
Abstract
Background
We investigated racial disparities in radiologic and clinical outcomes of patients after middle meningeal artery embolization (MMAE) for chronic subdural hematoma (CSDH) with or without evacuation surgery.
Methods
This multicenter retrospective study includes consecutive patients who underwent MMAE across 11 institutions in North America (10 in the United States and 1 in Canada). Patients were stratified using self-reported racial data. Outcomes of interest were complications, treatment failure/reoperations, resolution of hematoma, and functional independence at last follow-up. Multivariable regression models were used to assess and adjust for relevant confounders.
Results
A total of 557 patients underwent 663 MMAEs, including 323 White (58%), 150 Black (27%), 35 Hispanic (6%), 29 Asian (5%) patients, and 20 patients (4%) self-categorized as other/nondisclosed. The median age (interquartile range) of the cohort was 75 (65–81) years, and 412 (74%) patients were female. Middle meningeal artery embolization was the primary treatment for CSDH for 369 patients (66%) and adjunct treatment for 188 (34%). Black patients had a 51% lower likelihood of reoperation relative to other racial categories (adjusted odds ratio [OR] 0.49; 95% confidence interval [CI] 0.25–0.95, p = 0.034). White patients were twice as likely (11% difference; adjusted OR 2.24; 95% CI 1.43–3.51, p < 0.001) and Black patients 59% less likely (6% difference; adjusted OR 0.41; 95% CI 0.25–0.69, p = 0.001) to be independent at last follow-up.
Conclusion
This study highlights significant racial disparities in outcomes after MMAE for CSDH, with or without evacuation surgery. White patients had higher reoperation rates but were more likely to be functionally independent at last follow-up. Black patients, despite better baseline functional status, had lower odds of functional independence postoperatively.
Keywords
Introduction
Chronic subdural hematoma (CSDH) is prevalent in elderly populations and has an incidence that is expected to surpass other intracranial conditions to become the most common neurosurgical disease by 2030.1–3 Treatment options include observation and surgical evacuation, with varying success rates and risks of complications. 4 The recent integration of middle meningeal artery embolization (MMAE) into the treatment of CSDH has shown significant clinical benefits and demonstrated promise as a stand-alone method or as an adjunct to surgical evacuation.5–9
Efficacy and safety are the focus of multiple ongoing trials aimed at validating MMAE in its independent and adjunctive role in CSDH management. 10 As this new technique gains popularity, it is important to consider the effect of racial disparities—which have been widely documented across various medical and surgical specialties—on healthcare outcomes. 11 Studies have shown that patients from minority groups, particularly Black patients, often face worse outcomes after neurosurgical diagnoses, 12 which has been attributed to factors such as access to care, implicit bias, and socioeconomic barriers. 13 However, it remains unclear whether these broader disparities extend to differences in the functional status of patients presenting with CSDH, as well as in periprocedural events, retreatment rates, radiologic resolution, and postprocedural outcomes following MMAE with or without evacuation surgery.
Accordingly, we conducted a multicenter analysis to determine whether these disparities manifest in differences across baseline characteristics, procedural factors, and key clinical outcomes in patients undergoing MMAE.
Methods
Design, setting, and participants
We conducted a multicenter, retrospective cohort study across 11 urban, tertiary-care academic centers in North America (10 in the United States and 1 in Canada) between April 2018 and January 2023. Included patients underwent MMAE with or without concurrent evacuation surgery for CSDH. Institutional review board approval was obtained at each participating center before data collection with waivers of informed consent. This study followed the STrengthening the Reporting of OBservational Studies in Epidemiology guidelines for cohort studies to ensure completeness in reporting observational data. Patients were identified from the electronic health records at each institution and categorized into five groups (White, Black, Hispanic, Asian, and other/nondisclosed) using self-reported racial data. Patients who underwent either unilateral or bilateral CSDH were included, with bilateral cases assessed based on the most symptomatic side for outcome evaluation. If the symptomatic side was unclear (i.e., patients with generalized seizures or nonlateralizing presentations), the index side was determined as the larger subdural hematoma with an associated midline shift. Patients who received MMAE within 7 days of surgical evacuation were categorized as receiving adjunctive MMAE treatment.
Data extraction and statistical methods
Data were extracted and analysis was structured to describe baseline demographics (i.e., age, sex, race, and comorbidities), and presentation characteristics, followed by subdural hematoma features and procedural variables. Subsequent sections examined reintervention and complication rates, radiographic resolution of hematoma, and functional or clinical status at last follow-up. Comorbidities were documented as a binary variable (yes/no) and further categorized into broader diagnostic groups for analysis. Multivariable models included variables that were significantly different between racial groups in univariable analysis and that were clinically relevant to the outcomes assessed. Depending on significance patterns, this included either individual comorbidities or the composite “any comorbidity” variable.
