
Abstract
Background
Endovascular treatment of small (< 5 mm) and very small (≤ 3 mm) ruptured intracranial aneurysms remains technically challenging, historically carrying elevated procedural risks. Advances in coil technology, such as the Target Tetra Detachable Coil (TTDC), aim to improve embolization safety and efficacy. However, limited data exist on outcomes using TTDC coils specifically for ruptured aneurysms.
Objective
To evaluate the safety, angiographic efficacy, and clinical outcomes of TTDC for small and very small ruptured intracranial aneurysms.
Methods
We retrospectively analyzed 36 patients with ruptured intracranial aneurysms ≤5 mm treated using TTDC between 2023 and 2025 at a single center. Aneurysms were classified as small (n = 28) or very small (n = 8). Patient demographics, aneurysm characteristics, procedural details, angiographic outcomes, clinical outcomes, and complications were analyzed.
Results
Median patient age was 57 years (IQR 43–73); 33.3% were male. The mean aneurysm dome height was 2.6 ± 0.9 mm, the mean neck diameter was 2.4 ± 0.7 mm, and the median dome-to-neck ratio was 1.0. Immediate complete occlusion (Raymond-Roy Class I) was achieved in 42.7% of aneurysms, and residual neck filling (Raymond-Roy Class II) in 25.0%. Follow-up imaging (mean 4.9 months) showed complete occlusion in 37.5% of aneurysms. Recanalization occurred in 29.2% of patients with repeat imaging and 6 (25%) requiring retreatment. Favorable clinical outcomes (mRS 0–2) occurred in 75.0%. Procedural complications occurred in 13.9% (five cases), including two intraprocedural perforations. No rebleeding occurred.
Conclusion
Early experience with TTDC demonstrates safe, effective embolization for ruptured small and very small intracranial aneurysms, supporting the broader use of modern coils in these challenging lesions.
Introduction
The management of small (< 5 mm) and very small (≤ 3 mm) ruptured intracranial aneurysms presents considerable technical and clinical challenges. Coil embolization is particularly challenging as these aneurysms have thin and fragile walls, making it difficult to safely obtain a stable microcatheter position for the deployment of coils. 1 Historically, endovascular treatment of such aneurysms has historically been associated with higher procedural risks. Early series and meta-analyses of coiling very small aneurysms (≤ 3 mm) estimate intraprocedural rupture rates of ∼7% and thromboembolic complication rates of ∼4%.2,3 In the context of acute rupture, however, treatment is mandatory despite these technical challenges, as early re-rupture carries significant risk. 4 Additionally, landmark trials such as the International Subarachnoid Aneurysm Trial (ISAT) 5 and the Barrow Ruptured Aneurysm Trial (BRAT) 6 demonstrated improved clinical outcomes with endovascular coiling compared to clipping in aneurysmal subarachnoid hemorrhage (aSAH). While large aneurysms are thought to have higher rupture risk, studies have demonstrated small aneurysms are responsible for 34%–41% of all aSAH, making it all the more important to be able to endovascularly treat these aneurysms effectively.7–10 Recent advances in coil technology have aimed to improve the safety and efficacy of embolizing tiny aneurysms. Softer, smaller microcoils and complex three-dimensional (3D) coil shapes allow more complete packing of small aneurysm sacs with less catheter kick-back and a lower risk of coil prolapse. 11 Stryker's (Stryker Neurovascular, Fremont, California, USA) Target Detachable Coil (TDC) family, including Ultra, Nano, and the newer Target TDC (TTDC), were designed specifically for small aneurysm embolization. The TTDC, introduced in 2023, features a tetrahedral-shaped framing coil with a stretch-resistant braided core to maximize stability within the aneurysm dome. 12 Theoretically, this design helps the coil conform to the tiny sac, reducing the need for adjunctive stents or balloons to prevent coil herniation. 12 Early multicenter experiences like the ULTRA registry have demonstrated that using Target Ultra and Nano coils in aneurysms ≤5 mm can yield high occlusion rates with an excellent safety profile (zero coil-related complications in 100 small aneurysm cases). 13 Likewise, a recent series using TTDCs for aneurysms up to 10 mm (mostly unruptured) reported ∼89% complete occlusion immediately and no cases of recanalization at short-term follow-up. 11
Despite these advances, there is limited data focusing specifically on ruptured small and very small aneurysms treated with the newest generation coils. Many prior studies combined ruptured and unruptured cases or excluded aneurysms below 3 mm due to perceived risk. To address this gap, we present our early single-center experience using Stryker TDCs for ruptured small (<5 mm) and very small (≤3 mm) aneurysms.
