
Abstract
Background
Supportive guide catheters are needed to navigate large endovascular devices through complex cerebral vasculature. The Q'Apel SelectFlex family of distal access guide catheters may eliminate the need for triaxial systems through a simplified biaxial approach with reduced costs and similar effectiveness as traditional systems.
Methods
A retrospective review of patients who underwent neuroendovascular interventions using SelectFlex catheters at 4 US sites between April 2021 and August 2022 was performed. We assessed the ability to successfully access the target location (biaxially or triaxially), the need for a bailout intermediate catheter (when performed biaxially), and adverse events (AE) attributed to SelectFlex.
Results
A total of 366 patients (66.9% [245/366] female; mean age: 58.3 ± 13.3) who underwent a cerebrovascular intervention with the SelectFlex system were included. The procedures performed were aneurysm embolization (251/366, 68.6%; coiling: 130/366, 35.5%, flow diversion: 121/366, 33.1%), middle meningeal artery embolization (10.1%, 37/366), Woven EndoBridge deployment (7.9%, 29/366), ruptured arteriovenous malformation/dural arteriovenous fistula embolization (4.6%, 17/366), tumor embolization (2.7%, 10/366), carotid stenting (1.9%, 7/366), percutaneous transluminal angioplasty (1.6%, 6/366), venous sinus stenting (1.1%, 4/366), and parent vessel occlusion for trauma/aneurysm (0.5%, 2/366). Transfemoral and transradial access were each used in 180 (49.2%) cases. Successful placement occurred in 100% of cases (366/366). In cases performed biaxially, 4.1% (13/320) required the addition of an intermediate catheter. One SAE related to SelectFlex occurred (0.3%).
Conclusions
This study demonstrates good performance and safety with SelectFlex in a variety of neurointerventional procedures. SelectFlex may reduce the need for triaxial support.
Introduction
As the neuroendovascular surgery space continues to evolve, new procedures and devices such as flow diversion, intrasaccular devices, middle meningeal artery (MMA) embolization, intracerebral hemorrhage (ICH) evacuation, cerebrospinal fluid diversion and venous sinus stenting are added at an impressive pace. These procedures encompass all areas of the cerebrovascular anatomy, including arterial and venous systems, requiring robust, stable access to the target anatomy.1,2 Traditionally, this has been achieved with triaxial guide catheter systems comprised of a long sheath, intermediate guide catheter, and a microcatheter. 1 Triaxial systems are limited by the intermediate catheter inner diameter (ID) which limits device compatibility and bailout options. In addition, the triaxial set-up requires additional time to set up, costs, and multiple flushes which could potentially increase the risk of thromboembolic complications.3–6
A biaxial approach using a guide catheter and microcatheter can simplify neuroendovascular procedures by eliminating the need for an intermediate catheter, thereby potentially reducing costs, operating time, number of flushes, and could potentially eliminate constraints for devices used and bailout limitations related to intermediate catheter ID. To fully replace the triaxial approach, a biaxial system would need to achieve a position which provides a stable platform to deliver a broad spectrum of devices across a variety of neurovascular interventions. There is a need for a versatile distal access catheter that provides adequate support in a variety of complex indications without using an intermediate catheter to simplify procedures, reduce costs and procedure time.
The Q'Apel SelectFlex Neurovascular Access System Family (SelectFlex, Q’Apel Medical, Inc., Fremont, California, USA) is a novel group of 7 Fr 0.72-inch distal access guide catheters designed to overcome many of the limitations of a triaxial system. The SelectFlex catheters are designed to be used ubiquitously across the spectrum of neurovascular interventions. We present our collective early experience with SelectFlex guide catheters.
Methods
Study design and patient selection
A multicenter retrospective review of consecutive patients who underwent a neurovascular interventional procedure performed with the SelectFlex System at 4 sites in the United States between April 2021 and August 2022 was performed.