Key clinical and radiographic outcomes included functional independence, defined as a modified Rankin Scale (mRS) score of 0–2 at last follow-up; CSDH size reduction, defined as a ≥50% reduction in maximal thickness on axial computed tomography (CT) from initial measurement to last follow-up; and retreatment rates, defined as the need for additional surgical intervention during the index hospitalization or subsequent follow-up period. Hematoma thickness was measured as the maximal thickness in millimeters in the axial plane on noncontrast CT scan, and the presence of membranes was identified by hyperdense linear signals within the hypodense subdural collection on noncontrast CT.14,15
Continuous values were presented as mean (standard deviation) or median (interquartile range [IQR]) depending on distribution, and univariable analysis was performed using the Student's t-test or Mann–Whitney U test. Categorical values were presented with frequencies and were compared using Chi-square analysis. For multivariable assessments, logistic regression models were constructed to evaluate the association between race and key outcomes and to control for potential confounders noted through univariable screening between groups and previous literature. Because data were obtained from 11 distinct centers, we also included site-coded variables (fixed effects) in each regression model to adjust for potential intercenter variability in patient populations, procedural approaches, and follow-up protocols.
The primary analysis was performed on a patient-level basis, with bilateral CSDH and bilateral procedures noted and adjusted for in the multivariable models. To potentially capture clinically and socially relevant disparities, race groups were analyzed using binary indicators, creating distinctions such as “White vs. all other races” and “Black vs. all other races.” This approach allowed us to directly assess the independent effect of each race against all others to determine whether outcomes for specific racial groups are better or worse relative to others. By distinguishing individual racial comparisons, we aimed to address clinically meaningful questions on disparities rather than simply identify general differences across multiple groups.
To investigate the functional status at baseline (using mRS) based on racial groups, an ordinal logistic regression model was applied, and the coefficients were subsequently exponentiated to present the results as odds ratios (ORs) for ease of interpretation. Binary logistic regression was used for multivariable analyses of dichotomized outcomes, including retreatment (yes/no), hematoma resolution (≥50% vs. <50%), and functional independence at last follow-up (mRS 0–2 vs. 3–6). Odds ratios are reported with 95% confidence intervals (CIs), and statistical significance was set at p < 0.05. Sensitivity analyses were performed to verify robustness, including bilateral procedures. The study included cases with complete data on race/ethnicity reporting and outcomes. All statistical analyses were adjusted for confounders, including patient age, sex, baseline mRS, comorbidities, and procedural details. Statistics were performed with the latest STATA Software v18.0 (StataCorp., College Station, Texas, USA).
Results
Baseline demographics and presentation characteristics
A total of 557 consecutive patients underwent 663 MMAE procedures across 11 institutions. Among these, 369 patients (66%) underwent MMAE as a stand-alone treatment and 188 patients (34%) received MMAE as an adjunct to initial CSDH evacuation surgery. The cohort included 451 unilateral (68%) and 212 bilateral (32%) procedures, with 194 concurrent evacuation surgeries performed across 188 patients (including six bilateral evacuations). The median age [IQR] of the cohort was 75 years [65–81], and 412 patients (74%) were female (Table 1). Patient race was predominantly White (323 patients, 58%), followed by Black (150 patients, 27%), Hispanic (35 patients, 6%), Asian (29 patients, 5%), and other/nondisclosed (20 patients, 4%). Comorbidities were present in 67% of the overall cohort, with hypertension (35%) and diabetes (20%) observed most frequently.
Baseline demographic and presentation details by self-reported race.
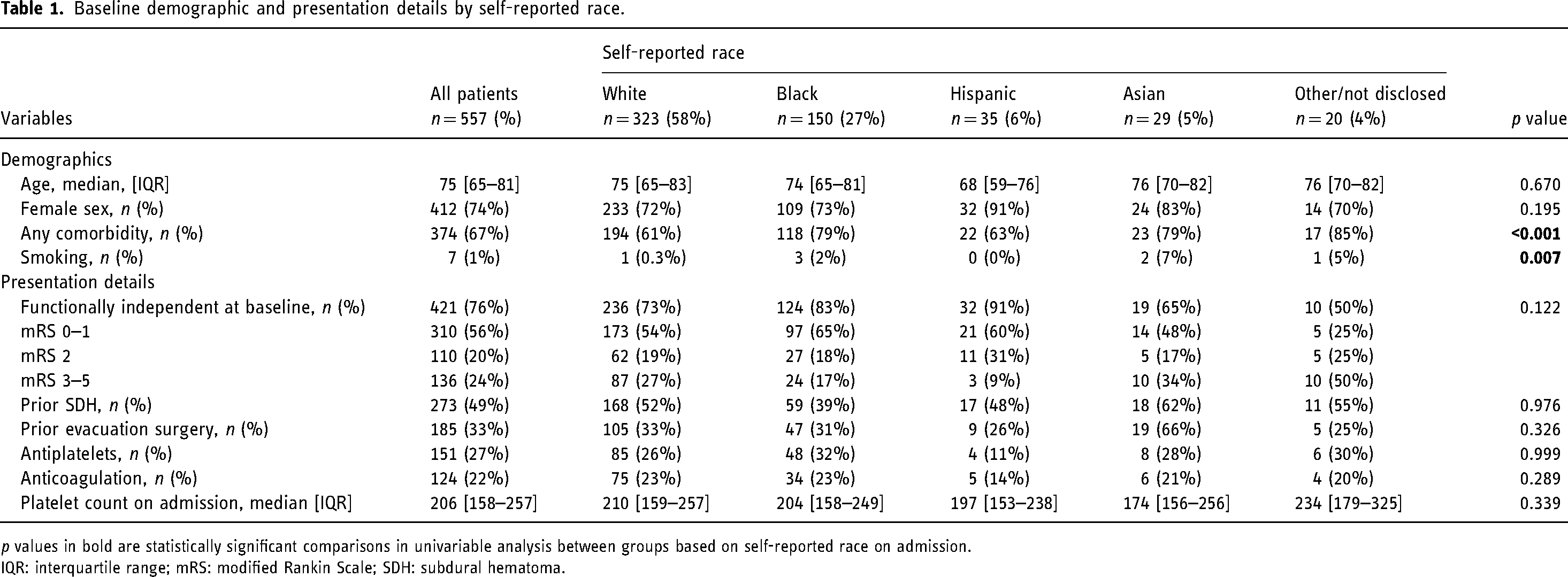
p values in bold are statistically significant comparisons in univariable analysis between groups based on self-reported race on admission.
