate analysis.
Multivariate logistic regression model for good outcomes, defined as mRS 0–2.
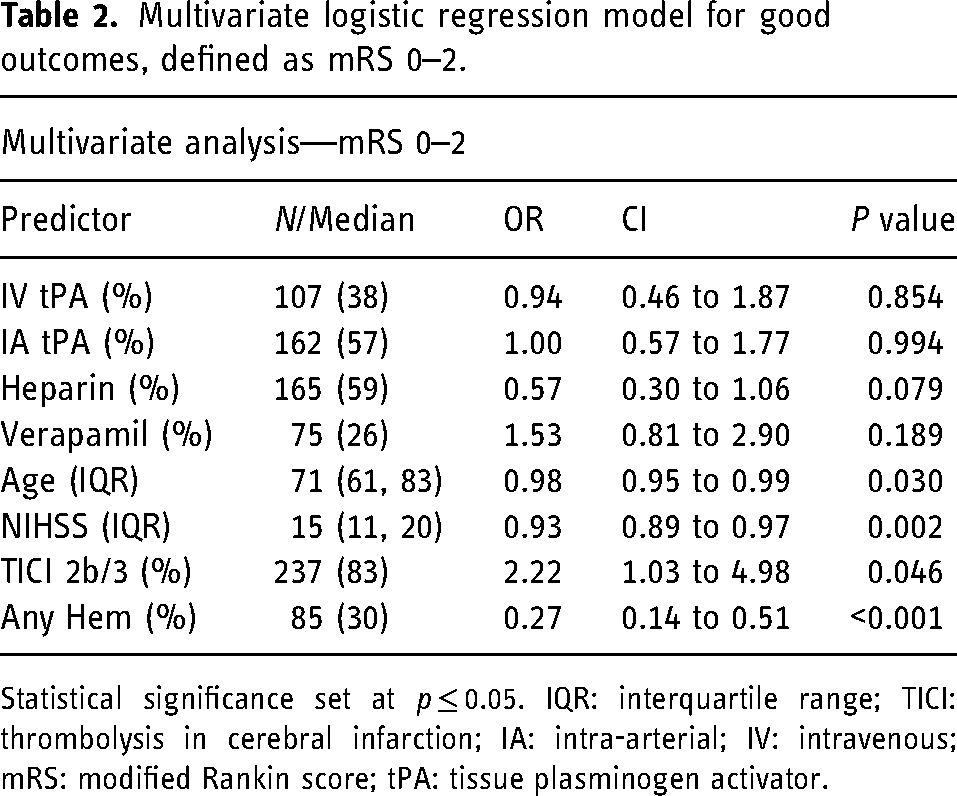
Statistical significance set at p ≤ 0.05. IQR: interquartile range; TICI: thrombolysis in cerebral infarction; IA: intra-arterial; IV: intravenous; mRS: modified Rankin score; tPA: tissue plasminogen activator.
In our multivariate model, successful recanalization (OR 2.22, 1.03–.4.98), presence of any hemorrhage (OR 0.27, 0.14–0.51), lower age and lower NIHSS, were significant predictors of good outcome when controlled for all of our candidate medications, as well as CAD, CKD, ICAD, DVT, smoking, preoperative anticoagulation medication, and primary aspiration technique (Table 2).
In the multivariate analysis for any postoperative hemorrhage, initially, IV tPA and history of smoking were protective, while a tandem lesion increased the odds of hemorrhage when controlled for candidate medications, and CKD. While none of the candidate medications were predictive of hemorrhage in this multivariate model, we speculated that tandem lesions, which are usually cervical carotid stenosis > 50% (Spearman r = 0.52, p < 0.00), might be associated with more medication use, particularly Heparin. However, no relationship was identified (Heparin OR = 1.44, 95% CI [0.70–3.12], p = 0.33). However, tandem lesions are associated with longer treatment times (OR = 1.01, 95% CI [1.00–1.02], p = 0.016).
To evaluate the possibility that IV tPA may be a surrogate for shorter LKWT, we added the LKWT to recanalization (minutes) to our multivariate model for any postoperative hemorrhage and found a better fit using Akaike's corrected Information Criteria. IV tPA was no longer associated with postoperative hemorrhage (as with all other candidate medications) while tandem lesion [OR 2.80, CI 1.23–6.40, P = 0.014], CKD[2.21, CI1.07–4.56, p = 0.031], smoking[OR 0.34, CI 0.11–0.89, p = 0.041], and LKWT to recanalization [OR 1.00, CI 1.001–1.002, P < 0.001] were significantly predictors of postoperative hemorrhage (Table 3). VIFs do not suggest collinearity (all <2).
