
Abstract
Background
Balloon guide catheters (BGCs) can optimize recanalization in endovascular thrombectomies, but recent studies suggest that aspiration catheters sized closely to the target vessel can be effective for recanalization.
Objective
To compare the outcomes, efficacy, and safety of a single-surgeon experience replacing BGCs with large distal platform (LDP) catheters.
Methods
This is a retrospective study of patients with anterior circulation large vessel occlusion undergoing endovascular thrombectomies. Our study population was divided based on use of either the Zoom™ 0.088” LDP (Imperative Care, Inc., Campbell, CA, USA) or Walrus™ BGC (Q’Apel Medical, Fremont, CA, USA). Primary outcomes were the thrombectomy technique used, time from groin puncture to recanalization, first pass effect (FPE), degree of final reperfusion (modified treatment in cerebral infarction [mTICI]), postoperative complications, and all-cause mortality at 90 days.
Results
We analyzed 48 cases: 27 with Walrus™ BGC and 21 with LDP. Contact aspiration was primarily used with LDP (p < 0.001), while a stent-retriever-based technique was preferred with BGC (p < 0.001). The median groin-to-recanalization time was shorter for the LDP cohort (p = 0.001). Both cohorts achieved mTICI ≥ 2b in all cases, with more mTICI of 3 in the LDP cohort (p = 0.38). The LDP cohort also had a greater FPE (p = 0.034). Four cases with iatrogenic dissections were observed with Walrus™ BGC (p = 0.12) and 2 cases with downstream emboli with using the LDP (p = 0.19). All-cause mortality was similar between cohorts (p > 0.99).
Conclusion
The super-bore LDP offers a significant advantage over BGCs, achieving faster reperfusion times without compromising safety or recanalization effectiveness. Switching to super-bore 0.088” Zoom may enhance thrombectomy procedures.
Introduction
In the United States, stroke remains the fifth most common cause of death and functional disabilities. 1 Among patients with acute ischemic stroke (AIS), approximately one-third have an underlying large vessel occlusion (LVO). 2 The advent of endovascular thrombectomy (EVT) has revolutionized care compared to medical management alone. 3 For eligible patients, EVT offers significant advantages in reducing time to (vessel) reperfusion and improving outcomes such as independent ambulation. 4
The clear benefits of EVT have driven efforts to identify the most suitable neurointerventional tools for maximizing procedural and clinical outcomes. Balloon guide catheters (BGCs) are preferred for achieving proximal flow arrest and reducing clot fragmentation, thus minimizing distal emboli and downstream complications.5,6 Recent advancements include large distal platform (LDP) catheters, which are capable of navigation beyond the cervical internal carotid artery (ICA), potentially bypassing the need for flow arrest.7,8 These LDP guide catheters do not require the same preparation as BGCs and may be faster to utilize during mechanical thrombectomy. Despite these advancements, BGCs continue to be widely used. 9
EVT usage is projected to increase by 5% to 10% annually. 10 As more patients become eligible for mechanical thrombectomy, increased demands may cause delays in access to care. Improving access can be achieved by targeting workflow efficiency, particularly by selecting either BGCs or LDP guide catheters to optimize EVTs.
This study compares a single-surgeon experience of switching from BGCs to super-bore guide catheters for mechanical thrombectomy in anterior circulation LVO AIS, seeking to assess direct impact on user experience, safety, and tool efficacy.
Methods
Ethics approval
The analysis of a prospectively maintained database was approved by the University of Maryland, Baltimore Institutional Review Board (Approval HP-00104512). This is an IRB-approved retrospective study, and all patient information was de-identified and patient consent was not required.
Study design
This study is a retrospective review conducted at a single center. All consecutive patients with ischemic stroke due to LVO treated with EVT between June 2021 and September 2023 were screened for inclusion.
We collected patient demographics, including the location of the occluded vessel and the time last known well (LKW). Stroke metrics obtained on admission were the National Institutes of Health Stroke Scale (NIHSS) and the modified Rankin scale (mRS). Procedural data included the primary thrombectomy technique (either contact aspiration or stent retriever clot retrieval), number of passes, time from groin puncture to reperfusion, postoperative complications, and mortality.
Cases were included if LKW was less than 24 hours, the occlusion was located at the ICA or the M1/M2 segments of the middle cerebral artery. Cases had employed either the Walrus™ BGC (Q’Apel Medical, Fremont, CA, USA) or Zoom™ 0.088” LDP (Imperative Care, Inc., Campbell, CA, USA) as the primary guide catheter. During the study period, LDP was introduced at our institution in April 2023. Only consecutive LDP cases beyond that time point were included in the cohort, while the patients prior to that timepoint were limited to the Walrus™ BGC cohort.
Procedures
All procedures were performed by a single fellowship-trained neurosurgeon who has had routine experience using the BGC prior to switching to LDP. Femoral access was obtained utilizing standard micro-puncture technique. Eight French access was used in all cases, and the target vessel was catheterized with various diagnostic catheters chosen based on patient-specific anatomy.