IQR: interquartile range; mRS: modified Rankin Scale; SDH: subdural hematoma.
We recorded the distribution of mRS scores across racial groups (Table 1). Overall, 76% of the cohort (421 patients) were functionally independent at baseline (mRS 0–2). Across the racial groups, the distribution of mRS scores varied, with 27% (87/323) of White patients, 17% (24/150) of Black patients, 9% (3/35) of Hispanic patients, 34% (10/29) of Asian patients, and 50% (10/20) of other/undisclosed patients classified as mRS 3–5. Although univariable analysis showed no statistically significant differences across groups (p = 0.122), a trend toward significance prompted further investigation.
To better understand the relationship between baseline functional status and racial group, we performed adjusted analyses accounting for age, sex, prior subdural hematoma, prior evacuation surgery, and comorbidities. These adjusted regression models revealed that White patients were more likely to present with worse baseline functional status compared with other racial groups (adjusted OR [aOR] 1.37, 95% CI 1.01–1.87, p = 0.046). Conversely, Black patients were more likely to present with better baseline functional status compared with all other groups (aOR 0.49, 95% CI 0.34–0.65, p < 0.001).
There were no major differences in the distribution of prior subdural hematoma, evacuation surgeries, use of antiplatelets or anticoagulation, and platelet count on admission across racial groups. Table 1 provides details on baseline demographic and presentation characteristics by self-reported race.
Subdural and procedural details
Radiographic and procedural characteristics and outcomes are shown in Table 2. The median [IQR] CSDH thickness was 15 mm [11–19], with a median midline shift of 4 mm [1–6]. Black patients had the highest proportion of subdural membranes (84%) compared with all other racial groups; however, the difference was not statistically significant (p = 0.559). Although the presence of subdural membranes was not statistically significant on univariable analysis, we included it in the final regression model given prior literature associating membranes with recurrence rates.14,15 This approach ensured that any potential influence of membranes on postoperative outcomes was accounted for. Notably, when included in our multivariable models, the presence of membranes did not independently predict reoperation or functional status at last follow-up.
Subdural hematoma procedural and outcome-related details by self-reported race.
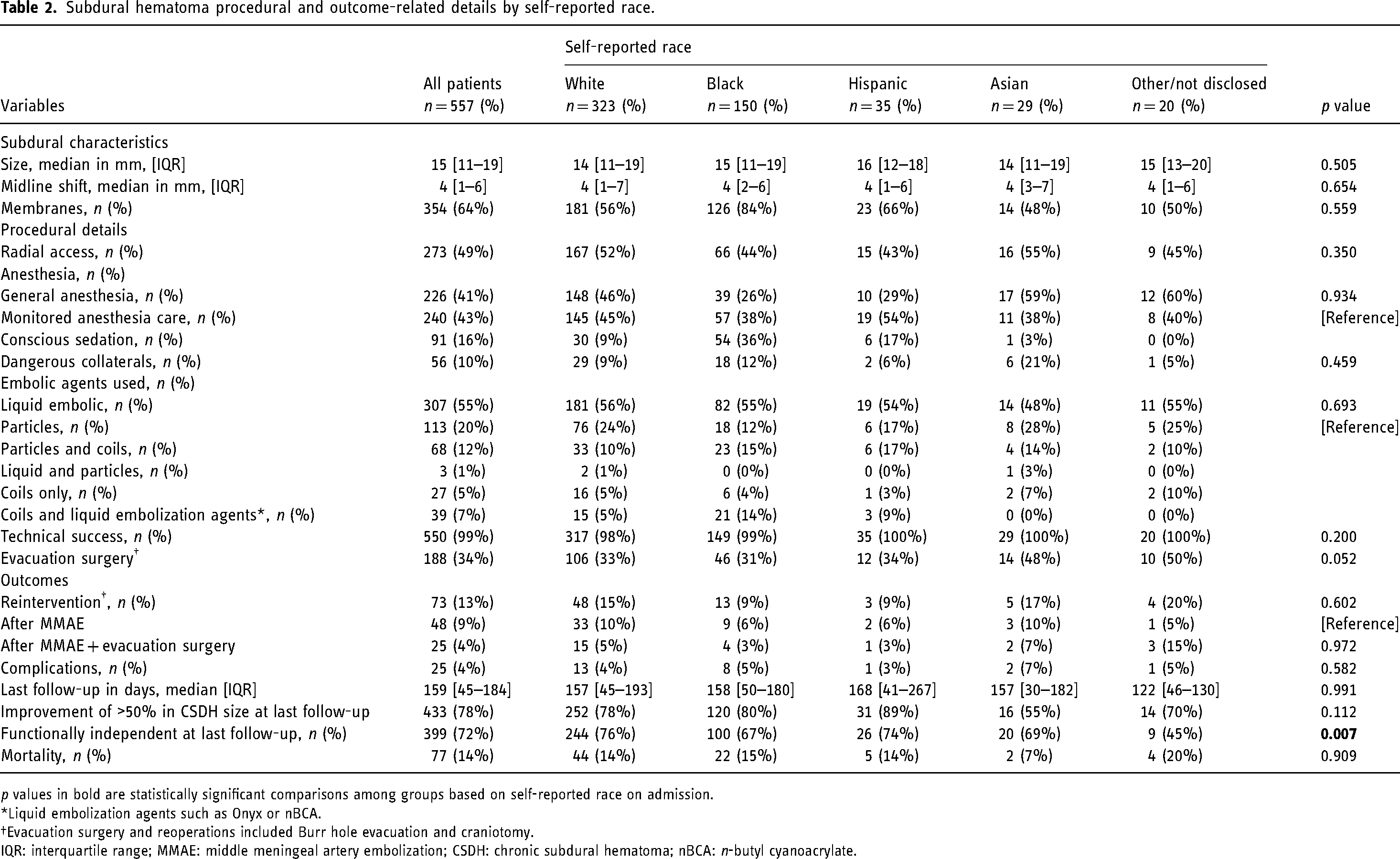
p values in bold are statistically significant comparisons among groups based on self-reported race on admission.
*Liquid embolization agents such as Onyx or nBCA.
Evacuation surgery and reoperations included Burr hole evacuation and craniotomy.
IQR: interquartile range; MMAE: middle meningeal artery embolization; CSDH: chronic subdural hematoma; nBCA: n-butyl cyanoacrylate.
