
Abstract
Background
Therapeutic occlusion of major cerebral arteries is sometimes required in pediatric cerebrovascular conditions of the head and neck. However, this procedure carries a considerable risk of stroke and de novo intracranial aneurysm formation. This study aims to assess the long-term clinical and radiographic outcomes of therapeutic cerebral artery occlusion in a pediatric cohort.
Methods
A retrospective review was conducted on pediatric patients who underwent endovascular therapeutic occlusion between January 2002 and June 2023. Clinical presentation, radiographic findings, management strategies, and follow-up data were analyzed.
Results
Eighteen children (male-to-female ratio: 2:1, mean age: 8.8 years) were included. Most cases (83%) were symptomatic at presentation. The diagnoses included aneurysm (44.4%), arterial dissection (22.2%), arteriovenous shunting (22.2%), and craniocervical neoplasm (11.1%). Eight patients underwent carotid circulation occlusion, and 10 underwent vertebrobasilar system occlusions; the majority (77.7%) were performed electively. Detachable coils were the primary devices used. Complete occlusion was observed in 89.9% of cases on immediate control angiography, and repeat embolization was performed in 2 cases. Perioperative ischemic strokes were observed in five cases: three asymptomatic and two with mild symptoms that completely resolved on follow-up. No new infarcts, transient ischemic attacks, de novo intracranial aneurysms, or mortality were observed over a mean clinical and radiographic follow-up duration of 6.9 years and 4 years, respectively.
Conclusions
Therapeutic occlusion of major cerebral arteries appears to be a safe and effective treatment in pediatric patients. Nevertheless, long-term follow-up is recommended due to the theoretical risk of de novo aneurysm formation over their lifespan.
Keywords
Introduction
Therapeutic parent artery occlusion (PAO) is a well-established treatment for complex pathologies of the head and neck that are not amenable to reconstructive vascular approaches. 1 PAO has been successfully employed in the management of various challenging pediatric cases, including complex aneurysms,2–11 arteriovenous shunts,12,13 vascular injuries,14,15 and conditions requiring presurgical PAO.4,16–18 Despite the usefulness of balloon test occlusion (BTO) as a preoperative tool, the deconstructive nature of PAO inherently carries the risks of ischemic complications, as well as the potential for delayed de novo aneurysm formation.19–25
We describe our single-center experience with endovascular PAO in children with various head and neck pathologies, with a focus on the long-term clinical and radiographic outcomes.
Methods
Patient selection and description
The ethics committee and the research review board of our institution reviewed and approved the study protocol. A retrospective review of a prospectively maintained cerebrovascular database between January 2002 and June 2023 was performed. Patients aged ≤18 years who underwent endovascular PAO of major cerebral arteries, including the common carotid artery (CCA), internal carotid artery (ICA), vertebral artery (VA), and basilar artery (BA), were identified. Electronic medical records and radiographic images were reviewed, and the following data were collected: demographics, presentation, diagnosis, treatment details, and angiographic and clinical outcomes. One patient was lost to follow-up and was excluded from the analysis. Three patients in this study had been previously reported in the literature.13,16,26
All patients underwent either endovascular trapping or proximal arterial occlusion under general anesthesia. The specific treatment method was selected based on the affected arterial segment and underlying pathology. When feasible, a preoperative BTO was performed through angiographic assessment in all cases. Neurological examinations and/or adjunctive electroencephalography (EEG) monitoring were conducted as appropriate in some instances. A successful BTO was determined by the presence of adequate collateral circulation to the occluded territory, as indicated by a venous delay of ≤2 s or a stable neurological examination and EEG. A favorable clinical outcome was classified as both a Glasgow Outcome Scale (GOS) score of >4 and a return to the neurological baseline at the last follow-up.
Statistical analysis
Summary statistics of continuous variables are reported as mean ± SD and range, and categorical variables are reported as frequency counts and percentages. Comparative statistics were not performed due to the small sample size.
Results
Demographics and presentations
Eighteen children were included in the study, with a male-to-female ratio of 2:1. The mean age of the patients was 8.8 ± 5.6 years, ranging from 0.6 to 17.4 years. Most patients (15, 83%) were symptomatic at presentation. Eight patients (44.4%) underwent endovascular occlusion for arterial aneurysms, four (22.2%) for arterial dissections, four (22.2%) for arteriovenous shunting, and two (11.1%) for presurgical tumor resections. A variety of comorbidities were observed in eight patients. Eight patients underwent occlusion of the carotid artery and its branches, while 10 patients underwent occlusion of the vertebrobasilar system. Fourteen of the procedures were performed electively. Four patients required emergency or urgency treatment: one presented with cervical ICA dissection and a history of massive bleeding (Figure 1); another had a ruptured recurrent distal ICA aneurysm with intracranial hemorrhage; a third had vertebral artery dissection with recurrent basilar artery occlusion; and one patient had a ruptured cervical cord perimedullary arteriovenous fistula (AVF) with rapidly progressive symptoms. Detailed patient data are presented in Table 1.