Methods
Study design and patient selection
This study is a retrospective single-center cohort analysis of patients with ruptured intracranial saccular aneurysms under 5 mm in maximum diameter, treated endovascularly with TDC between 2023 and 2025. Institutional Review Board approval was obtained, and patient consent for treatment and data collection was secured in accordance with institutional policies. Surgical cases were not included—only aneurysms managed by coil embolization were analyzed. Any patients whose ruptured aneurysm was treated by surgical clipping or flow diversion during the study period were excluded. Patients who were treated primarily with another coil type were excluded. For each case, procedural and imaging records were reviewed to extract aneurysm characteristics and treatment details. Aneurysm size was defined as the maximum length on pre-treatment angiography, and aneurysm neck width was measured on 3D rotational angiograms. Aneurysms were categorized by size into “small” (3–5 mm) and “very small” (<3 mm) groups for subgroup analysis. There were a total of 36 patients included in the study with eight in the “very small” group and 28 in the “small group.” Aneurysm location was recorded (anterior communicating artery, posterior communicating artery, middle cerebral artery, etc.) to characterize anatomical distribution. Endovascular techniques used were noted: specifically, whether the case was performed with primary coiling versus with adjunctive support. Balloon-assisted coiling was utilized at the operators’ discretion, and stent-assisted coiling was used sparingly given the need for antiplatelet therapy in the context of subarachnoid hemorrhage.
In this series, all aneurysms were treated using TTDC or a combination of TTDC and additional coils as deemed necessary by the operator for aneurysm occlusion. Procedural anticoagulation (e.g. heparin) was administered per standard protocol after securing hemostasis of the rupture. Neurologic intensive care management after coiling followed standard-of-care for aneurysmal subarachnoid hemorrhage.
Outcome measures
