
Abstract
Stent-retriever-based mechanical thrombectomy (MT) is an effective treatment for acute ischemic stroke (AIS) caused by large vessel occlusion (LVO). First-pass effect (FPE) is one most powerful predictors of positive outcomes in LVO AIS patients treated with MT. We performed an independent central reader review of our prospectively maintained database to identify all patients treated first with the NeVa stent retriever at our single high-volume Comprehensive Stroke Centre.
Overall, 89 patients met our inclusion criteria. The median age was 73 yrs (range 28–88; 52% male). The median presentation NIHSS was 16 (range 5–30) and 49% received IV tPA prior to MT. 93% of target occlusions were in the anterior circulation (n = 83) with a median ASPECT score on plain CT of 8 (range 5–10). A Balloon Guide Catheter (BGC) was used in 80% of cases and a distal aspiration catheter was used in all cases. Longer NeVa models (≥29 mm) were used in 89% of cases. FPE was demonstrated in 57% of cases (eTICI score of ≥2c) with modified FPE demonstrated in 65.1% of cases (eTICI score of ≥2b (67%)). A final eTICI score of ≥2c was achieved in 87% of cases. Good functional outcome (mRS ≤2) was achieved in 40% of patients (n = 81).
The NeVa stent-retriever has a very high rate of FPE and final recanalization in this real-world cohort of patients from the NeVa One registry. These results are higher than those previously published and may support longer NeVa device use with a BGC and proximal aspiration to optimize FPE.
Introduction
Since the publication of the seminal trials several years ago,1–5 mechanical thrombectomy (MT) has become the gold standard treatment for acute ischaemic stroke (AIS) caused by large vessel occlusion (LVO). Further studies demonstrated the efficacy of the procedure in patients presenting beyond 6 hours6,7 and more recent studies demonstrated a positive effect in basilar artery occlusion and patients with large core infarction8,9
Over the last decade, our understanding of clot types 10 and stent-retriever–clot interaction11–13 has improved significantly. We have also gained further insights into how both the stent-retriever and the clot interact with the vessel wall during retrieval. 14 This improvement in our overall understanding has led to the development of stent-retrievers with distinct designs.
Optimizing the FPE is one of the major goals in mechanical thrombectomy. As previous studies have shown, this increases the chance of a good functional outcome at 90 days 15 and consequently has a more favourable health economic benefit.16,17 A recent study by Jadhav et al. demonstrated that patients undergoing MT and achieving FPE had a higher rate of 90-day mRS 0-1 (52.6% vs. 38.6%), higher rates of mRS 0-2 (65.4% versus 52.0%, P = .003), and lower 90-day mortality (12.0% versus 18.7%, P = .038). Health economic benefits varied across countries but savings could be up to 33% in procedural and hospitalization costs and up to 27% in annual care costs. 17 The drive to optimize FPE in MT is therefore understandable both from the perspective of patient outcomes and of costs, with the added benefit of reduced procedure times for clinicians.
The NeVa Stent-retriever is a novel stent-retriever device characterized by a high radial force and multiple ‘Drop Zones’ along its length, designed to entrap clots inside the device structure. The device is currently available in three sizes: 4.0 × 22 mm, 4.5 × 29 mm and 5.5 × 37 mm. The 4.0 × 22 mm device contains two ‘Drop Zones’ whilst the larger sizes contain three. More recently an alternative device called the NeVa Net has been released which incorporates a distal ‘Clot Catcher’ component. The currently available sizes were introduced in 2020. More recently the NeVa NET device has also become available. The NeVa device has been designed to tackle all clot types and pre-clinical tests have demonstrated that it is more effective than conventional stent-retrievers, particularly with tough clot varieties.18,19 The NeVa stent-retriever has been designed specifically to improve the first-pass recanalization rates.
To date, there are limited publications describing the experience with the NeVa stent-retriever. Here, we report the outcomes of our first 89 cases treated and reviewed by an independent central reader.
Materials and methods
At our single high-volume comprehensive stroke centre, we performed a retrospective review of our prospectively maintained database to identify all patients treated with the NeVa stent-retriever between January 2021 and December 2024 and who met the inclusion/exclusion criteria.
Independent review of imaging data
A clinician trained in stroke imaging interpretation and mechanical thrombectomy and independent of our department and hospital reviewed all imaging data, including baseline CT/CTA, operative catheter angiograms, and post-operative CT head studies. This was to provide an independent evaluation of eTICI scores.
Study population
The inclusion criteria included:
Age ≥18 National Institutes of Health Stroke Scale (NIHSS) score >5 ASPECT score ≥5 LVO on CT angiography Pre-morbid mRS 0-2 Life expectancy of >6 months The NeVa device was the first stent-retriever device attempted for the treatment of the identified intracranial occlusion
Patients were excluded if another device was used as the initial strategy for the MT procedure. The following variables were collected: baseline demographics, smoking, hypertension, diabetes and atrial fibrillation status, pre-stroke mRS, presentation NIHSS, pre-procedural ASPECTS, presence and length of a hyperdense clot, clot location, collateral score, method of anaesthesia, puncture site, presence of a tandem lesion, use of and type of balloon guide catheter, guide catheter and aspiration catheter, number of pulls with NeVa, the size of NeVa, details of any other stent-retriever used, starting, first pull and final eTICI, distal embolization or embolization to new territories, use of intracranial or extracranial balloon plasty or stenting, any intracranial or extracranial complications, the presence or absence of post-procedural symptomatic ICH or SAH, 90-day mRS and 24 hours post-MT CT. Patients were included if pre-procedural or intraprocedural data was present, even if 90-day mRS and 24 hours post-MT CT were not available.