Data collection and endpoints
Baseline demographic and clinical information, date of the procedure, institution where the procedure was performed, intended procedure, and final guide catheter placement at pre-defined segments (cervical, petrous, cavernous, paraclinoid) of the internal carotid artery 1 or vertebral artery were recorded. Procedural characteristics including procedure type, access site, guide catheter location, and intermediate catheter support (planned or not). Intermediate support was defined as the use of any intermediate distal access catheter in addition to the device delivery microcatheter. Adverse events (AE), serious adverse events (SAE), and any AE or SAE related to the device were recorded.
Performance endpoints included the ability to successfully access the target location (biaxially or triaxially), and the need for a bailout intermediate distal access catheter (when performed biaxially). Safety endpoints included completion of the procedure without the occurrence of AE attributed to SelectFlex.
SelectFlex devices
The SelectFlex System is composed of a SelectFlex Neurovascular Access Catheter, a 3cc Mode Control Syringe, a peel away Introducer, Luer Activated Valve, and a dilator. The SelectFlex Neurovascular Access Catheter is a 7 Fr guide catheter that was originally available in two lengths (95 and 105 cm) with variable stiffness, transitions, and hydrophilic coating along its length and an inner diameter of 072. The catheters have a novel, proprietary, physician-activated dual mode stiffness mechanism on the distal portion of the catheter that allows the device to transition between a supple track mode and a stiffer support mode.
Statistical analysis
The data for this study was imported into R (version 4.2.2) using the ‘readxl’ package and cleaned with the ‘tidyverse’ package. Prior to analysis, the dataset underwent refinement, including standardization of dates, confirmation of data type integrity, conversion of categorical data to factors, and handling of missing entries by assigning default values.
Descriptive statistics for baseline continuous variables were summarized using means, standard deviations (SD), medians, and interquartile ranges (IQR), while categorical variables were presented as counts and percentages. Ninety-five percent confidence intervals (95% CI) for primary outcomes were calculated using the Clopper-Pearson exact binomial method. AEs were reported descriptively as counts and percentages. The data for this study are available from the corresponding author upon reasonable request.
Ethical considerations
Local IRB approval was obtained from each institution.
Results
Patients and procedures