Immediate aneurysm occlusion was graded by the Raymond-Roy Occlusion Classification (RROC): complete occlusion (RROC I), residual neck (RROC II), or residual aneurysm (RROC III). Follow-up occlusion was evaluated with digital subtraction angiography (DSA), magnetic resonance angiography (MRA), or computed tomography angiography (CTA), typically 1 to 12 months post-procedure. Any worsening of occlusion at follow-up was considered recanalization. Clinical outcomes were assessed using the modified Rankin Scale (mRS) at 90 days, when available. Procedural complications—including coil-related issues, thromboembolic events, and intraprocedural perforations—were documented.
Statistical analysis
Descriptive statistics were computed for all variables. Continuous variables are reported as mean/median ± standard deviation or range, while categorical variables are presented as frequencies or percentages. No hypothesis testing was conducted due to the small sample size. All analyses were performed using R software version 4.1 (Vienna, Austria).
Results
Patient and aneurysm characteristics
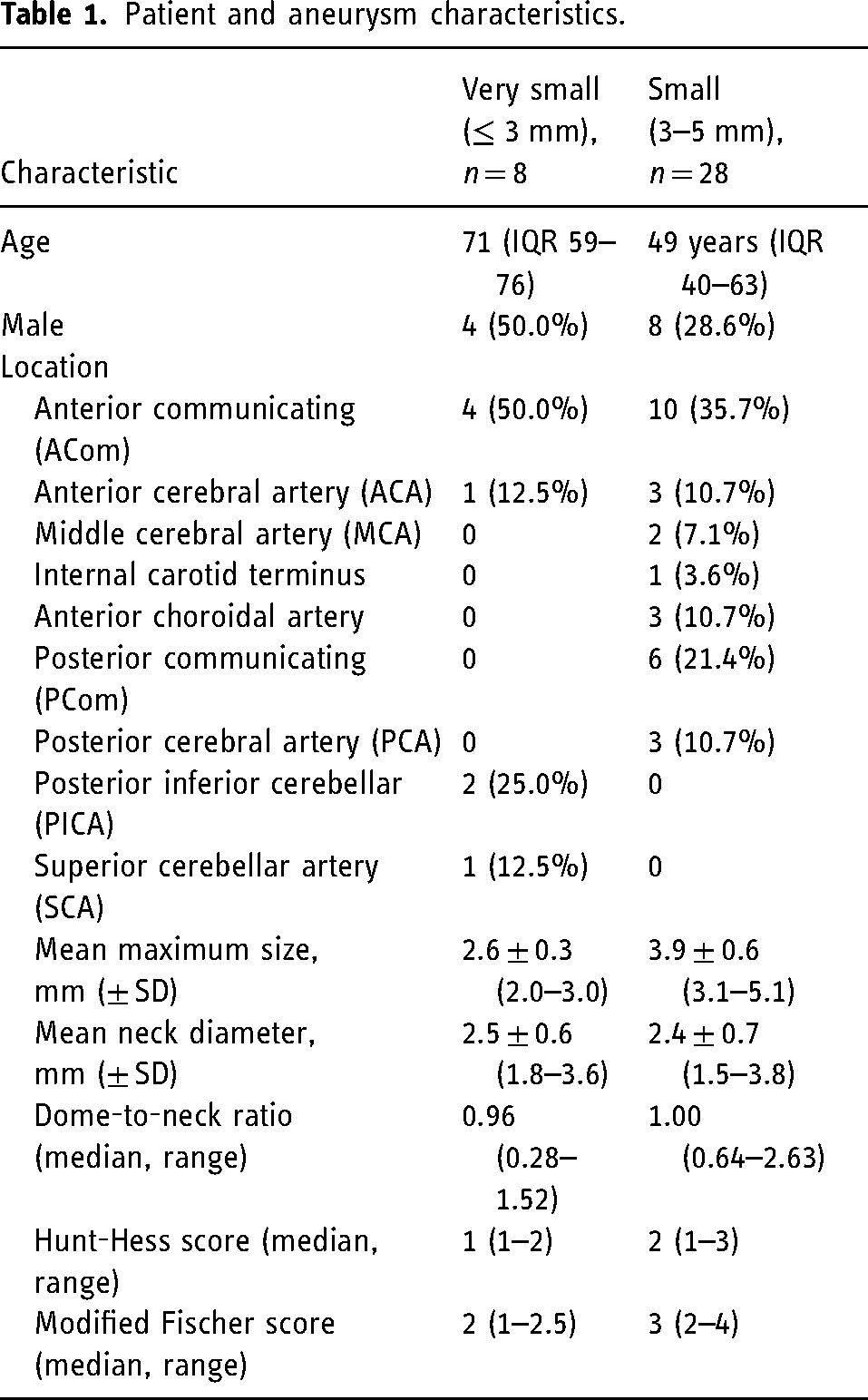
The median age for the entire cohort was 57 years (IQR, 43–73), with younger patients in the small aneurysm group (49 years; IQR, 40–63) compared to the very small aneurysm group (71 years; IQR, 59–76) (Table 1). Overall, 33.3% of patients were male, including 8 (28.6%) in the small aneurysm group and 4 (50.0%) in the very small aneurysm group. The 36 aneurysms had a mean dome height of 2.6 ± 0.9 mm, a mean neck diameter of 2.4 ± 0.7 mm (range, 1.5–3.8 mm), and a median dome-to-neck ratio of 1.0 (range, 0.3–2.6). Most aneurysms were classified as small (28; 77.8%), while 8 (22.2%) were very small. The majority (66.7%) were located in the anterior circulation, predominantly involving the anterior communicating artery (AComm) and anterior cerebral artery (ACA) (50.0%). The baseline subarachnoid hemorrhage severity was mild-to-moderate overall. In the very small aneurysm group, median Hunt-Hess score was 1 (range 1–2), and median modified Fisher score was 2 (range, 1–2.5); in the small aneurysm group, median Hunt-Hess score was 2 (range, 1–3), and median modified Fisher score was 3 (range, 2–4). The distribution of aneurysms by size and location is detailed in Table 1.
Patient and aneurysm characteristics.