BGC cohort
A Walrus™ BGC was advanced into the distal cervical ICA over the diagnostic catheter, which was then removed. A 6 French 070 Sofia (Microvention/Terumo, Tustin, CA, USA) distal access catheter was navigated to the occlusion site. An 0.025” Velocity® (Penumbra, Inc., USA, Alameda, CA, USA) microcatheter, when used, was guided over a microwire past the thromboembolism. The BGC catheter was then advanced into the proximal petrous ICA and inflated for flow arrest. Aspiration was performed via the distal access catheter for several minutes, then retracted under flow arrest. If a stent retriever was used, it was deployed in the target vessel through the microcatheter. After allowing for clot integration, the device was removed with aspiration via the distal access catheter combined with BGC flow arrest.
LDP cohort
A 110-cm Zoom™ 0.088” catheter was typically delivered to the distal cervical ICA. After removing the diagnostic catheter, an aspiration catheter (0.070” Sofia™, Zoom™ 0.071”, or Zoom™ 0.045”) was advanced into the cavernous ICA. The Zoom™ 0.088” guide catheter was then brought higher over the aspiration catheter into the petro-cavernous ICA. The aspiration catheter was then navigated to the proximal occlusion site, and aspiration was applied. If a stent retriever was used, an 0.025” Velocity® microcatheter was guided over a microwire through the aspiration catheter and advanced past the thromboembolism. The stent retriever was deployed, and after clot integration, the device was removed with aspiration via the aspiration catheter.
General anesthesia was used in all procedures. Post-thrombectomy angiography confirmed successful recanalization for both techniques. An arteriotomy closure device was used to achieve hemostasis.
Outcome measures