Overall, approximately half of the cases were performed via radial access, and the anesthesia technique was similar among groups. The presence of dangerous collaterals was reported in 10% of all cases, with the highest prevalence found in Asian patients (21%); however, racial differences were not significant (p = 0.459). Liquid embolic agents were the most commonly used embolic material, comprising 55% of cases, followed by particles alone (20%) and coils with particles (12%) (Table 2). The overall technical success rate was 99%. The procedure was unsuccessful in seven cases because of factors such as excessive tortuosity leading to an inability to access the external carotid artery as well as great vessel stenosis. One case involving a dangerous collateral—aberrant origin of the ophthalmic artery—was deemed technically unsuccessful. These failures were not significantly different among racial groups.
Reinterventions and complications
Reintervention was required in 13% of the overall cohort; 9% of patients who underwent MMAE alone required reintervention, compared with 4% of those who received MMAE as an adjunct to initial surgical evacuation. Retreatment was performed in 15% of White patients compared with 11% of patients in all other race groups (OR 1.79, 95% CI 1.001–3.19, p = 0.048) (Figure 1A). In contrast, Black patients had a 9% retreatment rate compared with 15% of patients among all other groups (aOR 0.49, 95% CI 0.25–0.95, p = 0.034) (Figure 1B).
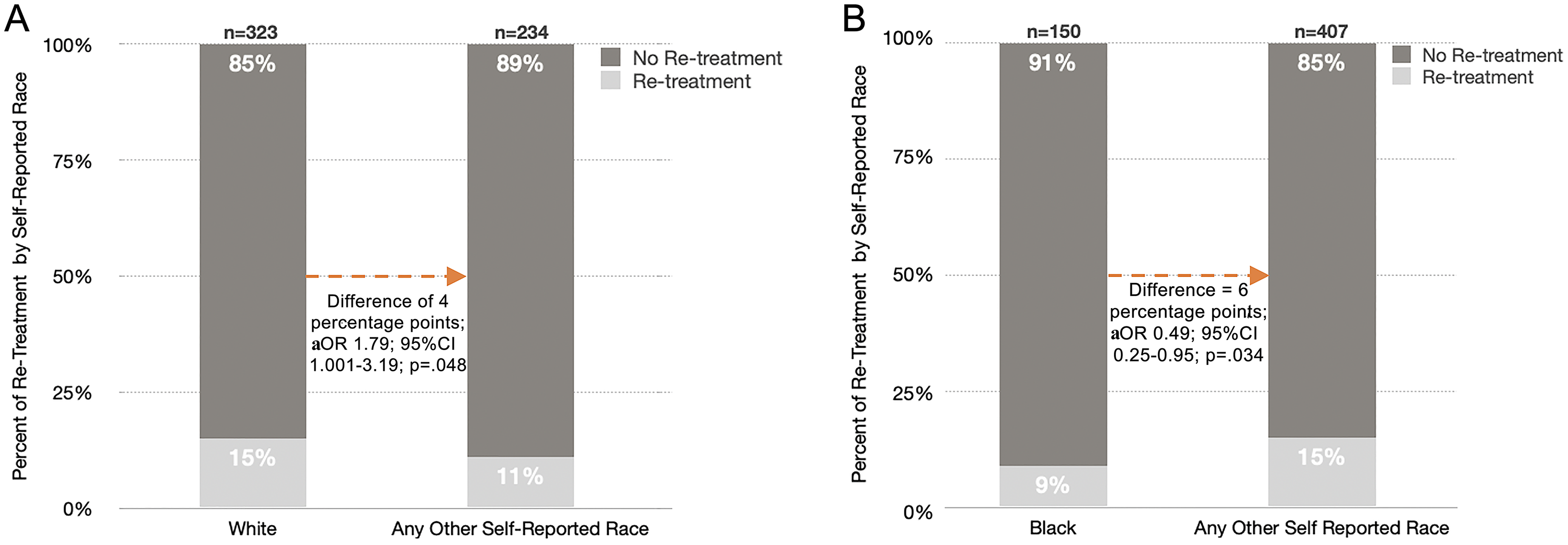
Analysis of reintervention and subdural resorption outcomes by race after MMAE with or without evacuation surgery. (A) Comparison of the reintervention rates between White patients and patients of other self-reported races after MMAE. Among White patients, 15% (n = 48) underwent retreatment, compared with 11% (n = 26) of patients in other racial groups. The difference was statistically significant, with a 4-percentage point difference and an OR of 1.79 (95% CI 1.001–3.19, p = 0.048). (B) Comparison of the reintervention rates between Black patients and patients of other self-reported races. Among Black patients, 9% (n = 13) underwent retreatment, compared with 15% (n = 60) of patients in other racial groups. The difference between groups was statistically significant, with a 6-percentage point difference and an OR of 0.49 (95% CI 0.25–0.95, p = 0.034). MMAE: middle meningeal artery embolization; aOR: adjusted odds ratio; CI: confidence interval.
Complication rates were low (4%) across the cohort, and no significant differences in complication rates were observed across racial groups (Table 2). Major complications accounted for 2.15% (n = 12) and included ischemic stroke (0.72%, n = 4), hemorrhagic stroke (0.36%, n = 2), iliac artery dissection (0.18%, n = 1), MMA dissection (0.18%, n = 1), parietal branch perforation with hemorrhage (0.18%, n = 1), left-sided central retinal artery occlusion (0.18%, n = 1), and seizure (0.36%, n = 2). Minor complications accounted for 2.33% (n = 13) and included groin hematomas (1.80%, n = 10), transient cranial nerve IV palsy (0.18%, n = 1), and persistent headaches (0.36%, n = 2).