Treatment characteristics
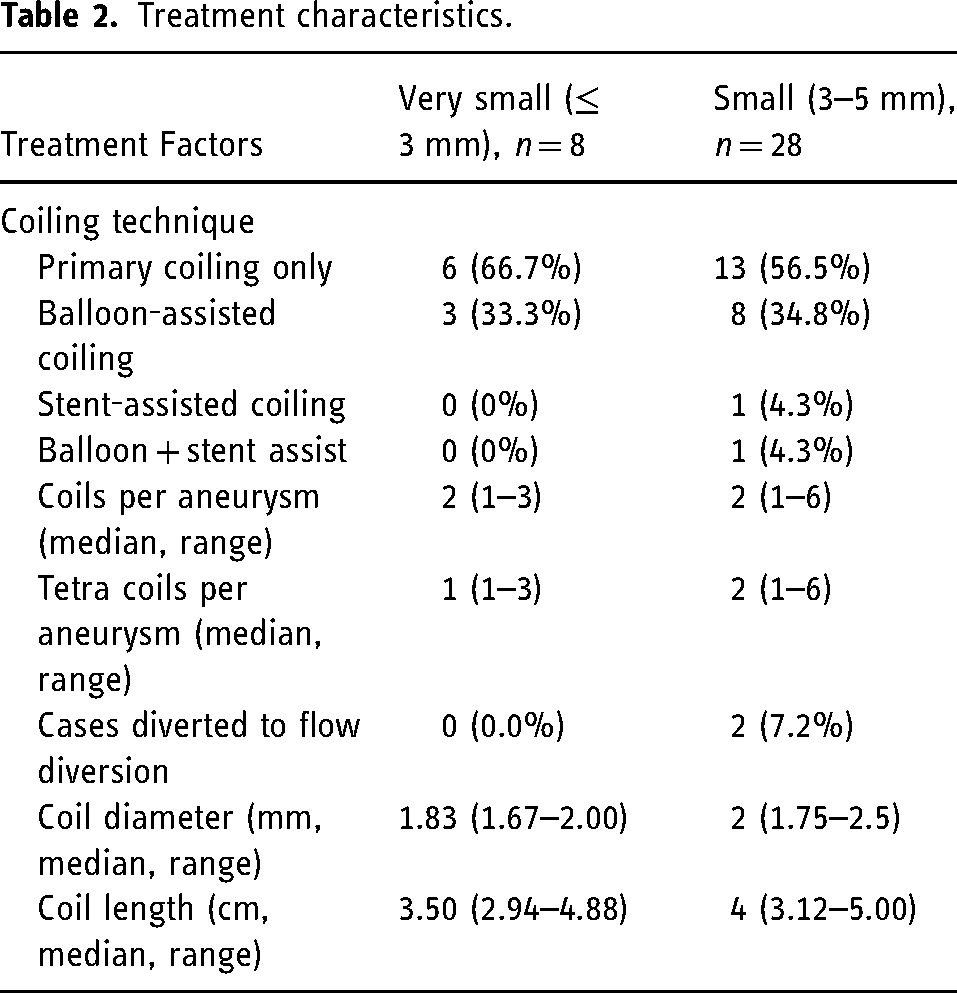
Most aneurysms were treated with primary coiling alone (19 cases, 52.8%), although adjunctive balloon assistance was frequently used (11 cases, 30.6%), and stent assistance was rare (Table 2). Two cases (7.1%) in the small aneurysm group required flow diversion. The median number of coils deployed per aneurysm was 2 (range, 1–6), with a median of two Tetra coils used per aneurysm (range, 1–6). The median coil diameter used in the very small aneurysm group was 1.83 mm (range, 1.67–2.00) while the median length was 3.5 cm (range 2.94–4.88). The median coil diameter in the small aneurysm group was 2 mm (range 1.75–2.50) while the median coil length was 4 cm (range 3.12–5.00). Treatment characteristics by aneurysm size group are summarized in Table 2.
Treatment characteristics.
Angiographic outcomes
Immediate angiographic results showed complete occlusion (Raymond-Roy Class I) in 15 out of 36 aneurysms (41.7%). An illustrative example of successful complete occlusion following deployment of a single Target Tetra coil is provided in Figure 1. Nine aneurysms (25.0%) had residual neck filling (Raymond-Roy Class II), while 8 (22.2%) demonstrated residual aneurysm filling (Raymond-Roy Class III) (Table 3). Follow-up imaging was available for 24 aneurysms (66.7%), obtained at a mean interval of 4.9 months. At follow-up, complete occlusion was seen in nine aneurysms (37.5%), residual neck in five (20.8%), and residual aneurysm filling in four (16.7%) (Table 3). Recanalization occurred in seven aneurysms (29.2% of followed cases), with retreatment required in six cases (25.0% of followed cases), predominantly among small aneurysms (Table 3). DSA was predominantly used as the follow-up imaging modality, with a few cases being followed by MRA and one case with CTA.