Primary outcomes assessed included the primary thrombectomy technique used, time from groin puncture to recanalization, degree of successful final reperfusion (defined as modified treatment in cerebral infarction [mTICI] score ≥ 2b), first pass effect (FPE), number of passes, postoperative complications (particularly downstream emboli and iatrogenic dissection), and all-cause mortality at 90 days. FPE was defined as achieving an mTICI score ≥ 2b at the first device pass.
Statistical analysis
Baseline characteristics were presented using descriptive statistics. The Mann–Whitney U test was used to compare the median time to recanalization. t-Test assessed the relationship between the average number of passes. Fisher's exact test was used to compare proportions of patients treated with the Walrus™ BGC or Zoom™ 0.088” guide catheters for all other outcome measures, including the total individual number of passes. The level of significance was set at p < 0.05. All statistical analyses were performed using Python (version 3.12.0, Python Software Foundation, Delaware, USA).
Results
Baseline characteristics
During the study period, 48 patients with AIS secondary to embolism were treated by a single surgeon at our center. Of the 48 patients, 27 (56.2%) underwent thrombectomy with the Walrus™ BGC and 21 (43.8%) with the Zoom™ 0.088” LDP (Table 1). Both cohorts had a comparable distribution of sexes, with slightly more males in the Zoom cohort (57.1% vs. 55.6%) (Table 1).
Baseline patient characteristics.
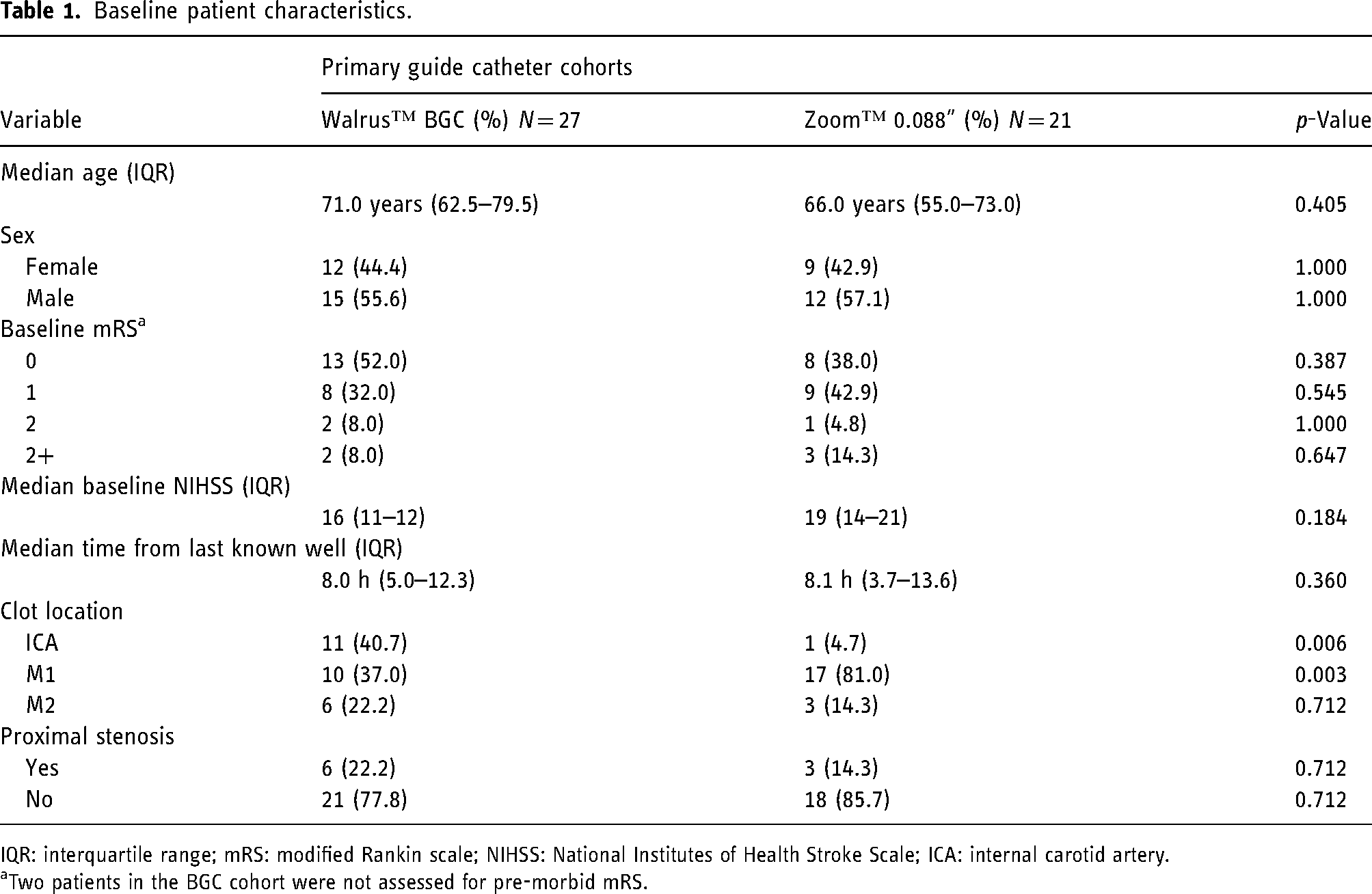
IQR: interquartile range; mRS: modified Rankin scale; NIHSS: National Institutes of Health Stroke Scale; ICA: internal carotid artery.
Two patients in the BGC cohort were not assessed for pre-morbid mRS.