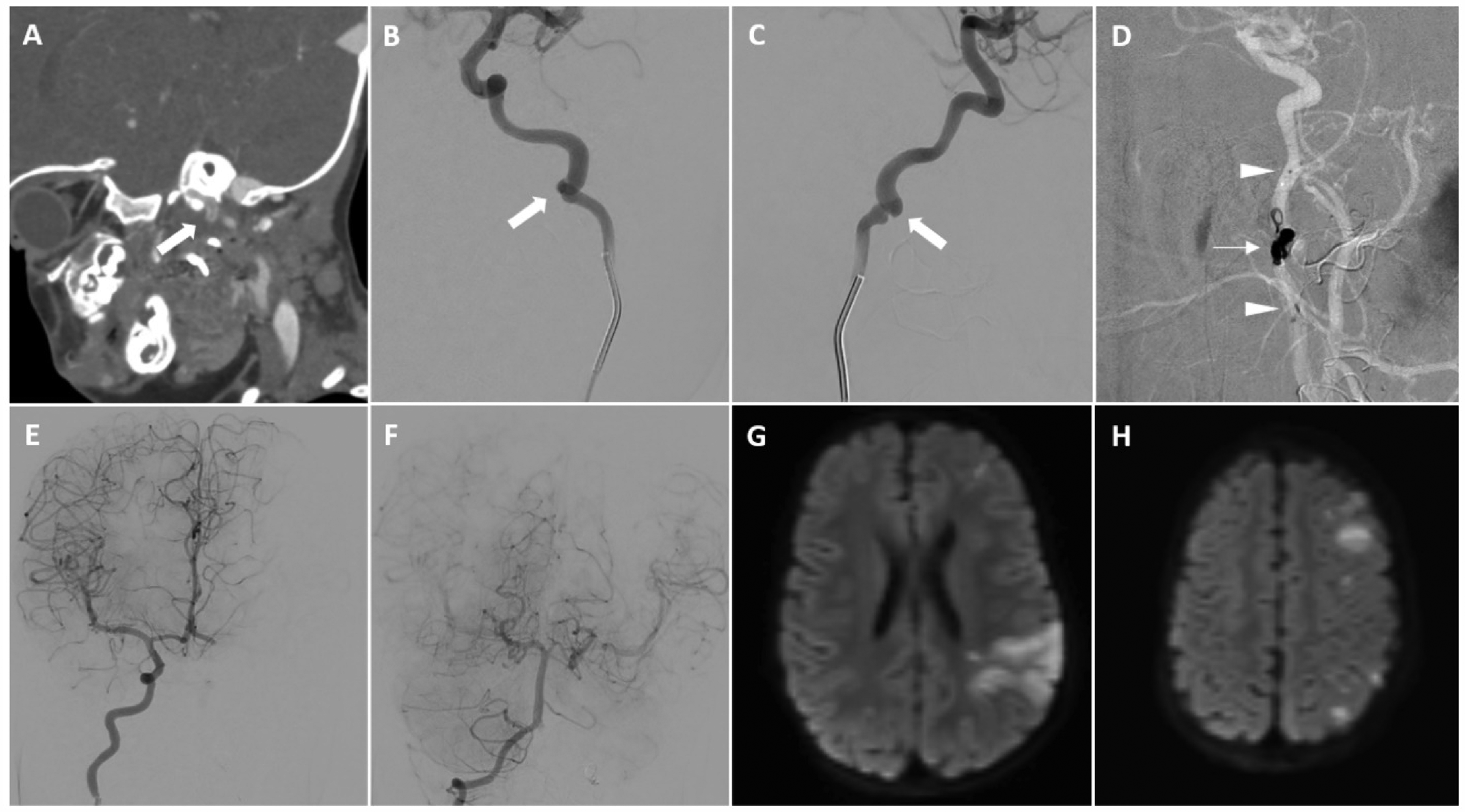
Case 9: A 1-year-old girl presented with massive bleeding after adenoidectomy and a history of hemodynamic instability. CTA of the brain and neck (A) detects an intraluminal flap (bold arrow) at the distal left cervical ICA and thromboembolic infarction in the left parietal lobe (not shown). A left ICA angiogram (B and C) reveals focal irregularity at the distal left cervical ICA (bold arrow). A roadmap image of left CCA during embolization (D) shows trapping occlusion of the left ICA with microvascular plugs (arrowheads) and coils (arrow). Right ICA (E) and right VA (F) angiograms, post parent artery occlusion, show good collateral circulation to the left MCA territory. An immediate brain MRI (G and H) reveals acute infarctions in the left parietal lobe and cortical watershed zone of the left cerebral hemisphere.
Details of 18 pediatric patients who underwent therapeutic occlusion of major cerebral arteries.