Subdural resolution
The median follow-up was 159 days (IQR 45–184), and radiographic outcomes demonstrated significant differences in CSDH resolution across racial groups (Table 2). Overall, resolution rates were 79% for White patients, 77% for Black patients, 89% for Hispanic patients, 55% for Asian patients, and 74% for patients categorized as other/undisclosed. Hispanic patients exhibited the highest resolution rates, with 89% achieving significant resolution compared with 77% among all other racial groups (aOR 9.62, 95% CI 1.27–73.14, p = 0.029). Conversely, Asian patients had the lowest resolution rates, with only 55% achieving significant reduction, compared with 79% among other racial groups (aOR 0.26, 95% CI 0.11–0.61, p = 0.002).
Functional status and clinical status at last follow-up
To address potential biases introduced by dichotomizing mRS scores at the last follow-up (0–2 vs. 3–5), we examined the distribution of mRS scores at the cutoff point of 2 across racial groups at baseline. This analysis revealed that a comparable proportion of White and Black patients (19% vs. 18%, respectively) had an mRS score of 2 at baseline, suggesting that differences in functional outcomes were not confounded by baseline disparities at this cutoff point for independence (Table 1 and Figure 2).
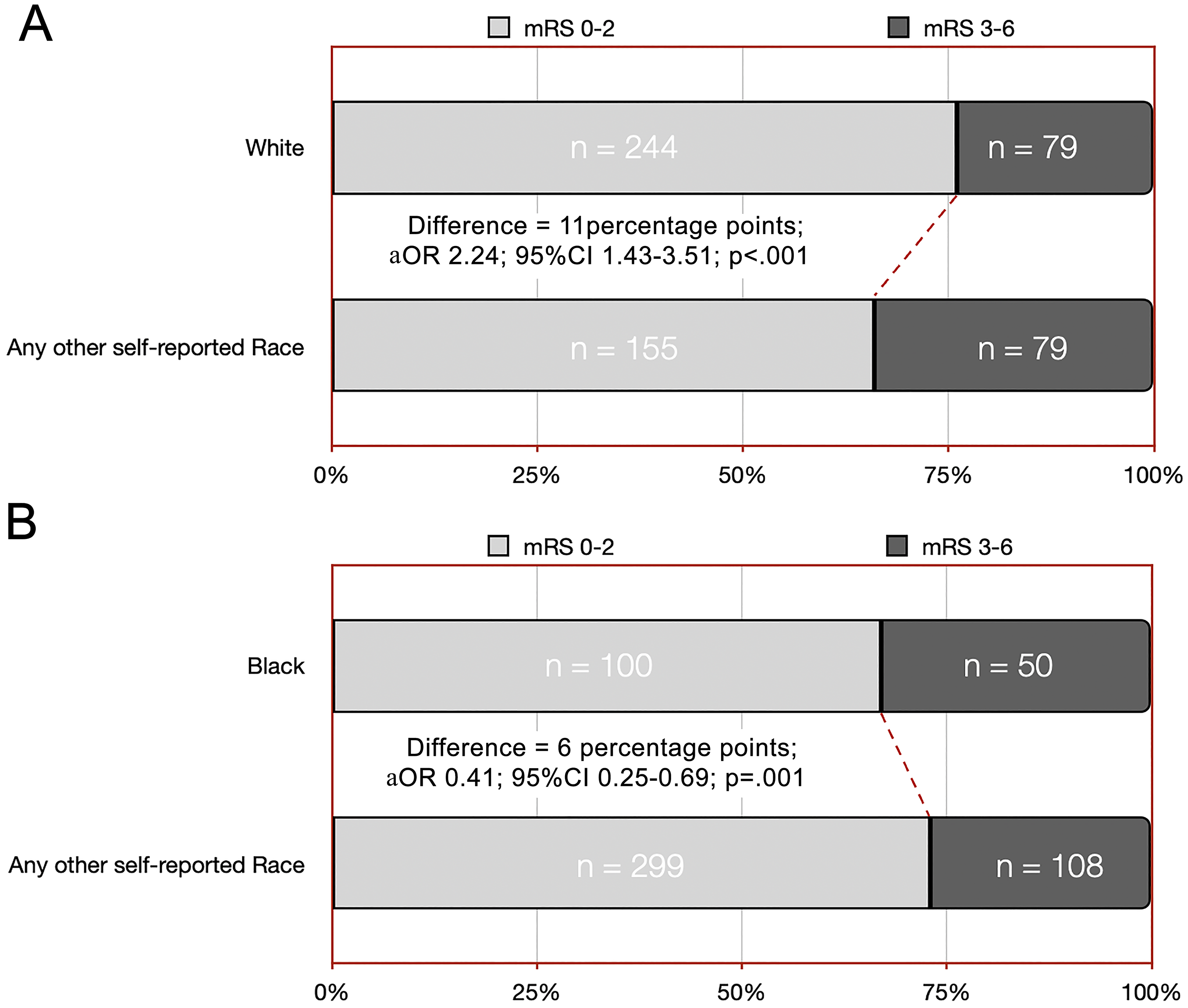
Multivariable adjusted distribution of functional independence at last follow-up by self-reported racial group. (A) Comparison of the distribution of functional independence (mRS 0–2) between White patients and other self-reported races. Among White patients, 76% (n = 244) were functionally independent and 24% (n = 79) were functionally dependent (mRS 3–6). In comparison, 66% (n = 155) of patients from other racial groups were functionally independent and 34% (n = 79) were functionally dependent. The difference between the groups was statistically significant, with an 11-percentage point difference and an aOR of 2.24 (95% CI 1.43–3.51, p < 0.001), indicating that White patients had higher odds of being functionally independent at last follow-up compared with other racial groups. (B) Comparison of functional independence between Black patients and patients of other self-reported races Of the Black patients, 67% (n = 100) were functionally independent and 33% (n = 50) were functionally dependent. Among patients from other racial groups, 73% (n = 299) were functionally independent and 27% (n = 108) were functionally dependent. The analysis revealed a 6-percentage point difference, with Black patients