Patient and procedure characteristics are presented in Table 1. A total of 366 patients were included (females: 245 [66.9%]) with an average age of 58.3 ± 14.3 years. The majority of cases were in the anterior internal circulation (259/366, 70.8%), followed by external (59/366, 16.1%), posterior (43/366, 11.7%) and venous (4/366, 1.1%) circulations. There were an equal number of femoral and radial access cases with 180 (49.2%) each, and 4 (1.6%) venous cases. The SelectFlex was most commonly placed in the petro-cavernous ICA (231/366, 63.1%).
Summary of patient and procedure characteristics.
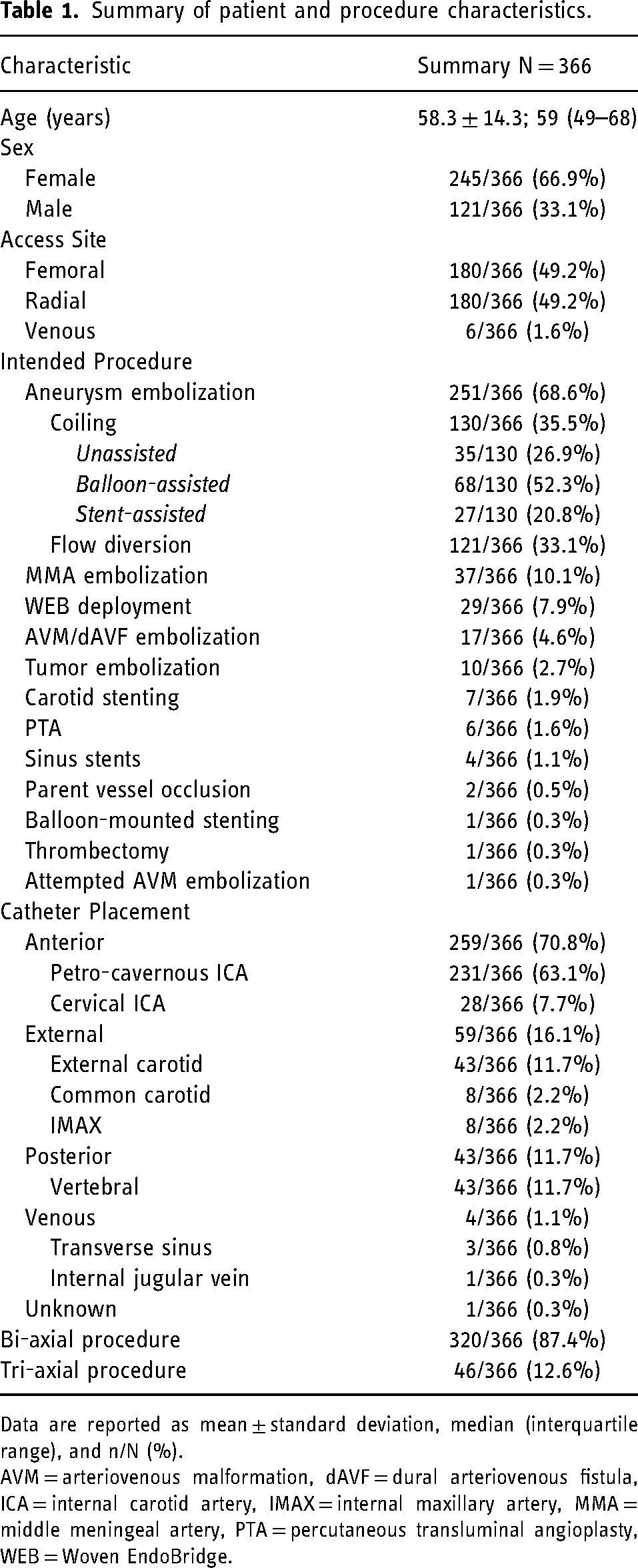
Data are reported as mean ± standard deviation, median (interquartile range), and n/N (%).
AVM = arteriovenous malformation, dAVF = dural arteriovenous fistula, ICA = internal carotid artery, IMAX = internal maxillary artery, MMA = middle meningeal artery, PTA = percutaneous transluminal angioplasty, WEB = Woven EndoBridge.
The most common procedure performed was treatment of intracranial aneurysms (251/366, 68.6%) (205/366 [56%] unruptured and 95/366 [26%] ruptured aneurysms). Of those, 130/366 (35.5%) were coiled, 121/366 (33.1%) were treated with flow diversion, and 29/366 (7.9%) were treated with Woven EndoBridge (WEB) embolization. Additional procedures included MMA embolization (37/366, 10.1%), ruptured arteriovenous malformation (AVM)/dural arteriovenous fistula (dAVF) embolization (17/366, 4.6%), tumor embolization (10/366, 2.7%), carotid stenting (7/366, 1.9%), percutaneous transluminal angioplasty (PTA) (6/366, 1.6%), sinus stents (4/366, 1.1%), and parent vessel occlusion (PVO) of vessel due to trauma (2/366, 0.5%); balloon-mounted stent, thrombectomy, and attempted AVM embolization that failed because of distal tortuosity each accounted for 1 case (0.3%).
Of the 366 cases 46 (12.6%) were performed triaxially initially, 41 of which were performed at a single center and are reflective of their practice where a tri-axial set-up is standard. The remaining 320/366 (87.4%) cases were performed biaxially.
Performance and safety outcomes
A summary of the study outcomes is presented in Table 2. Technical success in guide catheter placement was achieved in 100% of cases (95% CI: 99.0–100%). However, there were 4/366 (1.1%; 95% CI: 0.3–2.8%) cases where the guide catheter did not reach the intended location. A total of 13/320 (4.1%, 95% CI: 2.2–6.8%) biaxial cases required the addition of an intermediate catheter to successfully complete the procedure. Of these 13 cases; 11 were radial and 2 were with femoral access. A majority of these were flow diversion procedures (7/13, 53.8%), 3/13 (23.1%) were aneurysm coil embolizations, 1/13 (7.6%) was a WEB embolization (large MCA bifurcation aneurysm), and 2/13 (15.4%) were distal AVM embolizations.
Summary of primary outcomes.