All patients underwent plain CT and CT Angiogram from the arch to the vertex prior to the MT procedure. All included patients, as per the criteria, had an ASPECT score ≥5, a baseline mRS ≤2 and a life expectancy >6 months (in the case of known underlying malignancy). All patients were given IV tPA if there was no contraindication. No patients were excluded from the study based on an ASPECT score <5 or based on their age. One patient received a thrombectomy but was excluded from the study due to a pre-stroke mRS score of 4.
Endovascular procedure
The decision to use the NeVa device as a first-line stent-retriever was driven primarily by operator preference as well as the availability of different stent-retrievers at the time of each procedure. Patients were treated with local or general anaesthesia on a case-by-case basis dependent on the operating team's discretion.
The choice of ancillary devices used in combination with the NeVa device varied between the different operators. A Flowgate 2 (Stryker) or Walrus (Q’Apel) balloon guide catheter and a distal aspiration catheter were the most often preferred options used. Alternatively, a distal aspiration catheter, typically a 6Fr Sofia (Microvention), was introduced via a standard guide catheter such as a NeuronMax (Penumbra). All punctures were performed under ultrasound guidance. Two cases were performed via the right radial artery, one via the left common femoral artery and one via the left common carotid artery after failed access via the right common femoral artery. The rest of the procedures were performed via the right common femoral artery.
Successful reperfusion was defined as final eTICI ≥2b (67%) (i.e. 67% of the threatened territory was re-perfused). First-pass effect (FPE) was defined as eTICI ≥2c after the first stent-retriever thrombectomy attempt. Modified FPE was defined as eTICI ≥2b (67%) after the first stent-retriever thrombectomy attempt.
Post-procedure
Post-procedural imaging was routinely performed at 24 ± 6 hours unless there was a sudden deterioration in level of consciousness which prompted an earlier scan. In cases of intracranial or extracranial stenting, a CTA was also performed.
The 90-day mRS is recorded via telephone interview or clinic review by a trained stroke physician.
The data recorded included the demographics (age, gender, underlying medical conditions, admission NIHSS, etc.), use of IV tPA, radiological findings including the ASPECT score prior to MT, clot location, endovascular procedural information, and relevant timings. The eTICI score was recorded after the first pass of the device and also at the end of the procedure alongside any complications and the 90-day mRS where available. All imaging was reviewed and scored by an independent reviewer as outlined earlier.
Results
Baseline demographics
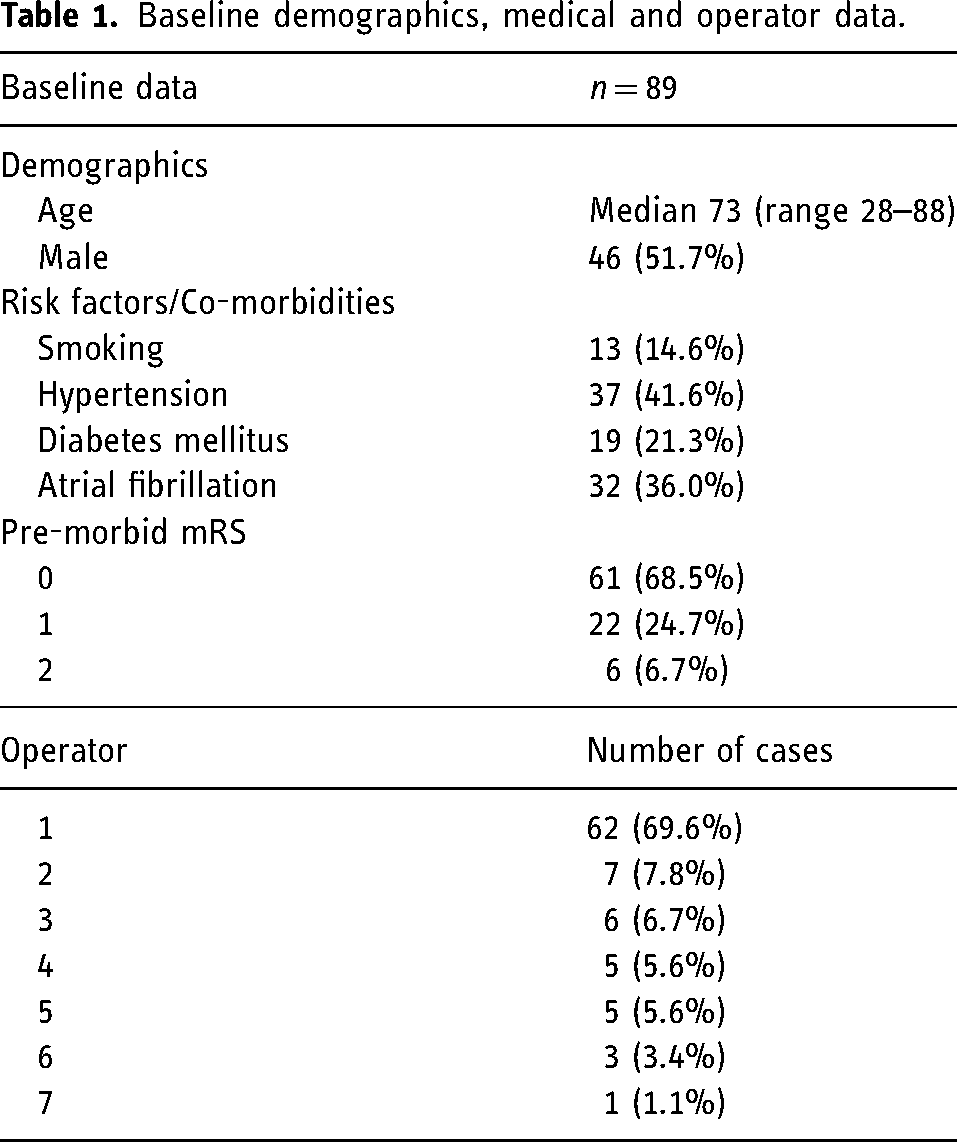
We identified 89 patients that met our inclusion and exclusion criteria. The median age was 73 yrs (range 28–88) and 51.7% were male. Hypertension was relatively common, with other medical conditions such as diabetes mellitus and atrial fibrillation occurring at a lower frequency. Similarly, the vast majority of our patients were recorded as mRS 0 or 1 at the time of treatment. Seven different operators contributed to the data set with 69.6% of the cases performed by one operator. The results are summarized in Table 1.
