
Abstract
Objective
Intracranial plaque enhancement (IPE) is a potential biomarker of plaque vulnerability but lacks a standardized definition. While subjective assessment may be prone to observer variability, a voxel-based quantification method can detect subtle signal intensity (SI) changes. This study aimed to compare the inter-rater reliability of subjective IPE evaluation with that of a voxel-based quantification method.
Methods
Patients with stroke due to intracranial atherosclerosis were prospectively imaged using 7 T vessel wall magnetic resonance imaging. Two adjudicators independently assessed IPE, with discrepancies resolved by a third, experienced neuroradiologist. IPE distribution was quantified using a semiautomated method based on SI measurements from post-contrast T1-weighted images. The mean enhancement ratio was calculated for each plaque to assess gadolinium enhancement. Inter-rater reproducibility and the concordance between subjective and objective assessments were evaluated. Regression analysis was performed to identify plaque morphological features that influenced the reliability of subjective IPE adjudication compared to the objective method.
Results
We analyzed 75 plaques from 41 patients. Inter-rater agreement for IPE adjudication was poor (κ = 0.34). Following consensus, 43% of plaques (32/75) were classified as enhancing, whereas 57% (43/75) were non-enhancing. The agreement between subjective and objective IPE assessments was moderate (κ = 0.40, p < 0.001). Subjective assessment was more likely to reliably adjudicate IPE for plaques exhibiting >50% stenosis (odds ratio (OR), 1.04; p = 0.02) and a positive remodeling index (OR, 2.20; p = 0.02). In contrast, it was less reliable when evaluating posterior circulation plaques (OR, 0.23; p = 0.01).
Conclusion
Subjective assessment of IPE demonstrated poor inter-rater agreement and only moderate concordance with voxel-based quantification following consensus.
Keywords
Introduction
High-resolution vessel wall imaging (HR-VWI) is a useful tool for characterizing different vasculopathies, such as atherosclerosis and vasculitis.1,2 It helps clinicians distinguish intracranial atherosclerotic disease from other vasculopathies. 3 HR-VWI can also help detect the culprit atherosclerotic plaques in patients formerly classified as having cryptogenic stroke. 4 Additionally, it aids in stratifying stroke risk in patients with non-stenotic intracranial plaques by detecting high-risk features such as positive remodeling, intraplaque hemorrhage and post-gadolinium (Gd) intracranial plaque enhancement (IPE). 5 Among the most promising imaging biomarkers of symptomatic plaques is the enhancement after the administration of intravenous Gd. 6 A meta-analysis by Song et al., evaluating 1750 atherosclerotic lesions, found IPE to be strongly associated with stroke recurrence. 7 In clinical practice, IPE is determined by visually comparing pre- and post-contrast images, an approach that relies on the reader's experience, 1 making it susceptible to human error. Furthermore, the lack of a standardized definition for IPE and the small size of intracranial plaques makes HR-VWI interpretation challenging.6,8 Additionally, flow artifacts—more prominent on post-contrast imaging—can mimic arterial wall lesions and affect the assessment of enhancement. 9
Subjective adjudication of IPE may lack reproducibility, underscoring the need for objective methods to accurately assess plaque enhancement. 10 Currently, no reference standard exists for IPE quantification, and quantitative approaches remain limited. Sanchez et al. employed a semiautomated technique to analyze signal intensity (SI) distribution within atherosclerotic plaques, reporting an area under the curve of 0.87 for identifying symptomatic lesions. 11 This method was optimized for voxel-based IPE detection, allowing for the identification of subtle changes in SI distribution and detailed sampling of small plaques while minimizing contamination from adjacent structures. Additionally, it allowed for histogram analysis of pre- and post-contrast enhancement curves, aiding in the identification of false-positive findings. Given the variability inherent in subjective IPE assessment, we evaluated inter-rater reproducibility using 7 T HR-VWI. We then compared consensus-based subjective evaluation with a voxel-based quantification method and explored morphological factors that may affect the reliability of subjective assessments relative to the objective approach.
Methods
After institutional review board approval, patients with ischemic stroke attributed to intracranial atherosclerotic disease were prospectively imaged with 7 T HR-VWI. The intracranial atherosclerotic disease stroke etiology was adjudicated according to the Trial of Org 10172 in Acute Stroke Treatment. 12 Informed consent was obtained prior to enrollment, and participants were imaged between August 2019 and April 2024. Patients who were medically unstable, were claustrophobic or had a glomerular filtration rate of <60 mL/min per 1.73 m2 were excluded. Demographical information was then retrieved from electronic medical records (Figure 1).