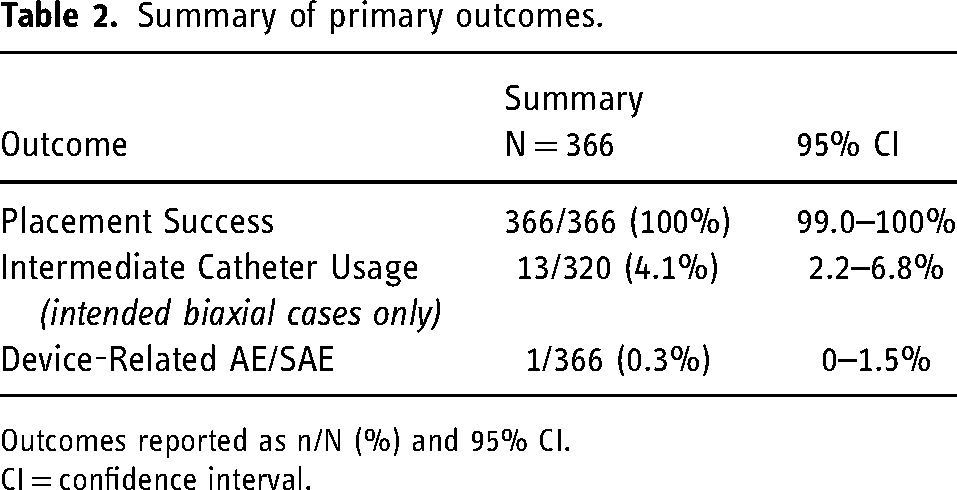
Outcomes reported as n/N (%) and 95% CI.
CI = confidence interval.
Adverse events
A summary of AEs and SAEs is found in Table 3. A total of 13 AEs occurred across 10 patients (2.7% with ≥1 AE). Of these cases, there were 10 SAEs which occurred in 9 patients (2.5% with ≥1 SAE). Procedure-related AEs included one case of branch occlusion and two non-flow limiting dissections which were unrelated to the device and required no additional intervention. SAEs included three cases of intraoperative aneurysm rupture and one case each of contrast media extravasation, dissection, metabolic encephalopathy, and recurrent nosebleeds. Only one SAE was directly related to the use of SelectFlex (0.3%; 95% CI: 0–1.5%), which was a single case of flow-limiting dissection in a tortuous internal carotid artery tonsillar loop that required stenting to restore patency and flow. This occurred during a stent-assisted coiling for an A1-A2 aneurysm.
Summary of adverse events and serious adverse events.
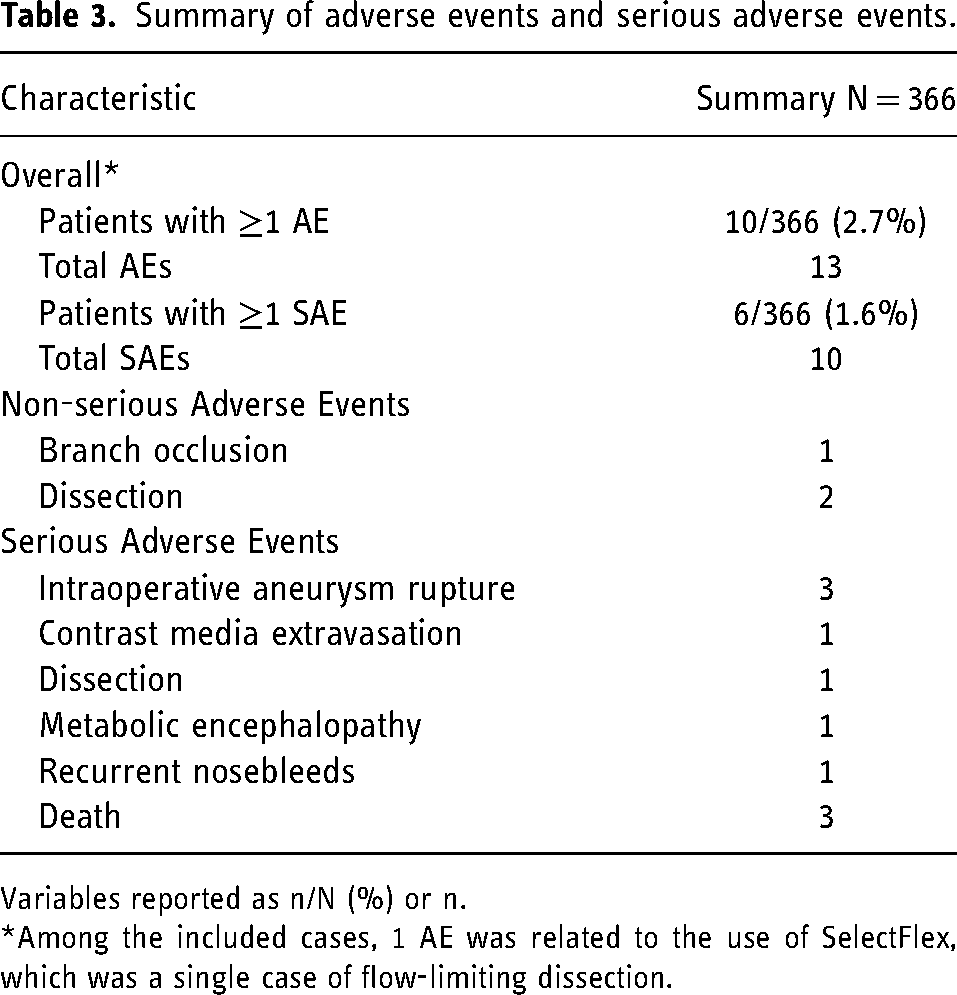
Variables reported as n/N (%) or n.
*Among the included cases, 1 AE was related to the use of SelectFlex, which was a single case of flow-limiting dissection.
Additionally, there were 3 deaths, none of which were related to the SelectFlex system. The first was an in-hospital death of a patient with a large frontal parenchymal hemorrhage with SAH who had undergone balloon angioplasty for vasospasm. The patient expired from sequelae of IPH. The second patient presented with a HH4F4 SAH and had undergone treatment of a ruptured PCOM aneurysm. This patient expired from sequelae of SAH. Another case, occurring after hospital discharge, was also due to SAH-related sequelae in a patient who had undergone coiling in the vertical petrous ICA via transradial access (TRA). The third death occurred in an elderly patient who presented with multiple aneurysms, extensive intracranial atherosclerotic disease, and occlusion of the basilar artery. The patient had extremely tortuous vessels, and upon advancement of a balloon experienced a dissection and extravasation of contrast. The patient was discharged from hospital (mRS 5) and eventually expired.
Discussion