Multivariate logistic regression model for any hemorrhage.
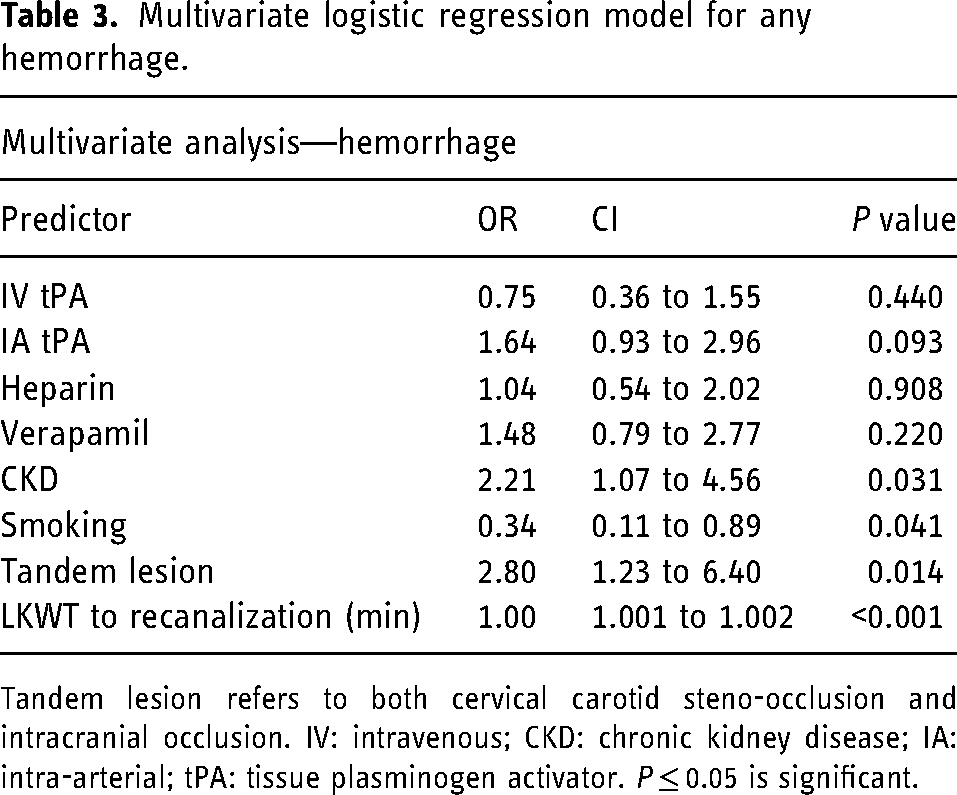
Tandem lesion refers to both cervical carotid steno-occlusion and intracranial occlusion. IV: intravenous; CKD: chronic kidney disease; IA: intra-arterial; tPA: tissue plasminogen activator. P ≤ 0.05 is significant.
Discussion
This single-center study representing a real-world cohort confirms that favorable recanalization strongly predicts good functional outcome. Thus, we can say that recanalization is the single most cerebroprotective measure in the absence of concurrent or subsequent hemorrhage. The publication of four trials of endovascular recanalization of large core infarcts provides additional support for the finding that taking a patient for endovascular intervention improves outcomes. 14 This raises questions whether the benefits arise purely from mechanical processes (e.g., recanalization and reperfusion), from putative cerebroprotective agents administered during the procedure, or from an unmeasured interaction between the process of thrombectomy and better outcomes (e.g., implicit bias towards post-embolectomy patients resulting in more intensive care and better likelihood of rehabilitation). This study attempts to address the second possibility by evaluating the use of multiple agents and their impact on standard outcomes of hemorrhage and mRS.