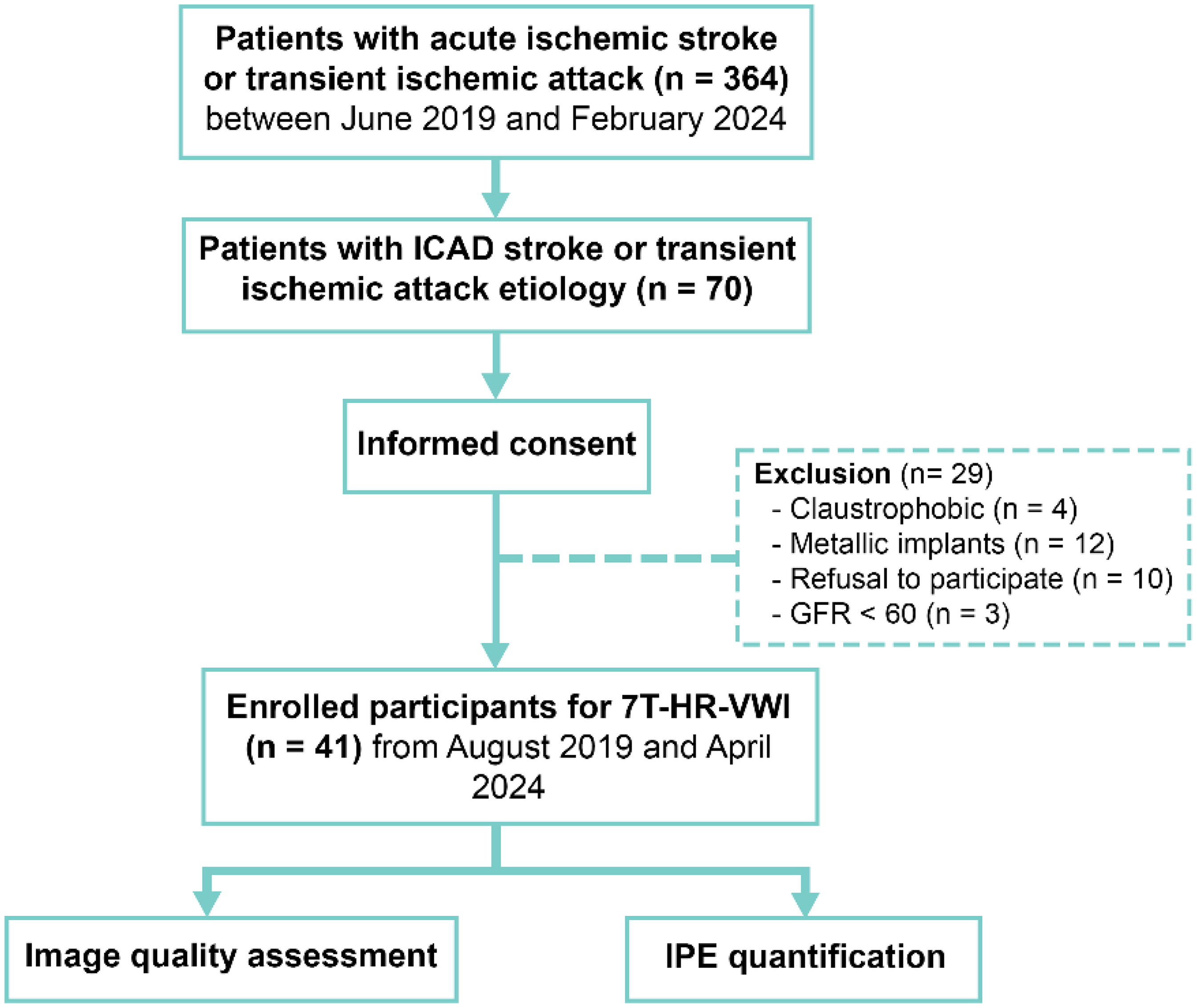
Study inclusion and exclusion flowchart. ICAD: intracranial atherosclerotic disease; GFR: glomerular filtration rate; HR-VWI: high-resolution vessel wall imaging; IPE: intracranial plaque enhancement.
Magnetic resonance imaging vessel wall imaging protocol
A MR950 7 T scanner (GE Healthcare, Waukesha, WI) equipped with an eight-channel head coil was used for imaging. The following isotropic sequences were acquired: pre- and post-3D T1-weighted fast spin-echo CUBE (TR/TE, 1000/10 ms); flip angle, 90; matrix, 384 × 384 × 230; resolution, 0.5 × 0.5 × 0.5 mm; echo train length, 22; acceleration, ARC 2 (phase) × 2 (slice); acquisition time, 4 min 27 s); and 3D time-of-flight. Post-contrast T1-weighted images were obtained 5 min following Gd administration (Table S1).