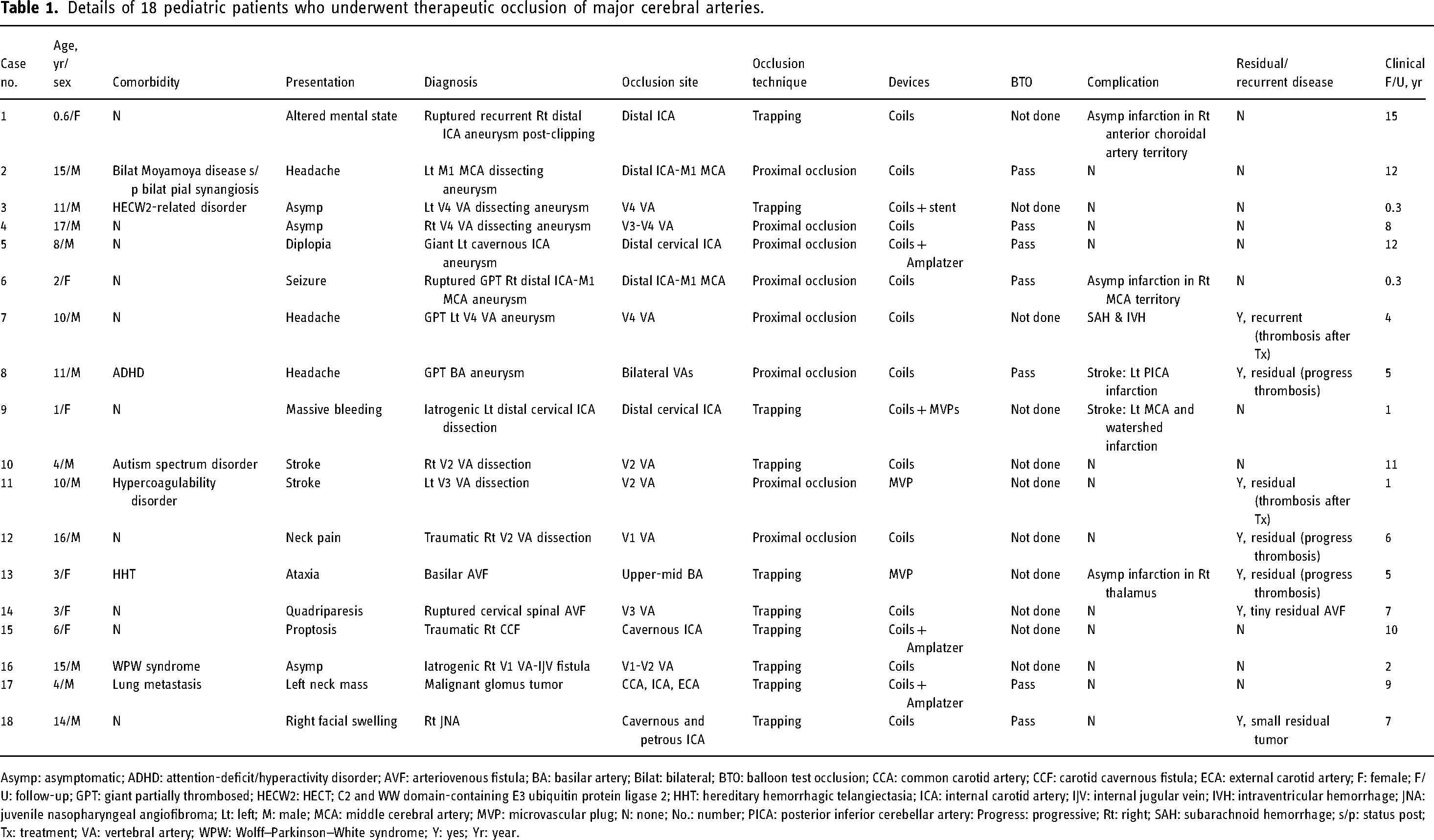
Asymp: asymptomatic; ADHD: attention-deficit/hyperactivity disorder; AVF: arteriovenous fistula; BA: basilar artery; Bilat: bilateral; BTO: balloon test occlusion; CCA: common carotid artery; CCF: carotid cavernous fistula; ECA: external carotid artery; F: female; F/U: follow-up; GPT: giant partially thrombosed; HECW2: HECT; C2 and WW domain-containing E3 ubiquitin protein ligase 2; HHT: hereditary hemorrhagic telangiectasia; ICA: internal carotid artery; IJV: internal jugular vein; IVH: intraventricular hemorrhage; JNA: juvenile nasopharyngeal angiofibroma; Lt: left; M: male; MCA: middle cerebral artery; MVP: microvascular plug; N: none; No.: number; PICA: posterior inferior cerebellar artery: Progress: progressive; Rt: right; SAH: subarachnoid hemorrhage; s/p: status post; Tx: treatment; VA: vertebral artery; WPW: Wolff–Parkinson–White syndrome; Y: yes; Yr: year.
BTO was conducted in seven patients who underwent elective occlusion, including five with aneurysms and two with craniocervical tumors. Adjunct neurological assessment was used in three patients and EEG monitoring in two patients (Figure 2(D)). BTO demonstrated sufficient collateral circulation and ischemic tolerance in all patients. BTO was not feasible in four emergency cases.
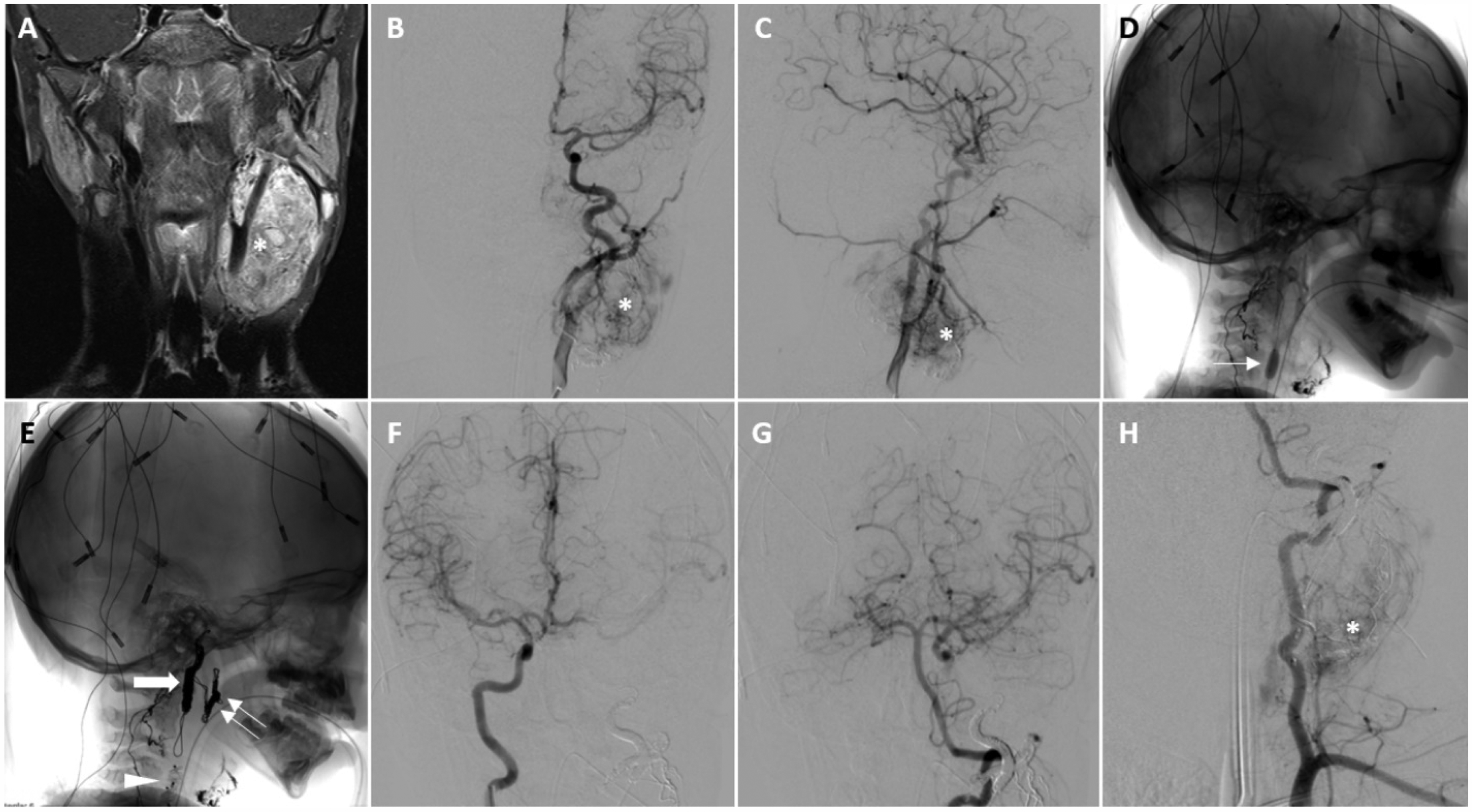
Case 17: A 4-year-old boy with a malignant glomus tumor presented as a left-sided neck mass. Post-contrast neck MRI (A) reveals an enhancing mass (asterisk) encasing the left CCA, ECA, and ICA. Left common carotid angiograms (B and C) show a hypervascular left cervical tumor (asterisk), visualized as tumoral blush staining. A lateral skull film (D) shows balloon occlusion of the left CCA (arrow) with EEG monitoring. Another lateral skull film (E) shows post coiling occlusion of the left ECA (double arrow) and ICA (bold arrow) with an Amplatzer devices (arrowhead) occluding the left CCA. Post treatment right internal carotid (F) and left vertebral (G) angiograms show good collateral flow to the left ICA territory, primarily via the left Pcom artery. A left subclavian angiogram (H) identifies residual tumoral staining at the inferior aspect of the mass, supplied by left cervical arteries.