Pharmacologic intervention peri-procedurally does not improve outcomes
The presence of hemorrhage, favorable recanalization (TICI 2b-3), and good functional outcome (mRS 0–2) were the endpoints in our study. We examined the effect of tPA (both IV and IA), heparin, and verapamil on these endpoints. With TICI2b/3 rates of > 80% in our cohort and current literature, the focus of our study is on factors improving functional outcome, which lags at < 50% mRS 0–2 in recent metanalyses and in real-world studies such as ours.7,15–18 Mechanical issues such as technique have a significant impact on recanalization rates, however, hemorrhage and good outcomes may also be independently associated with pharmacologic agents. 19 In the present study, we see an effect with IV tPA in reducing the incidence of hemorrhage in multivariate analysis. We suspect this is primarily related to the early treatment window required for IV tPA administration within a cohort that includes both the early and late window. For functional outcome, we see potentially worsened outcomes with heparin (significant in univariate but not in multivariate analysis).
This finding is concordant with two recent studies which suggest that intraprocedural heparin worsens functional outcomes. MR CLEAN MED was a randomized control trial evaluating IV aspirin vs IV heparin peri-procedurally. 12 Despite improved 24-h recanalization with heparin, there is a nonsignificant trend towards worse clinical outcome, higher incidence of hemorrhage and worse functional outcomes with both agents. Wischmann et al. 11 performed a retrospective analysis of a large cohort which reports that periprocedural unfractionated heparin bolus had no benefit. When deploying MR CLEAN MED study inclusion (OR 1.44) to their cohort, they report worse outcomes. Further, when combined with IV thrombolytics, the odds ratio of worse functional outcome nearly doubled (OR 2.44). 11 Of note, however, the two studies differed in the application of heparin. Wischmann et al. utilized a heparin bolus (median dose 5000 units) given immediately after arterial access was achieved, consistent with our practice. In MR CLEAN MED, the heparin protocol was more complex, including a 5000-unit bolus, and a subsequent continuous infusion of two different doses for six hours. 12
Our group has previously evaluated IA tPA use as post-endovascular therapy and found no effect on hemorrhage, recanalization, or outcome. 9 The findings in the current study's multivariate model including other candidate medications continue to suggest that IA tPA has no impact on hemorrhage or functional outcome. Likewise, for verapamil, we find no association with recanalization, functional outcome, or hemorrhage in either univariate or multivariate models.
Basic science and clinical evidence for adjunct therapeutics in ischemic stroke
Heparin, tPA, and verapamil each have basic science studies supporting their putative cerebroprotective mechanisms. For example, there are endogenous forms of heparin with postulated anti-inflammatory properties apart from their anticoagulant interaction with antithrombin III (Hayman et al. 2017). Heparins have been shown to reduce lipopolysaccharide-induced nuclear translocation of NF-Kappa B, bind cellular adhesion molecules and inflammatory cytokines, and directly inhibit inflammatory mediators such as elastase and myelin basic protein. 20 Previous research has suggested a protective role for heparin in aneurysmal SAH, which shares several common mechanisms with ischemic stroke, including ischemia-associated reperfusion injury, oxidative stress, and blood–brain barrier (BBB) disruption. Our study suggests that the increased risk of periprocedural hemorrhage associated with peri-infarct heparin administration may offset its cytoprotective effects.
TPA also has endogenous forms and has activity independent of its proteolytic effect. Though it has been shown to increase NMDA-receptor signaling, which may cause harmful excitotoxicity, TPA has an antiapoptotic effect. 21 This may be dose dependent, such that low endogenous concentrations are protective but higher levels of exogenous TPA given for therapeutic reasons are neurotoxic. Exogenous IV tPA has become the standard of care for patients without contraindication and presenting up to 4.5 h after a confirmed ischemic insult. The administration of IA tPA during thrombectomy is not associated with improved functional outcomes. 9 In contrast, the CHOICE trial suggests a role for IA tPA following good recanalization. However, the doses of IA tPA used were higher (0.225 mg/kg in the trial, 15.75 mg for a 70 kg patient, maximum dose of 22.5 mg), and the trial was terminated early, with only a small fraction of angiographically eligible patients randomized. 22