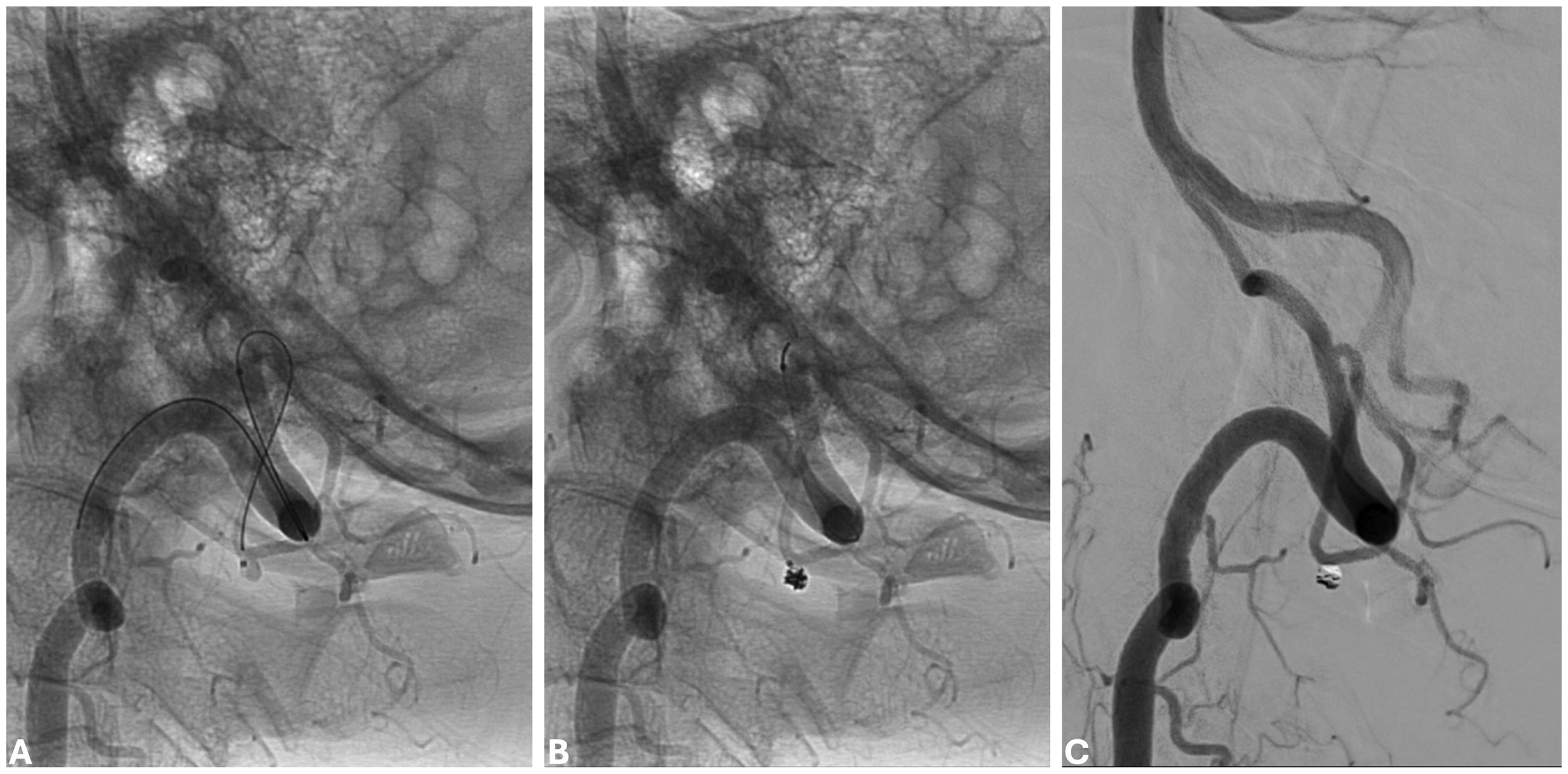
Example of Target Tetra Coil embolization of a small ruptured aneurysm. (A) Pre-treatment angiogram demonstrates a small ruptured aneurysm of the right posterior inferior cerebellar artery (PICA). (B) Intraprocedural angiogram after deployment of a single Target Tetra Coil demonstrates stable positioning within the aneurysm dome. (C) Post-treatment angiogram demonstrates complete occlusion (Raymond-Roy Class I) of the aneurysm with preservation of the parent vessel.