having lower odds of functional independence, reflected by an aOR of 0.41 (95% CI 0.25–0.69, p = 0.001). The analysis in both panels was adjusted for key confounders, including age, sex, the presence of any comorbidity (yes/no), concurrent surgery, prior subdural hematoma, use of antiplatelets/anticoagulants, bilateral procedures, anesthesia type, complications, subdural size on admission, preoperative mRS, follow-up days, center-coded variables, and the resolution of subdural hematomas. mRS: modified Rankin Scale; aOR: adjusted odds ratio; CI: confidence interval.
At their last follow-up, 76% of White patients were functionally independent, compared with 65% among all other racial groups—a significant difference of 11 percentage points after adjusting for confounders including age, the presence of any comorbidity (yes/no), and procedural details (aOR 2.24, 95% CI 1.43–3.51, p < 0.001) (Figure 2A). Conversely, Black patients were less likely to be functionally independent at their last follow-up, with 67% of Black patients categorized as functionally independent compared with 73% among all other racial groups (aOR 0.41, 95% CI 0.25–0.69, p = 0.001) (Figure 2B).
Adjusted regression analyses revealed that these differences at follow-up were not reflective of baseline trends, where White patients were more likely to present with worse baseline functional status (mRS 3–5) compared with other racial groups, whereas Black patients were more likely to present with better baseline functional status (mRS 0–2). This indicates that the observed follow-up disparities persisted despite controlling for baseline functional status and other covariates (Figure 2B).
Discussion
This multicenter retrospective cohort study is the first to examine racial disparities in procedural and clinical outcomes among patients undergoing MMAE for the treatment of CSDH, with or without concurrent evacuation surgery. Our findings reveal a notable difference between baseline and follow-up functional independence trends. At baseline, White patients were more likely to present with worse functional status compared with patients in all other racial categories, and Black patients presented with better functional status compared with patients in all other racial categories. At the last follow-up, these trends reversed—White patients had significantly higher odds (2-fold) of functional independence and Black patients had 59% lower odds of being functionally independent. These findings remained robust after adjusting for baseline mRS, subdural characteristics, clinical presentation, procedural details, and demographic factors, underscoring the potential role of postprocedural recovery disparities. We also found that Hispanic patients had 10-fold greater odds of having their CSDH resolved by more than 50% and Asian patients had a 74% lower likelihood of having resolved CSDH during follow-up.