Procedure details
Endovascular trapping was performed in 10 patients, while proximal occlusion was performed in eight patients, including six with large or giant aneurysms and two with arterial dissection. Standalone coils were used in 11 cases, coils plus Amplatzer vascular plug (Abbot) in three cases, coils plus a stent in one case, coils plus a microvascular plug (MVP, Medtronic) in one case, and standalone MVP in two cases.
Complete occlusion of the targeted arterial segment was confirmed on immediate control angiography in 16 cases (89.9%). Residual minimal antegrade flow was seen in the remaining two cases; a traumatic vertebral dissection managed with proximal coiling and a basilar AVF treated with an MVP (Figure 3).
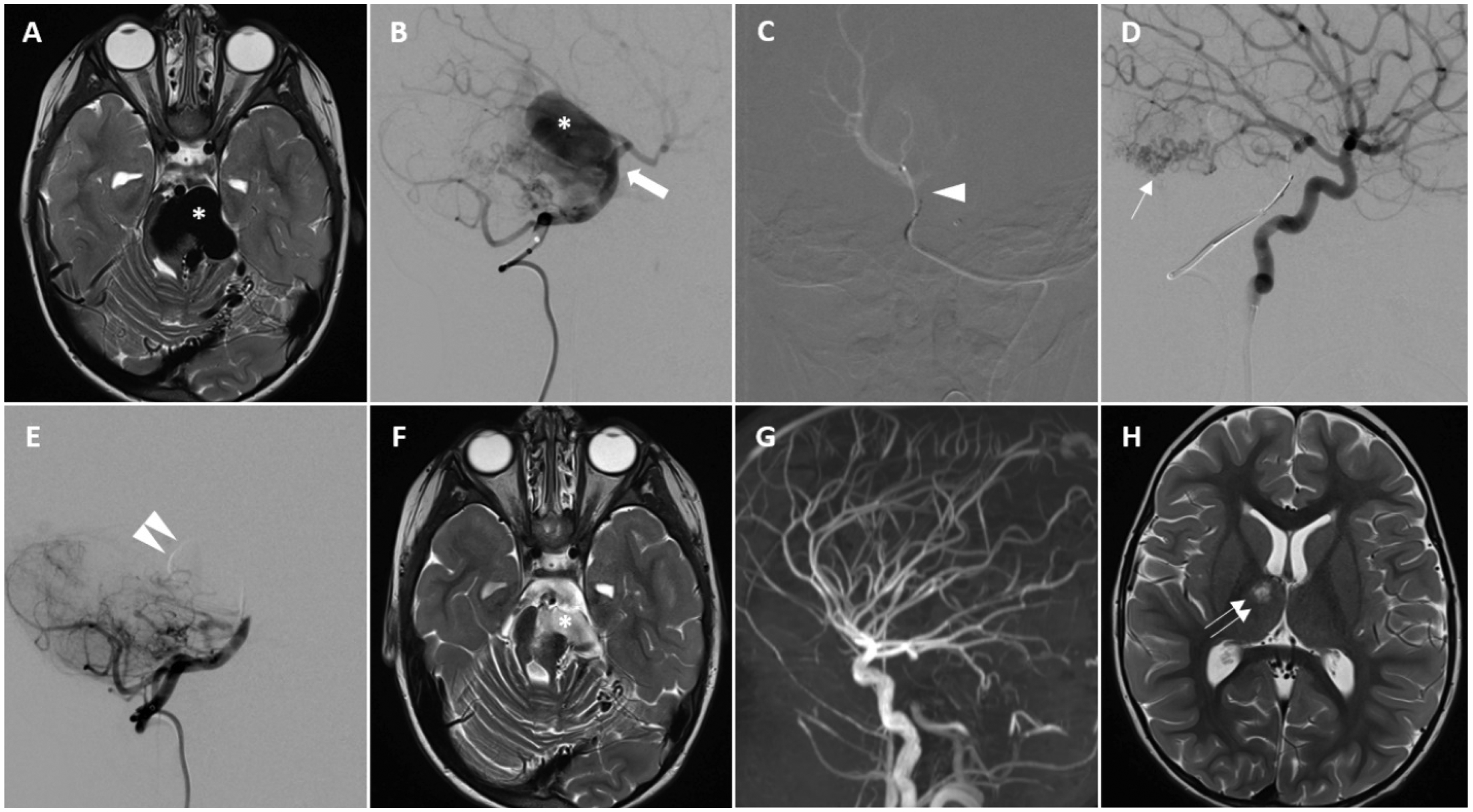
Case 13: A 3-year-old girl presented with ataxia. Brain MRI (A) shows a pontomesencephalic high-flow arteriovenous fistula with a dilated venous varix (asterisk), seen as an arterial-signal flow void compressing the pons. The left vertebral angiogram (B) reveals dilated venous varix (asterisk) from the basilar arterial fistula (bold arrow). A roadmap image from a right PCA angiogram (C) shows the deployment of the Micro Vascular Plug (MVP) (arrowhead) in the upper basilar artery. The left internal carotid angiogram (D) with the MVP deployed shows robust collateral supply to the left posterior cerebral artery and also detects another non-contiguous arteriovenous shunting via the left P2 segment (arrow). Left vertebral angiogram post-MVP detachment (E) shows minimal antegrade flow into the venous varix with contrast stagnation in its dependent part (double arrowhead). An immediate postoperative MRI (F) demonstrates decreased mass effect of the venous varix with lesional signals indicating early thrombosis. An immediate postoperative MRA (G) shows internal carotid artery supply to the posterior cerebral artery via the posterior communicating artery bilaterally. The basilar artery terminates at the level of the anterior inferior cerebellar arteries, and the varix is not seen. A 2-week follow up MRI (H) identifies new subacute infarction at right thalamus (double arrow). Genetic testing of the patient reveals a duplication in the endoglin gene, implicated in HHT.