Plaques’ characterization
Pre- and post-contrast T1-weighted multiplanar sequences were analyzed using a Picture Archiving and Communication System (PACS, version 12.1.6.1005, Carestream Vue). The supraclinoid internal carotid, middle cerebral, anterior cerebral, vertebral, basilar, and posterior cerebral arteries were examined for the presence of plaques, defined as a marked eccentric or focal thickening of the arterial wall relative to an adjacent normal segment, with a plaque burden exceeding 40%.4,13 The degree of stenosis for each plaque was measured using the WASID criteria on time-of-flight imaging, and quantified as follows: [1 − (Diameter at stenosis/Diameter of proximal normal artery) × 100]. 14 Regions of interest were then selected to determine the area of the vessel lumen at the point of maximal stenosis, the area of the outer vessel wall at maximal stenosis, and the area of the vessel lumen proximal to the site of maximal stenosis. Plaque morphology was classified as concentric if wall thickening encompassed ≥50% of the arterial wall circumference on cross-sectional views. 4 The degree of stenosis based on plaque area was obtained using the formula: [(Area of the lumen at proximal normal segment − Area of the lumen at maximal stenosis)/Area of the lumen at proximal normal segment × 100%]. 15 Remodeling index was computed following the methodology described by Qiao et al., where the outer vessel wall area at the point of maximal stenosis is divided by the outer wall area at a proximal, presumably normal reference segment. A plaque was classified as having positive remodeling if its index exceeded 1.05. 16 Plaque burden was determined as follows: [(Area of the outer vessel wall at maximal stenosis − Area of the vessel lumen at the point of maximal stenosis)/Area of the outer vessel wall at maximal stenosis × 100%]. 17
Subjective adjudication of IPE
IPE was assessed across multiple planes. 6 Following the criteria established by Qiao et al., IPE was defined as enhancement equal to or higher than that of the pituitary stalk, 18 with no visible enhancement on pre-contrast images. The pituitary stalk was used as a reference due to its anatomic proximity to the circle of Willis, consistent strong post-contrast enhancement, hyperintense signal relative to white matter, and prior use in similar studies.6,19,20 Two raters, each with 2 years of experience in HR-VWI interpretation, independently reviewed five training cases—acquired using the same imaging parameters of the clinical cohort. They then proceeded to evaluate all study cases. Any discrepancies were resolved by a senior neuroradiologist with over 30 years of experience. All adjudicators adhered to the recommendations of the American Society of Neuroradiology Intracranial VWI Study Group, 1 and were partially blinded to clinical information (limited to knowledge of stroke location from imaging).
Objective quantification of IPE