Verapamil, a calcium channel blocker, has been particularly well studied as a translational agent for stroke. Maniskas et al. 23 and Fraser et al. 10 showed that verapamil has a dose dependent, U-shaped curve in reducing infarct volume in murine models of acute ischemic stroke. This was followed by a Phase I clinical trial, SAVER-I, demonstrating safety of IA infusion of 10 mg of verapamil in 11 patients. However, these observations have not been translated successfully to improved clinical outcomes in observational studies congruent with the results of the present study. There is also evidence that IA nitroglycerin reduces infarct volume in murine models, again with an apparent upper limit. 24
Recent neuroprotection clinical trials have all utilized IV access
Nerinetide, an eicosapeptide shown to reduce excitotoxicity through inhibition of post-synaptic density protein 95, demonstrated promise in pre-clinical stroke models of ischemia-reperfusion. However, it did not translate to improved functional outcomes in the ESCAPE-NA1 multi-institutional randomized controlled trial. 25 Important caveats to the ESCAPE-NA1 trial were the possibility of an interaction between neritenide and IV tPA in addition to the timing of neritenide administration relative to thrombectomy, two factors not controlled for in the trial. 8 Additional examples of clinical trials utilizing IV medications are CHARM, a Phase 3 study of IV Glibenclamide for cerebral edema after large hemispheric infarction, which has been terminated as of April 2024 and RODIN, a Korean trial studying the effects of the selective NMDA receptor antagonist, nelonemdaz.26,27
The IA route is readily available during endovascular therapies and despite the rise of endovascular recanalization as standard of care, little attention has been paid to this route of delivery. IA routes have allowed effective chemotherapy for some GI malignancies and retinoblastoma.28,29 It can produce a higher concentration of drug to the target while avoiding first-pass metabolism and limiting systemic toxicity. In neuro-oncology, the BBB must first be disrupted by one of several means to allow adequate central nervous system penetration. 29 However, therapeutic agents for acute ischemic stroke can easily bypass the BBB, which is disrupted by the ischemic event. In a rat reperfusion model, there is a biphasic opening of the BBB with ischemic insults. The initial opening occurs immediately after reperfusion, closes 1–4 h later and then reopens after 22 h. 30 BBB opening has been associated with hemorrhagic transformation. 31 In humans, DSC T2* weighted magnetic resonance imaging demonstrates reversible BBB disruption, and the degree of restoration correlates with the percent reperfusion. 32 Additionally, and relevant to endovascular techniques, regions with focal severe BBB disruption were at particularly high risk for hemorrhage with thrombolysis. Conversely, the disruption of the BBB can be harnessed as an avenue for treatment. Our study shows that postembolectomy hemorrhage is associated with poor outcomes, therefore, the most direct way to improve outcomes may be to direct therapeutics toward stabilizing or restoring the BBB. Using an IA approach would direct therapeutics to the region of interest and is routinely done with endovascular thrombectomy. However, most medications have a dose–response curve that transitions to a point of toxicity. This is demonstrated with multiple IA therapeutics including verapamil, nitroglycerin, and therapeutic hypothermia via chilled blood.10,24,33 Proposed therapies should be specifically evaluated for their IA pharmacokinetics and toxicity.
Distinguishing between an IV and IA administration is not necessarily obvious. One example is the most studied medication in stroke, heparin. While the use of heparin in our study and current literature, as previously discussed, is associated with worse outcomes, it has been shown to have an in vitro lytic effect. 34 Heparin is administered as a bolus during neurointerventional procedures either via the sheath (IA) or via IV bolus. In either case, heparin is functionally IV by the time it circulates to the cerebral vasculature, as it must pass through the liver and venous system before re-entering the arterial system. This perhaps accounts for some of the counterintuitive effect. It remains to be studied if delivering heparin bolus directly to the occluded artery (similar to IA tPA or IA Verapamil) may result in an improved effect or less harm. In our cohort, heparin was associated with longer LKWT to recanalization and a lower likelihood of receiving IV tPA thrombolysis despite faster recanalization times, which may explain the poorer clinical outcomes observed in the heparin group.