Previous studies have documented racial and ethnic disparities, often attributed to factors such as access to care, socioeconomics, and implicit bias, in patients requiring neurosurgical interventions 16 ; however, literature addressing specific racial disparities within the population of patients with CSDH managed with MMAE is lacking. Our findings, like those of similar studies, show that minority populations often experience less favorable outcomes.17–19 For example, Black patients have been shown to have higher mortality rates and poorer functional outcomes after intracerebral hemorrhage and traumatic brain injury. 20
The observed differences in functional independence among Black patients in our study may reflect a systemic issue that extends beyond the immediate clinical care setting. The higher reoperation rates observed in White patients might reflect intrinsic differences in availability and use patterns of the healthcare system. Conversely, the lower reoperation rates in Black and Hispanic minority groups could indicate barriers to accessing subsequent care; however, this is unexplored territory with a lack of evidence. The paradoxical finding of White patients having worse preoperative functional status yet better postoperative outcomes suggests that factors including rehabilitation, social support, and healthcare navigation play an important role in driving these observations.21,22
Despite the observed differences in CSDH resolution rates among racial groups, the current literature offers no clear evidence or explanations for the significantly higher resolution rates found among Hispanic patients or the lower rates of resorption observed among Asian patients. Although biological factors may contribute to these findings, their clinical significance remains uncertain. Anatomical variations—such as the greater likelihood of the presence of dangerous collaterals in Asian patients—could play a role. However, this finding should be interpreted cautiously given the small number of patients in this cohort. Similarly, the higher rate of subdural membranes among Black patients might influence outcomes; however, the precise effects and underlying mechanisms are not yet well understood.
These disparities have important implications for clinical practice. Although our study did not directly assess factors such as access to care, socioeconomic barriers, or anatomical differences, these remain plausible contributors to the observed outcomes and warrant further investigation. There is a need for future research to identify actionable factors and tailor interventions to address them.
Limitations
This study is subject to all inherent limitations of a retrospective design, including potential selection bias. Self-reported race may not capture the complexity of patient diversity and may overlook factors unknown to the investigators. Although we adjusted for center-specific variables and known confounders in our multivariable models, unmeasured factors—such as variations in social support, insurance coverage, or rehabilitation access—may have also influenced patient outcomes. Consequently, our findings should be interpreted primarily as associative rather than definitively causal. Nevertheless, these results highlight a potentially important clinical signal of racial disparities in MMAE outcomes. Future prospective studies with larger and more diverse populations, as well as standardized protocols and more granular data on socioeconomic and healthcare access variables, will be crucial to validate these findings, explore the key drivers underlying the observed disparities, and clarify whether causal relationships exist.
Conclusion
This study highlights significant racial disparities in outcomes following MMAE for CSDH, with or without evacuation surgery. White patients had higher reoperation rates but were more likely to be functionally independent at their last follow-up. Black patients, despite better baseline functional status, had lower odds of functional independence postoperatively. Hispanic patients exhibited the highest rates of hematoma resolution and Asian patients showed the lowest rates. These findings underscore the need for further investigation into the underlying factors contributing to these disparities, including biological, socioeconomic, and healthcare-related determinants.
Supplemental Material
sj-doc-1-ine-10.1177_15910199251339536 - Supplemental material for Effect of race on procedural and clinical outcomes in middle meningeal artery embolization for primary and adjunctive treatment of chronic subdural hematoma
Supplemental material, sj-doc-1-ine-10.1177_15910199251339536 for Effect of race on procedural and clinical outcomes in middle meningeal artery embolization for primary and adjunctive treatment of chronic subdural hematoma by Santiago Gomez-Paz, Mohamed M Salem, Cordell Baker, Okkes Kuybu, Georgios S Sioutas, Kate T Carroll, Mira Salih, Adam A Dmytriw, Jane Khalife, William Smith, Diego Alejandro Ortega Moreno, Robert W Regenhardt, Nicole M Cancelliere, Alejandro M Spiotta, Omar Tanweer, Christopher J Stapleton, Michael Lang, Vitor M Pereira, Aman B Patel, Adnan H Siddiqui, Elad I Levy, Christopher S Ogilvy, Daniel Tonetti, Ajith J Thomas, Visish M Srinivasan, Brian T Jankowitz, Michael R Levitt, Bradley A Gross, Jan-Karl Burkhardt and Ramesh Grandhi in Interventional Neuroradiology
Footnotes
Acknowledgements
The authors thank Cortlynd Olsen and Kristin Kraus for editorial assistance.