Angiographic outcomes.
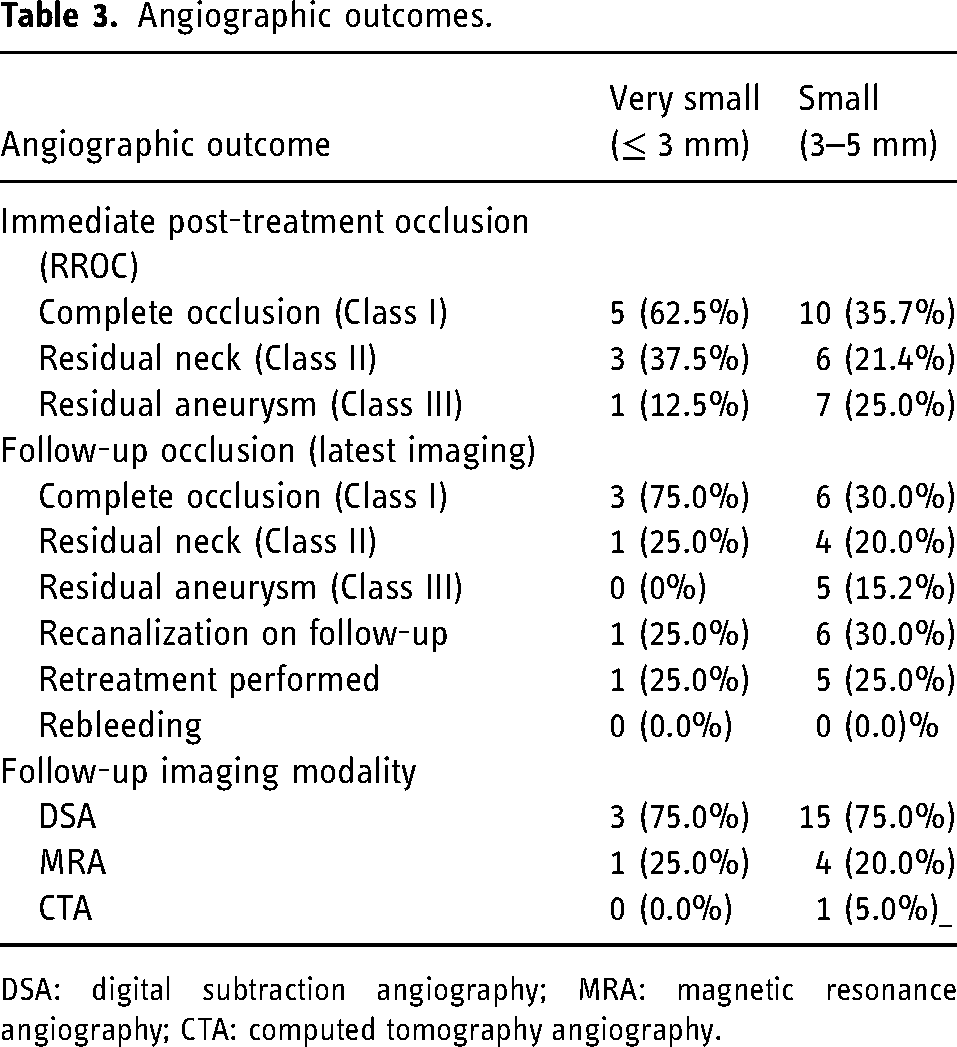
DSA: digital subtraction angiography; MRA: magnetic resonance angiography; CTA: computed tomography angiography.