Our work coincides with the recognition that the ischemic cascade is multifaceted. The terms cerebroprotection or cytoprotection better reflect the understanding that all cells of the neurovascular unit, including neurons, astrocytes, microglia, endothelia and pericytes, are at risk.8,35 Different cell types react differently to ischemic stress and intervention, as demonstrated by a series of in vitro experiments that evaluated the responses of neurons, astrocytes, and endothelia to oxygen–glucose deprivation followed by “reperfusion” with varying degrees of hypothermia. 36 While neurons survived better with lower temperatures and longer durations of hypothermia overcame delays in cooling, astrocytes paracrine protection for neuronal culture was blunted by hypothermia. The recognition that the goal should be to address multiple cellular targets, each of which may have a particular window of opportunity for intervention, along with attention to dose–response effects and BBB penetration form the basis for STAIR XI recommendations. 37
Limitations
As a single-center, retrospective review, this study's findings may not be generalizable to other populations with differing patient demographics, clinical protocols, and procedural techniques. The sample size, while relatively robust may yet limit the power to detect smaller differences in outcomes related to IA pharmacologic interventions analyzed in this study. We suspect this is seen in the effect of heparin on bleeds and outcomes, in which larger cohorts of MR CLEAN and GSR-ET showed a clearer effect. Additionally, treatment decisions were not standardized across patients and reflect individual operator preference as it pertains to IA medication, choice of devices and techniques, as well as unselected case difficulty. Given the overlap of cerebroprotective medications administered to patients, our sub-group analysis of patients receiving each agent in isolation may be underpowered to detect true differences in outcomes and adverse events. Differences in IA intervention doses or administration timing may influence the efficacy of these interventions and were not controlled in this retrospective analysis. This is suggested in prior work by Kohli et al. and the CHOICE trial. Through this analysis, we identified a lack of standardization of how routine administration of heparinization is performed. As pointed out above, IA administration through the sheath is probably not a true IA administration with respect to the brain and is likely the same as IV administration by the anesthesiologist.
The role of time from last known well appears to be associated with the risk of hemorrhage. However, given that randomized trials and guidelines all support extended window intervention out to 24 hours, it remains unclear how much this highly significant variable ultimately impacts clinical practice.
The motivation for this post hoc evaluation came from the publication of multiple large core trials showing a significant effect favoring intervention. Our study reflects selection practice prior to the adoption of endovascular therapy for large-core infarcts. This introduces a homogeneity favoring smaller infarct size, but does not control for time to intervention, which included patients out to 24 hours. There may be a more complex interaction between infarct core and timing that would not be evaluated by a limited cohort.
Conclusion
Despite multiple agents both routinely used during stroke thrombectomy and demonstrating convincing pre-clinical efficacy for cerebroprotection, none are effective in improving real-world outcomes. Given that fewer than 50% of LVO patients undergoing mechanical thrombectomy achieve good functional outcomes despite over 80% recanalization rates, there remains opportunity to improve efficacy of mechanical thrombectomy via IA therapeutics. Our real-world data clearly supports recanalization as the single most cerebroprotective intervention we have. Given the negative effect of hemorrhage on outcomes, future cerebroprotection trials should focus on reducing hemorrhagic transformation via BBB stabilization strategies. This is probably best accomplished with an IA approach, which may optimize dose while minimizing systemic complications.
Supplemental Material
sj-xlsx-1-ine-10.1177_15910199251337167 - Supplemental material for In search of real-world cerebroprotection: An institutional perspective and review of the literature
Supplemental material, sj-xlsx-1-ine-10.1177_15910199251337167 for In search of real-world cerebroprotection: An institutional perspective and review of the literature by Lewis JR Thompson, Taylor Furst, Racquel Whyte, Gurkirat S Kohli, Derrek A Schartz, Tarun Bhalla, Vincent N Nguyen, Matthew T Bender and Thomas K Mattingly in Interventional Neuroradiology
Supplemental Material
sj-xlsx-2-ine-10.1177_15910199251337167 - Supplemental material for In search of real-world cerebroprotection: An institutional perspective and review of the literature
Supplemental material, sj-xlsx-2-ine-10.1177_15910199251337167 for In search of real-world cerebroprotection: An institutional perspective and review of the literature by Lewis JR Thompson, Taylor Furst, Racquel Whyte, Gurkirat S Kohli, Derrek A Schartz, Tarun Bhalla, Vincent N Nguyen, Matthew T Bender and Thomas K Mattingly in Interventional Neuroradiology
Footnotes
Author contributions
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request. Additionally, previous analyses of this data set are referenced within the manuscript.
Declaration of conflicting interest
The authors have no disclosures or conflicts of interest to report.
Ethical approval
The studies involving humans were approved by Research Subjects Review Board—University of Rochester. The studies were conducted in accordance with the local legislation and institutional requirements.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
The University of Rochester Research Subjects Review Board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because this study was exempted under category 4, as this was secondary research using de-identified patient data (Study ID: STUDY00004702). The data were anonymized in a way such that subjects could not be identified directly through identifiers linked to the subjects; the authors of this article did not contact the participants, and data were retrieved through chart review. All direct identifiers have been removed from this manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.