A semiautomated method for analyzing SI in pre- and post-contrast black blood sequences was customized for a voxel-based IPE quantification (Figure 2). 11 This method has been previously used in both 3 T and 7 T scanners.11,21,22 In a cohort of 80 plaques, this method demonstrated 83% sensitivity, 86% specificity, and an area under the curve of 0.87 for identifying culprit plaques. 11 Plaque segmentations were performed using a 3D Slicer (version 5.6.1). A training session was conducted on 15 plaques to standardize the segmentation process. Once adequate agreement was achieved, two researchers—each with over a year of experience using 3D Slicer—segmented all study cases. Following adequate co-registration, the same segmentation was applied to both pre- and post-contrast T1-weighted images for SI analysis. In cases of suboptimal alignment, segmentations were carefully reviewed and adjusted to ensure consistency across sequences. A 2 mm region of interest from the corpus callosum was segmented and used for SI normalization. This method normalizes SI to the corpus callosum due to its minimal enhancement (<4%) and its larger size, which reduces partial volume effects. The pituitary stalk was not used for SI normalization because its avid enhancement after Gd administration can introduce artifacts in objective quantification (Supplemental Figure 1). 11 Voxel-based color maps were then generated with an in-house MATLAB 2024a code (MathWorks, Natick, MA, USA). The mean SI of the entire plaque on pre- and post-contrast sequences, normalized to the corpus callosum, was calculated for comparison. The mean post-contrast SI after normalization was defined as the mean enhancement ratio (MER), a standardized metric of contrast enhancement. 11 Histograms were then created to analyze IPE distribution. An intracranial plaque was considered as objectively “enhancing” if the MER (SI of the plaque post/SI of the corpus callosum post) was greater than one, indicating higher SI in the plaque compared to the corpus callosum (Figure 2). Although not a definitive standard, the MER >1 offers an objective metric that helps mitigate bias in IPE assessment, particularly given the heterogeneous enhancement patterns and variable Gd uptake observed in intracranial plaques on T1-weighted imaging.23,24 This metric has been previously validated, demonstrating significantly higher values in culprit compared to non-culprit plaques (0.80 ± 0.30 vs. 0.61 ± 0.17, p = 0.004). 11
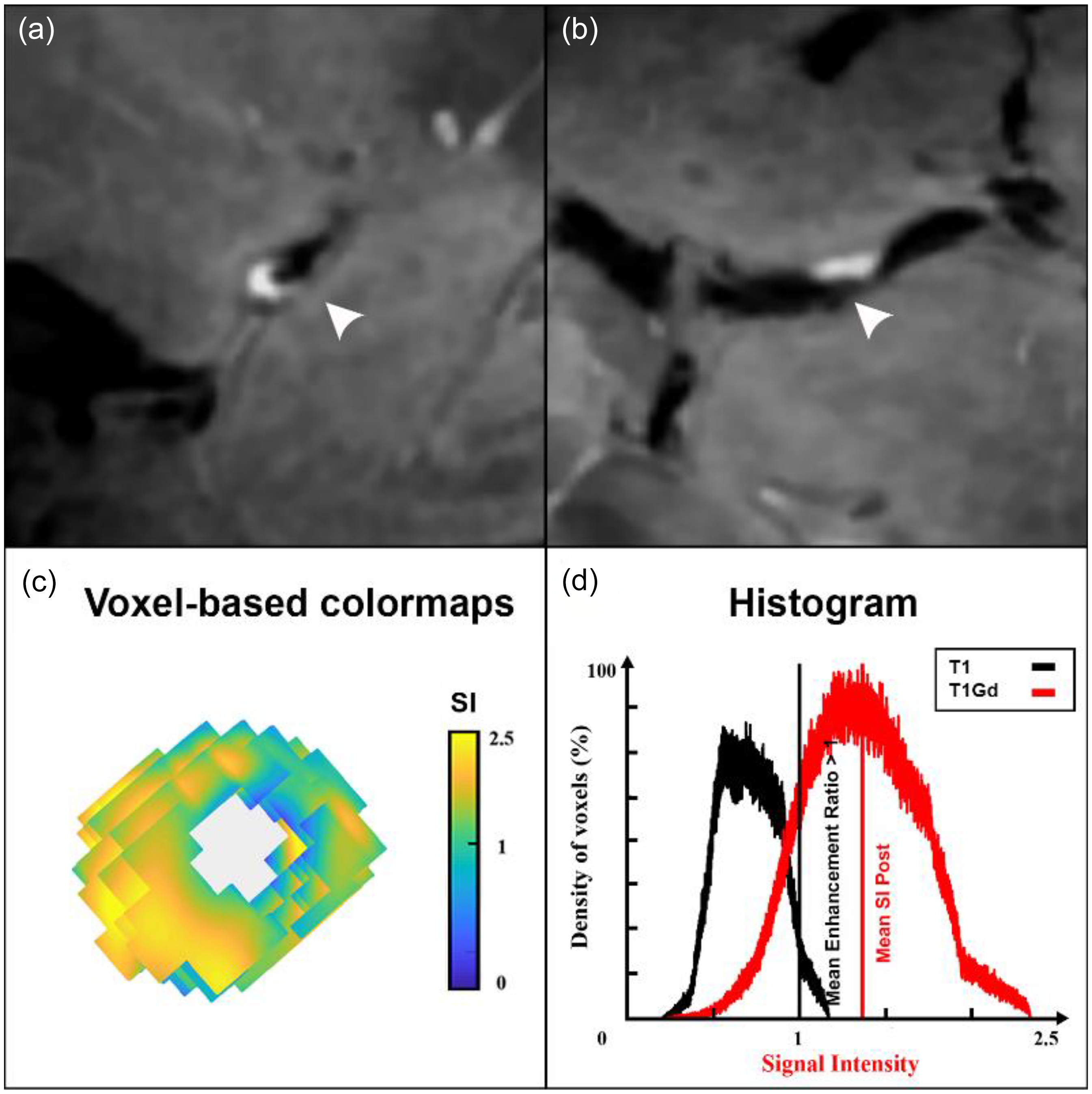
Quantification of intracranial plaque enhancement (IPE) using three-dimensional voxel-based analysis. The signal intensity (SI) of the entire plaque is obtained from T1 and T1+Gd MRI sequences. Voxel-based color maps depicting the SI distribution within the plaque are then generated. Histograms are used to ensure that the SI measurements are restricted to the plaque itself, excluding surrounding structures such as cerebrospinal fluid and brain parenchyma. Finally, the mean SI in T1+Gd MRI is calculated to determine the mean enhancement ratio (MER =SI of the plaque post-Gd/SI of the corpus callosum post-Gd > 1). (a, b) A highly enhancing plaque in the middle cerebral artery is visualized on sagittal and axial 7T HR-VWI images. (c) A corresponding color map shows brighter areas indicating regions of greatest enhancement. (d) The histogram displays the SI distribution within the intracranial plaque: the left curve (T1) represents pre-contrast values, and the right curve (T1+Gd) represents post-contrast values, demonstrating a rightward SI shift after gadolinium administration. X axis = SI after normalization with the corpus callosum, and Y axis=percentage of voxels within the plaque. Gd: gadolinium; MRI: magnetic resonance imaging; HR-VWI, high-resolution vessel wall imaging.