Baseline demographics, medical and operator data.
Clinical and angiographic results
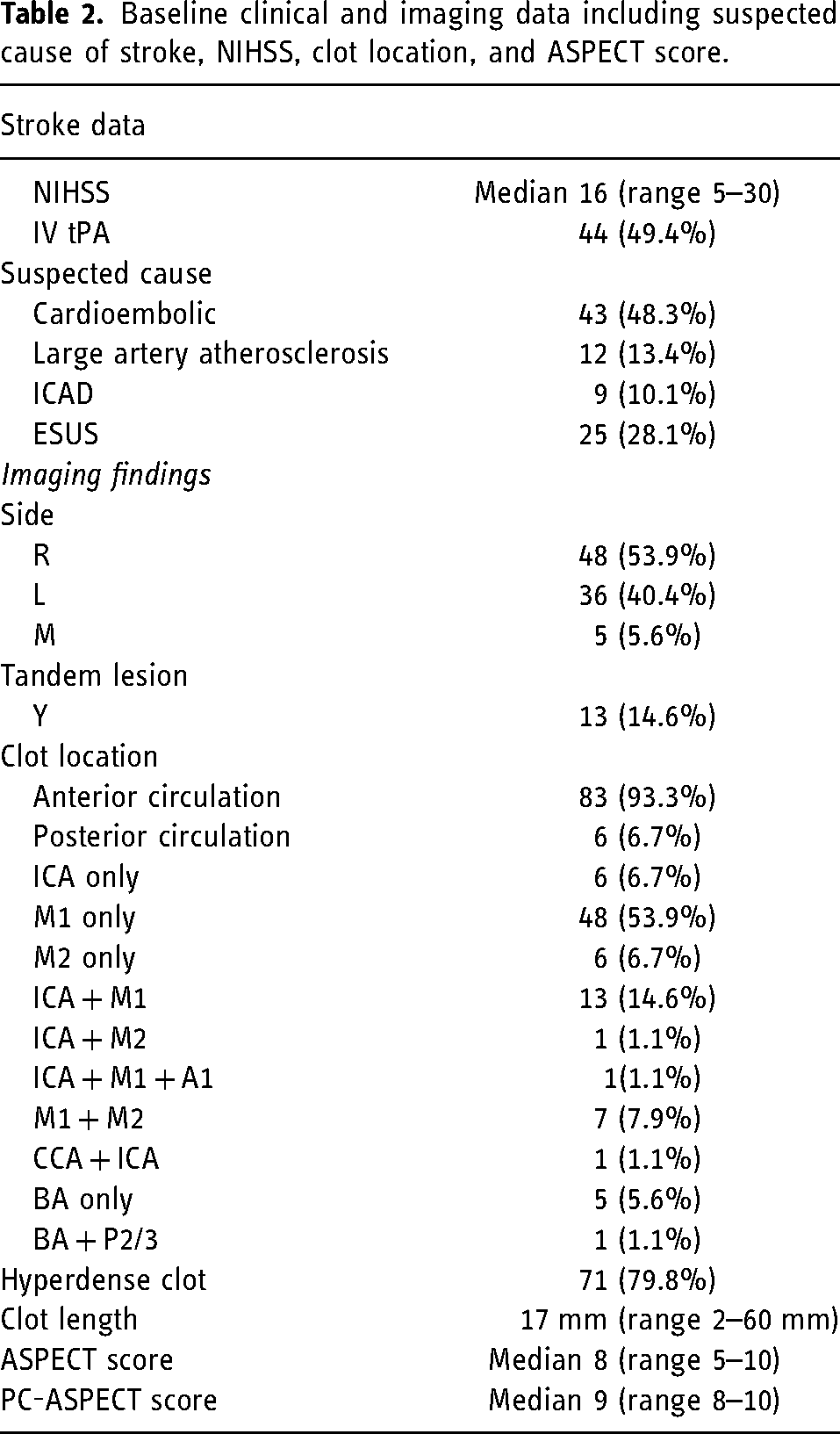
The median NIHSS at presentation was 16 (range 5–30) and 49.4% received IV tPA prior to MT. The cause of the stroke was thought to be cardioembolic (48.3%) or secondary to large artery atherosclerotic disease (13.4%) in the majority of cases. Right-sided occlusions were seen slightly more frequently in our cohort (53.9%) and a small number of cases involved posterior circulation occlusions (6.7%). 14.6% of cases were tandem lesions. The median ASPECT score on plain CT was 8 (range 5–10) with a median PC-ASPECT score of 9 (range 8–10). The results are summarized in Table 2.