Data availability
Data are available upon reasonable request to the corresponding author.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: SG-P, MMS, CB, OK, GSS, KTC, MS, AAD, JK, WS, DAOM, RWR, NMC, OT, CJS, ML, VMP, CSO, DT, VMS, BTJ: No relevant relationships. AMS receives research support from RapidAI, Penumbra, Medtronic, MicroVention, and Stryker and is a consultant for Penumbra, MicroVention, and RapidAI. ABP is a consultant for Penumbra, MicroVention, and Medtronic. AHS is a consultant for Adona Medical, Inc., Basecamp Vascular SAS, Bend IT Technologies, Ltd, BlinkTBI, Inc., Borvo Medical, Inc., Cerebrotech Medical Systems, Inc., Code Zero Medical, Inc., Cognition Medical, Collavidence, Inc., CVAID Ltd, E8, Inc., Endostream Medical, Ltd, Galaxy Therapeutics, Inc., Hyperion Surgical, Inc., Imperative Care, Inc., InspireMD, Ltd, Instylla, Inc., Launch NY, Inc., Neurolutions, Inc., NeuroRadial Technologies, Inc.(Sold to Medtronic in 2021), Neurovascular Diagnostics, Inc., Peijia Medical, PerFlow Medical, Ltd, Piraeus Medical, Inc., Q’Apel Medical, Inc., QAS.ai, Inc., Radical Catheter Technologies, Inc., Rebound Therapeutics Corp. (Purchased 2019 by Integra Lifesciences, Corp), Rist Neurovascular, Inc. (Purchased 2020 by Medtronic), Sense Diagnostics, Inc., Serenity Medical, Inc., Silk Road Medical, Sim & Cure, Spinnaker Medical, Inc., StimMed, LLC, Synchron, Inc., Tulavi Therapeutics, Inc., Vastrax, LLC, Viseon, Inc., Whisper Medical, Inc., Willow Medtech, Inc., Amnis Therapeutics, Apellis Pharmaceuticals, Inc., Boston Scientific, Canon Medical Systems USA, Inc., Cardinal Health 200, LLC, Cerebrotech Medical Systems, Inc., Cerenovus, Cordis, Corindus, Inc., Endostream Medical, Ltd, Hyperfine Operations, Inc., Imperative Care, InspireMD, Ltd, Integra, IRRAS AB, Medtronic, MicroVention, Minnetronix Neuro, Inc., Peijia Medical, Penumbra, Piraeus Medical, Inc., Q’Apel Medical, Inc., Rapid Medical, Serenity Medical, Inc., Silk Road Medical, StimMed, LLC, Stryker Neurovascular, VasSol, Viz.ai, Inc., Cerenovus EXCELLENT and ARISE II Trial; Medtronic SWIFT PRIME, VANTAGE, EMBOLISE and SWIFT DIRECT Trials; MicroVention FRED Trial & CONFIDENCE Study; MUSC POSITIVE Trial; Penumbra 3D Separator Trial, COMPASS Trial, INVEST Trial, MIVI neuroscience EVAQ Trial, Rapid Medical SUCCESS Trial, and InspireMD C-GUARDIANS IDE Pivotal Trial. EIL has shareholder/owner interest in NeXtGen Biologics, RAPID Medical, Claret Medical, Cognition Medical, Imperative Care (formerly the Stroke Project), Rebound Therapeutics, StimMed, Three Rivers Medical. Dr Levy has a patent for Ultrasonic Surgical Blade and has National PI for Medtronic (merged with Covidien Neurovascular)–Steering Committees for SWIFT Prime and SWIFT Direct Trials, Site PI: Stratis Study Sub 1, MicroVention-Site PI: CONFIDENCE Study. Dr Levy has an Honorarium for Training & Lectures by Medtronic (formerly Covidien Neuro-vascular), Penumbra, Microvention, Integra, and is a consultant for Clarion, GLG Consulting, Imperative Care (formerly the Stroke Project), Medtronic (formerly Covidien Neurovascular), StimMed, Misionix, Mosiac. Dr Levy is Chief medical Officer at Haniva Technology and is on the Advisory Board for Stryker (AIS Clinical Advisory Board), NeXtGen Biologics, MEDX, Cognition Medical, Endostream Medical, IRRAS AB (Consultant/Advisory Board). Dr Levy has a Site PI Study for Microvention (CONFIDENCE Study), Medtronic (STRATIS Study—Sub I). Dr Levy is in a leadership or fiduciary position in other board, societies, committees, or advocacy groups, paid or unpaid, for CNS, ABNS, UBNS, and renders medical/legal opinions as an expert witness. AJT receives consulting fees from Stryker, Medtronic, and Cerevasc. MRL: Unrestricted educational grants from Medtronic and Stryker; consulting agreements with Aeaean Advisers, Metis Innovative, Genomadix, AIDoc, and Arsenal Medical; equity interest in Propio, Stroke Diagnostics, Apertur, Stereotaxis, Fluid Biomed, Synchron, and Hyperion Surgical; editorial board membership for the Journal of NeuroInterventional Surgery; and participates in the data safety monitoring board of Arsenal Medical. BAG: Consulting fees from Medtronic and MicroVention. JKB: Consulting fees from Q`Apel Medical, Stryker, Medtronic, Cerenovous, and MicroVention. RG: Consulting fees from Medtronic Neurovascular, Balt Neurovascular, Stryker, Rapid Medical, and Cerenovus.
Ethical approval
This study exclusively used data from a multicenter repository of previously treated patients, which was anonymized and de-identified before analysis. The database adhered to institutional review board requirements and ethical guidelines from each participating center at the time of initial data collection.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.