Statistical analysis
Statistical analyses were performed using R version 4.3.3. Normally distributed continuous variables are presented as mean ± standard deviation and not normally distributed variables as median and interquartile range. Inter-rater agreement on plaque identification was assessed using Cohen's kappa, while inter-rater reproducibility for SI quantification was evaluated using the intraclass correlation coefficient (ICC) on a subset of 15 plaques. Kappa statistics were used to determine: (1) inter-rater agreement between the two adjudicators and (2) agreement between subjective consensus adjudication and objective IPE assessment. Kappa coefficients below 0.4 were classified as poor, values between 0.4 and 0.75 as fair to good, and values above 0.75 as excellent reliability. 25 The impact of plaque location, morphology, degree of stenosis, remodeling index, the area degree of stenosis, and plaque burden on subjective assessment were analyzed with univariate logistic regression. A multivariable model was constructed using the predictors from the previous univariate models. An all-subsets approach was used to find the optimal multivariate model as dictated by the Akaike information criterion. Predictor variables with correlation coefficients greater than 0.5 were not included in the same model.
Results
A total of 75 plaques from 41 patients (mean age, 59 years ± 12 SD, 20 men and 21 women) were evaluated (Figure 1). The middle cerebral artery was the most common plaque location, accounting for 44% (33/75) of the plaques (Table 1).
Study participant demographics.
AIS: acute ischemic stroke; HR-VWI: high-resolution vessel wall imaging, MER: mean enhancement ratio.
All significant p values are highlighted in bold.
Subjective versus objective assessments of plaque enhancement
Inter-rater agreement for plaque identification was good (κ = 0.8), whereas agreement for assessing IPE was low (κ = 0.34). Following final adjudication by the senior reviewer, 32 of the 75 plaques (43%) were classified as “enhancing,” whereas 43 (57%) were deemed “non-enhancing.” In the training subset of 15 plaques, the voxel-based method of SI quantification achieved strong inter-rater reproducibility, with an ICC of 0.85. Across all plaques analyzed, voxel-based IPE quantification demonstrated higher mean SI post-contrast versus pre-contrast (1.08 ± 0.42 vs. 0.57 ± 0.17, p < 0.001). Using a MER > 1 threshold, 49% (37 plaques) were classified as “enhancing” and 51% (38 plaques) as “non-enhancing.” The subjective and objective classifications of IPE were different (p < 0.001) and achieved a moderate level of agreement after consensus (κ = 0.40; Table 2 and Figure 3).
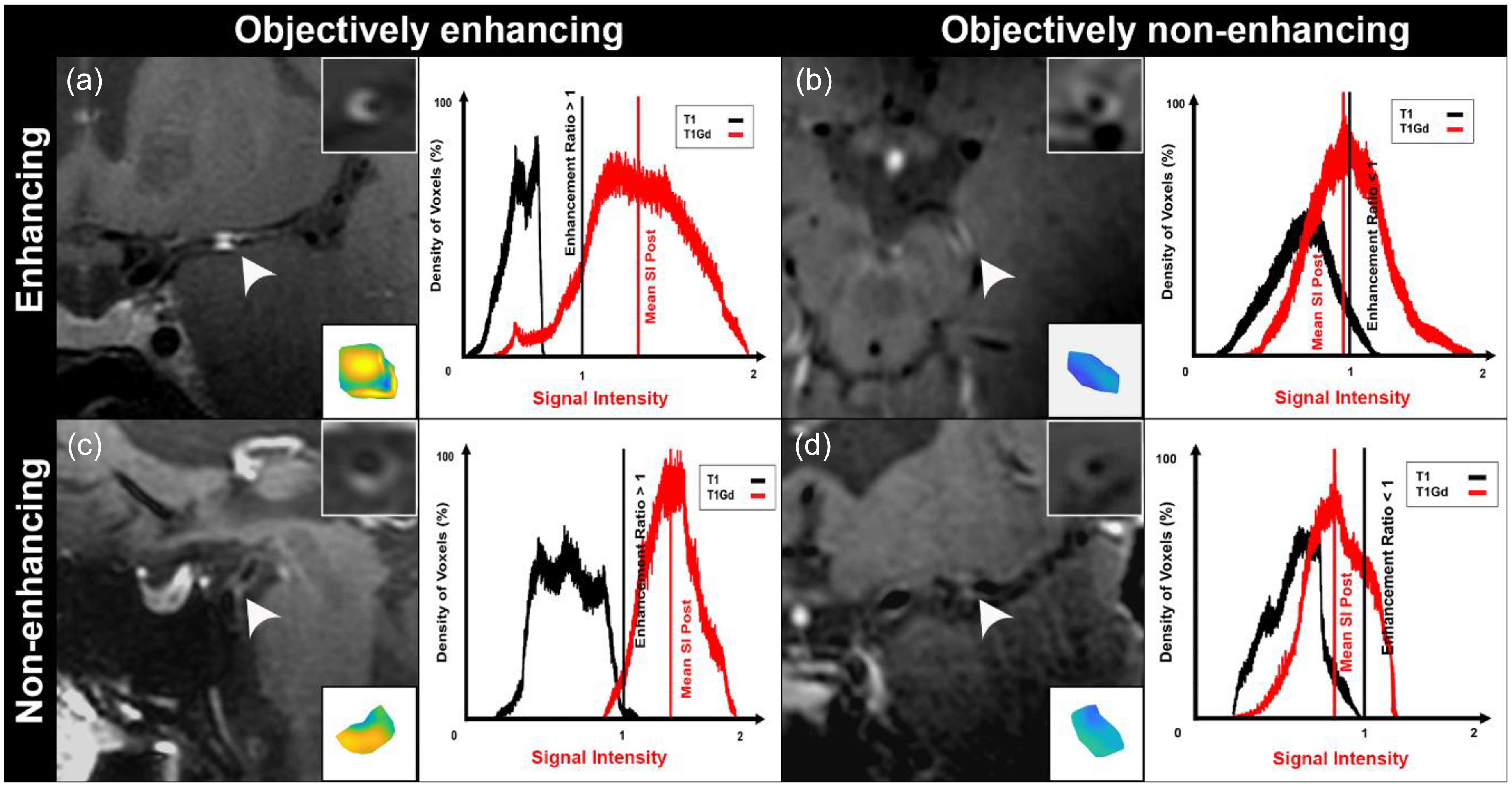