Preprocedural dual antiplatelet therapy was required in the case of a large fusiform vertebral aneurysm scheduled for PAO with coils and protective stent placement in the BA and contralateral VA. The majority of cases (83.3%) were heparinized during the procedure except for three cases as the risk of hemorrhage was deemed too high. These included a case with a recent ruptured recurrent ICA aneurysm post-clipping, a case of ruptured spinal AVF, and a case of cervical trauma with vertebral artery dissection associated with a cervical spine fracture requiring spinal fixation immediately following PAO.
Postoperative heparin anticoagulation therapy was used in seven cases, including four large or giant aneurysms treated with proximal occlusion, a basilar AVF with a large venous varix treated by endovascular trapping, and two VA dissections—one treated by endovascular trapping and the other by proximal occlusion. Post-procedural single antiplatelet therapy was given in four cases: one traumatic VA dissection, one traumatic carotid-cavernous fistula, and two cases with underlying Moyamoya disease and arrhythmia. Dual antiplatelet therapy was continued postoperatively after deployment of a protective stent as mentioned earlier.
Periprocedural complications (<30 days post-intervention)
Complications were observed in six cases (33.3%), including five ischemic events. One case developed subarachnoid and intraventricular hemorrhage in the setting of low-molecular-weight heparin 13 days after treatment of a giant partially thrombosed VA aneurysm. The patient underwent emergent ventriculostomy, and angiography demonstrated decreased residual aneurysm filling without active extravasation. Among the five ischemic events observed, two were symptomatic. The first symptomatic case involved a patient treated with flow-reversal for a giant partially thrombosed basilar aneurysm. This patient developed a distal embolism in the left cerebellar hemisphere 11 days post-procedure (Figure 4(E)), which manifested as mild dysmetria. The second case developed mild facial drooping following endovascular trapping of a dissected cervical ICA due to infarctions in the MCA territory and watershed regions (Figure 1(G) and (H)).