Clinical outcomes
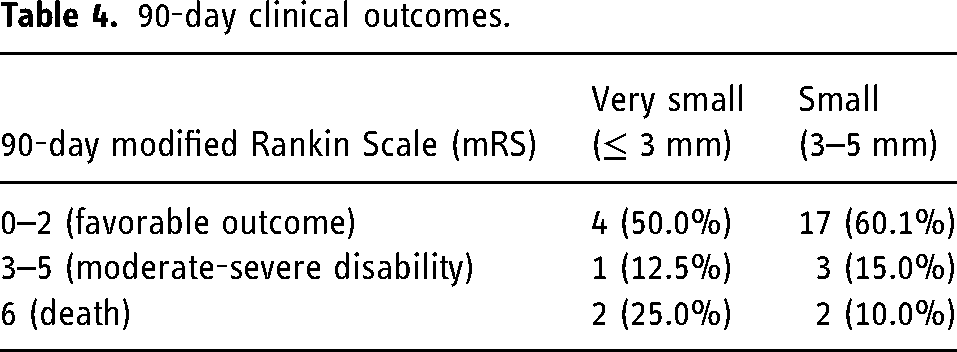
Ninety-day mRS scores were available for 28 patients (77.8%) and were favorable (mRS 0–2) in 21 patients (75.0%) (Table 4). Moderate-to-severe disability (mRS 3–5) was observed in four patients (14.3%), and mortality (mRS 6) occurred in four patients (14.3%). Detailed clinical outcomes by aneurysm size category are presented in Table 4. Notably, there were no cases of early re-rupture in any of the treated aneurysms.
90-day clinical outcomes.
Procedural complications
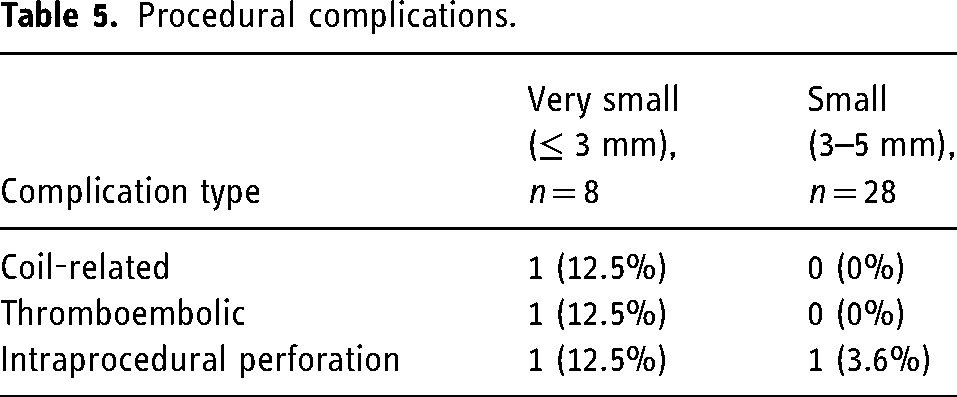
Procedural complications occurred in five cases (13.9%), including coil protrusion into the parent vessel (n = 1), thromboembolic events requiring intervention (n = 1), and intraprocedural perforation (n = 2; 5.6%) (Table 5). Clinical information regarding the intraprocedural perforations is as follows. In the first case with intraprocedural perforation, contrast extravasation was noted on follow-up angiography after placing the final coil. Protamine was administered immediately and a balloon was advanced into the preceding A1 segment and was inflated and remained inflated until no further contrast extravasation was seen. Follow-up flat panel CT demonstrated stable ventricular size with small volume contrast extravasation in basal cisterns. This patient was then admitted to the Neurosciences Critical Care Unit (NSICU) and underwent standard aSAH management. She had an excellent subsequent clinical course and was discharged home. The second patient with intraprocedural perforation was noted to have contrast extravasation after placement of the fourth coil. The balloon microcatheter, which was positioned in the A1 segment proximal to the aneurysm was inflated and after some time was deflated, with follow-up angiography demonstrating no further contrast extravasation. Follow-up flat panel CT demonstrated small volume contrast in the basal cisterns, and this patient also had an excellent neurological outcome, with discharge home after standard NSICU post-aSAH care. The detailed breakdown of procedural complications by aneurysm size group is shown in Table 5.
Procedural complications.