Subjective assessment of intracranial plaque enhancement (IPE) compared to three-dimensional voxel-based IPE analysis. In clinical practice, IPE determination relies on visual adjudication which is susceptible to bias. In the objective quantification of IPE, the mean SI on T1 + Gd is normalized to the SI of the corpus callosum and is defined as the mean enhancement ratio (MER). An intracranial plaque is considered objectively “enhancing” if the MER value was higher than one. In the objective assessment, intracranial plaques that are “enhancing” are represented with yellow color, on the other hand, “non-enhancing” plaques display blue color. (a) Coronal view of a left middle cerebral artery plaque subjectively adjudicated as “enhancing” and objectively as “enhancing.” (b) Axial view of a left posterior cerebral artery “plaque.” While this plaque appears deceptively enhancing on visual inspection, objective assessment confirmed the absence of true enhancement. (c) Sagittal view of a basilar artery plaque subjectively adjudicated as “non-enhancing”; however, it was objectively “enhancing.” (d) Coronal view of a left middle cerebral artery plaque subjectively described as “non-enhancing” and objectively defined as “non-enhancing.” The histograms represent the mean SI on pre- and post-Gd T1, which is used for determination of MER (SI of the plaque post-Gd/SI of the corpus callosum post-Gd > 1). Inlets show orthogonal views of each arterial segment depicted in the histograms. SI: signal intensity; Gd: gadolinium.
Subjective adjudication of plaque enhancement compared to 3D voxel-based quantification of signal intensity.
MER, mean enhancement ratio.
Subjective assessment was more reliable for identifying IPE in plaques with >50% stenosis (odds ratio (OR), 1.05; 95% confidence interval (CI), 1.02–1.08; p = 0.003), larger plaque stenosis (OR, 1.03; 95% CI, 1.01–1.06; p = 0.004), higher plaque burden (OR, 1.06; 95% CI, 1.02–1.10; p = 0.008), and a positive remodeling index (OR, 2.30; 95% CI, 1.30–4.48; p = 0.008). Conversely, adjudicators were less likely to reliably identify IPE when compared to the objective voxel-based method in plaques located in the posterior circulation (OR, 0.29; 95% CI, 0.09–0.82; p = 0.02). In multivariable analysis, subjective IPE adjudication remained less reliable for plaques with <50% stenosis (OR, 1.04; 95% CI, 1.01–1.08; p = 0.02), negative remodeling (OR, 2.20; 95% CI, 1.17–4.54; p = 0.02), and those located in the posterior circulation (OR, 0.23; 95% CI, 0.06–0.73; p = 0.01; Table 3).
Univariable and multivariable analysis of plaque morphological parameters associated with reliable subjective adjudication of plaque enhancement.
NA: not applicable; OR: odds ratio; 95% CI: 95% confidence interval.
Posterior location includes basilar, posterior cerebral and vertebral arteries.
All significant p values are highlighted in bold.
Discussion
In this study, subjective IPE determination was compared with a voxel-based method of SI quantification. Inter-rater agreement for subjective IPE adjudication was low (κ = 0.34), while the overall concordance between subjective and objective methods was moderate (κ = 0.40). Subjective adjudication was less reliable for non-stenotic plaques, plaques exhibiting negative remodeling, and those located in the posterior circulation.