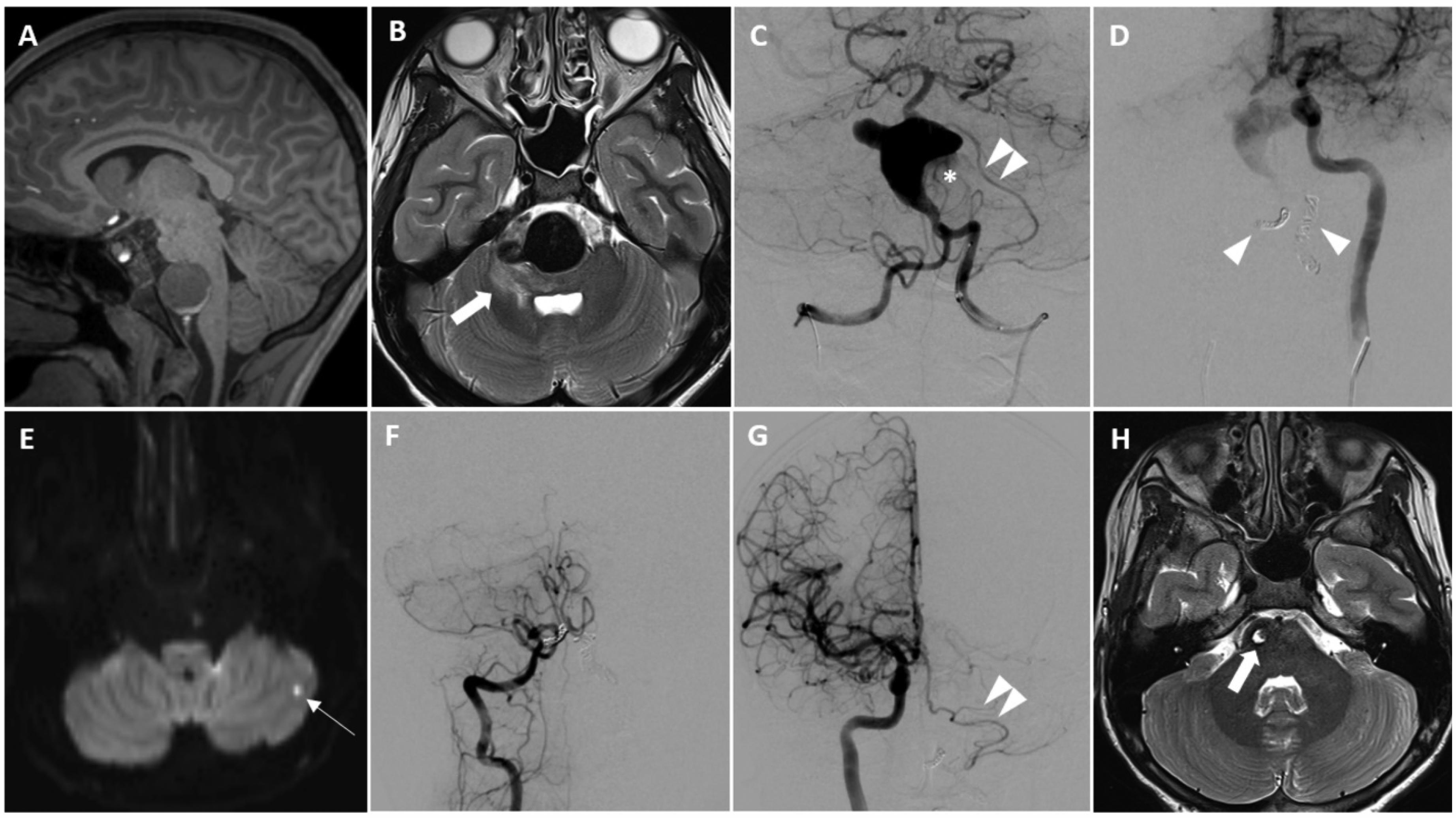
Case 8: An 11-year-old boy presented with headache. Brain MRI (A and B) shows a giant partially thrombosed fusiform aneurysm involving the mid and lower basilar artery with a daughter sac at the right superolateral aspect and associated perilesional edema (bold arrow). The left vertebral angiogram (C) reveals a thrombosed part as a filling defect on the left side of the aneurysm (asterisk) and shows the left AICA-PICA arising from the aneurysm (double arrowhead). The left internal carotid angiogram (D), following coiling occlusion of the bilateral vertebral arteries (arrowheads), demonstrates retrograde flow from the left posterior communicating artery to the upper basilar artery with faint filling of the aneurysm. Ten days post-operation, patient developed mild right-sided dysmetria. Diffusion-weighted imaging reveals a punctate infarction in the left lateral cerebellar hemisphere (arrow, E). A 1-year follow-up angiogram (F, G) shows no residual aneurysm with good collateral circulation to the lower basilar territory and preserved upper basilar artery down to the left AICA-PICA (double arrowhead). A 1-year follow-up MRI (H) shows the resolution of the aneurysm and edema with residual foci of gliotic change in the right-sided pons (bold arrow).
The remaining three ischemic cases were asymptomatic post-treatment infarctions detected on MRI at 1, 1, and 14 days post-procedure in a ruptured recurrent distal ICA aneurysm, a basilar AVF, and a giant partially thrombosed ICA-MCA aneurysm, respectively. Notably, the giant partially thrombosed basilar aneurysm and the basilar AVF developed ischemic events despite negative immediate post-treatment brain MRI.
Follow-up clinical and imaging outcomes
Symptom resolution (73.3%) or improvement (26.7%) was observed in all symptomatic patients. No new strokes, transient ischemic attacks, or mortality was observed over a mean follow-up duration of 6.9 ± 4.5 years (range, 0.3–15.6 years). All cases of symptomatic ischemic or hemorrhagic complications returned to baseline without residual neurological deficits at the last follow-up. All patients who underwent PAO had favorable outcomes at the last follow-up.