The foundation of any successful embolization procedure is a stable access platform. As neurointerventional procedures have become more complex, utilizing larger devices, the guide catheter and access systems have evolved. Earlier systems were relatively simple, such as the 6 Fr Envoy XB (Cordis, Miami Lakes, FL) designed for placement in the cervical carotid and to resist axial loads, which were effective for simple coiling procedures. Evolution of the simple guide catheters revolved around the introduction of the novel Penumbra Benchmark (Penumbra, Inc. Alameda, CA) guide catheter which had a distal flexible tip that allowed the catheter to be placed beyond the cervical segment of the carotid. The distal placement was shown to be safe and reduced the incidence of dissections and catheter related vasospasm. 5 This distal access guide catheter achieved stability with geometric anchoring, using the turns of the petrous and cavernous carotid to “anchor” the device in place, eliminating much of the axial loading seen in traditional guide catheters. This distal placement also helped overcome challenges from tortuous anatomy where traditional guide catheters had to remain proximal. With the introduction of flow diverters, there was a need for more robust systems. Delivery of earlier flow diverters was challenging largely due to the stiffness of the system. Traditional guide catheters did not offer the support needed to deliver these systems and there was a shift to triaxial support systems consisting of a robust long 6f sheath and an intermediate catheter. This system provided the support needed to deliver larger systems but came with a significant limitation, namely a smaller ID of the intermediate catheter, which allowed delivery of 0.27-inch catheter distally but limited an operator's ability to deliver two microcatheters. Tri-axial systems also require multiple flushes and may require a larger femoral sheath for access. As catheter technology continued to improve, navigable, larger systems able to provide more distal access while also being able to navigate proximal tortuous anatomy have become available. These larger systems do come at a cost, namely larger femoral access with potential increases in access site complications. An ideal system needs to balance the challenges of delivering larger, stiffer embolization devices distally with an adequate ID that allows for appropriate bailout techniques when needed, while overcoming challenging cerebrovascular anatomy at an OD size that mitigates access site complications.