HR-VWI is commonly used to diagnose intracranial vasculopathies (94.4%) and characterize symptomatic atherosclerotic plaques (37.6%). 2 Additionally, HR-VWI enables early detection of asymptomatic plaques, helping identify individuals at increased long-term risk of ischemic stroke. 26 IPE on HR-VWI has emerged as a promising biomarker for detecting plaques at risk of causing ischemic stroke. A meta-analysis by Gupta et al., which analyzed 295 intracranial plaques, found a strong correlation between IPE and acute stroke in the ipsilateral vascular territory. 6 Similarly, Song et al. included 1750 plaques, demonstrating a significant association between IPE and recent ischemic stroke (OR, 7.42; 95% CI, 3.35–16.43). 27 In current practice, IPE is assessed by comparing pre- and post-contrast HR-VWI sequences.1,6 However, this approach may be prone to human error, limiting its reproducibility. In addition, HR-VWI interpretation can be challenging due to inadequate flow suppression, limited spatial resolution, and the potential for confusing plaques with artifactual wall thickening or adjacent veins. 28 Furthermore, variations in IPE degree across sequential post-contrast phases on HR-VWI, 29 may further complicate adjudicators’ interpretation. The optimized contrast-to-noise ratio of the 7 T HR-VWI can improve the assessment of intracranial plaques. For instance, Zwartbol et al. analyzed 130 patients using 7 T HR-VWI, finding that 96% had at least one atherosclerotic lesion. 30 Similarly, Harteveld et al. demonstrated that 7 T HR-VWI had superior sensitivity in detecting IPE (29 vs. 7 enhancing plaques) compared to 3 T HR-VWI. Additionally, 41% of the lesions detected on 7 T were not visible on 3 T HR-VWI. 31 However, flow artifacts, which can mimic arterial wall lesions, are often more pronounced on post-contrast imaging and hinder visual enhancement adjudication. 9 Despite utilizing 7 T HR-VWI, a standardized 5-min Gd administration protocol, and a standard definition of IPE based on Qiao et al. criteria, 18 in this study the subjective adjudication of IPE achieved a poor inter-rater agreement (κ = 0.34). Given the variability of subjective IPE adjudication—even with the improved spatial resolution at 7 T HR-VWI—there is a need for quantitative methods to accurately assess plaque enhancement.
The voxel-based SI quantification method used in this study can detect subtle changes in IPE distribution and allows for histogram-based analysis of enhancement curves to help identify false-positive enhancement. This approach has the potential of identifying plaques at higher risk of causing future strokes. In a prospective study by Kim et al., 138 patients with intracranial atherosclerotic disease stroke were assessed with HR-VWI, revealing IPE in 78.3% of cases. The authors identified that the 1-year stroke recurrence rate was 30.3% in the “enhancing” group, compared to 6.8% in the “non-enhancing” group of plaques. 32 Similarly, Huang et al. found enhancing plaques in 90% of symptomatic and 50% of asymptomatic patients with intracranial atherosclerosis using HR-VWI. 33 These findings highlight the importance of accurate IPE assessment for risk stratification. Most clinical studies rely on a qualitative assessment of IPE by two adjudicators, 6 moreover, even methods deemed as “objective” may introduce bias, as “enhancing” regions are subjectively selected from two-dimensional views. 10 For instance, Shi et al. highlighted the limitations of two-dimensional sampling for SI analysis of atherosclerotic plaques, due to the lower spatial resolution and challenges of slice positioning in vessels with varied orientations. The authors suggested that 3D SI analysis might offer a more reliable estimation of IPE. 24 Sanchez et al. developed a post-acquisition processing method that uses orthogonal spokes to sample the arterial wall and plaque, creating 3D color maps of arterial and plaque enhancement. This approach achieved an area under the curve of 0.87 for detecting symptomatic plaques. 11 We refined this method by performing 3D plaque segmentation, isolating the arterial wall and assessing the SI distribution of the entire plaque, thereby minimizing potential contamination from adjacent structures. Additionally, we generated 3D color maps and Gd-enhancement histograms for plaque analysis and quality control. In our study, the agreement between subjective and objective IPE determinations was moderate (κ = 0.40). Although not a formal reference standard, voxel-based quantification of IPE provides an objective metric that can aid in resolving reader discrepancies and may enhance the detection of intracranial atherosclerosis in patients with cryptogenic stroke. 4
Plaques exhibiting certain characteristics may appear more likely to enhance, which can be attributed to factors such as larger size or specific locations—such as the middle cerebral artery—which can introduce bias at the time of determining if a plaque is symptomatic. We identified that plaques with >50% stenosis, larger size, greater plaque burden, and a positive remodeling index were more likely to be classified as “enhancing.” These features, commonly observed in symptomatic plaques, also correlate with increased IPE. 10 We identified that adjudicators were less reliable in assessing IPE in plaques located in the posterior circulation (OR, 0.29; 95% CI, 0.09–0.82; p = 0.02). Consistent with our findings, Mossa-Basha et al. reported poor to fair inter-rater reproducibility for atherosclerotic plaques identification located in the vertebrobasilar segments (κ = 0.13–0.26) on 3 T HR-VWI. 34 Consequently, plaque location may affect the reliability of IPE determination. Slow-blood flow with inadequate flow suppression can lead to pseudo enhancement on HR-VWI, 28 a phenomenon that may be more pronounced in posterior circulation arteries due to their slower flow rates. Buijs et al. used two-dimensional phase-contrast magnetic resonance (MR) angiography in 250 adults and found that the mean volume flow rate in the basilar artery was lower than in the internal carotid arteries. 