Baseline clinical and imaging data including suspected cause of stroke, NIHSS, clot location, and ASPECT score.
Procedural outcomes
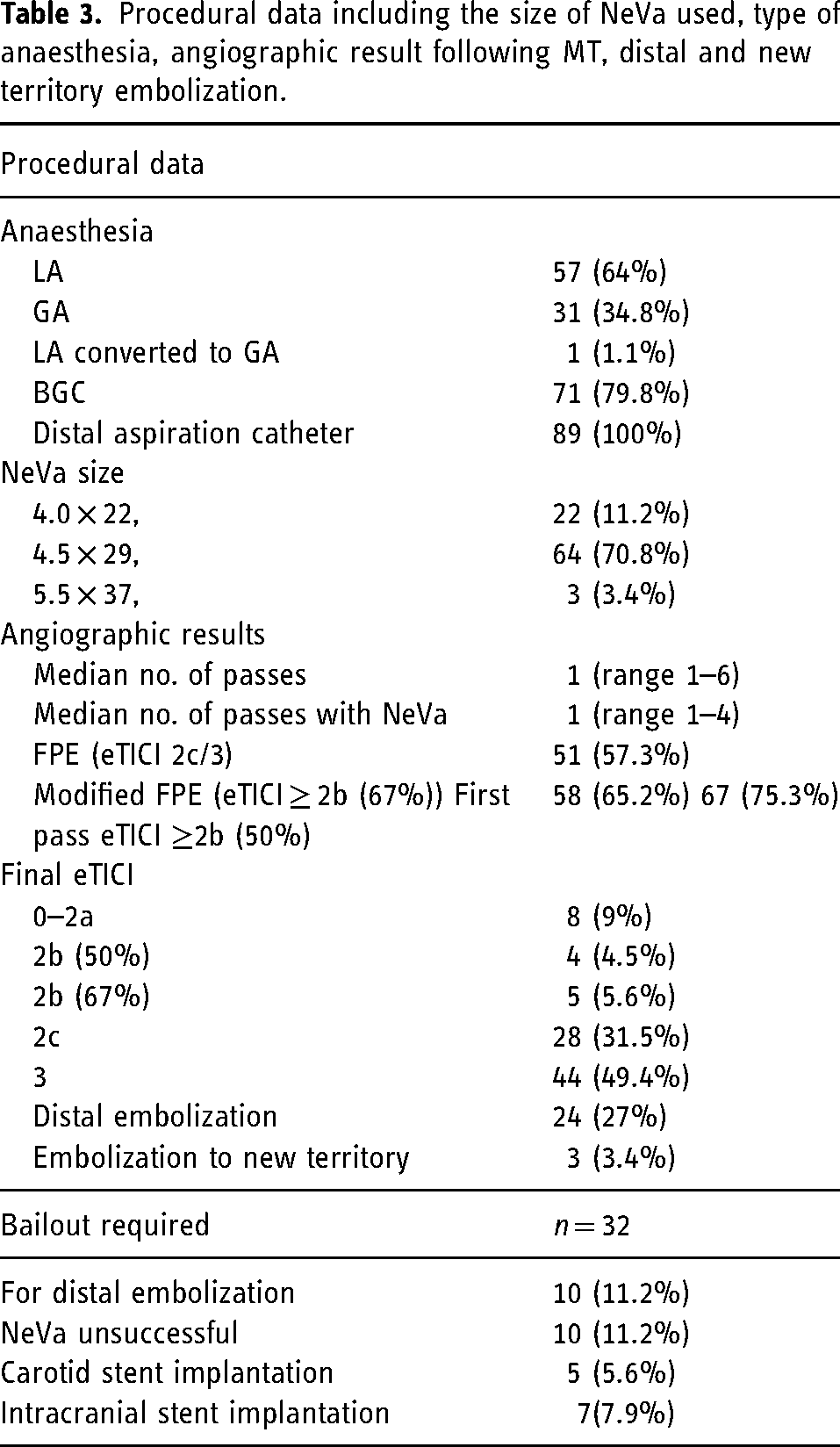
The majority of cases were performed with local anaesthesia and conscious sedation. A BGC was used in 79.8% of cases and a distal aspiration catheter was used in all cases. The longer NeVa models (≥29 mm in working length) were used in 88.8% of cases. First-pass effect (FPE) was seen in 57.3% of cases (Figure 1), modified FPE (eTICI ≥2b 67%) was seen in 65.2% and eTICI ≥2b 50% after the first pass was seen in 75.3% of cases. Distal embolization was seen in 24 cases (27%); however, half of these represented very distal (M4) clots. In the remaining cases with more proximal emboli, for example in the distal M2 or M2/3 segments, dedicated small stent-retrievers or aspiration were used to retrieve the clots.