No significant differences were observed in age between the LDP and BGC cohorts (median age and IQR of 66.0 [62.5–79.5] vs. 71.0 [62.5–79.5]), baseline mRS, median baseline NIHSS (19 [11–12] vs. 16 [14–21]), and stenosis proximal to the target vessel (14.3% vs. 22.2%) (Table 1).
Compared to the BGC cohort, the LDP cohort had more M1 occlusions (81.0% vs. 37.0%, p = 0.003) and had higher proportions of first pass recanalization (80.9% vs. 48.1%, p = 0.03) (Table 1). However, the BGC cohort had more occlusions in the ICA (40.7% vs. 4.7%, p = 0.006) (Table 1).
Outcomes
The primary technique used in the LDP cohort was contact aspiration or ingestion (90.5% [19/21] vs. 40.7% [11/27], p < 0.001) compared to the BGC cohort. Use of stent-retrievers were more common with the Walrus™ BGC (59.3% [16/27] vs. 9.5% [2/21], p < 0.001) (Figure 1). The LDP cohort had the same number of cases requiring switch to another technique (e.g., failed aspiration followed by contact aspiration or vice versa) (9.5% [2/21] vs. 7.4% [2/27], p > 0.99).
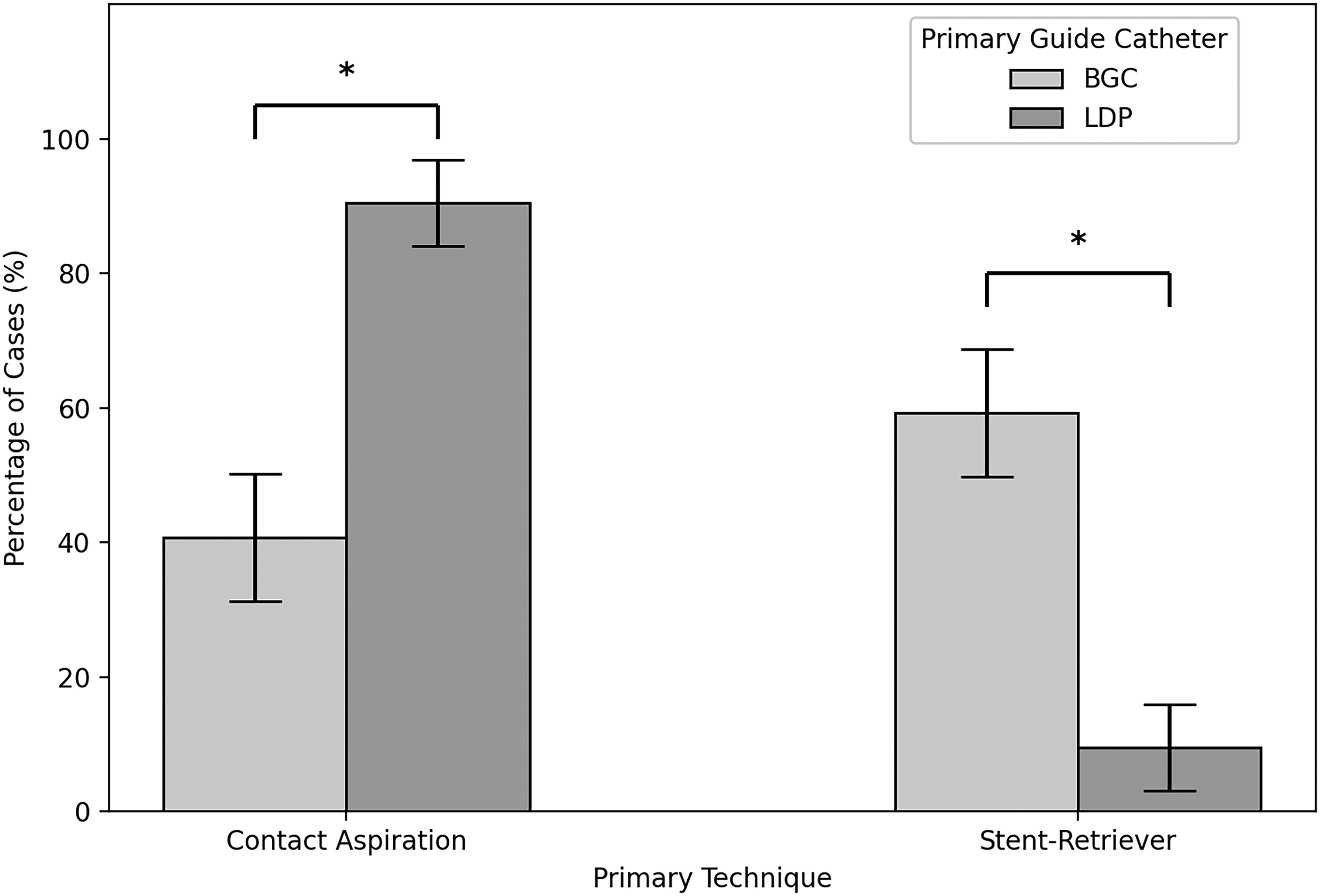
Primary technique for thrombectomy significantly associated with catheter type. Contact aspiration or ingestion was the primary technique in large distal platform (LDP) cohort, whereas stent-retrieval was the primary technique in the balloon guide catheter (BGC).
The LDP cohort had a significantly shorter median time from groin puncture to recanalization (22 minutes vs. 40 minutes, p < 0.001). LDP cases ranged between 19 and 28 minutes, while Walrus™ BGC cases ranged between 32 and 53 minutes (Figure 2).
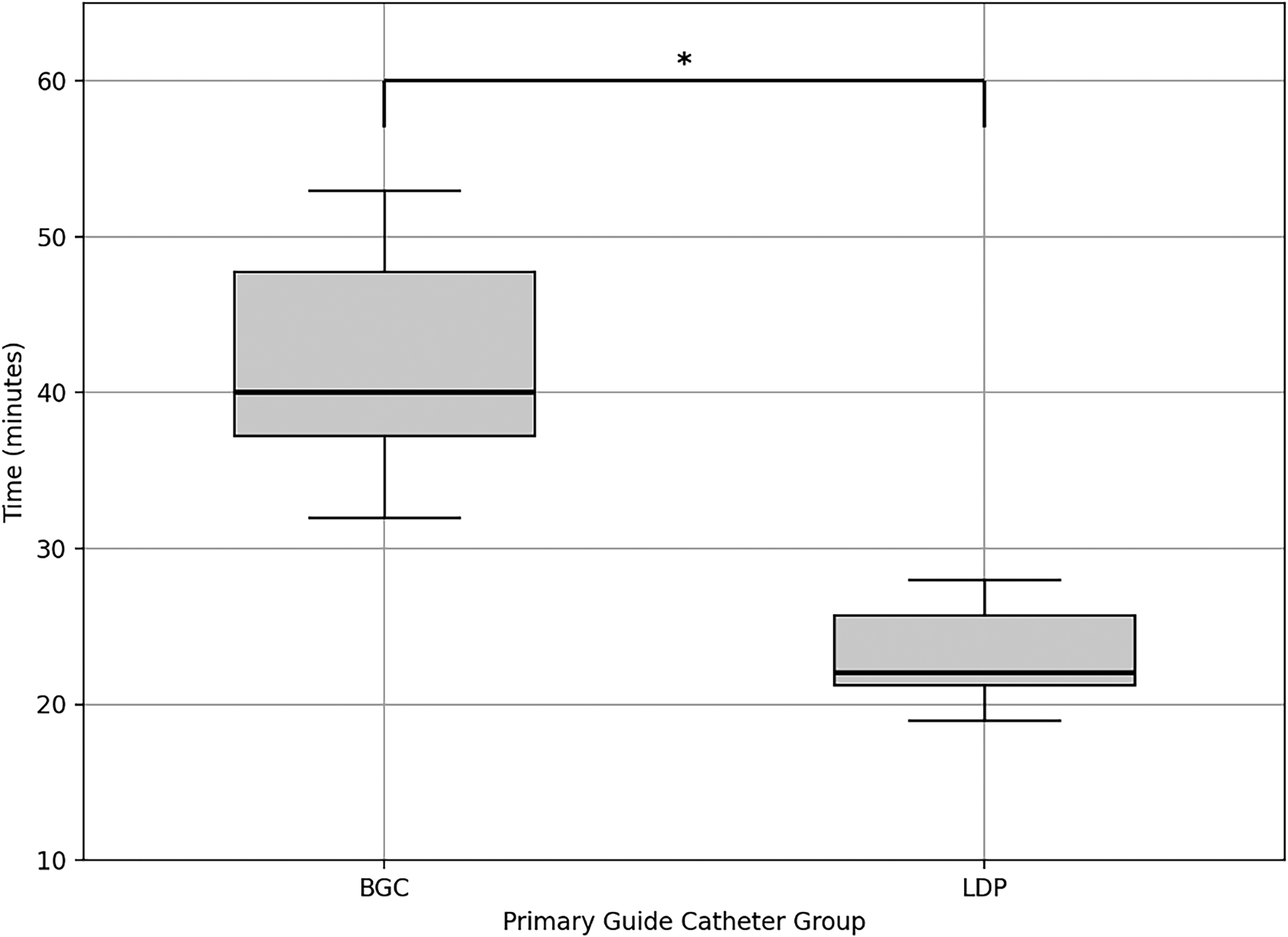
Rapid groin-to-recanalization time achieved by large distal platform (LDP) compared to balloon guide catheter (BGC). LDP achieved a significantly reduced groin-to-recanalization time at a median of 22 minutes compared to a median of 40 minutes achieved by BGC.