35 Similarly, Zarrinkoob et al. observed via high-resolution phase-contrast magnetic resonance imaging (MRI) that posterior circulation flow rates (202 ± 44 mL/min) were slower than those in the anterior circulation (515 ± 96 mL/min). 36 These confounders may lead to false-positive assessments of IPE in the posterior circulation, even if plaques appear objectively “non-enhancing.” Additionally, hyperdynamic cerebrospinal fluid flow in the prepontine cistern can introduce artifacts, further complicating the assessment of the basilar artery. 34 For instance, Klein et al. reported Gd enhancement of the basilar artery wall in 35% (6/17) of patients with pontine infarction, despite no evidence of intracranial plaques and normal arterial lumen on MR angiography. 37 The assessment of IPE may also be compromised by the peripheral location of the vertebral arteries within the imaging field, where reduced signal quality and artifacts limit reliable interpretation. In contrast, voxel-based IPE quantification enables histogram analysis of pre- and post-contrast enhancement curves, helping to distinguish true enhancement from false positives based on the distribution of SI changes.
This study has several limitations. First, we compared subjective IPE assessment to a quantification method that, although subjected to multiple quality checks via histogram analyses, is not validated as a reference standard. Consequently, this prevented us from performing receiver operating characteristic analysis. Second, the cross-sectional design precludes establishing causal relationships between IPE and clinical outcomes such as stroke recurrence. Third, inadequate blood-flow suppression may have influenced the subjective evaluation of IPE, although the objective method's histogram analysis of color maps helped detect false positives. Fourth, partial blinding of adjudicators to stroke location may have introduced bias in the subjective assessment of IPE; however, full blinding was not feasible, as stroke location is visible on imaging. Fifth, patient enrollment for 7 T HR-VWI was constrained by logistical barriers, including medical contraindications and claustrophobia, which limited our study population. Due to the sample size, there is a potential risk of overfitting bias in the multivariable analysis; however, this is a pilot study and validation in an external cohort is needed to confirm our findings and improve generalizability. Sixth, quantitative metrics were not provided to the readers during plaque enhancement assessment, thereby precluding evaluation of whether these metrics influenced their interpretation or improved diagnostic performance. However, in most clinical practices, neuroradiologists do not use quantitative metrics in the determination of increased enhancement. Finally, all conclusions are based on 7 T data; however, the study was done with a 7 T scanner to maximize the spatial resolution at the time of subjective adjudication.
A standardized definition of IPE is essential. Although 7 T HR-VWI offers improved spatial resolution, slow flow artifacts—particularly in posterior circulation arteries—can mimic enhancement and lead to misinterpretation. Recognizing these limitations, the adoption of standardized and objective methods is recommended to reliably differentiate true enhancement from pseudoenhancement. Such approaches can reduce interobserver variability, resolve cases of disagreement, and improve risk stratification, as enhancing plaques are linked to a higher risk of stroke recurrence in patients with intracranial atherosclerotic disease.
Conclusion
Subjective assessment of IPE on 7 T HR-VWI demonstrates poor inter-rater agreement (κ = 0.34), reflecting inherent observer variability and susceptibility to human error. In contrast, voxel-based quantification provides objective enhancement metrics that are independent of reader interpretation. This method may improve the reliability of IPE evaluation, particularly in challenging cases such as non-stenotic or negatively remodeling plaques in the posterior circulation.
Supplemental Material
sj-docx-1-ine-10.1177_15910199251368719 - Supplemental material for Inter-rater reliability of atherosclerotic plaque enhancement on 7 T vessel wall MRI: Comparison with quantitative analysis
Supplemental material, sj-docx-1-ine-10.1177_15910199251368719 for Inter-rater reliability of atherosclerotic plaque enhancement on 7 T vessel wall MRI: Comparison with quantitative analysis by Carlos Dier, Sultan Alhajahjeh, Abdallah A Alqudah, Andres Gudino, Navami Shenoy, Martin A Cabarique, Elena Sagues, Sebastian Sanchez, Connor Aamot, Linder Wendt, Bruno A Policeni, Minako Hayakawa and Edgar A Samaniego in Interventional Neuroradiology
Footnotes
Ethical approval and informed consent statements
Written informed consent was obtained from all subjects (patients) in this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Roy J. and Lucille A. Carver College of Medicine, University of Iowa, (grant number 1S10RR028821-01).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.