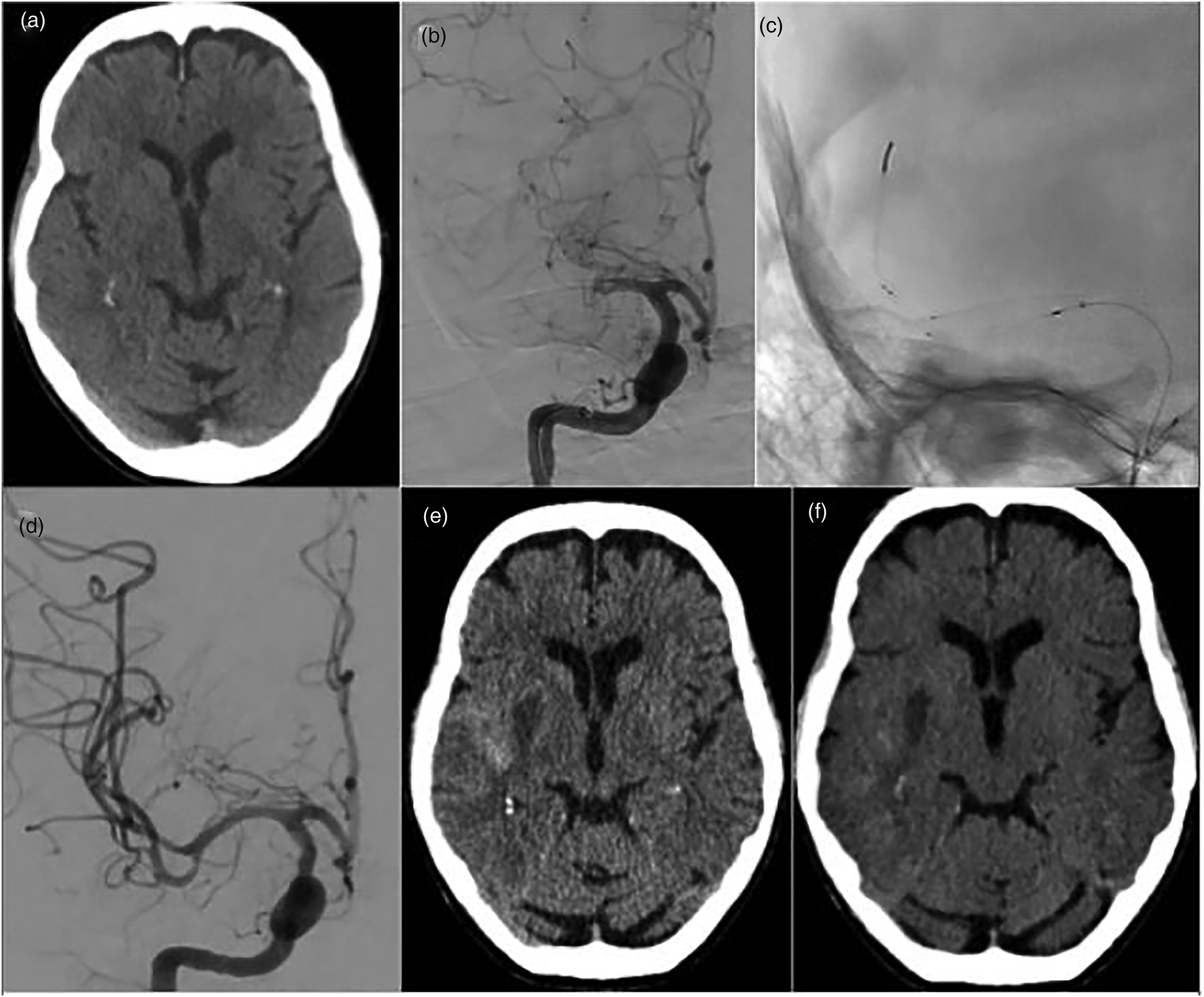
A patient in their 70s presented with an NIHSS score of 6 and ASPECT score 9 (figure 1(a)). After CTA confirmed an occlusion, the patient was transferred for MT. Initial angiography confirmed occlusion of the right mid-M1 (figure 1(b)). A NeVa 4.0 × 30 mm was deployed for 5 minutes per our standard practice. Angiography demonstrated eTICI 3 recanalization after the first pull (figure 1(d)). The 24-hour CT scan showed infarction within the basal ganglia (ASPECT score 8) with high density seen in the Sylvian fissure (figure 1(e)) with minimal sub-arachnoid haemorrhage seen on the virtual non-contrast spectral reconstruction (figure 1(f)).
Carotid stents were implanted in five cases (5.6%) and intracranial stents were implanted in seven cases (7.9%), all of which were related to ICAD. The median number of passes when only NeVa was used was 1 (range 1–6) with the mean number of passes at 1.4. At the end of the procedure a final eTICI score of ≥2b (67%) was achieved in 86.5% with eTICI 2c/3 seen in 80.9% of cases. There were no device-related or intra-procedural serious adverse events. The results are summarized in Table 3.
Procedural data including the size of NeVa used, type of anaesthesia, angiographic result following MT, distal and new territory embolization.