All cases achieved greater than or equal to mTICI 2b. Minimal differences were observed in achieving mTICI ≥ 2c between LDP and Walrus™ BGC (76.1% [16/21 ] vs. 81.5% [22/27], p = 0.73). There was a non-significant trend favoring better reperfusion with mTICI 3 using LDP (47.6% [10/21] vs. 33.3% [9/27], p = 0.38) (Figure S1) with Figure 3 demonstrating a successful case.
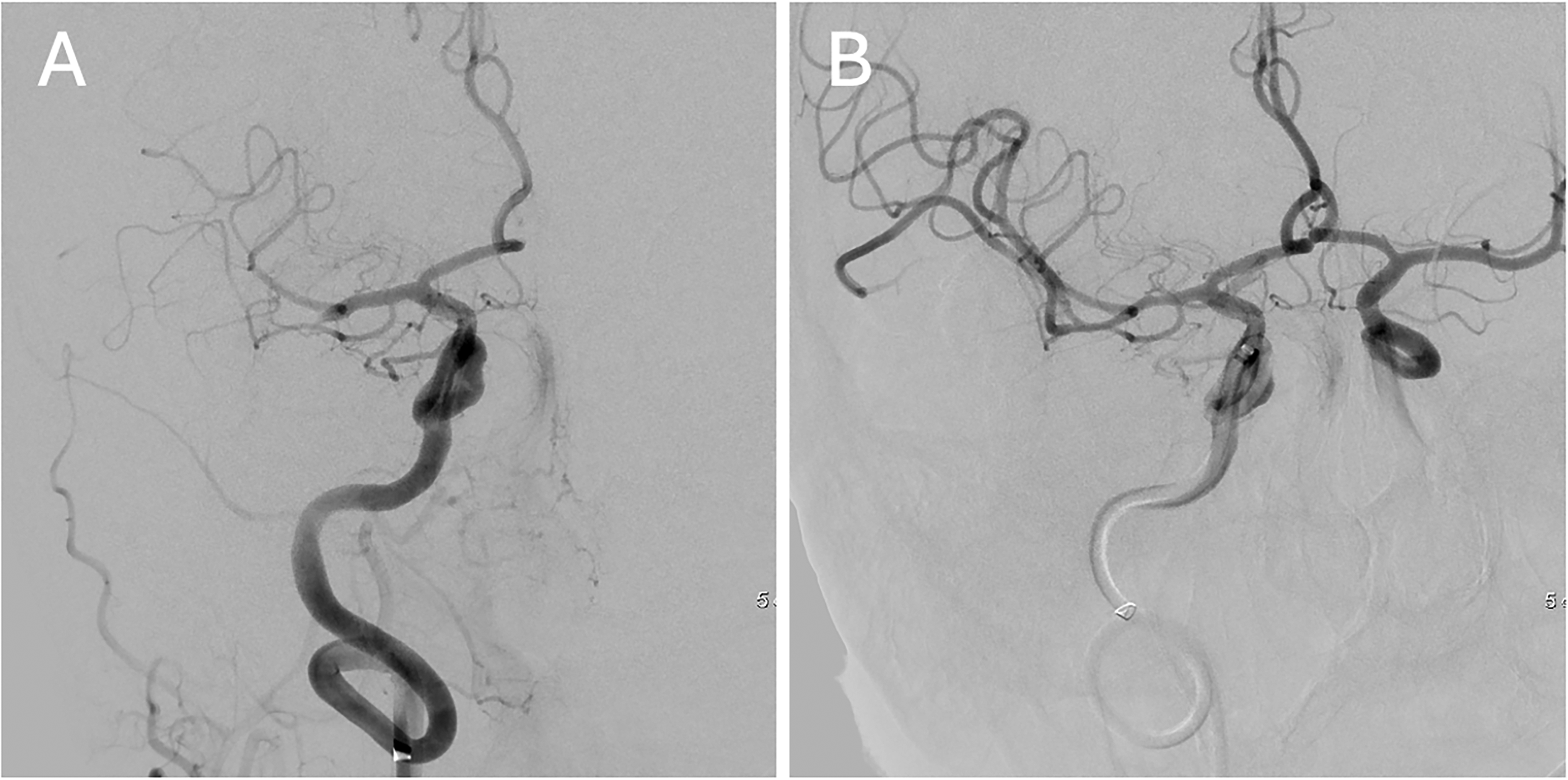
TICI 3 reperfusion with large distal platform. Complete occlusion of the proximal dominant M2 division of the right MCA (A) with complete reperfusion and LDP visualized at the cavernous segment of ICA (B).