The mean follow-up neurovascular imaging period was 4 ± 3.5 years (range, 0.04–12 years). Follow-up cerebral angiography was available in 11 patients. Seven cases had residual or recurrent disease on early follow-up imaging (within 3 months); two underwent further embolization, three exhibited complete progressive thrombosis, and two had tiny residual lesions, which were managed conservatively. Among the two cases requiring additional embolization, one involved a giant partially thrombosed vertebral aneurysm that underwent proximal coiling occlusion, which developed mild displacement of coil mesh three days post-operation, resulting in recanalization of the occluded arterial segment. It was managed with additional Onyx embolization. The other case involved vertebral dissection presenting with recurrent occlusion of basilar artery, which underwent proximal occlusion with an MVP. Follow-up angiography at 3 months showed residual dissected arterial segment via the spinomuscular collaterals, which was managed by trapping occlusion of the dissected segment with coil embolization. Both cases demonstrated complete occlusion of the target arterial segment on immediate postoperative angiography.
For the progressive thrombosis group, the first case involved a giant partially thrombosed basilar aneurysm that underwent proximal coiling occlusion, exhibiting complete thrombosis of the aneurysm on one-year follow-up angiography. The other two cases were the previously mentioned ones with residual minimal flow on immediate post-procedural angiography: a basilar AVF, which exhibited complete obliteration of the AVF with thrombosis of the venous varix on one-year follow-up angiography, and a traumatic vertebral dissecting occlusion, which showed complete occlusion of the target arterial segment on one-month follow-up brain magnetic resonance angiography (MRA).
For the residual disease group, there were two cases with residual diseases due to the formation of collateral supply from adjacent vessels. One involved a cervical spinal perimedullary AVF post-coiling occlusion of left lateral spinal arterial feeder and left vertebral artery, showing a tiny residual arteriovenous shunt (AVS) supplied by the anterior spinal artery. The other case involved a juvenile nasopharyngeal angiofibroma post-coiling occlusion of the ICA and tumoral removal, exhibiting small residual tumor.
No evidence of recanalization was found on the most recent follow-up imaging in all cases. Follow-up intracranial vascular imaging was available in 17 cases, demonstrating no new infarctions or de novo intracranial aneurysms over the radiographic follow-up period.
Discussion
This study represents the first investigation into endovascular therapeutic occlusion procedures in pediatric patients. The findings demonstrate that endovascular occlusion is an effective treatment option for various vascular anomalies in children, including arterial aneurysms, dissections, arteriovenous shunting, and conditions requiring presurgical PAO.
BTO is a useful diagnostic tool that aids in decision-making and safer PAO outcomes in patients who demonstrate ischemic tolerance.24,25 A recent meta-analysis by Butterfield et al. reported symptomatic ischemic events in 3.7% of cases following successful BTO, with no conclusive evidence of differences between methods of perfusion assessment. 25 Nevertheless, ischemic infarction may still occur after an uneventful BTO, with incidence rates reported between 4.7 and 25%.1,19 In our cohort, one out of seven cases (14.3%) developed symptomatic cerebral infarction despite a successful BTO. Moreover, BTO was not performed in seven elective cases, including five patients with co-dominant VAs who underwent VA occlusion without ischemic complications. This is consistent with studies suggesting that VA occlusion can be safely performed without antecedent BTO, especially in cases with co-dominant VA anatomy.27,28
In the remaining two elective cases (non-co-dominant VA), BTO was not performed due to specific clinical or anatomical considerations. One patient had a high-flow vascular malformation causing rapidly progressive brainstem compression, necessitating immediate PAO to relieve the mass effect. In the other case, a traumatic carotid-cavernous fistula with a large cavernous ICA defect precluded vessel preservation. Given the robust collateral circulation demonstrated on angiography, therapeutic ICA occlusion was performed without BTO.
In our study, endovascular occlusion using either proximal occlusion or trapping was carefully guided by the anatomical characteristics and underlying pathology, underscoring the importance of a flexible and individualized approach in pediatric neurointerventions.7,8 Coils were used as the primary occlusive devices in 11 cases, while stents, Amplatzers, and microvascular plugs were used in the remaining cases, either in combination with coils or as standalone occlusive tools. This reflects the evolution of endovascular devices and techniques over the study period. Several reports have documented the successful use of Amplatzers16,29–31 and microvascular plugs13,18,32 as occlusive tools for pediatric neurointerventions. Our 89.9% rate of immediate occlusion is similar to the 90.5% reported by Nishi et al. in adult patients who underwent PAO for unruptured aneurysms. 33
Periprocedural complications were observed in 33.3% of cases, with ischemic events being the most common. Ischemic complications occurred in 27.8% of cases, and hemorrhagic complications in 5.6%. These findings are consistent with the study by Koizumi et al., which reported a rate of early ischemic stroke and target aneurysm rerupture in adult patients who underwent endovascular PAO of 27.9% and 1%, respectively. 20 Additionally, Nishi et al. reported periprocedural ischemic and hemorrhagic complication rates of 17.5% and 2.5%, respectively. 33
Among the five ischemic cases, two involved giant partially thrombosed aneurysms. The first patient, with a right distal ICA-MCA aneurysm treated by proximal coiling, developed an asymptomatic right MCA infarction on postoperative day 1. The second case involved a basilar aneurysm with the left AICA-PICA arising from it, treated by bilateral vertebral artery occlusion; this patient developed a symptomatic left PICA infarction on day 11, despite a negative immediate post-procedure MRI.
A third case, involving a ruptured recurrent right distal ICA aneurysm treated with distal ICA trapping, resulted in an asymptomatic infarction in the anterior choroidal artery territory. The fourth case, a basilar arteriovenous fistula treated with trapping using an MVP, led to a delayed asymptomatic right thalamic infarction, despite a negative immediate post-procedure MRI.