Follow-up imaging and clinical results
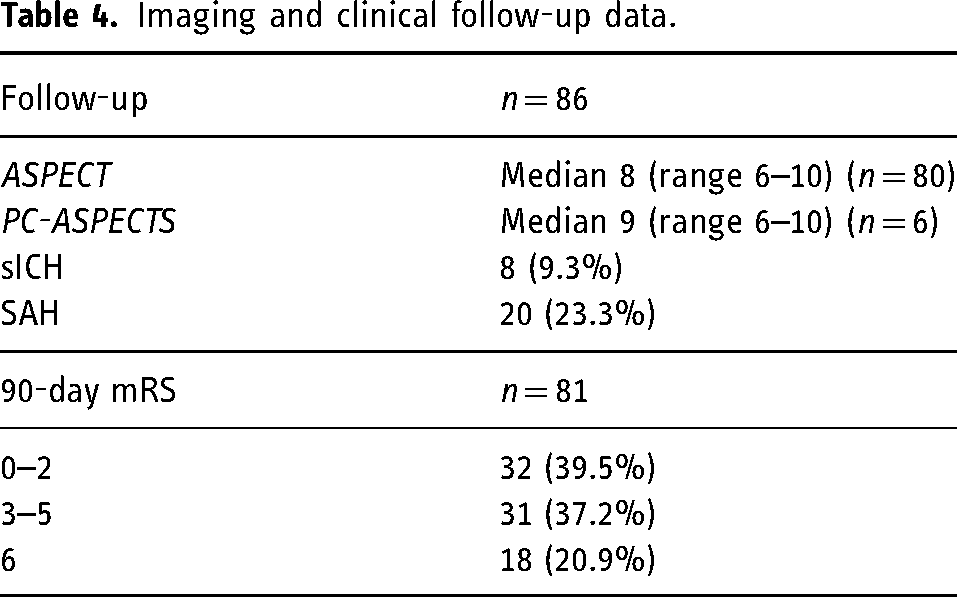
Follow-up CT scans performed at 24 hours were available for 86 patients. The median ASPECT score was 8 (range 6–10). Subarachnoid haemorrhage was seen in 20 patients (23.3%) however, in most cases this was very small (Figure 1). The 90-day mRS was available for 81 patients. The nine patients with missing 90-dat mRS scores were repatriated to their local stroke unit and lost to telephone follow-up. A good functional outcome was achieved in 39.5%. The 90-day mortality rate (i.e. mRS 6) was 20.9%. The results are summarized in Table 4.
Imaging and clinical follow-up data.
Discussion
In our series, we observed a high first-pass effect (FPE) of over 57% and a modified first-pass effect (mFPE), defined as eTICI 2b ≥ 67%, of approximately 65%. The performance of the NeVa device in the context of this series exceeds the reported performance of other strent-retreivers in the literature. For example, the FPE of the Solitaire (Medtronic) averages 32%20–23 whilst the FPE of the Trevo (Stryker) ranges from 27.8% to 40.8%.24–26 Our results are improved but comparable to the largest series to date on the results of 145 patients treated with the NeVa device, 27 which reported an FPE of 53.8%. Our results represent an improvement compared to those reported by other previous authors who have published their experience with the NeVa device. An FPE of 44.9% was reported by Akpinar et al., 28 47% by Ribo et al. 29 and 48.3% by Borggrefe et al. 30 The average FPE across the previously reported series stands at 48.5%.
To date there have been limited publications regarding the NeVa device and these, to our knowledge, have all been investigator-initiated studies from single centres. The largest study to date has been the company-sponsored NeVa Clear study. 31 This was a prospective, multicentre, open-label, single-arm study using the NeVa stent-retriever with the primary endpoint being the rate of successful reperfusion (eTICI ≥2b) within three NeVa passes without rescue. Secondary endpoints included mFPE (eTICI ≥2b), eTICI ≥2b after all NeVa passes, eTICI ≥ 2c after all passes and good functional outcome at 90 days (mRS 0–2). In the modified ITT group (n = 107) the baseline age of enrolled patients was 65.1 ± 13.2 years, with NIHSS of 16 (range 12–20) and CT ASPECT score of 9 (range 8–10). The majority of occlusions were located in the M1 segment and 99.1% of occlusions were in the anterior circulation. A BGC was used alone in 13.1% of cases and in combination with a DAC in a further 15.9% of cases. On analysis of the modified intention to treat population (mITT) (n = 107), eTICI ≥ 2b was achieved within three passes in 90.7% of cases. When compared to the pre-specified performance goal, eTICI ≥2b in 72% of cases with predicate devices and a −10% margin of non-inferiority, the NeVa demonstrated non-inferiority (P < .0001). Similarly, the NeVa further demonstrated post hoc superiority to the predicate performance goal (P = .001). In terms of key secondary endpoints, mFPE was achieved in 73.8% compared to 57.8% (P = .0008) for predicate devices and eTICI ≥2c was achieved in 48.6% with the NeVa device compared to 41.4% (P = .13). Good functional outcome at 90 days was achieved in 65.1% compared to 54.7% with the predicated devices (P = .03). From a safety perspective 5% of patients experienced sICH at 24 hours (95% CI: 2.5–10%) and 9.4% of patients were mRS 6 at 90 days. Our own results in an unselected population demonstrate similar rates of mFPE and improved FPE rates compared to the NeVa CLEAR study. However, functional independence at follow-up in the present study was lower in comparison. This could reflect the nature of this series as well as being caused by other non-device/procedure-related factors such as poor access to rehabilitation.