Biaxial systems have many benefits; primarily, the need for fewer access devices which ultimately result in reduced procedure and fluoroscopy time, costs, complexity, and fewer complications compared to triaxial systems.4–6 A 2020 retrospective study by Vakharia, et al. compared biaxial (49 patients) versus triaxial (33 patients) systems in patients undergoing embolization procedures with Pipeline for intracranial aneurysms and found significantly decreased procedure time (24.0 ± 18.7 min vs. 38.4 ± 31.1 min, p = 0.005), fluoroscopy time (28.8 ± 23.0 min vs. 50.3 ± 27.1 min, p = 0.001), and radiation exposure (1243.7 ± 808.2 mGy vs. 2074.6 ± 1505.6 mGy, p = 0.003) with biaxial systems, without significant differences in clinical outcomes or complications. 3 The same study also reported cost savings for procedures performed using biaxial systems ($1790 vs. $3285), with intermediate catheter usage driving the difference in costs. 3
A major limitation of biaxial systems is the inability to provide distal access or support to deliver large devices. This may require the addition of an intermediate catheter for more distal access to reach the target lesion. In our series of the procedures initially performed bi-axially only 4% (13/320) required additional support with an intermediate catheter. The majority of these cases were flow diversion (7) embolization cases (other cases included 2 stent assisted coiling cases, 2 AVM embolizations, 1 coiling of a distal pericallosal aneurysm, and 1 WEB embolization of a large MCA aneurysm). Given that larger devices require more force to be advanced and delivered to the target vessel, it is impressive that a small portion of cases required an additional intermediate catheter which speaks to the SelectFlex catheters ability to navigate distally and provide adequate support. Additionally, we did not experience any device kinking or prolapse as reported by others. 7
Recently there has been a push for many of the procedures to be performed transradially due to a perceived safety benefit. TRA presents its own unique set of challenges with a smaller access artery, anatomy that requires different transitions and areas for support. Indeed, there are dedicated “radial” access catheters; however, one of the advantages of the SelectFlex catheters is that it is ubiquitous and performs equally well femorally or radially. 8 Procedural success in this study is comparable to other studies assessing the safety and efficacy of other guide catheters.9–11 A 2021 retrospective study by Hassan, et al. 12 evaluated 68 patients who underwent various neuroendovascular procedures (mechanical thrombectomy, carotid stenting, liquid embolization, flow diversion, endovascular coiling, balloon angioplasty) in several anatomic locations via both TFA (76% of cases) and TRA (24% of cases) with the Ballast Long Guiding Sheath and reported a 100% technical success rate. A 2024 retrospective study by Saei, et al. 13 evaluated 60 patients who underwent various neuroendovascular procedures in various anatomic locations via both TFA (95% of cases) and TRA (5% of cases) with the Fubuki XF Guide Catheter and reported a technical success rate of 100%. Of note, all procedures in Hassan, et al. and Saei, et al. were performed using a triaxial system12,13 where in our large case series the majority of cases were performed bi-axially with 100% placement success and only one significant catheter related complication.
There was one procedure-related complication related to guide catheter access in our series; a flow limiting dissection of a tortuous common carotid which occurred during a stent-assisted coiling procedure of an A1-A2 junction aneurysm. This is comparable to the studies by Hassan and Saei, et al. that reported no complications attributed to guide catheters.12,13 Recent studies have also assessed complication rates for neuroendovascular procedures performed transradially. A 2020 systematic review by Joshi, et al. assessed 21 studies comprising 1342 patients using TRA for various neurointerventional treatments, reporting a minor complication rate of 2.75% and a major complication rate of 0.15% for TRA procedures. 9 Other studies have reported TRA complication rates of 0–2%,14,15 and TFA complication rates of 6.5–7%.14,15 These rates are comparable to the findings in our study, highlighting the versatility of SelectFlex for use on multiple access routes.