LDP achieved significantly higher complete recanalization from a single pass (80.9% [17/21] vs. 48.1% [13/27], p = 0.034) (Figure 4(a)). It also had a marginally lower average number of passes (1.33 vs. 2.0, p = 0.035). There were few cases where LDP required multiple passes, though these were not all statistically significant: 2 passes (4.8% [1/21] vs. 29.7% [8/27], p = 0.06), 3 passes (14.3% [3/21] vs. 11.1% (3/27], p > 0.99), and 4 or more passes (0% [0/21] vs 11.1% [3/21], p = 0.2)) (Figure 4(b)).
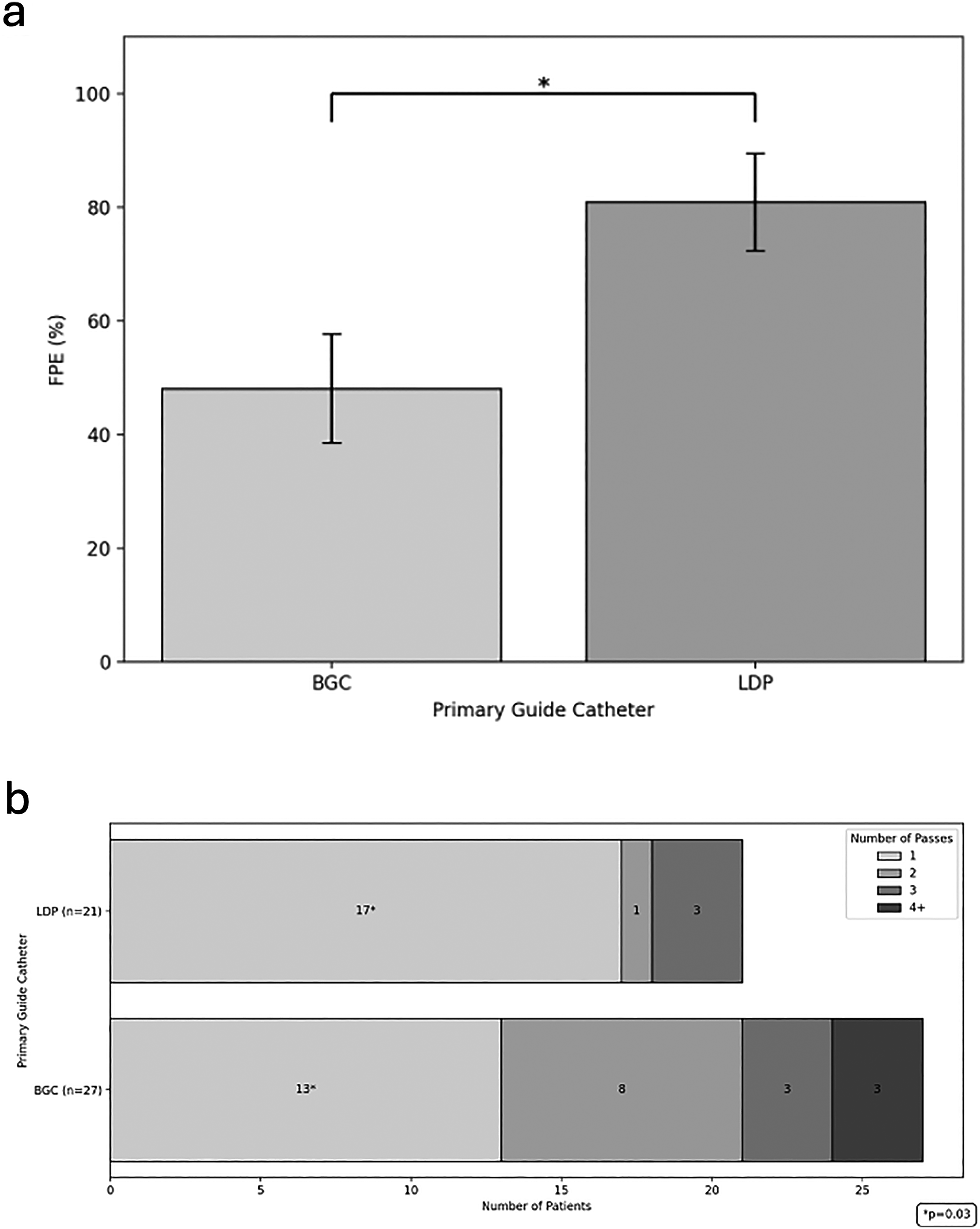
Passes by large distal platform (LDP) and balloon guide catheter (BGC). LDP demonstrates superior first pass effect (FPE) with significantly more cases achieving complete recanalization with one pass (a). Multiple passes were seen in both catheter groups, but a non-significant trend favored fewer passes with LDP (b).