The exact reason for the discrepancy between our FPE results and those reported previously is uncertain, however, it may be the result of multiple factors that are interacting with one another. In our series, a BGC and distal aspiration catheter were used in the majority of cases, in conjunction with stripping the microwire prior to retrieval. A distal aspiration catheter was used in all cases, and a BGC was used in two-thirds of cases. In the study by Ribo et al., a BGC was used in 20% of cases and in that of Akpinar et al. in 13.6% of cases. A BGC did not appear to be used in the remaining studies published on the NeVa device. Although there are no randomized controlled trials on the use of BGC during mechanical thrombectomy, there are numerous studies that support the use of a BGC. Bai et al. 32 showed, in their meta-analysis of 17 studies and 6186 patients, that the use of BGC (OR:1.60,95% CI: 1.17–2.18; P = .003) was significantly associated with successful recanalization with FPE. Ahn et al. 33 and Zaidat et al. 34 showed similar advantages to using a BGC: improved FPE compared to conventional guide catheter use (48% vs. 26%, P = .001) and to distal access catheter (48% vs. 35%, P = .002), higher rates of mFPE, and higher rates of functional independence vs. conventional guide catheter (61% vs. 42%, P = .007) and distal access catheter (61% vs. 52% P = .027). In previous studies published on NeVa, BGC use seems to be very limited and instead, the authors report using distal access catheters preferentially. It can be argued that the use of the available BGCs limits the use of the newer generation large bore aspiration catheters, but there is limited data on the use of these newer devices in combination with either stent-retrievers or BGCs. There is certainly evidence to suggest that optimizing proximal flow control by combining the largest aspiration catheters with a BGC offers additional advantages. 35 In our own series, the 5Fr Sofia was the most frequently used DAC due to its excellent navigability and consistent interaction with the Flowgate 2 BGC. The use of larger DACs with Flowgate 2 or larger BGCs such as the Walrus (Q’Apel) may assist in achieving further improvements in the FPE. We believe that the high rate of BGC use in our series may have contributed to the improvement in FPE in comparison to the previously published literature. The recent results of the PROTECT-MT 36 have raised questions regarding the use of BGCs and improved outcomes although other studies on the use of BGCs are limited and do support higher FPE. 37
We also believe that clot-related factors may have played a role in our high FPE rate. In 79.8% of our cases, clots were hyperdense on baseline imaging. Hyperdense clots on non-contrast CT imaging have been shown to be rich in red blood cells (RBCs)38,39 relative to non-hyperdense clots. The exact implications of this are yet to be fully understood, however, there is some evidence to suggest that these hyperdense thrombi and RBC-rich thrombi are associated with easier recanalization.40,41 These may be more amenable to stent-retriever-based MT techniques as was recently suggested in the meta-analysis of Ye et al. 42 In the recent publication of Mohammaden et al. 43 the authors showed that the FPE for patients undergoing MT with a stent-retriever was significantly higher than those undergoing MT with contact aspiration (SR 41.3% vs. CA 22.2%, P = .001, adjusted OR 2.1195% CI 1.2 to 3.7). Similarly, the use of a BGC was associated with FPE for both hyperdense and non-hyperdense clots. The nature of RBC-rich clots may make them prone to fragmentation 44 and as a result of this property a stent-retriever, particularly one with a distal clot catcher such as the NeVa, may be more suitable for the removal of these clots. The additional use of proximal aspiration and flow arrest with a BGC is likely to confer additional benefits when faced with friable RBC-rich clots. It is also noteworthy that the average clot length in our study was ≈19 mm and although the clot length was not mentioned in the previous NeVa publications we believe that this may also be of importance due to the interaction between the clot and stent-retriever lengths. Previous publications have shown that longer stents are associated with higher rates of FPE across a range of different devices45–47 but more recently Belachew et al. 48 have reported that it is the ratio of the clot and stent-retriever lengths that is of importance with a higher stent-retriever to thrombus length ratio being associated with a higher rate of FPE. One possible advantage of stent-retrievers in comparison to aspiration is that the former can control both the proximal and distal end of the clot whereas the latter only controls the proximal end of the clot. This only holds true if the stent-retriever is longer than the clot and placed in the correct branch to maximize clot engagement. In our series, 66.7% of NeVa stents used were of the longer size (≥29 mm), and this is because we believe, in general, that longer stent-retrievers are more effective. In the previous studies, it is unclear which sizes were predominantly chosen. Based on our experience we believe that where possible and safe to do so, the longer NeVa devices should be chosen even for shorter clots.
One final possible important factor may be related to the dwell time used in our study. As a standard, we use a minimum 5-minute dwell time when performing stent-retriever-based MT. The exact nature in which stent-retrievers interact with different clots is likely to vary based on clot architecture and stent-retriever design features. Electron microscopic and micro-CT studies have begun to look at the different ways in which stent-retrievers are interacting with removed thrombi and a variety of different types of interactions have been observed.11,13 There is some evidence that the stent-strut indentation into clots increases over time 44 along with preliminary evidence that longer dwell times may be associated with higher FPE and mFPE. 49 The exact reason for this is likely multifactorial and probably relates to an improved stent–clot interaction. Although the dwell time was not specifically looked at in the previous papers, it was suggested that a shorter dwell time could be adopted with the NeVa device due to the higher radial force. We believe that a minimum 5-minute dwell time is likely to be beneficial and an even longer dwell time may be preferred if a platelet-rich clot is suspected.