Limitations
Limitations of this study include the retrospective nature of the study and the lack of a comparator group. Additional analyses are needed to compare the outcomes of SelectFlex to other distal access guide catheters.
Conclusion
This study demonstrates the versatility, safety, and effectiveness of the SelectFlex guide catheters across a variety of neuroendovascular procedures. The SelectFlex guide catheter is unique in that it can be used across the entire spectrum of interventional cases regardless of access route (TFA, TRA, TV), procedure type (hemorrhagic or ischemic cases), or target location (internal, external carotid, vertebrobasilar, or venous). Furthermore, the catheter is supple enough to overcome challenging tortuous anatomy and robust enough to provide adequate support. It may simplify procedures by reducing the need for a triaxial system and result in cost savings from not routinely using an intermediate catheter.
Footnotes
Acknowledgements
The authors acknowledge Superior Medical Experts for medical writing and statistical assistance. Superior Medical Experts is submitting on behalf of the authors with their approval.
Author contributions
All authors made substantial contributions to the conception or design of the work or the acquisition, analysis, or interpretation of data; drafted or reviewed the manuscript critically for intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. IC acts as the guarantor of this study.
Ethical considerations
This study received ethical approval from the Baylor College of Medicine IRB (protocol #16–58, August 7, 2017; protocol #H-43183, February 16, 2021; protocol #850268, December 15, 2021).
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Declaration of conflicting interests
MIC serves as a consultant for Q’Apel Medical, Inc., Imperative Care, Cerenovus, Microvention, Medtronic, Kaneka, Vasorum. MIC has equity interest in Borvo Medical, Echovate, Endostream, FreeOx, Imperative Care, Q’apel Medical, RIST, Sealonix, Serenity, Synchron, The NEAR Center, Three Rivers Medical, Tulavi, Truvic, VMT Medical, Vastrax, Vasorum, Viseon. RH reports grants from the National Institutes of Health, Microvention, Interline Endowment, Stryker, and CNX; consulting fees from Medtronic, Cerenovus, Balt, Rapid Medical, Stryker, Microvention, Phenox, and Q'Apel Medical, Advisory board for MiVi, Three Rivers Medical, Shape Medical, eLum, and Corindus, holds equity in InNeuroCo, eLum, Three Rivers Medical, Rist, Corindus, Cerebrotech, Endostream, Scientia, BlinkTBI, and NTI. OC is a consultant for Medtronic, Stryker, Microvention, Siemens, Balt, Q'Apel Medical, Scientia, EO Solutions, Nuvascular; received honoraria from Serenity Medical. JKB Consultant for Stryker, Microvention, Q'Apel Medical, Siemens, BALT, Cerenovus. OT Consultant for Stryker, Viz Ai, Penumbra, Inc, Balt, Imperative Care, Microvention, Q’apel Medical. Educational/Research Grants from Q’apel. AST claims equity in Q’apel and Imperative Care and serves as CMO for Imperative Care. VS serves as a consultant for Stryker, Cerenovus, Imperative Care, Rapid AI, and NFL, and reports grant support from Medtronic and Stryker. RDT serves as a consultant for Silk Road Medical, Medtronic, Integra LifeSciences. Is an employee of Siemens Healthineers and has equity interest in Q’Apel Medical, Endostream, Viseon, Borvo Medical, E8, Ischmicure, The NEAR center, Echovate. JV serves as a consultant to Imperative Medical, Viz.AI, Precision Neuro, Telos, Kaneka, Q'Apel Medical, Medtronic, and Scientia; and owns stock in Radial, Synchron, Borvo, Imperative, and Viz.AI. All other authors have nothing to disclose.
Funding
Support for this study and manuscript development was provided by Q'Apel Medical, Inc.
Data availability
Data will be available upon reasonable request by the corresponding author.