There were two postoperative complications analyzed. While non-significant, LDP did not have any iatrogenic dissections compared to the BGC cohort (0% [0/21] vs. 14.8% [4/27], p = 0.12). Figure 5 demonstrates one case. However, downstream emboli were observed in the LDP cohort (9.5% [2/21] vs. 0% [0/27], p = 0.19). All dissections were non-flow-limiting, and none required further endovascular treatment. All-cause mortality was similar between cohorts, with the BGC cohort demonstrating slightly lower rates (7.4 [2/27] vs. 9.5 [2 /21], p = 1.0) (Figure S2).
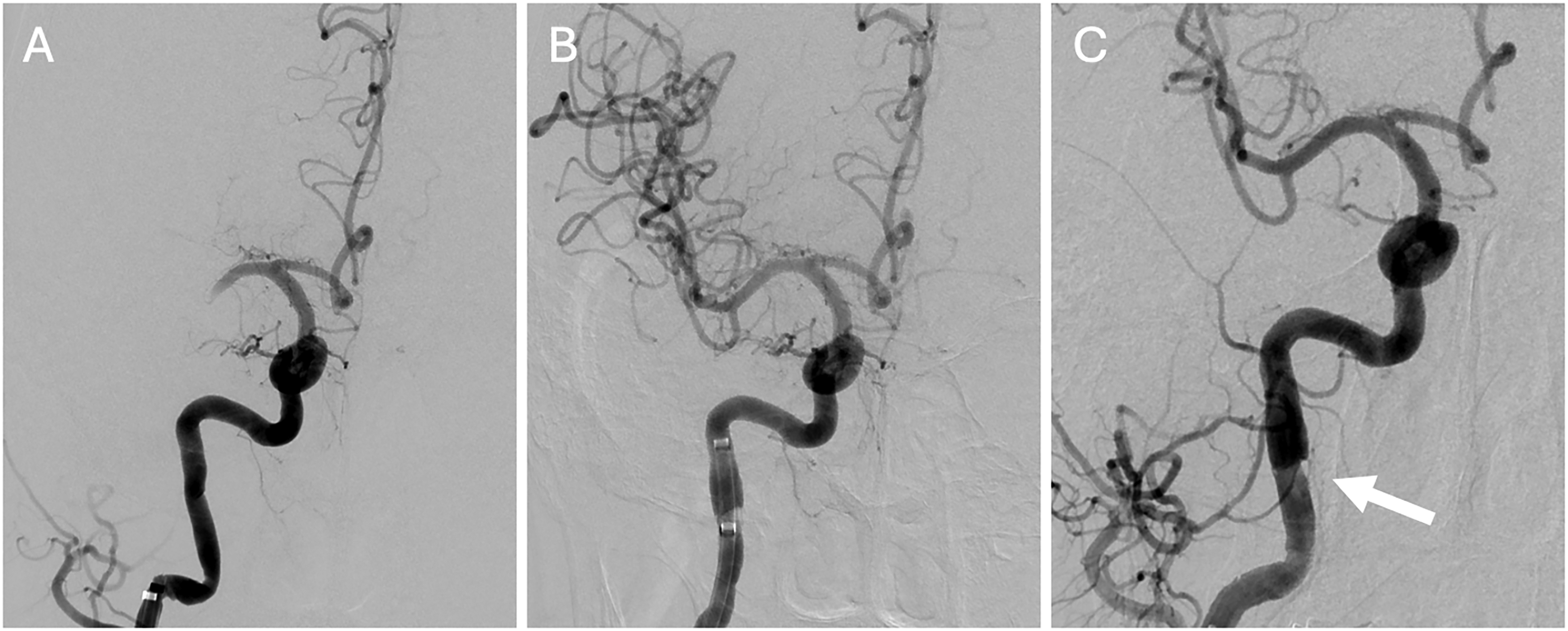
Dissection with use of balloon guide catheter. Digital subtraction angiography (DSA) demonstrating complete occlusion at M1 segment of right MCA (A) with subsequent TICI 2 recanalization following aspiration (B) and dissection at the proximal petrous segment of the ICA after BGC removal (C).
Discussion
This study demonstrates that using super-bore 0.088” LDP in EVT for anterior circulation LVO significantly enhances rapid procedure completion and successful recanalization on the first pass. Compared to BGCs, there is a non-significant trend favoring LDP catheters for achieving higher mTICI scores. Overall, LDPs are safe tools that can enhance thrombectomies.
Technique
Our analysis showed a preference for aspiration technique with LDP, while stent retrievers were more often used with BGCs. Regardless of technique employed for management at the clot interface, BGCs are utilized primarily to prevent clot fragmentation with flow arrest and reversal. However prior series supporting the use of BGCs have been based on stent-retriever thrombectomy technique. 11 In our study, the transition to LDPs was combined with a preference for contact aspiration-based thrombectomy technique, allowing for direct clot ingestion at the point of aspiration catheter application. 12 With the clot successfully pulled down into the guide catheter, the role of flow arrest or reversal achieved by a stent retriever may not have been as applicable.