Discussion
Our initial single-center experience highlights the feasibility, efficacy, and safety of using TTDCs for ruptured small (< 5 mm) and very small (≤ 3 mm) ruptured intracranial aneurysms. Immediate angiographic outcomes were favorable, with approximately half of the aneurysms achieving complete occlusion (Raymond-Roy Class I) and most others showing minimal residual neck filling (Raymond-Roy Class II). At mid-term follow-up (∼6 months), occlusion durability remained robust, consistent with prior literature evaluating small aneurysm coiling outcomes.11,14
Importantly, very small aneurysms (≤ 3 mm) performed comparably to those between 3 and 5 mm in terms of occlusion stability, reflecting recent data demonstrating high occlusion rates (≥ 85%) achievable with modern coil technologies, even in these extremely small lesions.11,14 This finding contrasts earlier studies citing significant technical challenges, elevated recanalization, and complication rates for aneurysms ≤ 3 mm, underscoring advances in coil design and delivery systems.12,13
Recanalization was observed in 27.9% of aneurysms who had mid-term follow-up imaging, predominantly among those with incomplete initial occlusion (Raymond-Roy Class III). Retreatment was required in several of the small aneurysms but in only one of the very small aneurysms. These retreatments were seen in predominantly aneurysms with complex morphology or more than one daughter sac, making the initial treatment particularly challenging. Prior case series of TTDC include Kim et al. 12 which included a primarily unruptured (98%) population, and demonstrated an excellent rate (89%) of immediate occlusion, with neck remnants seen in 1 (2.3%) patient and residual aneurysm in 2 (4.7%) patients on follow-up. No re-treatment was required in this series. Another relevant case series is the ULTRA registry, 13 which reported the experience with Target Ultra/Nano coils for aneurysms <5 mm in a mixed ruptured and unruptured population. This registry demonstrated 92% complete or near complete occlusion on immediate angiographic follow-up. 15% of patients in this series required retreatment by final follow-up which is comparable to the retreatment rate seen in our study (as 16.7% of the entire cohort required re-treatment), again highlighting the success of TTDC in treating a historically challenging type of aneurysm.11,13 Notably, the ULTRA registry had no intraprocedural ruptures and no coil-related adverse events. When comparing our current study with these and other prior case series, it is important to note that the treatment strategy for ruptured aneurysms, particularly those that are small, is often much more conservative than unruptured or larger aneurysms, as the primary goal is to secure the dome and/or bleeding side, permitting incomplete occlusion if necessary and at times prompting repeat treatment. 15 That being said, in this series, complete initial occlusion appeared protective against recurrence, underscoring the importance of achieving optimal initial coil packing. Another important point is that stent assistance is often avoided in the acute rupture setting to avoid necessitating the use of antiplatelet agents, and this may also contribute to a lower rate of complete occlusion than that seen in unruptured series.
The overall complication profile was acceptable and consistent with previous studies evaluating small aneurysms.11,14 Specifically, the intraprocedural perforation rate (≈3%) and coil-related complication rate (∼5%) are comparable to rates cited in recent series, demonstrating improved safety profiles of newer-generation coils, such as the TTDCs.12,13 Although our study reported a slightly higher rate of intraprocedural rupture than the ULRA registry, both ruptures were easily controlled and they took place in likely thin-walled complex aneurysms that were highly prone to rupture. Importantly, no intraprocedural rupture was seen in the very small aneurysm group. Importantly, procedural complications did not lead to permanent neurological deficits or rebleeding in our cohort.
Limitations include our study's retrospective, single-center design, modest sample size, and relatively short follow-up duration (∼5 months). Additionally, as is the case with retrospective analyses, the lack of a control group limits the ability to perform a direct comparison. One important limitation is the variable interval follow-up as well as the use of different imaging modalities. As DSA is the most sensitive imaging modality, patients who underwent MRA or CTA may have had small remnants that were not detected, although in our study the majority of patients underwent follow-up with DSA. The variable interval follow-up in this study may also confound the follow-up angiographic outcomes. Similarly, one-third of the patients did not have follow-up imaging, and those who did had a relatively short mean follow-up time of ∼5 months. These factors limit durability conclusions from this study. Future multicenter registries with extended follow-up periods and volumetric analyses of coil packing density will be valuable in confirming these findings and optimizing endovascular techniques.
In conclusion, our results suggest that modern detachable coils, particularly Tetra coils, enable safe and effective endovascular management of ruptured very small (≤ 3 mm) and small (< 5 mm) aneurysms. High initial occlusion rates, sustained mid-term durability, and low complication rates support expanding the role of coil embolization for these challenging lesions.
Footnotes
Authors’ contributions
AM and MTC: concept and design; AM, JF, DG, and MTC: data collection; AM, MTC, DG, JF, SM, RDL, CK, and TS: analysis and interpretation of data; AM, JF, DG, MTC: drafting of manuscript; MTC, JF, SM, RDL, CK, and TS: critical revision for intellectual content; MTC: study supervision. All authors reviewed and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.