The final case involved a left ICA dissection in a patient with pre-existing hypotension and subtle hypodensity in the left MCA territory observed preoperatively. Immediate postoperative MRI revealed more extensive infarcts in both the MCA and watershed regions. It remains difficult to ascertain whether these infarctions were entirely pre-existing or a combination of pre-existing and postoperative events.
Given the complexity of the vascular anatomy and the timing of infarctions in these cases, both hemodynamic compromise secondary to PAO and procedural-related thromboembolic mechanisms—including potential device-related factors such as MVP-associated thrombus formation 34 —may have contributed to these outcomes.
The single case of hemorrhagic complication in our cohort involved a giant partially thrombosed vertebral aneurysm treated with proximal occlusion with post-procedural anticoagulation. Trapping was not feasible due to severe tortuosity and narrowing of both vertebral arteries, which precluded distal V4 segment access. The postoperative angiography demonstrated slowed retrograde filling of the aneurysm from the contralateral vertebral artery with contrast stasis. Thirteen days post-treatment, the patient developed a subarachnoid hemorrhage with intraventricular hemorrhage and hydrocephalus. This complication is consistent with a previous report by Piepgras et al., who suggested that occult aneurysm disruption could result from the combination of aneurysm sac expansion and alteration in local hemodynamic stress during extensive thrombosis. 35
The early postoperative period is crucial for monitoring complications, as evidenced by the ischemic and hemorrhagic events observed. However, our mid- to long-term follow-up results are encouraging, showing good clinical outcomes, no new strokes, transient ischemic attacks, or mortality over the follow-up period, suggesting a durable benefit of endovascular occlusion. Similar long-term efficacy has been reported in adult patients undergoing PAO.19,20 All patients in our study had favorable outcomes at the last follow-up, indicating that pediatric patients tolerate the PAO procedure well. This observation aligns with previous review suggesting that pediatric patients tend to tolerate PAO more effectively than adults, 9 likely due to their more adaptable and plastic vascular systems, which may facilitate the development of robust collateral circulation post-occlusion.
In our study, no new aneurysms were observed during a mean follow-up period of 4 years. In contrast, Hetts et al. reported a high incidence (8.4%) of new or enlarging untreated aneurysms in pediatric patients after initial aneurysm treatment or observation, with a mean follow-up of 5.9 years. The risk of developing new or enlarging aneurysms is higher in cases involving multiple aneurysms at presentation, fusiform aneurysms, and treatment with PAO. Notably, five out of nineteen aneurysm cases that underwent PAO in their study developed new aneurysms. Furthermore, their findings suggested that pediatric patients are likely to develop new and enlarging aneurysms at a faster rate compared to adults. 22
The incidence of de novo aneurysm formation following carotid occlusion is reported to vary widely, ranging from 0% to 20%, with a mean incidence of approximately 4% to 11%. The time to de novo aneurysm formation after therapeutic carotid occlusion has been documented to range from 4 to 25 years, with a mean of 9.6 years.21,23 The mean follow-up time of 4 years in our study may be insufficient to detect de novo aneurysm formation. This underscores the importance of diligent long-term follow-up, as the formation of new aneurysms could present significant challenges in the future. The varying follow-up durations in our cohort highlight the need for standardized recommendations for imaging follow-up in this patient group.
Limitations
This study was limited by its small sample size, which is attributable to the rarity of complex pediatric neurovascular pathologies requiring PAO. Additionally, the retrospective nature of our investigation introduces inherent biases that may affect the interpretation of the results. The follow-up duration varied significantly among patients, which limits the ability to assess the long-term outcomes comprehensively. Moreover, the heterogeneity of the patient population and the variety of pathologies treated introduce variability in the outcomes. Future studies with larger cohorts and standardized protocols are essential to validate these findings and further refine the treatment strategies for pediatric cerebrovascular anomalies.
Conclusions
Endovascular therapeutic occlusion is a relatively safe and effective treatment modality for a variety of cerebrovascular pathologies in pediatric patients. The high technical success rate, coupled with favorable long-term outcomes, supports the continued use of these interventions in carefully selected cases. However, the potential for long-term complications highlights the importance of careful patient selection and long-term follow-up.
Footnotes
Author note
Kittiphop Somboonnithiphol is currently affiliated with the Department of Diagnostic and Therapeutic Radiology, Ramathibodi Hospital, Bangkok, Thailand. Soliman Oushy is currently affiliated with the Department of Neurosurgery, University of Miami School of Medicine, Miami, Florida, USA.
Acknowledgments
We would like to sincerely acknowledge Julie Meadows, Clinical Research Specialist, for her invaluable support and contributions to this study.
Author contributions
Conception and design: Kittiphop Somboonnithiphol; acquisition of data: Kittiphop Somboonnithiphol; analysis and interpretation of data: all authors; drafting of the article: Kittiphop Somboonnithiphol and Soliman Oushy; critical revision of the article: Kittiphop Somboonnithiphol and Darren B. Orbach; review of the submitted version of the manuscript: Kittiphop Somboonnithiphol; statistical analysis: Kittiphop Somboonnithiphol; study supervision: Kittiphop Somboonnithipholand Darren B. Orbach.
Data availability
Upon reasonable request, anonymized data will be available, subject to IRB oversight.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study received ethical approval from the Boston Children's Hospital Institutional Review Board (IRB-P00047447) on 24 July 2024. This is an IRB-approved retrospective study; all patient information was de-identified and patient consent was not required. Patient data will not be shared with third parties.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.