Groin-to-recanalization time
The Zoom™ 0.088” LDP was associated with significantly reduced groin-to-recanalization time in this study, similar to previous studies.13,14 Shorter durations with LDP may result from choosing aspiration over stent retrieval, which often involves waiting 3 to 5 minutes for clot integration. 15 LDPs with more hydrophilic coating on the distal tip can further optimize procedure time. 16 In contrast, managing balloon inflation with BGCs may further prolong procedures. 17 The significant difference in median groin-to-recanalization times can thus be partially explained by technical requirements for BGCs.
Recanalization
While many studies support BGCs for higher mTICI scores, our study provides insights into the comparable use of LDPs. Studies like ASTER show no significant trend favoring either technique for mTICI scoring. 18 In our study, LDP was associated with more mTICI 3 recanalizations, which have better clinical outcomes. 19 This may be due to their design for complete clot ingestion with fewer distal emboli.20,21 Our study did not evaluate secondary outcomes for mTICI scoring, so a small but potentially significant difference cannot be discounted.
The useful design of the LDP can be leveraged for greater frequency of FPE. Contrary to our results, one multicenter study suggests that BGC use is a predictor of FPE. 22 This discrepancy may be due to the LDP's strong suction force, while BGC success may depend on factors such as vessel tortuosity.23,24 Our study notably has a greater number of cases with ICA occlusions in the BGC cohort. While these occlusions have been associated with worse outcomes 25 and may impact FPE in our BGC cohort, the BGC catheter with the stent retriever technique has also been shown to still achieve frequent FPE with these ICA occlusions. 26 Therefore occlusion location alone cannot explain limitations to BGC performance in our study since the catheter was most often used with the stent-retriever technique and thus optimized for successful FPE. Ultimately, the benefit of FPE with LDPs is evidenced by shorter median groin-to-recanalization times. Patients achieving recanalization on the first pass have better clinical results, but these benefits may diminish in procedures over 30 minutes.22,27 This study supports the efficacious use of LDPs based on enhanced outcomes.
Complications and mortality
While clinically insignificant in this series, more iatrogenic dissections were observed in the BGC cohort. 28 Other studies suggest catheter type is not associated with iatrogenic dissection risk. 29 However dissections with BGC may result from difficulty with navigation and manipulation of the catheter into tortuous vessels, leading to an intimal tear. 29 Most iatrogenic dissections can be managed medically, though immediate stenting may be required. 30 Further, transitioning to LDP was not significantly associated with increased clot fragmentation. This might be driven by multiple factors, such as the ability of LDPs to create effective flow arrest by their improved distal deliverability and sufficiently large caliber.8,31
Our findings suggest comparable mortality rates between LDPs and BGCs, aligning with studies comparing non-BGC to BGC use. 32 Rather than catheter type, predictors of mortality may include age, clinical severity, and sICH. 33
Strengths and limitations
Data were collected from a single center, limiting sample size, and there is a risk of selection bias in guide catheter choice. We did not collect data on patient comorbidities or long-term outcomes as mRS at 90-day follow up was not readily available. A strength is the consistency in skill from a single surgeon, reducing variability compared to a heterogeneous provider group. However, there is potential for a learning curve effect with improved provider skill as time progressed within the study. Future studies may include multicenter data with case matching to account for potential cofounding variables. Given the role of ICA tortuosity in procedural complexity, 34 studies may also compare the effectiveness of these catheters depending on the classification of ICA tortuosity. These insights can inform practices for improved workflow.
Conclusions
This retrospective study of a single-surgeon experience demonstrates that transitioning from BGCs to super-bore 0.088 LDP catheters was associated with significantly faster groin-to-recanalization with a higher first pass rate and higher complete recanalization without increased morbidity and mortality.
Supplemental Material
sj-docx-1-ine-10.1177_15910199251347789 - Supplemental material for Does endovascular thrombectomy using super-bore 0.088” large distal platform offer advantages over balloon guide catheters in acute ischemic stroke secondary to large vessel occlusion?
Supplemental material, sj-docx-1-ine-10.1177_15910199251347789 for Does endovascular thrombectomy using super-bore 0.088” large distal platform offer advantages over balloon guide catheters in acute ischemic stroke secondary to large vessel occlusion? by Annie Trang, Clint Badger, Jose Marino, Souvik Singha, Shyam Majmundar, Timothy Miller, Dheeraj Gandhi and Jacob Cherian in Interventional Neuroradiology
Supplemental Material
sj-docx-2-ine-10.1177_15910199251347789 - Supplemental material for Does endovascular thrombectomy using super-bore 0.088” large distal platform offer advantages over balloon guide catheters in acute ischemic stroke secondary to large vessel occlusion?
Supplemental material, sj-docx-2-ine-10.1177_15910199251347789 for Does endovascular thrombectomy using super-bore 0.088” large distal platform offer advantages over balloon guide catheters in acute ischemic stroke secondary to large vessel occlusion? by Annie Trang, Clint Badger, Jose Marino, Souvik Singha, Shyam Majmundar, Timothy Miller, Dheeraj Gandhi and Jacob Cherian in Interventional Neuroradiology
Footnotes
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Data availability
De-identified data from this study may be made available upon reasonable request to the corresponding author.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the University of Maryland, Baltimore Institutional Review Board (Approval HP-00104512) on January 5th, 2023. This is an IRB-approved retrospective study, and all patient information was de-identified and patient consent was not required. Patient data will not be shared with third parties.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.