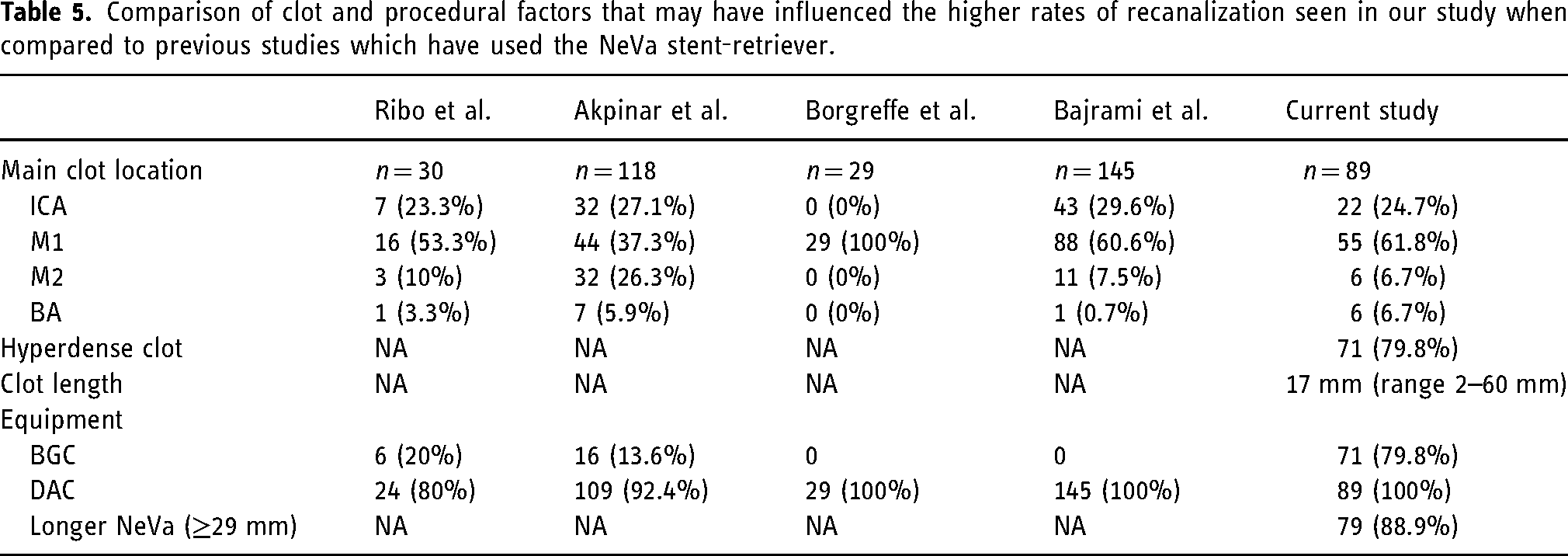
We believe that the combination of these discussed factors may have led to a significantly higher FPE and mFPE in our cohort compared to previous studies and whether this high rate can be maintained with an increasing number of patients remains to be seen. A comparison of the features we believe may have contributed to our results versus the existing literature is summarized in Table 5.
Comparison of clot and procedural factors that may have influenced the higher rates of recanalization seen in our study when compared to previous studies which have used the NeVa stent-retriever.
The limitations of this study include it being retrospective in design, with all the bias that this entails. There is also a lack of randomization with other thrombectomy devices and the impossibility of blinding the type of device used. There was no attempt to standardize ancillary device use as this was left to the operator choice. Moreover, as 69.6% of cases were performed by one operator, one would expect the results to be skewed towards the ability of that operator.
Conclusion
The NeVa stent-retriever has a very high rate of first-pass effect and final recanalization in this real-world cohort of patients from the NeVa One registry. These results are higher than previously published literature, and we believe this may support the use of the longer NeVa devices in conjunction with a BGC and proximal aspiration to optimize FPE.
Footnotes
Authors’ contribution
PB – manuscript preparation, editing, revision; MM – data collection, editing, guarantor; RF – data collection, editing, guarantor; KP – data collection, editing, guarantor; GK – data collection, editing, guarantor; LM – data collection, editing, revision; KW – data collection, editing, revision; KW – data collection, editing, revision; OS – manuscript preparation, editing, revision.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: PB – consulting agreements Phenox, JnJ MedTech Balt, Brainomix, Perfuze, PockIt Diagnositcs, Vesalio, Penumbra; LM – consulting agreements Cerenovus, Balt, Perfuze, Microvention, Penumbra, Neuroventures. The remaining authors declare no conflicts of interest.
Informed consent statement
Informed consent was taken from all individual patients in those who were able to provide consent. In patients who could not provide consent the thrombectomy procedures were discussed with next of kin/ available family members and consent was taken by the operating team and stroke physicians.
Institutional review board statement
Ethics committee approval for a retrospective study of this nature is not required. The data collection and review were registered as an audit of clinical effectiveness.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Vesalio provided an educational grant (modest) to support this work.